
Implementing Brief Tobacco Cessation Interventions in Community Pharmacies: An Application of Rogers’ Diffusion of Innovations Theory

 , , and
, , and
Abstract
:1. Introduction
1.1. Pharmacists’ Role in Tobacco Cessation
1.2. Brief Interventions for Tobacco Cessation in Community Pharmacies: Ask-Advise-Refer
2. Material and Methods
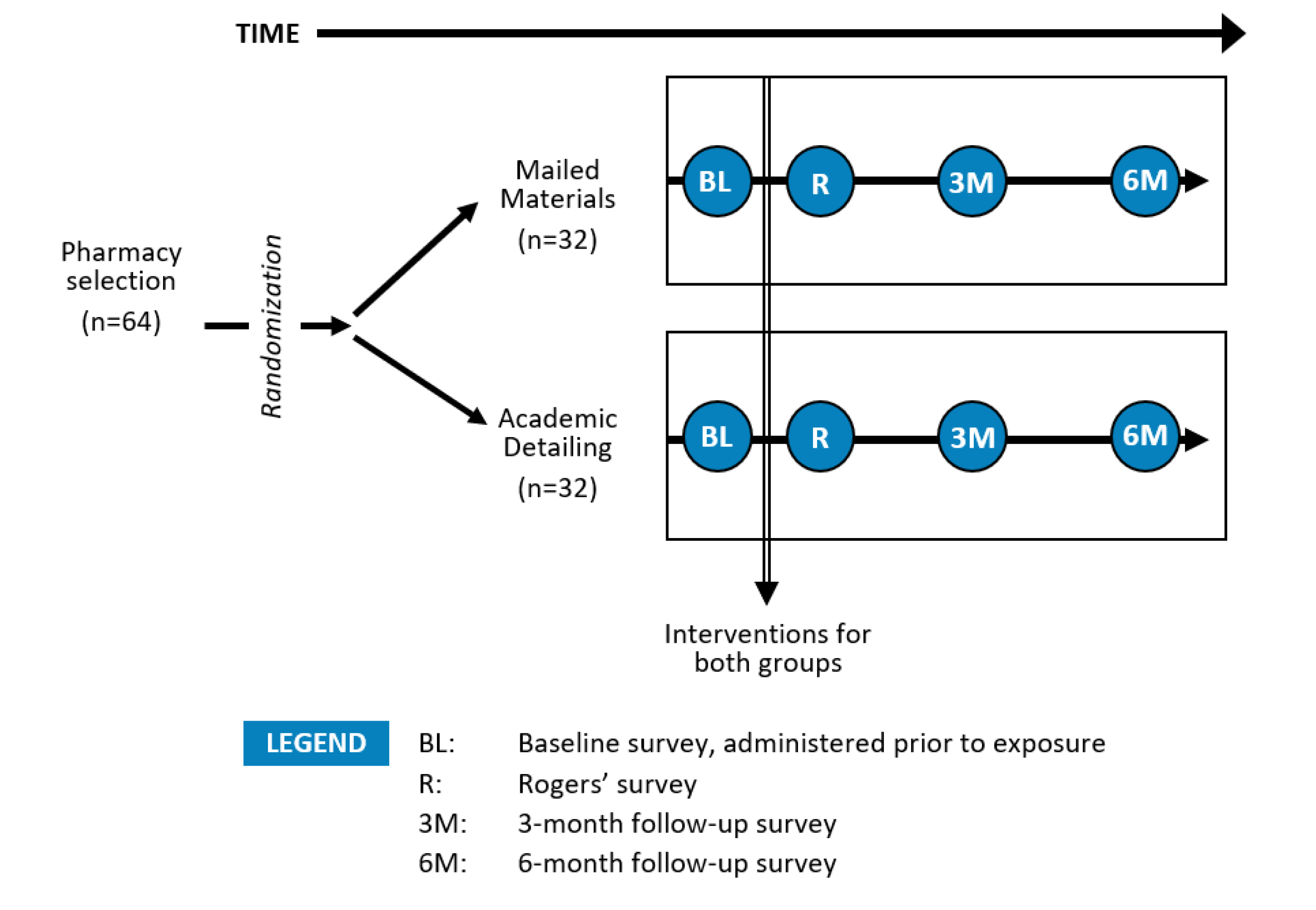
2.1. Study Design
2.2. Intervention Arms
2.3. Study Measures
2.4. Statistical Analyses
3. Results
3.1. Pharmacy and Pharmacist Characteristics
3.2. Perceived Characteristics of the Ask-Advise-Refer Approach
3.3. Anticipated Use of Implementation Materials
3.4. Barriers to Implementing Ask-Advise-Refer
3.5. Self-Reported Personal Efforts and Success in Implementing Ask-Advise-Refer
3.6. Perceived Role of Pharmacy in Tobacco Cessation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Babb, S.; Malarcher, A.; Schauer, G.; Asman, K.; Jamal, A. Quitting Smoking among Adults—United States, 2000–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 65, 1457–1464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobbie, F.; Hiscock, R.; Leonardi-Bee, J.; Murray, S.; Shahab, L.; Aveyard, P.; Coleman, T.; McEwen, A.; McRobbie, H.; Purves, R.; et al. Evaluating Long-term Outcomes of NHS Stop Smoking Services (ELONS): A prospective cohort study. Health Technol. Assess. 2015, 19, 1–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merritt Hawkins. 2017 Survey of Physician Appointment Wait Times and Medicare and Medicaid Acceptance Rates. Available online: https://www.merritthawkins.com/news-and-insights/thought-leadership/survey/survey-of-physician-appointment-wait-times/ (accessed on 24 May 2022).
- Hefner, J.L.; Wexler, R.; McAlearney, A.S. Primary care access barriers as reported by nonurgent emergency department users: Implications for the US primary care infrastructure. Am. J. Med. Qual. 2015, 30, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Qato, D.M.; Zenk, S.; Wilder, J.; Harrington, R.; Gaskin, D.; Alexander, G.C. The availability of pharmacies in the United States: 2007–2015. PLoS ONE 2017, 12, e0183172. [Google Scholar] [CrossRef] [Green Version]
- Hudmon, K.S.; Prokhorov, A.V.; Corelli, R.L. Tobacco cessation counseling: Pharmacists’ opinions and practices. Patient Educ. Couns. 2006, 61, 152–160. [Google Scholar] [CrossRef]
- Aquilino, M.L.; Farris, K.B.; Zillich, A.J.; Lowe, J.B. Smoking-cessation services in Iowa community pharmacies. Pharmacotherapy 2003, 23, 666–673. [Google Scholar] [CrossRef]
- Saba, M.; Diep, J.; Saini, B.; Dhippayom, T. Meta-analysis of the effectiveness of smoking cessation interventions in community pharmacy. J. Clin. Pharm. Ther. 2014, 39, 240–247. [Google Scholar] [CrossRef]
- Carson-Chahhoud, K.V.; Livingstone-Banks, J.; Sharrad, K.J.; Kopsaftis, Z.; Brinn, M.P.; To-A-Nan, R.; Bond, C.M. Community pharmacy personnel interventions for smoking cessation. Cochrane Database Syst. Rev. 2019, CD003698. [Google Scholar] [CrossRef]
- Bauld, L.; Boyd, K.A.; Briggs, A.H.; Chesterman, J.; Ferguson, J.; Judge, K.; Hiscock, R. One-year outcomes and a cost-effectiveness analysis for smokers accessing group-based and pharmacy-led cessation services. Nicotine Tob. Res. 2011, 13, 135–145. [Google Scholar] [CrossRef]
- Dent, L.A.; Harris, K.J.; Noonan, C.W. Tobacco interventions delivered by pharmacists: A summary and systematic review. Pharmacotherapy 2007, 27, 1040–1051. [Google Scholar] [CrossRef]
- Patwardhan, P.D.; Chewning, B.A. Ask, advise and refer: Hypothesis generation to promote a brief tobacco—Cessation intervention in community pharmacies. Int. J. Pharm. Pract. 2009, 17, 221–229. [Google Scholar] [CrossRef] [PubMed]
- McBane, S.E.; Corelli, R.L.; Albano, C.B.; Conry, J.M.; Della Paolera, M.A.; Kennedy, A.K.; Jenkins, A.T.; Hudmon, K.S. The role of academic pharmacy in tobacco cessation and control. Am. J. Pharm. Educ. 2013, 77, 93. [Google Scholar] [CrossRef] [Green Version]
- Wray, J.M.; Funderburk, J.S.; Acker, J.D.; Wray, L.O.; Maisto, S.A. A Meta-Analysis of Brief Tobacco Interventions for Use in Integrated Primary Care. Nicotine Tob. Res. 2018, 20, 1418–1426. [Google Scholar] [CrossRef] [PubMed]
- Chavarria, J.; Liu, M.; Kast, L.; Salem, E.; King, A.C. A pilot study of Counsel to Quit®: Evaluating an Ask Advise Refer (AAR)-based tobacco cessation training for medical and mental healthcare providers. J. Subst. Abuse Treat. 2019, 99, 163–170. [Google Scholar] [CrossRef]
- Simerson, D.; Hackbarth, D. Emergency Nurse Implementation of the Brief Smoking-Cessation Intervention: Ask, Advise, and Refer. J. Emerg. Nurs. 2018, 44, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Baggarly, S.A.; Jenkins, T.L.; Biglane, G.C.; Smith, G.W.; Smith, C.M.; Blaylock, B.L. Implementing a referral to telephone tobacco cessation services in Louisiana community pharmacies: A pilot study. Ann. Pharmacother. 2010, 44, 1395–1402. [Google Scholar] [CrossRef] [PubMed]
- Patwardhan, P.D.; Chewning, B.A. Effectiveness of intervention to implement tobacco cessation counseling in community chain pharmacies. J. Am. Pharm. Assoc. 2012, 52, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Hudmon, K.S.; Corelli, R.L.; de Moor, C.; Zillich, A.J.; Fenlon, C.; Miles, L.; Prokhorov, A.V.; Zbikowski, S.M. Outcomes of a randomized trial evaluating two approaches for promoting pharmacy-based referrals to the tobacco quitline. J. Am. Pharm. Assoc. 2018, 58, 387–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenhalgh, T.; Macfarlane, F.; Steed, L.; Walton, R. What works for whom in pharmacist-led smoking cessation support: Realist review. BMC Med. 2016, 14, 209. [Google Scholar] [CrossRef] [Green Version]
- Rogers, E.M. Diffusion of Innovations, 5th ed.; The Free Press: New York, NY, USA, 2003. [Google Scholar]
- Corelli, R.L.; Zillich, A.J.; de Moor, C.; Giuliano, M.R.; Arnold, J.; Fenlon, C.M.; Douglas, C.L.; Magnusson, B.; Zbikowski, S.M.; Prokhorov, A.V.; et al. Recruitment of community pharmacies in a randomized trial to generate patient referrals to the tobacco quitline. Res. Soc. Adm. Pharm. 2013, 9, 396–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zillich, A.J.; Corelli, R.L.; Zbikowski, S.M.; Magnusson, L.B.; Fenlon, C.M.; Prokhorov, A.V.; de Moor, C.; Hudmon, K.S. A randomized trial evaluating 2 approaches for promoting pharmacy-based referrals to the tobacco quitline: Methods and baseline findings. Res. Soc. Adm. Pharm. 2013, 9, 27–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Celebrating the 15th Anniversary of the National Network of Tobacco Cessation Quitlines; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2019. [Google Scholar]
- Corelli, R.L.; Fenlon, C.M.; Kroon, L.A.; Prokhorov, A.V.; Hudmon, K.S. Evaluation of a train-the-trainer program for tobacco cessation. Am. J. Pharm. Educ. 2007, 71, 109. [Google Scholar] [PubMed] [Green Version]
- Corelli, R.L.; Kroon, L.A.; Chung, E.P.; Sakamoto, L.M.; Gundersen, B.; Fenlon, C.M.; Hudmon, K.S. Statewide evaluation of a tobacco cessation curriculum for pharmacy students. Prev. Med. 2005, 40, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Lang, W.; Elkhadragy, N.; Hudmon, K.S. Not blowing smoke: Academic pharmacy aims to reduce tobacco use to ashes. Acad. Pharm. Now 2016, 9, 12–20. [Google Scholar]
- Adams, A.J.; Hudmon, K.S. Pharmacist prescriptive authority for smoking cessation medications in the United States. J. Am. Pharm. Assoc. 2018, 58, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Hudmon, K.S.; Hoch, M.A.; Vitale, F.M.; Wahl, K.R.; Corelli, R.L.; de Moor, C. Tobacco cessation education for pharmacists: Face-to-face presentations versus live webinars. J. Am. Pharm. Assoc. 2014, 54, 42–44. [Google Scholar] [CrossRef] [PubMed]
- Hudmon, K.S.; Addleton, R.L.; Vitale, F.M.; Christiansen, B.A.; Mejicano, G.C. Advancing public health through continuing education of health care professionals. J. Contin. Educ. Health Prof. 2011, 31 (Suppl. S1), S60–S66. [Google Scholar] [CrossRef] [PubMed]
- Prokhorov, A.V.; Hudmon, K.S.; Marani, S.; Foxhall, L.; Ford, K.H.; Luca, N.S.; Wetter, D.W.; Cantor, S.B.; Vitale, F.; Gritz, E.R. Engaging physicians and pharmacists in providing smoking cessation counseling. Arch. Intern. Med. 2010, 170, 1640–1646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, B.A.; Bruskiewitz, R.H.; Chewning, B.A. Effect of a tobacco cessation continuing professional education program on pharmacists’ confidence, skills, and practice-change behaviors. J. Am. Pharm. Assoc. 2010, 50, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guglielmo, B.J. A prescription for improved chronic disease management: Have community pharmacists function at the top of their training: Comment on “Engaging physicians and pharmacists in providing smoking cessation counseling”. Arch. Intern. Med. 2010, 170, 1646–1647. [Google Scholar] [CrossRef]
- Corelli, R.L.; Merchant, K.R.; Hilts, K.E.; Kroon, L.A.; Vatanka, P.; Hille, B.T.; Hudmon, K.S. Community pharmacy technicians’ engagement in the delivery of brief tobacco cessation interventions: Results of a randomized trial. Res. Soc. Adm. Pharm. 2021, 18, 3158–3163. [Google Scholar] [CrossRef] [PubMed]
- Curran, G.M.; Shoemaker, S.J. Advancing pharmacy practice through implementation science. Res. Soc. Adm. Pharm. 2017, 13, 889–891. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Implementation Materials | Academic Detailing | Mailed Materials |
|---|---|---|
| Cover letter from the state quitline, describing the project and its collaborators/endorsers, including state and national pharmacy associations | ✓ | ✓ |
| A 1-page document describing the efficacy of the quitline and the process that occurs when a patient calls the quitline | ✓ | ✓ |
| Quitline cards | ✓ | ✓ |
| Quitline tri-fold brochures | ✓ | ✓ |
| Plastic counter-top display to hold the quitline cards and quitline brochures | ✓ | ✓ |
| “Ready to Quit? I can help” buttons to be worn on the lapel of pharmacy staff | ✓ | ✓ |
| Quitline stickers for placement on prescription bags | ✓ | ✓ |
| Quitline posters to be placed on walls near the pharmacy counter | ✓ | ✓ |
| Pharmacologic Product Guide and Drug Interactions with Tobacco Smoke resources for use by pharmacists (laminated) | ✓ | ✓ |
| How to Implement Ask-Advise-Refer resource, describing the step-by-step process for use by pharmacists and technicians (laminated) | ✓ | ✓ |
| Re-order form for materials | ✓ | ✓ |
| Quitline fax referral forms | ✓ | |
| CD-ROM with videos demonstrating Ask-Advise-Refer in a pharmacy setting | ✓ | |
| Relevant published literature supporting the concept of the tobacco quitline | ✓ |
| Characteristics and Confidence | Overall | Mailed Materials (n = 59) | Academic Detailing (n = 61) | p-Value |
|---|---|---|---|---|
| Characteristics of Ask-Advise-Refer [21] | ||||
| Compatibility of the Ask-Advise-Refer approach with your daily workflow in the pharmacy | 3.1 (0.6) | 3.2 (0.7) | 3.0 (0.6) | 0.24 |
| Advantage of the Ask-Advise-Refer approach over other tobacco cessation counseling approaches | 3.3 (0.7) | 3.2 (0.7) | 3.3 (0.6) | 0.50 |
| Acceptability of the Ask-Advise-Refer approach of implementing into routine practice | 3.2 (0.7) | 3.3 (0.6) | 3.2 (0.7) | 0.56 |
| Appropriateness of the Ask-Advise-Refer approach for use in your pharmacy | 3.4 (0.6) | 3.4 (0.6) | 3.4 (0.6) | 0.88 |
| Clarity of the three steps (Ask, Advise, Refer) | 3.7 (0.6) | 3.6 (0.6) | 3.7 (0.5) | 0.23 |
| Confidence in implementing Ask-Advise-Refer | ||||
| Personal confidence in ability to routinely implement AAR approach | 3.2 (0.7) | 3.2 (0.7) | 3.1 (0.7) | 0.49 |
| Confidence in pharmacy’s ability to routinely implement AAR approach | 3.1 (0.7) | 3.2 (0.7) | 3.0 (0.6) | 0.12 |
| Implementation Materials | Overall | Mailed Materials (n = 59) | Academic Detailing (n = 61) | p-Value |
|---|---|---|---|---|
| Quitline cards | 3.5 (0.7) | 3.5 (0.7) | 3.5 (0.7) | 0.79 |
| Quitline brochures | 3.6 (0.6) | 3.6 (0.5) | 3.6 (0.7) | 0.75 |
| Counter-top display | 3.6 (0.7) | 3.5 (0.8) | 3.6 (0.7) | 0.48 |
| Pharmacologic product guide | 3.2 (0.8) | 3.3 (0.7) | 3.0 (0.8) | 0.08 |
| Drug interactions with smoking table | 3.2 (0.8) | 3.2 (0.7) | 3.1 (0.9) | 0.91 |
| “Ready to quit? I can help” buttons | 2.6 (1.0) | 2.7 (1.0) | 2.5 (0.9) | 0.41 |
| Quitline stickers for prescription bags | 3.0 (0.9) | 3.1 (0.8) | 2.9 (0.9) | 0.19 |
| Quitline posters | 3.3 (0.9) | 3.3 (0.8) | 3.3 (0.9) | 0.83 |
| Barriers to Implementing Ask-Advise-Refer | Overall | Mailed Materials (n = 59) | Academic Detailing (n = 61) | p-Value |
|---|---|---|---|---|
| Lack of available time | 3.7 (1.1) | 3.8 (1.1) | 3.6 (1.1) | 0.43 |
| Lack of training | 2.6 (1.1) | 2.8 (1.2) | 2.4 (1.0) | 0.09 |
| Discomfort in asking patients about tobacco use | 2.7 (1.2) | 2.8 (1.3) | 2.7 (1.1) | 0.70 |
| Lack of staff’s perceived importance of tobacco cessation counseling as applicable to job | 2.4 (1.1) | 2.4 (1.2) | 2.5 (1.0) | 0.66 |
| Lack of confidence in counseling patients about quitting | 2.2 (1.0) | 2.2 (1.0) | 2.1 (0.9) | 0.55 |
| Rogers’ Characteristics and Barriers | Personal Efforts (rs) | Personal Success (rs) |
|---|---|---|
| Characteristics of Ask-Advise-Refer [21] | ||
| Compatibility of the Ask-Advise-Refer approach with your daily workflow in the pharmacy | 0.39 b | 0.36 b |
| Advantage of the Ask-Advise-Refer approach over other tobacco cessation counseling approaches | 0.29 b | 0.32 b |
| Acceptability of the Ask-Advise-Refer approach of implementation into routine practice | 0.27 b | 0.21 c |
| Appropriateness of the Ask-Advise-Refer approach for use in your pharmacy | 0.16 | 0.12 |
| Clarity of the three steps (Ask, Advise, Refer) | 0.14 | 0.12 |
| Barriers to implementing Ask-Advise-Refer | ||
| Lack of available time | −0.24 c | −0.21 c |
| Lack of training | −0.16 | −0.18 |
| Discomfort in asking patients about tobacco use | −0.31 b | −0.28 b |
| Lack of staff’s perceived importance of tobacco cessation counseling as applicable to job | −0.18 | −0.17 |
| Lack of confidence in counseling patients about quitting | −0.19 | −0.24 c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hilts, K.E.; Corelli, R.L.; Prokhorov, A.V.; Zbikowski, S.M.; Zillich, A.J.; Hudmon, K.S. Implementing Brief Tobacco Cessation Interventions in Community Pharmacies: An Application of Rogers’ Diffusion of Innovations Theory. Pharmacy 2022, 10, 56. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy10030056
Hilts KE, Corelli RL, Prokhorov AV, Zbikowski SM, Zillich AJ, Hudmon KS. Implementing Brief Tobacco Cessation Interventions in Community Pharmacies: An Application of Rogers’ Diffusion of Innovations Theory. Pharmacy. 2022; 10(3):56. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy10030056
Chicago/Turabian StyleHilts, Katy Ellis, Robin L. Corelli, Alexander V. Prokhorov, Susan M. Zbikowski, Alan J. Zillich, and Karen Suchanek Hudmon. 2022. "Implementing Brief Tobacco Cessation Interventions in Community Pharmacies: An Application of Rogers’ Diffusion of Innovations Theory" Pharmacy 10, no. 3: 56. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy10030056