Snoring and Sleep-Related Symptoms: A Novel Non-Invasive 808 nm Wavelength Diode Laser Non-Ablative Outpatient Treatment. A Prospective Pilot-Study on 45 Patients


 ,
,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Compliance with Ethical Standards and Study Population
2.3. Laser Treatment Description (The Fini Storchi–Unige Protocol)
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Overall Population
3.2. Laser Treatments Results
3.3. Subgroup Analysis
3.4. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ellenbogen, J.M. Cognitive benefits of sleep and their loss due to sleep deprivation. Neurology 2005, 64, E25–E27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valentino, D.J., III; O’Donnell, A.E. Reasons and referrals for sleep medicine consultation in obstructive sleep apnea. Chest 2006, 130, 264S. [Google Scholar] [CrossRef]
- Zamarrón, C.; Valdés Cuadrado, L.; Alvarez-Sala, R. Pathophysiologic mechanisms of cardiovascular disease in obstructive sleep apnea syndrome. Pulm. Med. 2013, 2013, 521087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Ma, Y.; Ouyang, R.; Zeng, Z.; Zhan, Z.; Lu, H.; Cui, Y.; Dai, Z.; Luo, L.; He, C.; et al. The relationship between inflammation and neurocognitive dysfunction in obstructive sleep apnea syndrome. J. Neuroinflamm. 2020, 17, 229. [Google Scholar] [CrossRef]
- Gałecki, P.; Florkowski, A.; Zboralski, K.; Pietras, T.; Szemraj, J.; Talarowska, M. Psychiatric and psychological complications in obstructive sleep apnea syndrome. Pneumonol. Alergol. Pol. 2011, 79, 26–31. [Google Scholar]
- Mannarino, M.R.; di Filippo, F.; Pirro, M. Obstructive sleep apnea syndrome. Eur. J. Intern. Med. 2012, 23, 586–593. [Google Scholar] [CrossRef]
- Di Carlo, G.; Zara, F.; Rocchetti, M.; Venturini, A.; Ortiz-Ruiz, A.J.; Luzzi, V.; Cattaneo, P.M.; Polimeni, A.; Vozza, I. Prevalence of sleep-disordered breathing in children referring for first dental examination. A multicenter cross-sectional study using pediatric sleep questionnaire. Int. J. Environ. Res. Public Health 2020, 17, 8460. [Google Scholar]
- Li, Z.; Celestin, J.; Lockey, R.F. Pediatric Sleep Apnea Syndrome: An Update. J. Allergy Clin. Immunol. Pract. 2016, 4, 852–861. [Google Scholar] [CrossRef]
- Garvey, J.F.; Pengo, M.F.; Drakatos, P.; Kent, B.D. Epidemiological aspects of obstructive sleep apnea. J. Thorac. Dis. 2015, 7, 920–929. [Google Scholar]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Stigter, H.; Lammers, G.J.; Rooyackers, J.M. Werkgroep Rijgeschiktheid. Sleep disorders and the ability to drive, revision of legislation. Ned. Tijdschr. Geneeskd. 2009, 153, A690. [Google Scholar]
- Stuck, B.A.; Dreher, A.; Heiser, C.; Herzog, M.; Kuhnel, T.; Maurer, J.T.; Pistner, H.; Sitter, H.; Steffen, A.; Verse, T. Diagnosis and treatment of snoring in adults-S2k Guideline of the German Society of Otorhinolaryngology, Head and Neck Surgery. Sleep Breath. 2015, 19, 135–148. [Google Scholar] [CrossRef]
- Sanches, I.; Martins, V.; dos Santos, J.M. Obstructive sleep apnea refractory to treatment due to floppy epiglottis. Arch Bronconeumol 2015, 51, 94. [Google Scholar] [CrossRef] [PubMed]
- Server, E.A.; Alkan, Z.; Yiğit, Ö.; Yasak, A.G. Long-term results of pillar implant procedure. Kulak Burun Bogaz Ihtis Derg 2016, 26, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Olszewska, E.; Panek, J.; O’Day, J.; Rogowski, M. Usefulness of snoreplasty in the treatment of simple snoring and mild obstructive sleep apnea/hypopnea syndrome—Preliminary report. Otolaryngol. Pol. 2014, 68, 184–188. [Google Scholar] [CrossRef]
- Chiesa Estomba, C.M.; Rivera Schmitz, T.; Ossa Echeverri, C.C.; Betances Reinoso, F.A.; Fariña Conde, J.; Alonso Parraga, D. The treatment of snoring by radiofrequency-assisted uvulopalatoplasty and results after one-session protocol: A prospective, longitudinal, non-randomized study. Eur. Arch Otorhinolaryngol. 2015, 272, 3059–3063. [Google Scholar] [CrossRef]
- Pazos, G.; Mair, E.A. Complications of radiofrequency ablation in the treatment of sleep-disordered breathing. Otolaryngol. Head Neck Surg. 2001, 125, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Mezzofranco, L.; Luigi, A.; Gracco, T.; Milano, F.; Di-Bernardo, G.A.; Vezzali, L.; Giovannini, D. Personality traits and oral device: A new challenge to increase compliance with MAD therapy for OSAS and snoring. Sleep Sci. 2020, 13, 10–17. [Google Scholar]
- Li, S.; Wu, D.; Shi, H. Reoperation on patients with obstructive sleep apnea-hypopnea syndrome after failed uvulopalatopharyngoplasty. Eur. Arch Otorhinolaryngol. 2015, 272, 407–412. [Google Scholar] [CrossRef]
- Rombaux, P.; Hamoir, M.; Bertrand, B.; Aubert, G.; Liistro, G.; Rodenstein, D. Postoperative pain and side effects after uvulopalatopharyngoplasty, laser-assisted uvulopalatoplasty, and radiofrequency tissue volume reduction in primary snoring. Laryngoscope 2003, 113, 2169–2173. [Google Scholar] [CrossRef]
- Tang, J.A.; Salapatas, A.M.; Bonzelaar, L.B.; Friedman, M. Long-Term Incidence of Velopharyngeal Insufficiency and Other Sequelae following Uvulopalatopharyngoplasty. Otolaryngol. Head Neck Surg. 2017, 156, 606–610. [Google Scholar] [CrossRef] [PubMed]
- Nishigawa, K.; Hayama, R.; Matsuka, Y. Complications causing patients to discontinue using oral appliances for treatment of obstructive sleep apnea. J. Prosthodont Res. 2017, 61, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Fini Storchi, I.; Parker, S.; Bovis, F.; Benedicenti, S.; Amaroli, A. Outpatient erbium: YAG (2940 nm) laser treatment for snoring: A prospective study on 40 patients. Lasers Med. Sci. 2018, 33, 399–406. [Google Scholar] [CrossRef]
- Cetinkaya, E.A.; Turker, M.; Kiraz, K.; Gulkesen, H.K. Er: YAG laser treatment of simple snorers in an outpatient setting. ORL J. Otorhinolaryngol. Relat. Spec. 2016, 78, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Mure, C.; Blumen, M.; Alali, A.; Page, L.; Chabolle, F. Surgical ablation of lingual tonsils in the treatment of obstructive sleep apnea. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 136, 19–23. [Google Scholar] [CrossRef]
- Pavelec, V.; Bohmanova, J. A comparison of postoperative recovery from laser-assisted uvulopalatoplasty using different laser systems. Otolaryngol. Head Neck Surg. 2008, 138, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Sher, A.E.; Thorpy, M.J.; Shprintzen, R.J.; Spielman, A.J.; Burack, B.; McGregor, P.A. Predictive value of Muller maneuver in selection of patients for uvulopalatopharyngoplasty. Laryngoscope 1985, 95, 1483–1487. [Google Scholar] [CrossRef]
- Vicini, C.; de Vito, A.; Benazzo, M.; Frassineti, S.; Campanini, A.; Frasconi, P.; Mira, E. The nose oropharynx hypopharynx and larynx (NOHL) classification: A new system of diagnostic standardized examination for OSAHS patients. Eur. Arch Otorhinolaryngol. 2012, 269, 1297–1300. [Google Scholar] [CrossRef]
- Belafsky, P.C.; Postma, G.N.; Koufman, J.A. The validity and reliability of the reflux finding score (RFS). Laryngoscope 2001, 111, 1313–1317. [Google Scholar] [CrossRef]
- Belafsky, P.C.; Postma, G.N.; Koufman, J.A. Validity and reliability of the reflux symptom index (RSI). J. Voice 2002, 16, 274–277. [Google Scholar] [CrossRef]
- Smith, S.S.; Oei, T.P.; Douglas, J.A.; Brown, I.; Jorgensen, G.; Andrews, J. Confirmatory factor analysis of the Epworth Sleepiness Scale (ESS) in patients with obstructive sleep apnoea. Sleep Med. 2008, 9, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M.; Hamilton, C.; Samuelson, C.G.; Lundgren, M.E.; Pott, T. Diagnostic value of the Friedman tongue position and Mallampati classification for obstructive sleep apnea: A meta-analysis. Otolaryngol. Head Neck Surg. 2013, 148, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Dams, S.D.; de Liefde-van Beest, M.; Nuijs, A.M.; Oomens, C.W.; Baaijens, F.P. Pulsed heat shocks enhance procollagen type I and procollagen type III expression in human dermal fibroblasts. Skin Res. Technol. 2010, 16, 354–364. [Google Scholar] [CrossRef]
- Unver, T.; Aytugar, E.; Ozturan, O.; Kıran, T.; Ademci, E.; Usumez, A. Histological effects of Er:YAG laser irradiation with snoring handpiece in the rat soft palate. Photomed Laser Surg. 2016, 34, 321–325. [Google Scholar] [CrossRef]
- Parker, S.; Cronshaw, M.; Anagnostaki, E.; Mylona, V.; Lynch, E.; Grootveld, M. Current Concepts of Laser Oral Tissue interaction. Dent. J. 2020, 8, 61. [Google Scholar] [CrossRef]
- Liu, H.; Dang, Y.; Wang, Z.; Chai, X.; Ren, Q. Laser induced collagen remodeling: A comparative study in vivo on mouse model. Lasers Surg. Med. 2008, 40, 13–19. [Google Scholar] [CrossRef]
- Lee, Y.S.C.; Lee, C.Y.C. Evaluation of a non-ablative Er: YAG laser procedure to increase the oropharyngeal airway volume: A pilot study. Dent. Oral Craniofac. Res. 2015, 1, 56–59. [Google Scholar]
- Kim, K.S.; Kim, J.H.; Park, S.Y.; Won, H.R.; Lee, H.J.; Yang, H.S.; Kim, H.J. Smoking induces oropharyngeal narrowing and increases the severity of obstructive sleep apnea syndrome. J. Clin. Sleep Med. 2012, 8, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.M.; Dibbern, R.S.; Santos, V.J.; Passeri, L.A. Influence of obesity on the correlation between laryngopharyngeal reflux and obstructive sleep apnea. Braz. J. Otorhinolaryngol. 2014, 80, 5–10. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Simple Snorers |
| OSAS * (Light OSAS and Moderate or Severe OSAS Patients That Refused Conventional Therapies That Were Thoroughly Explained, Including c-PAP) | |
| Exclusion Criteria | Central apnea |
| Pregnancy | |
| Children | |
| FNMM +: N ≥ 3; H ≥ 3; L ≥ 3 at NOHL # | |
| Reinke’s edema | |
| Tonsils size > 50% of obstruction of the oropharynx | |
| Nasal polyposis or other obstructive masses of nose, rhynopharynx or hypopharynx |
| Simple Snoring:Three3 Sessions (Polysomnography Was Performed) | |
|---|---|
| OSAS: Four or more sessions depending on severity. The laser treatments have to be performed 7–10 days apart (the last treatment may be performed one month after the previous treatment) | |
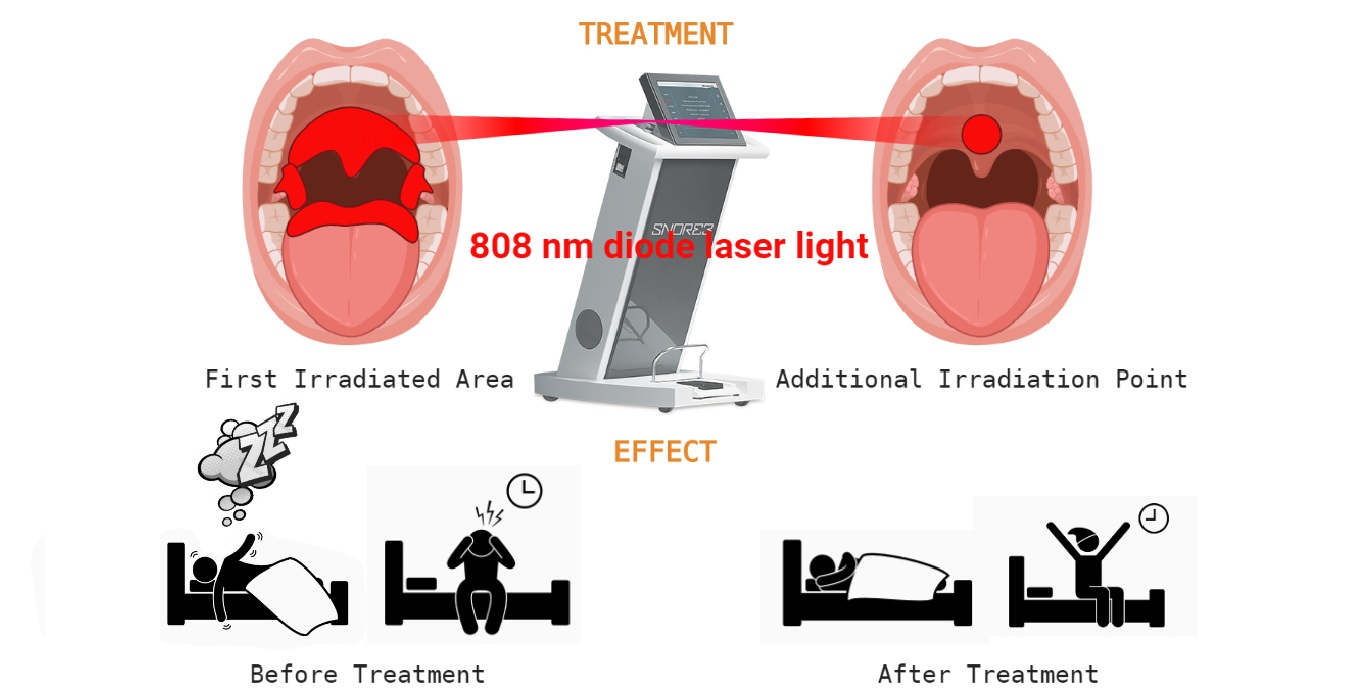
| Time of treatment | 30 min on the entire soft palate using the straight glass rod |
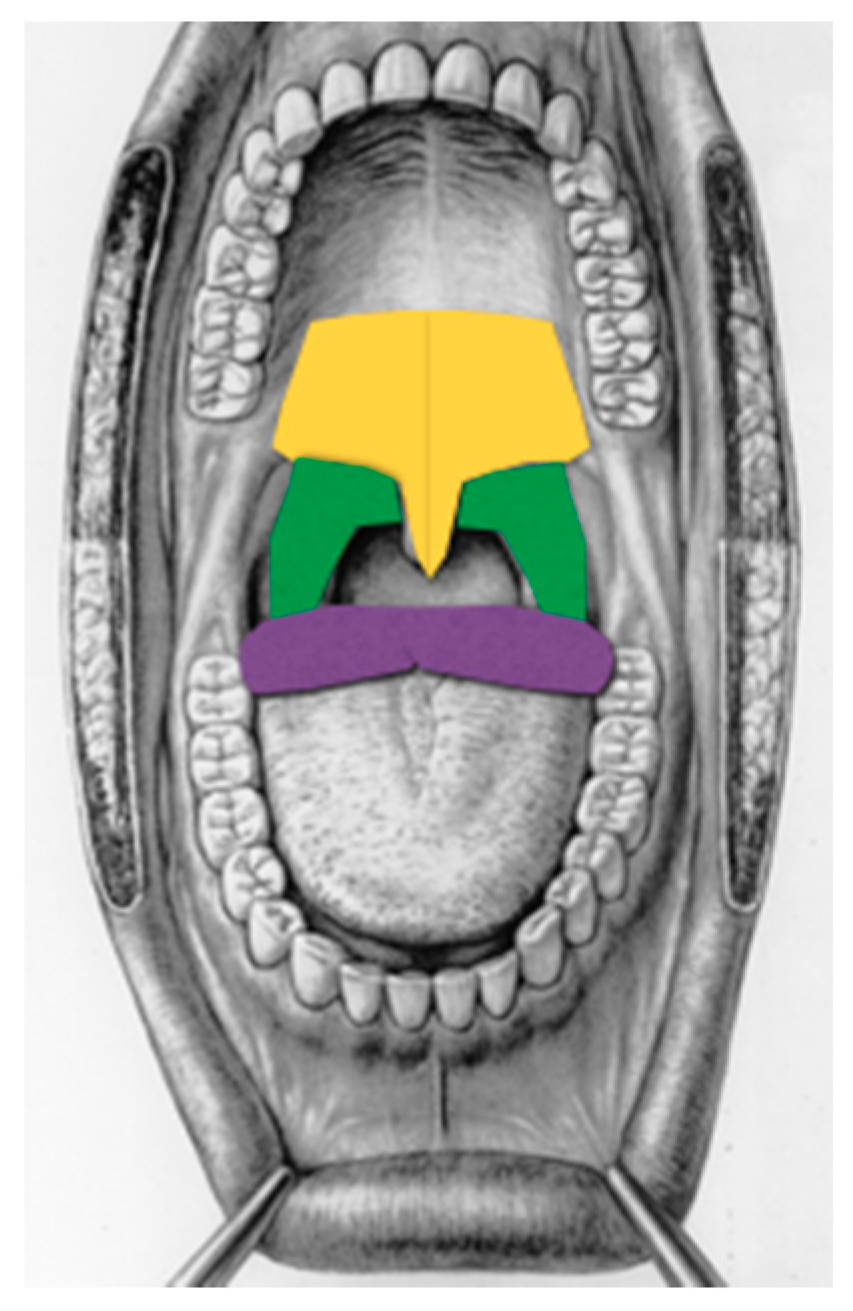
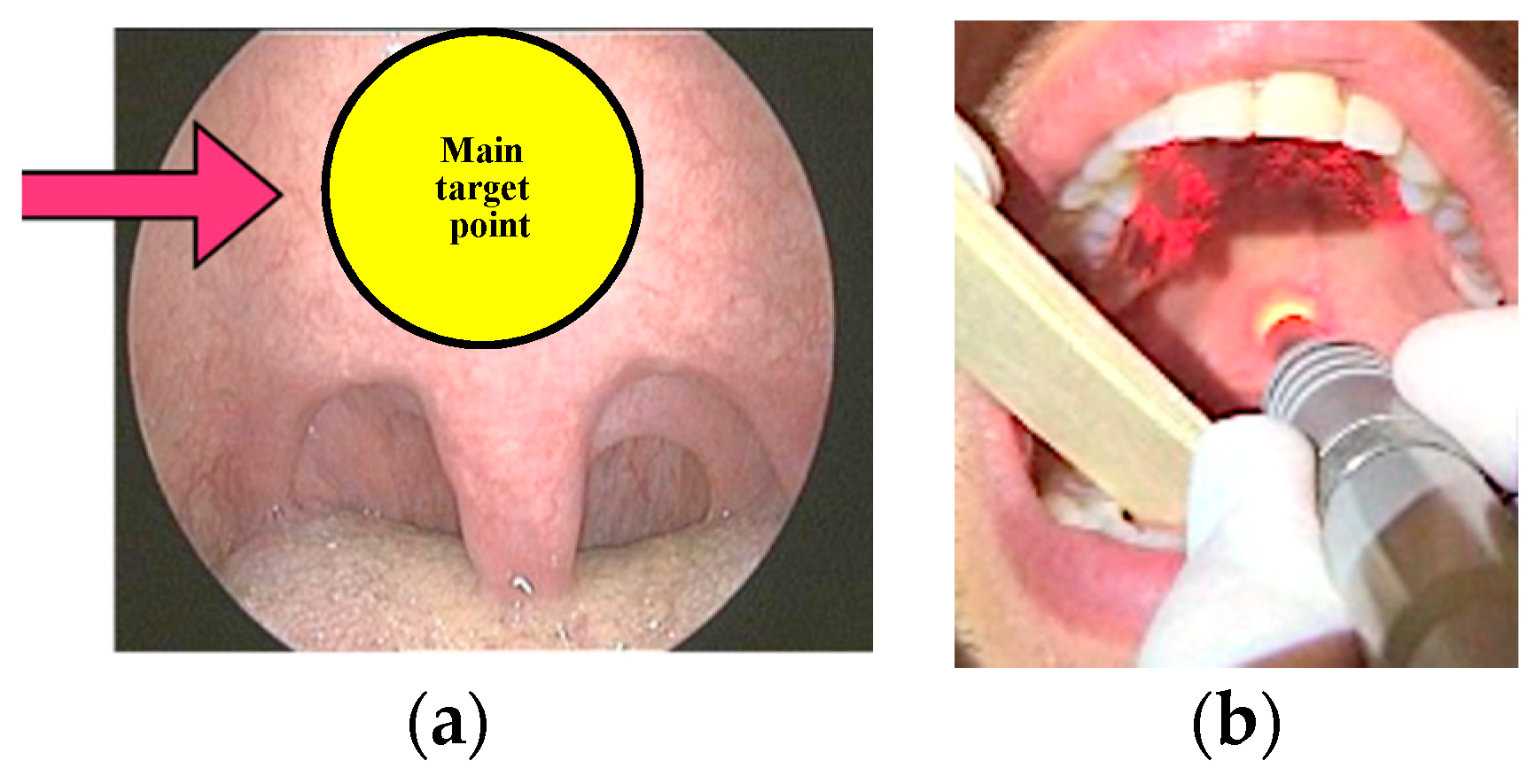
| 10 min of overlap on the so-called “main target point” using the straight glass rod. The main target point is the region of the soft palate midline posterior to the hard palate for an area of about 3 × 3 cm where the vibration of the soft palate begins (Figure 2) and, in the same region another three minutes of laser irradiation at 20 watts, frequency of 20,000 Hz, and 10 microseconds pulse duration (mean output of 4 watts) | |
| 10 min on lateral pharyngeal walls using either the straight or curved glass rod if needed (based on FNMM, which was compulsory before treatments in order to evaluate the exact region where the obstruction occurs) | |
| 15 min on the base of the tongue midline as far as possible holding the tongue with gauze (using the curved glass rod) if the FNMM showed an obstruction at that site. | |
| VAS + of snoring loudness from 1 to 10 (by bed partner) (rating of snoring intensity: 0 (no snoring) up to 10 (extreme snoring causing bed partner to leave the bedroom) |  | |
| - rating of waking up during sleep because of snoring: 0 (never) up to 10 (every night) | ||
| - subjective occurrence of dreaming during the night: 0 (sleep without dreams) up to 10 (sleep associated with dreaming) | ||
| - difficulty waking up in the morning: 0 (no difficulty) up to10 (extremely difficult) | ||
| - quality of sleep: 0 (restless sleep) up to 10 (restful sleep) | ||
| - dryness of mouth upon awakening: 0 (never) to 10 (always) | ||
| - tiredness on awakening: 0 (well-rested) up to 10 (poorly rested) | ||
| - day time sleepiness: 0 (never) to 10 (always) | ||
| FTP * and Mallampati patients’ classification evaluated before and after the laser treatments to achieve a more objective evaluation of the procedure | Class 1—full visibility of tonsils, uvula, and soft palate | |
| Class 2—visibility of hard and soft palate, the upper portion of tonsils and uvula | ||
| Class 3—soft and hard palate and base of the uvula are visible | ||
| Class 4—only hard palate visible | ||
| All Patients N = 45 | |
|---|---|
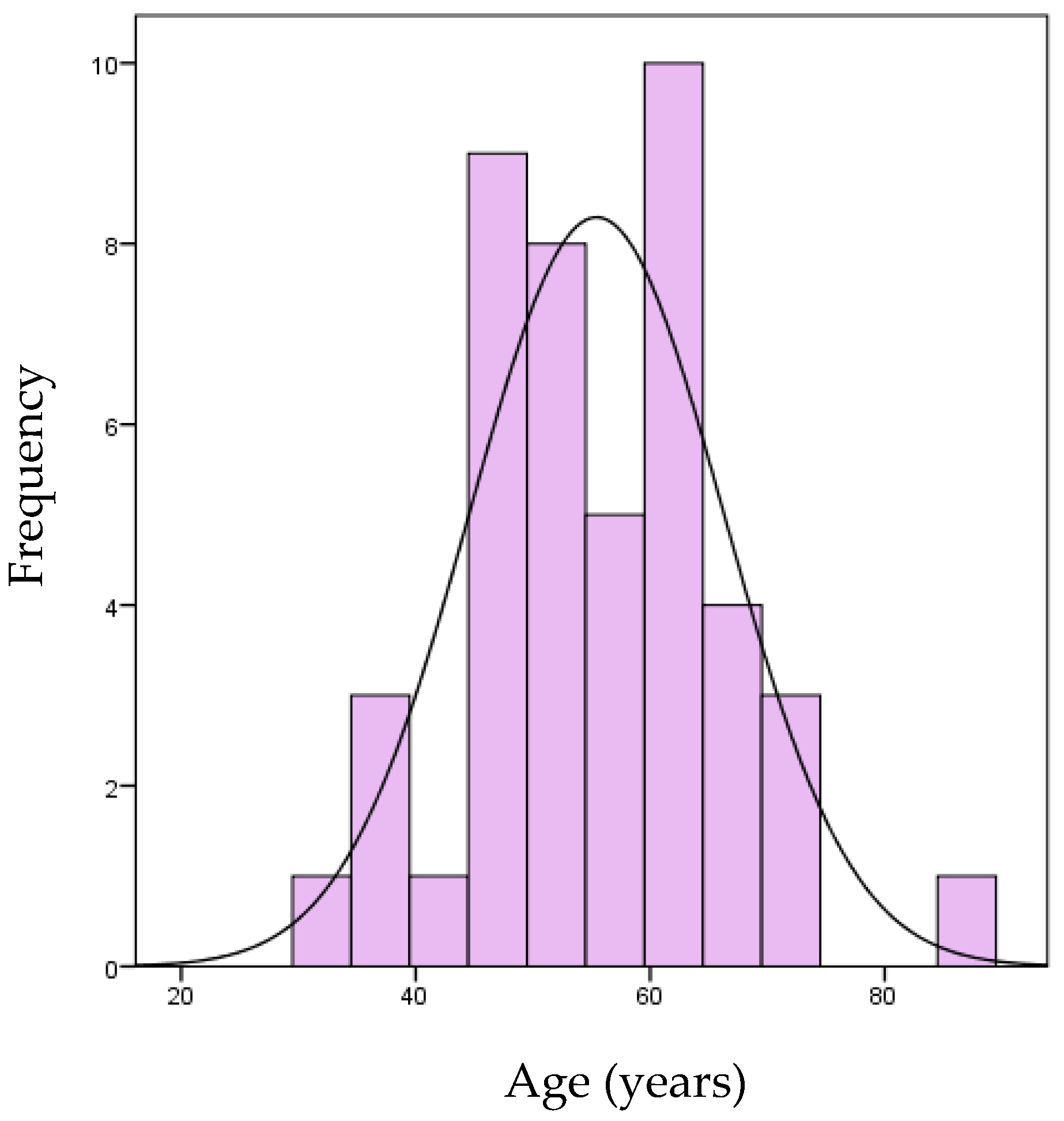
| Age, years (mean ± sd) | 55.4 (± 10.8) |
| Age, years | 55 (48–63) |
| Body Mass Index | 25.6 (23–27.5) |
| Weight of patients | |
| Normoweight | 22 (48.9%) |
| Overweight or obese | 23 (51.1%) |
| Presence of allergies | 12/42 (28.6%) |
| Smoking | 7 (15.6%) |
| Co-morbidities | 17 (37.8%) |
| Quality of the breath | |
| Good | 13 (29.5%) |
| Acceptable | 13 (29.5%) |
| Slightly compromised | 10 (22.7%) |
| Seriously compromised | 8 (18.3%) |
| Tonsils | |
| Intravelic | 17 (37.8%) |
| Extravelic < 50% | 16 (35.6%) |
| Extravelic > 50% | 1 (2.2%) |
| Tonsillectomy | 11 (24.4%) |
| Laryngo-pharyngeal reflux | 39 (86.7%) |
| Obstructive Sleep Apnea Syndrome | 23 (51.1%) |
| Before Treatment N = 45 | After Treatment N = 45 | p-Value | |
|---|---|---|---|
| Friedman Tongue Position | <0.0001 | ||
| Class 4 | 36 (80.0%) | 11 (24.4%) | |
| Class 3 | 8 (17.8%) | 29 (64.4%) | |
| Class 2 | 1 (2.2%) | 5 (11.1%) | |
| Mallampati | <0.0001 | ||
| Class 4 | 26 (57.8%) | 4 (8.9%) | |
| Class 3 | 15 (33.3%) | 29 (64.4%) | |
| Class 2 | 4 (8.9%) | 11 (24.4%) | |
| Class 1 | 0 (0.0%) | 1 (2.2%) | |
| Muller Test (O = oropharynx- retropalatal collapse) | <0.0001 | ||
| Class 4 | 37 (82.2%) | 7 (15.6%) | |
| Class 3 | 8 (17.8%) | 32 (71.1%) | |
| Class 2 | 0 (0.0%) | 6 (13.3%) | |
| Epworth Sleepiness Scale | 13 (11–15) N = 12 | 5 (3–9) N = 10 | <0.0001 |
| VAS Snoring | 10 (8–10) N = 44 | 3.5 (2–5) N = 44 | <0.0001 |
| Restful sleep | 5 (3–7) N = 43 | 8 (8–10) N = 43 | <0.0001 |
| Difficulty waking up | 0 (0–5.5) N = 44 | 0 (0–0) N = 44 | 0.001 |
| Dreaming during the night | 3 (1–8) N = 43 | 8 (6–10) N = 43 | <0.0001 |
| Waking up during sleep | 5 (0–5.5) N = 44 | 0 (0–0) N = 44 | <0.0001 |
| Dry mouth | 8 (5–10) N = 44 | 0 (0–5) N = 44 | <0.0001 |
| Presence of choking | 9/44 (20.5%) | 1/44 (2.3%) | 0.005 |
| Tiredness upon awakening | 5 (0–8) N = 43 | 0 (0–0) N = 43 | <0.0001 |
| Day time sleepiness | 5 (0–7) N = 43 | 0 (0–0) N = 43 | <0.0001 |
| Restless legs syndrome | 6/44 (13.6%) | 1/44 (2.3%) | 0.025 |
| Apnea-Hypopnea Index (AHI) | 29 (23.9–42.2) N = 23 | 16.8 (11.5–31) N = 23 | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fini Storchi, I.; Frosecchi, M.; Bovis, F.; Zekiy, A.; Benedicenti, S.; Amaroli, A.; Convissar, R.A. Snoring and Sleep-Related Symptoms: A Novel Non-Invasive 808 nm Wavelength Diode Laser Non-Ablative Outpatient Treatment. A Prospective Pilot-Study on 45 Patients. Photonics 2021, 8, 69. https://0-doi-org.brum.beds.ac.uk/10.3390/photonics8030069
Fini Storchi I, Frosecchi M, Bovis F, Zekiy A, Benedicenti S, Amaroli A, Convissar RA. Snoring and Sleep-Related Symptoms: A Novel Non-Invasive 808 nm Wavelength Diode Laser Non-Ablative Outpatient Treatment. A Prospective Pilot-Study on 45 Patients. Photonics. 2021; 8(3):69. https://0-doi-org.brum.beds.ac.uk/10.3390/photonics8030069
Chicago/Turabian StyleFini Storchi, Isabelle, Massimo Frosecchi, Francesca Bovis, Angelina Zekiy, Stefano Benedicenti, Andrea Amaroli, and Robert A. Convissar. 2021. "Snoring and Sleep-Related Symptoms: A Novel Non-Invasive 808 nm Wavelength Diode Laser Non-Ablative Outpatient Treatment. A Prospective Pilot-Study on 45 Patients" Photonics 8, no. 3: 69. https://0-doi-org.brum.beds.ac.uk/10.3390/photonics8030069