
Alcohol-Based Hand Sanitizers in COVID-19 Prevention: A Multidimensional Perspective


1
Department of Pharmaceutical Chemistry, School of Pharmacy, University of Nairobi, Nairobi P.O. Box 19676-00202, Kenya
2
Pharma Manufacturing Solutions, Nairobi P.O. Box 21297-00505, Kenya
*
Author to whom correspondence should be addressed.
Pharmacy 2021, 9(1), 64; https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy9010064
Submission received: 17 February 2021
/
Revised: 12 March 2021
/
Accepted: 16 March 2021
/
Published: 19 March 2021
Abstract
:The global use of alcohol-based hand sanitizers (ABHS) as an important means of controlling the transmission of infectious disease has increased significantly as governments and public health agencies across the world advocated hand hygiene as a preventative measure during the COVID-19 pandemic. Although the performance of these products is most commonly defined as a function of their alcohol concentration, they are multifaceted products in which an interplay of several factors is important in determining efficacy. This paper discusses the interplay between ABHS input (formulation) factors and output (product performance) factors in the context of a multidimensional perspective using a novel representative paradigm. In the model, represented in the form of a three-dimensional tetrahedron, each of the faces represents inputs in the manufacturing of the ABHS product, which are the type and amount of alcohol, the inactive ingredients, the formulation and the manufacturing practices. The four corners of the tetrahedron represent the product performance factors which include product efficacy, sensory characteristics, usage and compliance and product safety. The multidimensional approach to the formulation and evaluation of ABHS shows that several factors contribute to the effectiveness and utility of these products. The paradigm provides a useful framework for manufacturers of ABHS and related healthcare products.
1. Introduction
Alcohol-based hand sanitizers (ABHS) have emerged as an important tool in the fight against SARS-CoV-2, the virus that causes coronavirus disease 2019 (COVID-19) [1]. The disease has spread rapidly throughout the world thereby necessitating stringent measures and controls to minimize its transmission. One of the key measures that has been advocated is the need to ensure hand hygiene [2].
Hand sanitizers are products that are applied and rubbed on hands to inactivate pathogenic microorganisms. These products are designed to dry rapidly after application, thereby eliminating the need for soap, water and drying aids such as towels. The convenience and portability of hand sanitizers has led to their widespread usage in 2020 as ABHS were recommended by the World Health Organization (WHO) as an alternative hand hygiene measure [3].
Ethanol and isopropanol (2-propanol) are the commonly used alcohols in ABHS. They are typically formulated as aqueous mixtures with several other ingredients such as emollients, moisturizers and fragrances. Although the major focus of ABHS performance has been the alcohol concentration, added ingredients and auxiliary factors play a critical role in their efficacy, safety and long-term utility.
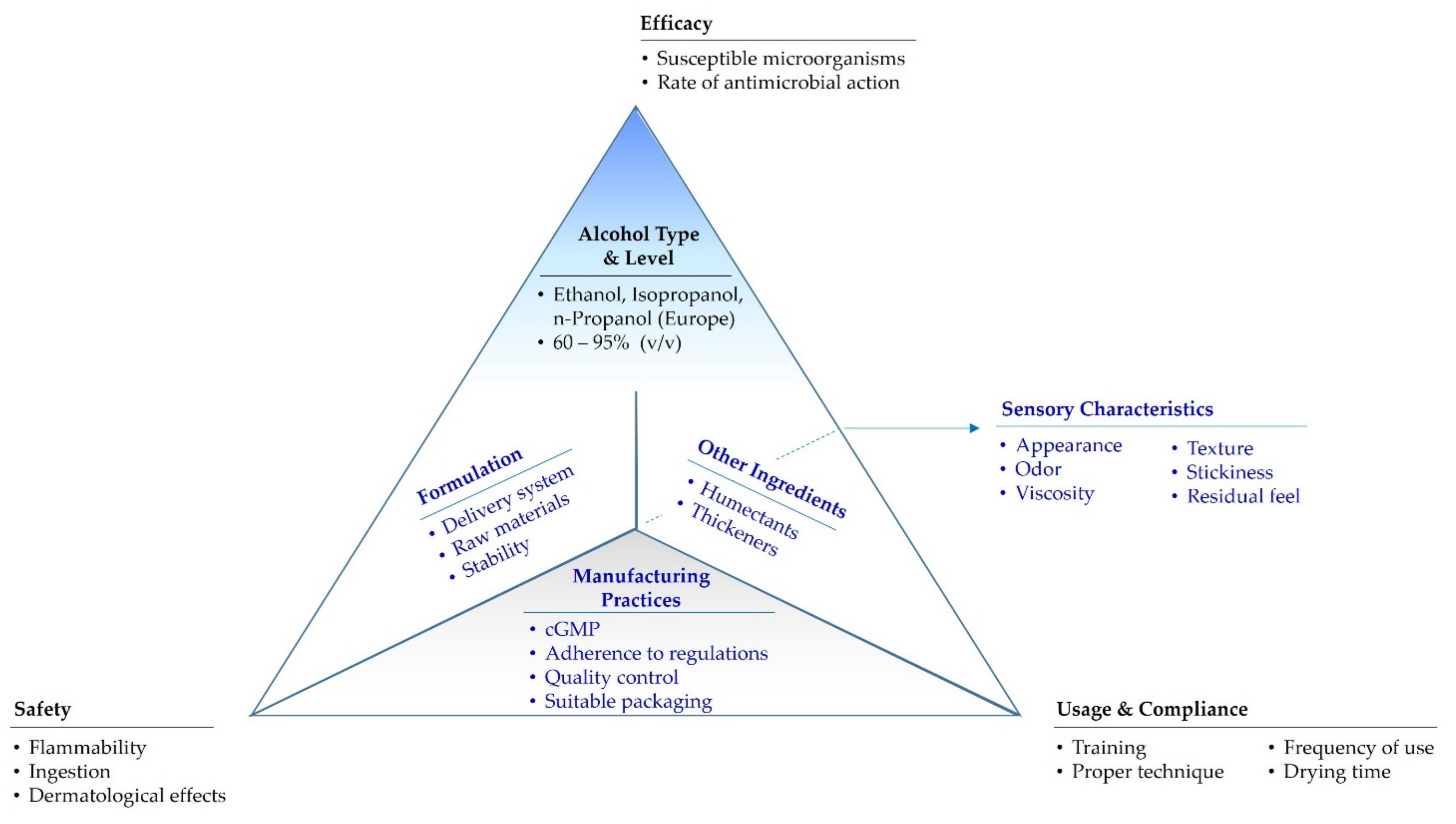
In this paper, the factors influencing the attributes of ABHS form a new multidimensional paradigm which is conveniently illustrated in the form of a tetrahedron (Figure 1). In this model, each of the faces of the tetrahedron represents inputs in the manufacturing of the product, i.e., (1) the type and amount of alcohol, (2) inactive ingredients, (3) the formulation, and (4) manufacturing practices. The four corners of the tetrahedron represent the product performance factors: (1) efficacy, (2) sensory characteristics, (3) usage and compliance and (4) product safety. While these factors are often considered individually, the long-term use of ABHS requires that manufacturers of these products address the manner in which the factors relate to each other and are integrated to provide a quality product.
2. Faces of the Tetrahedron: Inputs
The principal ingredients in ABHS are an alcohol (or mixture of alcohols) and water. Additionally, ABHS may have other ingredients which perform a variety of functions (Table 1). The influence of these ingredients on product efficacy, safety and usage must be considered. The WHO has developed two formulations based on either ethanol (80% v/v) or isopropanol (75% v/v) with glycerol (1.45% v/v) and hydrogen peroxide (0.125% v/v) [4]. Kratzel et al. demonstrated that WHO based formulations had broad spectrum antimicrobial activity including efficacy against SARS-CoV-2 [5]. Firms which manufacture commercial ABHS on a regular basis typically use proprietary formulations.
2.1. Alcohol Type and Level
The active ingredient in ABHS is an aqueous alcohol solution in optimized concentrations. Alcohols are known to possess broad-spectrum antimicrobial activity against bacteria, fungi and viruses. While the specific mechanism of action of alcohols is not clear, it is thought to be related to denaturation of membrane and enzymatic proteins [6,7,8].
Three alcohol homologs are utilized in ABHS namely, ethanol, isopropanol and n-propanol. In the United States, however, the Food and Drug Administration (FDA) does not permit the use of n-propanol in ABHS [9,10].
From the foregoing, the two most widely used alcohols in ABHS formulations are ethanol and isopropanol. Isopropanol is more effective against bacteria while ethanol is favorably virucidal, which may be due to differences in polarity [6]. Amongst the usable alcohols, ethanol emerges as the most common choice since it is easily produced through fermentation and distillation. For the formulation of ABHS, pharmaceutical or food grade ethanol is recommended. The use of technical grade alcohol is typically not permitted due the high level of impurities. Nevertheless, due to the high demand for ABHS during the COVID-19 pandemic, special authorization to use these products may be granted provided the raw materials meet the acceptance criteria that would justify application. The FDA guidance specifies control of alcohol impurities such as benzene, methanol, acetaldehyde and acetal to levels below specified limits. Non-compliance with these limits necessitates further testing for specific residual solvents [9].
The efficacy of alcohol as an antiseptic is dependent on its concentration. The recommended alcohol concentration in ABHS is generally cited as 60–95% (v/v). However, the optimum level is nuanced and is not necessarily the same for ethanol and isopropanol. This recommended alcohol ranges permit the alcohol to interact with functional proteins thus inactivating them. The lower range (60–75%) readily denatures proteins while higher levels (>95%) cause coagulation of membrane proteins hence preventing the alcohol from entering the cell. Moreover, alcohol levels of above 80% may reduce the contact time due to volatility which undermines efficacy of the formulation as well as adverse skin tolerance [11].
It may be desirable to prefer a median alcohol concentration of 70–80% (v/v). Products formulated with alcohol levels close to the 60% lower limit risk the active ingredient content falling below the threshold during processing, transport, storage or use as constituent alcohols may evaporate. Post market surveillance reports by regulatory authorities in a number of countries have found some products with alcohol assays below threshold limits [12,13].
2.2. Inactive Ingredients
Key considerations with regards to the use of ingredients are their influence on ABHS efficacy, safety and usage. The most commonly added ingredients in commercial ABHS formulations are humectants, thickeners and fragrances. Humectants such as glycerol help counteract the drying effect of alcohols, which may otherwise adversely affect skin integrity, especially with frequent and long term ABHS use. Thickeners, are added to increase viscosity and facilitate application of ABHS by making them easier to handle and reducing spillage. They are most often polymers of acrylic acid and its derivatives such as carbomers [11].
The other commonly encountered ingredients in commercial ABHS products are aloe and tocopherols, which in addition to possible beneficial dermatological effects, may enhance marketing appeal. Denaturing agents, such as denatonium benzoate, sucrose octaacetate, isopropanol or triethyl citrate are added to deter ingestion of ABHS [9].
The effects of ingredients in ABHS formulations may be complex sometimes resulting in unintended outcomes. An interesting example is glycerol, the most frequently used humectant, intended to reduce dryness and irritation of the products. Although structurally a sugar alcohol with reported antimicrobial activity of its own at high concentrations [14], a number of studies have reported that glycerol can reduce the antimicrobial activity of ABHS [15,16,17,18]. In a study which used the ethanol-based WHO formulation, lowering the glycerol level to 0.5% (v/v) was recommended as an optimal balance between antimicrobial efficacy and dermal tolerability [18]. The reason for glycerol’s effects on antimicrobial efficacy has not been elucidated, but may be related to its viscosity (which decreases the diffusion of the germicidal alcohol) when used above optimal levels. Since drying of the hands can be detrimental to skin integrity, the most commonly suggested solution has been to use a lower level of glycerol (as opposed to eliminating it completely).
Certain ingredients can potentiate antimicrobial ABHS activity. Organic acids, such as citric acid and phosphoric acid have been reported to increase the activity of ABHS against non-enveloped viruses [19,20,21,22].
Non-alcohol based hand sanitizers contain other antimicrobial agents such as benzalkonium chloride (BKC) [23]. Unlike alcohols, these ingredients are not volatile and hence antimicrobial activity can persist for longer periods [24]. Chlorhexidine is an example of an antimicrobial agent which has been combined with alcohol in some ABHS products [25,26] although its additional benefit has been questioned [27,28]. The use of such combinations is uncommon and may be restricted to ABHS employed in health care settings in some countries. Nevertheless, the use of non-alcoholic sanitizers in healthcare facilities is not recommended by the WHO.
An area which has not been extensively studied with ABHS is the potential for interactions between the various formulation ingredients. One reported example is that of chlorhexidine, which is cationic, with carbomer (an anionic polymer). Inactivation of chlorhexidine activity was observed in the presence of a carbomer containing ABHS [29]. There is also a potential for chlorhexidine to interact with anionic emulsifiers [30].
Additional potential interactions may arise from the presence of hydrogen peroxide (H2O2), a strong oxidizing agent which is a component of the two WHO recommended formulations [4]. The function of H2O2 is to inactivate bacterial spores as alcohols lack sporicidal action.
In good manufacturing practice (GMP) manufacturing environments, with more stringent control of raw materials, facilities and equipment, the use of H2O2 in the formulation is atypical. In cases where H2O2 is used, any ingredients that are susceptible to oxidation should not be included. Interactions between H2O2 and gel-forming polyacrylic acid polymers leading to a reduction in liquid viscosity have been reported [31]. In the study, polymer cross-link density, peroxide levels and the source/grade of H2O2 were shown to influence changes in viscosity.
The potential for ingredient–ingredient interactions and ingredient–container interactions will increase with the number of raw materials used in the formulation. Therefore, manufacturers should carefully consider the necessity of each added ingredient to the formulation.
2.3. Formulation
A number of delivery systems can be used for ABHS including liquids, gels, sprays, foams and wipes (Table 2). In hospitals and other public facilities, hand sanitizers are commonly packaged in dispensers. Low viscosity liquids and gels are the most common delivery modes for ABHS sold to the general public. Gels are essentially liquids with a significantly higher viscosity which assists in their application, especially from smaller containers. Free flowing liquids are better suited to delivery systems which have a higher degree of metering capability (e.g., dispensers, sprays and containers equipped with pump fittings).
Gels, along with foams, are preferred by many users due to greater ease of handling compared to low viscosity liquids [34]. Some studies, however, have suggested that the viscosity of gels may lower antimicrobial activity, possibly due to reduced diffusivity of the alcohol [35,36]. However, it appears that formulation factors such as increasing the concentration of alcohol may in such cases be used to improve efficacy [35].
The very different nature of other delivery formats makes comparisons challenging. Wipes or towelettes are a format that may be preferred by some people as they avoid the possibility of spillage that is associated with liquids or gels. A number of studies have compared different delivery systems. In one study, gel, foam and wipe ABHS delivery systems were comparable (no significant differences) in the reduction of virus counts on the hands [37]. Another study comparing a single-use ABHS packet that released product when folded to a single-use wipe revealed that patients in hospital or long-term care facility preferred the single-use packet to the wipe because they found it easier to handle [38].
2.4. Manufacturing and Packaging
In order to ensure that ABHS of suitable quality are produced, GMPs should be followed in their production. This includes the use of suitable manufacturing facilities, equipment, raw materials, systems, procedures, quality control testing, storage and distribution along with the requisite documentation and records.
Many countries have specific regulations that govern the production of ABHS [39]. In Europe, ABHS are regulated under the Biocidal Products Regulation [11,40] while in the United States, they are regulated as drug products by the FDA. Furthermore, the FDA distinguishes between health care and consumer antiseptic products [41].
Raw materials should meet the established standards for the countries in which the ABHS are marketed. For example, in the US, ethanol, isopropanol and glycerol should meet United States Pharmacopoeia (USP) or Food Chemicals Codex (FCC) specifications [9].
The safety of personnel involved in manufacturing and packaging operations is critical, especially given the potential of organic solvents to be flammable under uncontrolled conditions. Therefore, proper storage of alcohols and the use of air-conditioned and well-ventilated manufacturing rooms is necessary. Equipment grounding, the use of pneumatic mixers to prevent static discharge, lowering oxygen levels in mixing vessels and keeping alcohol vapor levels in the manufacturing rooms below threshold limits are examples of production safety measures that can be implemented [42].
While packaging may be sometimes considered secondary to the formulation of the ABHS, it is a critical component in ensuring product integrity, stability and delivery. ABHS are most commonly packaged in plastic containers. Container corrosion has been observed for the ethanol-based WHO formulation when packaged in aluminum beer cans [43].
Dispensers are commonly used for ABHS delivery in hospitals and other settings with high numbers of people. The design and function of dispensers are important in ensuring their effectiveness. In a study at a hospital which had recently installed dispensers, malfunctioning was found to be a common occurrence [44]. The need for regular auditing and maintenance of dispenser units has thus been stressed [45].
3. Corners of the Tetrahedron: Outputs
3.1. ABHS Efficacy
The efficacy of an ABHS is its key performance attribute. Depending on the application, target microorganisms and delivery mode, there are diverse standard test methods used to determine product efficacy [46]. Efficacy testing is generally performed using tests that measure the number of microorganisms before and after treatment with ABHS. Test results are typically expressed in terms of log10 reduction factors. The key factors influencing ABHS efficacy are the level and the type of alcohol used. However, added ingredients can also have significant influence on efficacy. For example, recent studies have shown that while the current WHO formulations do not meet the requirements for EN 1500 (hygienic hand rub) or EN 12,791 (surgical hand preparation), using higher alcohol levels (i.e., 80% ethanol or 75% isopropanol on a weight instead of the current volume basis) and lowering the glycerol level to 0.5% (v/v) enables these modified formulations to meet both EN test criteria [47].
3.2. Sensory Characteristics
The sensory characteristics of ABHS include the appearance, odor, viscosity, texture, skin feel, stickiness and residual feel of the product. Although sensory properties may not directly influence the efficacy of the product, they do play an important role in determining aesthetic appeal, which in turn determines the likelihood of individuals using a given product. Therefore, improving compliance may help reduce the transmission of infectious disease. The use of fragrances mitigates the intensity of the alcohol odor and also serves to distinguish various products, therefore making it an important manufacturing consideration.
Viscosity is a key property of ABHS as it influences factors such as dispensing, pourability, spreadability onto the skin and stickiness. Viscosity also influences drying time, which is an important consideration in user compliance.
The importance of sensory factors on compliance of ABHS has been studied [34]. Key desirable properties that were identified in the study included rapid absorption, a moisturizing hand feel, the absence of stickiness, a clean feel and the absence of or minimal odor. Gels have been reported to have better organoleptic properties than liquid formulations [36].
3.3. Use and Compliance
Proper product use is a critical component of the ABHS tetrahedron because even the best product will not be efficacious if used improperly. Key criteria in proper use of ABHS are the amount of product applied, the application time, the use of the proper technique and the drying time. Furthermore, application and drying times contribute to user acceptability and compliance. Multiple studies recommend that the minimum time required for hand rubbing is 15 s [48,49,50,51]. The benefits of instruction on ABHS use have been demonstrated with one study showing that training of health care workers on the proper technique resulted in improvements in both compliance and the effectiveness of hand sanitization [52,53].
Inadequate directions for use have been observed in many consumer ABHS products [54,55]. It is somewhat puzzling that manufacturers would invest time and resources into designing an efficacious product, yet to pay little attention to the importance of providing adequate directions to how users will apply the product. The need to view the product holistically is emphasized in the perspective of the tetrahedron. Improper use of ABHS will negate the ability of the product to properly disinfect hands. Additionally, the importance of readability and font size should be considered. This is especially a concern for small, portable ABHS bottle sizes.
ABHS users should be directed to apply amounts that are sufficient to wet the entire surface of the hands. Ideally, if the appropriate amounts of an efficacious ABHS are used, the applied product should dry rapidly so that the user can resume other activities. Long drying times, stickiness and residual effects are undesirable and may adversely influence compliance.
A study conducted among medical students demonstrated that reducing the six-step WHO hand hygiene technique to three steps yielded superior bacterial inactivation [52]. This proves that simplifying the hand hygiene procedure can achieve the desired results with improved adherence.
3.4. Safety
The main safety concerns with finished ABHS products at the consumer level are their flammability, ingestion (accidental or intentional) and potential adverse topical effects [56].
3.4.1. Flammability
Alcohols are volatile and flammable organic solvents with flashpoints (lowest temperature at which emitted vapors can ignite) below room temperature. Ethanol-water mixtures at the operational concentrations in ABHS have flashpoints in the range of 17.5–22 °C [57,58].
The flammability risk poses fire hazards to ABHS users if these products are incorrectly used or stored. The ABHS may catch fire in the containers, during application or once applied onto users’ hands thus causing thermal injuries. A case of an individual who suffered burns from exposing hands wet with sanitizer to a flame illustrates this potential risk [59]. It should however, be noted that hazardous fires attributable to ABHS are uncommon. Nonetheless, it is essential to provide appropriate warnings concerning flammability on product labels, dispensers and storage areas.
3.4.2. ABHS Ingestion (Accidental and Intentional)
ABHS, especially in liquid or gel packaged containers present ingestion risks [60]. ABHS products adulterated with methanol are especially concerning due to its higher toxicity. The intentional misuse of ABHS as a substitute for ethanolic beverages has led to serious adverse health consequences and deaths [61]. ABHS products may also be accidentally ingested by children [62]. In the US between 2011 and 2014 more than sixty-five thousand unintentional ABHS exposures in children aged ≤12 years were reported, the majority of which were by ingestion [63]. The FDA has also expressed concern about ABHS products with formulation (e.g., adding food flavors) or packaging (appealing coloring or markings) elements that may make them attractive to children [64].
Recently, the FDA has found methanol in several imported ABHS products in the US market [10]. The spike in demand for ABHS products occasioned by the COVID-19 pandemic, created an opportunity for substandard products to enter the market [65]. One of these products had a methanol concentration of 81% [66]. This highlights the importance of manufacturers ensuring that they have adequate quality controls to prevent adulterated products from reaching the market. In some cases, methanol is used as an ethanol substitute by ABHS manufacturers if it is more readily available or less costly than the permitted alcohols. Tragically, such actions resulted in hundreds of deaths and numerous cases of loss of sight in Iran in 2020 when individuals unknowingly consumed ABHS tainted with methanol [67].
The need for ABHS manufacturers to avoid methanol and methylated spirits containing methanol is critical [68]. Notably, the addition of denaturing agents to ABHS is a critical aspect of reducing the risk of their oral ingestion. Furthermore, stringent regulatory oversight is required to monitor ABHS manufacturers and supply chains [12].
3.4.3. Topical Effects
The tolerability of ABHS is listed as one of the six golden rules of hand hygiene [69]. Even though, the dermal tolerability of an ABHS does not affect efficacy, adverse skin effects will most likely have a negative effect on usage and compliance [70]. Frequent application of skin irritants and allergens can result in contact dermatitis [71]. Generally, ABHS have been considered to have a low incidence of adverse dermal effects except for, in some cases, drying of the skin [72,73,74]. Application of moisturizing creams if ABHS are frequently used has been suggested [75]. Alcohols show a low potential for contact dermatitis although they may cause a burning sensation if they are applied to irritated or damaged skin [76,77]. The incorporation of emollients in an ABHS was reported to reduce contact dermatitis in a controlled, randomized, double-blind trial [78].
Recently, a specific case was reported in which a 12 year-old child developed contact irritant dermatitis following the over-application of a 70% isopropanol-based hand sanitizer [79]. Ethanol has been reported to be capable of causing contact dermatitis, although the causative chemical may be not necessarily be the alcohol but associated impurities or the aldehyde metabolite [80]. The potential of isopropanol to cause contact dermatitis has also been reported [81].
Tocopherol, fragrances, propylene glycol, benzoate, and cetyl stearyl alcohol have been reported as common potential allergens in ABHS used in the United States [82]. Fragrances in particular are a frequent cause of contact allergies in personal care products [83]. While some fragrance compounds may themselves be weak sensitizers, the oxidation of parent compounds may result in the generation of potent allergens [84]. ABHS users with specific allergen sensitivities are advised to review ABHS product ingredient lists and use low-allergen sanitizers [82].
A rise in frequency of hand eczema resulting from increased hand hygiene measures has been reported [85,86,87] although these reports did not indicate whether this was due to increased hand washing or ABHS use. In one reported case, a patient developed palmar erythema due to excessive use of ABHS. The condition resolved soon after the use of the ABHS was reduced [88].
Another related potentially adverse topical effect that has been reported in the literature recently is accidental ocular exposure to ABHS [89,90,91]. It is therefore important that ABHS users be made aware of this risk and use by children be carefully monitored by an adult. Preventative measures for minimizing ocular exposure while using ABHS have been proposed [92].
The high use of ABHS during the COVID-19 pandemic has also been reported to be a possible cause of disulfiram alcohol reactions [93,94]. However, it has been proposed that inadvertent inhalation (especially if ABHS are used in poorly ventilated areas) rather than topical absorption is more likely to result in high enough amounts of alcohol exposure to elicit a disulfiram reaction [95].
4. Model Paradigm
The proposed hand sanitizer model paradigm captures the relationships between ABHS product inputs and outputs. For example, the previously mentioned approaches that have been used by a number of researchers to improve the efficacy of the WHO formulations reveal an interplay between alcohol level and added ingredients (e.g., glycerol) that influences product efficacy. The counteracting influence of humectants on the drying effects of alcohols show how potential adverse effects on the integrity of the skin by ABHS can be mitigated. ABHS delivery formats are a contributing factor to the use of ABHS by individuals who may exhibit preferences for a specific type of product. Delivery systems and sensory characteristics of ABHS play an important role in making these products more attractive to users which is a critical component of compliance. While it may be argued that sensory characteristics do not play a role in efficacy, it is quite clear from the widespread use of fragrances and coloring agents in commercially marketed ABHS products that they do influence customer appeal which indirectly relate to usage and compliance.
The majority of ABHS studies have been performed in hospital environments or controlled settings. The challenge though in the current COVID-19 environment is that ABHS are being widely used by the general public in a multitude of products and delivery formats. With the tremendous increase in ABHS use globally product factors such as ease of use, convenience, portability, user preferences, how well users follow directions for use and safety will become increasingly important. The evaluation of the quality attributes of ABHS products will therefore need to encompass a range of factors that are illustrated in the ABHS tetrahedron paradigm.
5. Conclusions
This review highlights the need for ABHS to be viewed from a multidimensional perspective from the design level as the factors that go into their formulation impact product attributes and performance. It is important to recognize the interplay of these factors in order to ensure ABHS product efficacy and safety. The review also emphasizes the following:
- ABHS are the method recommended by the WHO for ensuring hand hygiene to curb the spread of the COVID-19 pandemic due to superior efficacy and convenience.
- ABHS need to be carefully designed and formulated for the desired quality, efficacy and safety.
- Inactive ingredients used in ABHS may have unexpected effects on product performance.
- Safety features should be designed into ABHS products to minimize risks such as flammability and exposure by ingestion.
Author Contributions
Both authors contributed equally towards the preparation of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pradhan, D.; Biswasroy, P.; Kumar Naik, P.; Ghosh, G.; Rath, G. A Review of Current Interventions for COVID-19 Prevention. Arch. Med. Res. 2020, 51, 363–374. [Google Scholar] [CrossRef]
- Boyce, J.M.; Pittet, D.; Healthcare Infection Control Practices Advisory Committee; Society for Healthcare Epidemiology of America; Association for Professionals in Infection Control; Infectious Diseases Society of America; Hand Hygiene Task Force. Guideline for Hand Hygiene in Health-Care Settings: Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Infect. Control Hosp. Epidemiol. 2002, 23, S3–S40. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (COVID-19) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 12 September 2020).
- WHO. Guide to Local Production: WHO-Recommended Handrub Formulations. 2010. Available online: https://www.who.int/gpsc/5may/Guide_to_Local_Production.pdf (accessed on 12 September 2020).
- Kratzel, A.; Todt, D.; V’kovski, P.; Steiner, S.; Gultom, M.; Thao, T.; Ebert, N.; Holwerda, M.; Steinmann, J.; Niemeyer, D.; et al. Inactivation of Severe Acute Respiratory Syndrome Coronavirus 2 by WHO-Recommended Hand Rub Formulations and Alcohols. Emerg. Infect. Dis. 2020, 26, 1592–1595. [Google Scholar] [CrossRef]
- McDonnell, G.; Russell, A.D. Antiseptics and disinfectants: Activity, action, and resistance. Clin. Microbiol. Rev. 1999, 12, 147–179. [Google Scholar] [CrossRef] [Green Version]
- Daverey, A.; Dutta, K. COVID-19: Eco-Friendly Hand Hygiene for Human and Environmental Safety. J. Environ. Chem. Eng. 2020, 9, 104754. [Google Scholar] [CrossRef]
- Singh, D.; Joshi, K.; Samuel, A.; Patra, J.; Mahindroo, N. Alcohol-Based Hand Sanitisers as First Line of Defence against SARS-CoV-2: A Review of Biology, Chemistry and Formulations. Epidemiol. Infect. 2020, 148, e229. [Google Scholar] [CrossRef]
- FDA. Temporary Policy for Preparation of Certain Alcohol-Based Hand Sanitizer Products During the Public Health Emergency (COVID-19) Guidance for Industry. Available online: https://www.fda.gov/drugs/coronavirus-covid-19-drugs/hand-sanitizers-covid-19 (accessed on 12 September 2020).
- FDA. FDA Updates on Hand Sanitizers Consumers Should Not Use. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-updates-hand-sanitizers-consumers-should-not-use (accessed on 12 September 2020).
- Berardi, A.; Perinelli, D.R.; Merchant, H.A.; Bisharat, L.; Basheti, I.A.; Bonacucina, G.; Cespi, M.; Palmieri, G.F. Hand Sanitisers amid CoViD-19: A Critical Review of Alcohol-Based Products on the Market and Formulation Approaches to Respond to Increasing Demand. Int. J. Pharm. 2020, 584, 119431. [Google Scholar] [CrossRef] [PubMed]
- Jairoun, A.A.; Al-Hemyari, S.S.; Shahwan, M. The Pandemic of COVID-19 and Its Implications for the Purity and Authenticity of Alcohol-Based Hand Sanitizers: The Health Risks Associated with Falsified Sanitizers and Recommendations for Regulatory and Public Health Bodies. Res. Soc. Admin. Pharm. 2021, 17, 2050–2051. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, F.S., Jr.; e Brito, L.R.; Pimentel, M.F.; Leal, L.B. Determination of Ethanol in Gel Hand Sanitizers Using Mid and Near Infrared Spectroscopy. J. Braz. Chem. Soc. 2020, 31, 1759–1763. [Google Scholar] [CrossRef]
- Nalawade, T.M.; Bhat, K.; Sogi, S.H. Bactericidal Activity of Propylene Glycol, Glycerine, Polyethylene Glycol 400, and Polyethylene Glycol 1000 against Selected Microorganisms. J. Int. Soc. Prev. Community Dent. 2015, 5, 114–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suchomel, M.; Kundi, M.; Pittet, D.; Rotter, M.L. Modified World Health Organization Hand Rub Formulations Comply with European Efficacy Requirements for Preoperative Surgical Hand Preparations. Infect. Control Hosp. Epidemiol. 2013, 34, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Suchomel, M.; Rotter, M.; Weinlich, M.; Kundi, M. Glycerol Significantly Decreases the Three Hour Efficacy of Alcohol-Based Surgical Hand Rubs. J. Hosp. Infect. 2013, 83, 284–287. [Google Scholar] [CrossRef]
- Thaddeus, N.I.; Francis, E.C.; Jane, O.O.; Obumneme, A.C.; Okechukwu, E.C. Effects of Some Common Additives on the Antimicrobial Activities of Alcohol-Based Hand Sanitizers. Asian Pac. J. Trop. Med. 2018, 11, 222–226. [Google Scholar] [CrossRef]
- Menegueti, M.G.; Laus, A.M.; Ciol, M.A.; Auxiliadora-Martins, M.; Basile-Filho, A.; Gir, E.; Pires, D.; Pittet, D.; Bellissimo-Rodrigues, F. Glycerol Content within the WHO Ethanol-Based Handrub Formulation: Balancing Tolerability with Antimicrobial Efficacy. Antimicrob. Resist. Infect. Control 2019, 8, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macinga, D.R.; Sattar, S.A.; Jaykus, L.A.; Arbogast, J.W. Improved Inactivation of Nonenveloped Enteric Viruses and Their Surrogates by a Novel Alcohol-Based Hand Sanitizer. Appl. Environ. Microbiol. 2008, 74, 5047–5052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, R.B.; Fuls, J.L.; Rodgers, N.D. Effectiveness of Hand Sanitizers with and without Organic Acids for Removal of Rhinovirus from Hands. Antimicrob. Agents Chemother. 2010, 54, 1363–1364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ionidis, G.; Hübscher, J.; Jack, T.; Becker, B.; Bischoff, B.; Todt, D.; Hodasa, V.; Brill, F.H.; Steinmann, E.; Steinmann, J. Development and Virucidal Activity of a Novel Alcohol-Based Hand Disinfectant Supplemented with Urea and Citric Acid. BMC Infect. Dis. 2016, 16, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kampf, G. Efficacy of Ethanol against Viruses in Hand Disinfection. J. Hosp. Infect. 2018, 98, 331–338. [Google Scholar] [CrossRef]
- Golin, A.P.; Choi, D.; Ghahary, A. Hand Sanitizers: A Review of Ingredients, Mechanisms of Action, Modes of Delivery, and Efficacy against Coronaviruses. Am. J. Infect. Control 2020, 48, 1062–1067. [Google Scholar] [CrossRef]
- Bondurant, S.W.; Duley, C.M.; Harbell, J.W. Demonstrating the Persistent Antibacterial Efficacy of a Hand Sanitizer Containing Benzalkonium Chloride on Human Skin at 1, 2, and 4 Hours after Application. Am. J. Infect. Control 2019, 47, 928–932. [Google Scholar] [CrossRef] [Green Version]
- Olson, L.K.; Morse, D.J.; Duley, C.; Savell, B.K. Prospective, Randomized in Vivo Comparison of a Dual-Active Waterless Antiseptic versus Two Alcohol-Only Waterless Antiseptics for Surgical Hand Antisepsis. Am. J. Infect. Control 2012, 40, 155–159. [Google Scholar] [CrossRef]
- Deshpande, A.; Fox, J.; Wong, K.K.; Cadnum, J.L.; Sankar, T.; Jencson, A.; Schramm, S.; Fraser, T.G.; Donskey, C.J.; Gordon, S. Comparative Antimicrobial Efficacy of Two Hand Sanitizers in Intensive Care Units Common Areas: A Randomized, Controlled Trial. Infect. Control Hosp. Epidemiol. 2018, 39, 267–271. [Google Scholar] [CrossRef]
- Macinga, D.R.; Edmonds, S.L.; Campbell, E.; McCormack, R.R. Comparative Efficacy of Alcohol-Based Surgical Scrubs: The Importance of Formulation. AORN J. 2014, 100, 641–650. [Google Scholar] [CrossRef]
- Hennig, T.J.; Werner, S.; Naujox, K.; Arndt, A. Chlorhexidine Is Not an Essential Component in Alcohol-Based Surgical Hand Preparation: A Comparative Study of Two Handrubs Based on a Modified EN 12791 Test Protocol. Antimicrob. Resist. Infect. Control 2017, 6, 96. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, N.; Klein, D.; Karanja, P.; Greten, Z.; Newman, J. Inactivation of Chlorhexidine Gluconate on Skin by Incompatible Alcohol Hand Sanitizing Gels. Am. J. Infect. Control 2009, 37, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Jing, J.; Pei Yi, T.; Bose, R.; McCarthy, J.R.; Tharmalingam, N.; Madheswaran, T. Hand Sanitizers: A Review on Formulation Aspects, Adverse Effects, and Regulations. Int. J. Environ. Res. Public Health 2020, 17, 3326. [Google Scholar] [CrossRef] [PubMed]
- Lubrizol. Stability of Pharmaceutical Carbopol® Polymer Gels Containing Hydrogen Peroxide. Technical Data Sheet 2007. Available online: https://www.google.co.ke/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwj12dnloKrvAhUZO-wKHaE4BkcQFjAAegQIARAD&url=https%3A%2F%2Fwww.lubrizol.com%2F-%2Fmedia%2FLubrizol%2FLife-Sciences%2FDocuments%2FTDS%2FTDS-361_Stability_Pharm_Carbopol_Gels_Containing_Hydrogen_Peroxide.pdf&usg=AOvVaw3ty5UExf1NYBBnpan38-Jw (accessed on 12 September 2020).
- Eiref, S.D.; Leitman, I.M.; Riley, W. Hand Sanitizer Dispensers and Associated Hospital-Acquired Infections: Friend or Fomite? Surg. Infect. 2012, 13, 137–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hongsoongnern, P.; Britton, A.; Shah, V.; Kachur, R.; Nicksic, J.; Handley, A. Reduced Germ Exposure from Changing out Manual Soap and Sanitizer Dispensers to Touchless Closed System Dispensers. Am. J. Infect. Control 2016, 44. [Google Scholar] [CrossRef]
- Greenaway, R.E.; Ormandy, K.; Fellows, C.; Hollowood, T. Impact of Hand Sanitizer Format (Gel/Foam/Liquid) and Dose Amount on Its Sensory Properties and Acceptability for Improving Hand Hygiene Compliance. J. Hosp. Infect. 2018, 100, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.; Rudolph, P.; Kampf, G.; Pittet, D. Limited Efficacy of Alcohol-Based Hand Gels. Lancet 2002, 359, 1489–1490. [Google Scholar] [CrossRef]
- Ochwoto, M.; Muita, L.; Talaam, K.; Wanjala, C.; Ogeto, F.; Wachira, F.; Osman, S.; Kimotho, J.; Ndegwa, L. Anti-Bacterial Efficacy of Alcoholic Hand Rubs in the Kenyan Market, 2015. Antimicrob. Resist. Infect. Control 2017, 6, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larson, E.L.; Cohen, B.; Baxter, K.A. Analysis of Alcohol-Based Hand Sanitizer Delivery Systems: Efficacy of Foam, Gel, and Wipes against Influenza A (H1N1) Virus on Hands. Am. J. Infect. Control 2012, 40, 806–809. [Google Scholar] [CrossRef] [PubMed]
- Rai, H.; Knighton, S.; Zabarsky, T.F.; Donskey, C.J. Comparison of Ethanol Hand Sanitizer versus Moist Towelette Packets for Mealtime Patient Hand Hygiene. Am. J. Infect. Control 2017, 45, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Dicken, R.D.; Gallagher, T.; Perks, S. Overcoming the Regulatory Hurdles for the Production of Hand Sanitizer for Public Health Protection: The UK and US Academic Perspective. J. Chem. Saf. 2020, 27, 209–213. [Google Scholar] [CrossRef]
- ECHA. Information on Biocides. Available online: https://echa.europa.eu/information-on-chemicals/biocidal-products (accessed on 12 September 2020).
- FDA. Topical Antiseptic Products: Hand Sanitizers and Antibacterial Soaps. Available online: https://www.fda.gov/drugs/information-drug-class/topical-antiseptic-products-hand-sanitizers-and-antibacterial-soaps (accessed on 12 September 2020).
- Thomson, E.L.; Bullied, A.R. Production of Ethanol-Based Hand Sanitizer in Breweries during the COVID-19 Crisis. Tech. Q. Master Brew. Assoc. Am. 2020, 57, 47–52. [Google Scholar] [CrossRef]
- Thomson, E.L.; Bullied, A.R. Corrosion Resistance of Aluminum Beer Cans Containing Hand Sanitizer. J. Am. Soc. Brew. Chem. 2020, 78, 279–283. [Google Scholar] [CrossRef]
- Kohan, C.; Ligi, C.; Dumigan, D.G.; Boyce, J.M. The Importance of Evaluating Product Dispensers When Selecting Alcohol-Based Handrubs. Am. J. Infect. Control 2002, 30, 373–375. [Google Scholar] [CrossRef]
- Bánsághi, S.; Soule, H.; Guitart, C.; Pittet, D.; Haidegger, T. Critical Reliability Issues of Common Type Alcohol-Based Handrub Dispensers. Antimicrob. Resist. Infect. Control 2020, 9, 90. [Google Scholar] [CrossRef]
- Rotter, M.; Sattar, S.; Dharan, S.; Allegranzi, B.; Mathai, E.; Pittet, D. Methods to Evaluate the Microbicidal Activities of Hand-Rub and Hand-Wash Agents. J. Hosp. Infect. 2009, 73, 191–199. [Google Scholar] [CrossRef]
- Suchomel, M.; Eggers, M.; Maier, S.; Kramer, A.; Dancer, S.J.; Pittet, D. Evaluation of World Health Organization-Recommended Hand Hygiene Formulations. Emerg. Infect. Dis. 2020, 26, 2064–2068. [Google Scholar] [CrossRef]
- Voss, A.; Widmer, A.F. No Time for Handwashing!? Handwashing versus Alcoholic Rub: Can We Afford 100% Compliance? Infect. Control Hosp. Epidemiol. 1997, 18, 205–208. [Google Scholar] [CrossRef]
- Wilkinson, M.; Ormandy, K.; Bradley, C.R.; Fraise, A.P.; Hines, J. Dose Considerations for Alcohol-Based Hand Rubs. J. Hosp. Infect. 2017, 95, 175–182. [Google Scholar] [CrossRef]
- Kramer, A.; Pittet, D.; Klasinc, R.; Krebs, S.; Koburger, T.; Fusch, C.; Assadian, O. Shortening the Application Time of Alcohol-Based Hand Rubs to 15 Seconds May Improve the Frequency of Hand Antisepsis Actions in a Neonatal Intensive Care Unit. Infect. Control Hosp. Epidemiol. 2017, 38, 1430–1434. [Google Scholar] [CrossRef]
- Harnoss, J.C.; Dancer, S.J.; Kaden, C.F.; Baguhl, R.; Kohlmann, T.; Papke, R.; Zygmunt, M.; Assadian, O.; Suchomel, M.; Pittet, D.; et al. Hand Antisepsis without Decreasing Efficacy by Shortening the Rub-in Time of Alcohol-Based Handrubs to 15 Seconds. J. Hosp. Infect. 2020, 104, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Sutter, S.T.; Frei, R.; Dangel, M.; Widmer, A.F. Effect of Teaching Recommended World Health Organization Technique on the Use of Alcohol-Based Hand Rub by Medical Students. Infect. Control Hosp. Epidemiol. 2010, 31, 1194–1195. [Google Scholar] [CrossRef] [Green Version]
- Widmer, A.F.; Conzelmann, M.; Tomic, M.; Frei, R.; Stranden, A.M. Introducing Alcohol-Based Hand Rub for Hand Hygiene: The Critical Need for Training. Infect. Control Hosp. Epidemiol. 2007, 28, 50–54. [Google Scholar] [CrossRef]
- Nyamweya, N.N.; Abuga, K.O. A Survey of Alcohol-Based Hand Sanitizers in Nairobi: Packaging, Labelling and Regulatory Compliance. East Cent. Afr. J. Pharm. Sci. 2020, 23, 72–76. [Google Scholar]
- Abuga, K.; Nyamweya, N. Are Alcohol-Based Hand Sanitizers (Rubs) Being Used Properly? Available online: https://uonresearch.org/blog/are-alcohol-based-hand-sanitizers-rubs-being-used-properly/ (accessed on 29 January 2021).
- Atolani, O.; Baker, M.T.; Adeyemi, O.S.; Olanrewaju, I.R.; Hamid, A.A.; Ameen, O.M.; Oguntoye, S.O.; Usman, L.A. COVID-19: Critical discussion on the applications and implications of chemicals in sanitizers and disinfectants. EXCLI J. 2020, 19, 785–799. [Google Scholar] [CrossRef] [PubMed]
- Astbury, G.R.; Bugand-Bugandet, J.; Grollet, E.S.; Stell, K.M. Flash points of aqueous solutions of flammable solvents. Inst. Chem. Eng. Symp. Ser. 2004, 150, 1–18. [Google Scholar]
- Janès, A.; Chaineaux, J. Experimental determination of flash points of flammable liquid aqueous solutions. Chem. Eng. Trans. 2013, 31, 943–948. [Google Scholar] [CrossRef]
- O’Leary, F.M.; Price, G.J. Alcohol Hand Gel–a Potential Fire Hazard. J. Plast. Reconstr. Aesthet. Surg. 2011, 64, 131–132. [Google Scholar] [CrossRef]
- Gormley, N.J.; Bronstein, A.C.; Rasimas, J.J.; Pao, M.; Wratney, A.T.; Sun, J.; Austin, H.A.; Suffredini, A.F. The Rising Incidence of Intentional Ingestion of Ethanol-Containing Hand Sanitizers. Crit. Care Med. 2012, 40, 290–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yip, L.; Bixler, D.; Brooks, D.E.; Clarke, K.R.; Datta, S.D.; Dudley, S., Jr.; Komatsu, K.K.; Lind, J.N.; Mayette, A.; Melgar, M.; et al. Serious Adverse Health Events, Including Death, Associated with Ingesting Alcohol-Based Hand Sanitizers Containing Methanol—Arizona and New Mexico, May-June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1070–1073. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, A.; Eqan, M.; Pervez, S.; Alghamdi, H.A.; Tabinda, A.B.; Yasar, A.; Brindhadevi, K.; Pugazhendhi, A. COVID-19 and frequent use of hand sanitizers; human health and environmental hazards by exposure pathways. Sci. Total Environ. 2020, 742, 140561. [Google Scholar] [CrossRef] [PubMed]
- Santos, C.; Kieszak, S.; Wang, A.; Law, R.; Schier, J.; Wolkin, A. Reported Adverse Health Effects in Children from Ingestion of Alcohol-Based Hand Sanitizers—United States, 2011–2014. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 223–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FDA. COVID-19 Update: FDA Warns Consumers About Hand Sanitizer Packaged in Food and Drink Containers | FDA. Available online: https://www.fda.gov/news-events/press-announcements/covid-19-update-fda-warns-consumers-about-hand-sanitizer-packaged-food-and-drink-containers (accessed on 19 September 2020).
- Hasen, G.; Suleman, S. Regulatory Authorities’ Preparedness to Avert Poor Quality Alcohol Based Hand Sanitizers during COVID-19 Pandemic in Ethiopia: A Commentary. PPIJ 2020, 8, 322–323. [Google Scholar] [CrossRef]
- FDA. FDA Advises Consumers Not to Use Hand Sanitizer Products Manufactured by Eskbiochem. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-advises-consumers-not-use-hand-sanitizer-products-manufactured-eskbiochem (accessed on 12 September 2020).
- Delirrad, M.; Mohammadi, A.B. New Methanol Poisoning Outbreaks in Iran Following Covid-19 Pandemic. Alcohol Alcohol. 2020, 55, 347–348. [Google Scholar] [CrossRef]
- Dear, K.; Grayson, L.; Nixon, R. Potential Methanol Toxicity and the Importance of Using a Standardised Alcohol-Based Hand Rub Formulation in the Era of COVID-19. Antimicrob. Resist. Infect. Control 2020, 9, 129. [Google Scholar] [CrossRef]
- Kampf, G. The Six Golden Rules to Improve Compliance in Hand Hygiene. J. Hosp. Infect. 2004, 56 (Suppl. S2), 3–5. [Google Scholar] [CrossRef]
- Assefa, D.; Melaku, T.; Bayisa, B.; Alemu, S. Knowledge, Attitude and Self-Reported Performance and Challenges of Hand Hygiene Using Alcohol-Based Hand Sanitizers Among Healthcare Workers During COVID-19 Pandemic at a Tertiary Hospital: A Cross-Sectional Study. IDR 2021, 14, 303–313. [Google Scholar] [CrossRef]
- Jakasa, I.; Thyssen, J.P.; Kezic, S. The Role of Skin Barrier in Occupational Contact Dermatitis. Exp. Dermatol. 2018, 27, 909–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widmer, A.F. Replace Hand Washing with Use of a Waterless Alcohol Hand Rub? Clin. Infect. Dis. 2000, 31, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Graham, M.; Nixon, R.; Burrell, L.J.; Bolger, C.; Johnson, P.D.; Grayson, M.L. Low Rates of Cutaneous Adverse Reactions to Alcohol-Based Hand Hygiene Solution during Prolonged Use in a Large Teaching Hospital. Antimicrob. Agents Chemother. 2005, 49, 4404–4405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larson, E.; Girard, R.; Pessoa-Silva, C.L.; Boyce, J.; Donaldson, L.; Pittet, D. Skin Reactions Related to Hand Hygiene and Selection of Hand Hygiene Products. Am. J. Infect. Control 2006, 34, 627–635. [Google Scholar] [CrossRef] [PubMed]
- Rundle, C.W.; Presley, C.L.; Militello, M.; Barber, C.; Powell, D.L.; Jacob, S.E.; Atwater, A.R.; Watsky, K.L.; Yu, J.; Dunnick, C.A. Hand Hygiene during COVID-19. Recommendations from the American Contact Dermatitis Society. J. Am. Acad. Dermatol. 2020, 83, 1730–1737. [Google Scholar] [CrossRef]
- Kampf, G.; Löffler, H. Prevention of Irritant Contact Dermatitis among Health Care Workers by Using Evidence-Based Hand Hygiene Practices: A Review. Ind. Health 2007, 45, 645–652. [Google Scholar] [CrossRef] [Green Version]
- Löffler, H.; Kampf, G. Hand Disinfection: How Irritant Are Alcohols? J. Hosp. Infect. 2008, 70 (Suppl. S1), 44–48. [Google Scholar] [CrossRef]
- Kampf, G.; Wigger-Alberti, W.; Schoder, V.; Wilhelm, K.P. Emollients in a Propanol-Based Hand Rub Can Significantly Decrease Irritant Contact Dermatitis. Contact Dermatol. 2005, 53, 344–349. [Google Scholar] [CrossRef]
- Inder, D.; Kumar, P. Isopropyl alcohol (70%)-based hand sanitizer-induced contact dermatitis: A case report amid Covid-19. Indian J. Case Rep. 2020, 6, 403–405. [Google Scholar] [CrossRef]
- Ophaswongse, S.; Maibach, H.I. Alcohol Dermatitis: Allergic Contact Dermatitis and Contact Urticaria Syndrome. A Review. Contact Dermatol. 1994, 30, 1–6. [Google Scholar] [CrossRef]
- García-Gavín, J.; Lissens, R.; Timmermans, A.; Goossens, A. Allergic Contact Dermatitis Caused by Isopropyl Alcohol: A Missed Allergen? Contact Dermatol. 2011, 65, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Voller, L.M.; Schlarbaum, J.P.; Hylwa, S.A. Allergenic Ingredients in Health Care Hand Sanitizers in the United States. Dermatitis 2020. [Google Scholar] [CrossRef]
- Johansen, J.D. Fragrance Contact Allergy: A Clinical Review. Am. J. Clin. Dermatol. 2003, 4, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Bråred Christensson, J.; Hagvall, L.; Karlberg, A.-T. Fragrance Allergens, Overview with a Focus on Recent Developments and Understanding of Abiotic and Biotic Activation. Cosmetics 2016, 3, 19. [Google Scholar] [CrossRef]
- Guertler, A.; Moellhoff, N.; Schenck, T.L.; Hagen, C.S.; Kendziora, B.; Giunta, R.E.; French, L.E.; Reinholz, M. Onset of Occupational Hand Eczema among Healthcare Workers during the SARS-CoV-2 Pandemic: Comparing a Single Surgical Site with a COVID-19 Intensive Care Unit. Contact Dermatol. 2020, 83, 108–114. [Google Scholar] [CrossRef]
- Giacalone, S.; Bortoluzzi, P.; Nazzaro, G. The Fear of COVID-19 Infection Is the Main Cause of the New Diagnoses of Hand Eczema: Report from the Frontline in Milan. Dermatology 2020, 33, e13630. [Google Scholar] [CrossRef]
- Singh, M.; Pawar, M.; Bothra, A.; Choudhary, N. Overzealous Hand Hygiene during the COVID 19 Pandemic Causing an Increased Incidence of Hand Eczema among General Population. J. Am. Acad. Dermatol. 2020, 83, e37–e41. [Google Scholar] [CrossRef]
- Panda, P.K.; Sharawat, I.K. Fluctuating Palmar Erythema in a Toddler during COVID-19 Pandemic: Do You Know the Offender? J. Trop. Pediatr. 2021, 67, fmab011. [Google Scholar] [CrossRef] [PubMed]
- Sunny, C.L.K. Hand Sanitizer Associated Ocular Chemical Injury: A Mini-Review on Its Rise under COVID-19. Vis. J. Emerg. Med. 2020, 21, 100881. [Google Scholar] [CrossRef]
- Yangzes, S.; Grewal, S.; Gailson, T.; Grewal, S.P.S. Hand Sanitizer–Induced Ocular Injury: A COVID-19 Hazard in Children. JAMA Ophthalmol. 2021. [Google Scholar] [CrossRef]
- Martin, G.C.; Le Roux, G.; Guindolet, D.; Boulanger, E.; Hasle, D.; Morin, E.; Vodovar, D.; Vignal, C.; Gabison, E.; Descatha, A.; et al. Pediatric Eye Injuries by Hydroalcoholic Gel in the Context of the Coronavirus Disease 2019 Pandemic. JAMA Ophthalmol. 2021. [Google Scholar] [CrossRef]
- Shetty, R.; Jayadev, C.; Chabra, A.; Maheshwari, S.; D’Souza, S.; Khamar, P.; Sethu, S.; Honavar, S. Sanitizer Aerosol-Driven Ocular Surface Disease (SADOSD)—A COVID-19 Repercussion? Indian J. Ophthalmol. 2020, 68, 981. [Google Scholar] [CrossRef] [PubMed]
- De Sousa, A. Disulfiram Ethanol Reaction in a Patient Abstinent from Alcohol Caused by Hand Sanitizing. Alcohol Alcohol. 2020, 55, 349. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.; Mahintamani, T.; Balhara, Y.P.S.; Roub, F.E.; Basu, D.; Bn, S.; Mattoo, S.K.; Mishra, E.; Sharma, B. Disulfiram Ethanol Reaction with Alcohol-Based Hand Sanitizer: An Exploratory Study. Alcohol Alcohol. 2021, 56, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Brewer, C.; Streel, E. Is Alcohol in Hand Sanitizers Absorbed Through the Skin or Lungs? Implications for Disulfiram Treatment. Alcohol Alcohol. 2020, 55, 354–356. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The alcohol-based hand sanitizers (ABHS) tetrahedron of manufacturing inputs and performance factors. Factors represented by the hidden faces and vertex are shown in blue font. Abbreviation: cGMP—current good manufacturing practices.
Figure 1.
The alcohol-based hand sanitizers (ABHS) tetrahedron of manufacturing inputs and performance factors. Factors represented by the hidden faces and vertex are shown in blue font. Abbreviation: cGMP—current good manufacturing practices.


{kind=link}
Table 1.
Ingredients commonly used in commercial ABHS products.
| Ingredient | Functions | Examples † |
|---|---|---|
| Active (alcohol) | Inactivate susceptible microorganisms | Ethanol, Isopropanol, n-propanol ‡ |
| Solvent/Cosolvent | Facilitate alcohol protein denaturation Reduce product volatility | Water |
| Humectant | Facilitate skin hydration | Glycerol, Propylene glycol |
| Emollient | Maintain skin softness, smoothness, pliability | Caprylyl glycol, Isopropyl myristate |
| Thickener | Increase viscosity, facilitate handling; reduce spillage/runoff | Carbomer, Acrylates/C10-30 alkyl acrylate cross polymer |
| pH adjusting agent | Neutralization of acrylic acid-based polymers to enhance viscosity | Aminomethyl propanol, Triethanolamine |
| Fragrance | Enhance aesthetic appeal, ameliorate/mask alcohol odor | Linalool, Limonene |
| Others: Antioxidant Multifunctional | Ameliorate adverse effects of alcohols on the skin | Tocopheryl acetate Aloe vera |
† Some ingredients may have more than one or overlapping functions. ‡ n-propanol is not approved for use in the USA.
Table 2.
ABHS Delivery Formats.
| Formulation | Delivery System | Advantages | Disadvantages |
|---|---|---|---|
| Liquid (low viscosity solutions) | Pouring/squeezing from bottles Pumping from containers Dispensers | Portable Widely available | Spillage, dose metering Alcohol odor may be more pronounced |
| Gel | Pouring/squeezing from bottles Pumping from containers Dispensers | As for liquids, but with better dose metering, handling characteristics | Spillage, antimicrobial action may not be as rapid as that of liquids Longer drying time than liquids |
| Foams | Dispensers Special containers | As for gels, but with reduced spillage May be preferred by some consumers | More expensive than liquids or gels |
| Dispensers | Mechanical (lever) Touchless (sensor) | Controlled dose metering for liquids, gels and foams | Device malfunctioning will prevent dosing Potential fomite risks [32,33] |
| Sprays | Actuation of a valve | Controlled dose metering | Product losses to atmosphere Potential for inhalation Higher flammability risk if incorrectly used |
| Wipes | ABHS is transferred from wipe to surface of the skin | Dose metering Portable, convenient, no spillage | Needs to be designed to provide sufficient amount of ABHS in each wipe Non-biodegradable fabrics |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Abuga, K.; Nyamweya, N. Alcohol-Based Hand Sanitizers in COVID-19 Prevention: A Multidimensional Perspective. Pharmacy 2021, 9, 64. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy9010064
AMA Style
Abuga K, Nyamweya N. Alcohol-Based Hand Sanitizers in COVID-19 Prevention: A Multidimensional Perspective. Pharmacy. 2021; 9(1):64. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy9010064
Chicago/Turabian StyleAbuga, Kennedy, and Nasser Nyamweya. 2021. "Alcohol-Based Hand Sanitizers in COVID-19 Prevention: A Multidimensional Perspective" Pharmacy 9, no. 1: 64. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy9010064
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.