
Inhalation Exposure to PCB from Contaminated Indoor Air—How Much Is Absorbed into the Blood?

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Group
3.2. PCB in Indoor Air
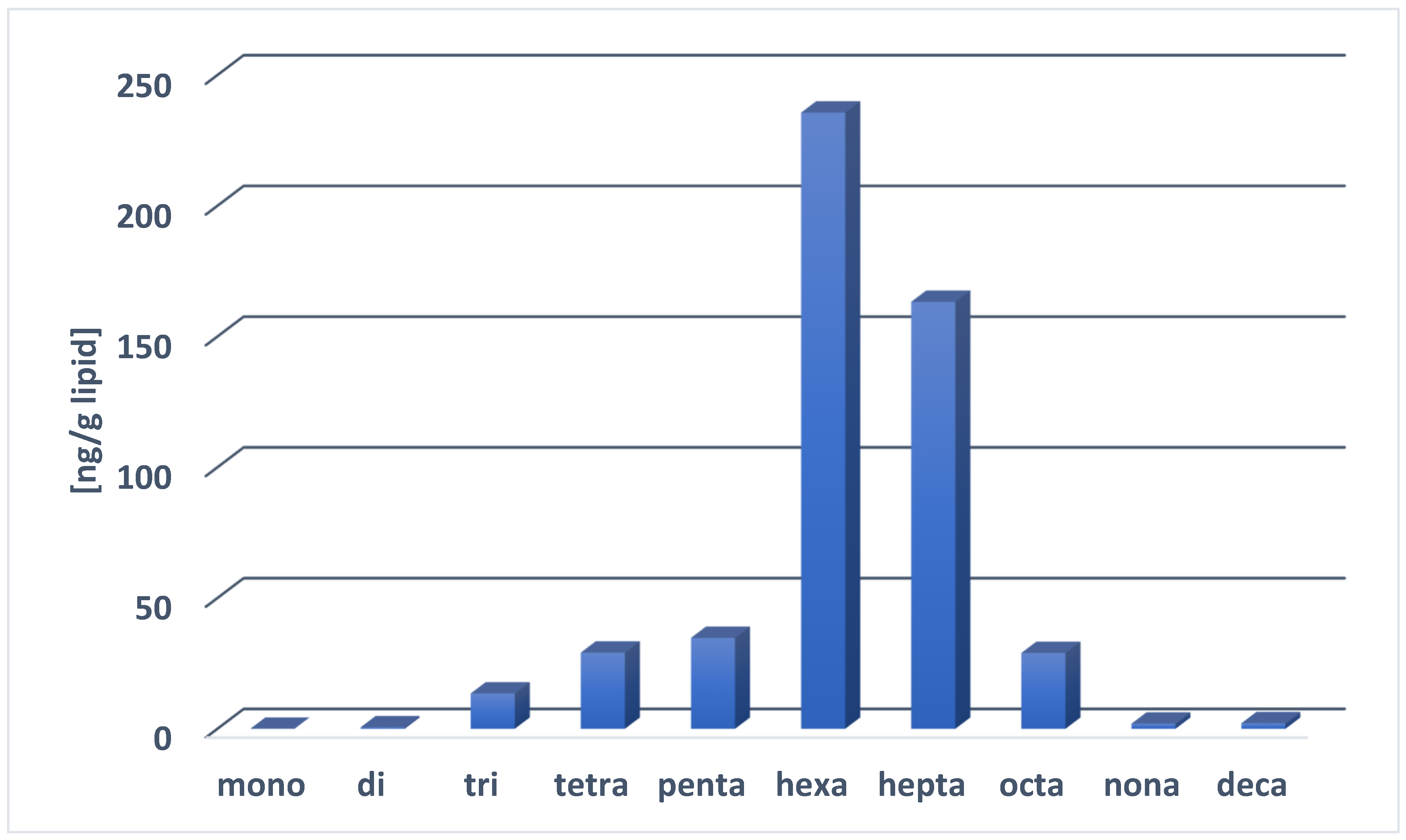
3.3. PCB in Blood
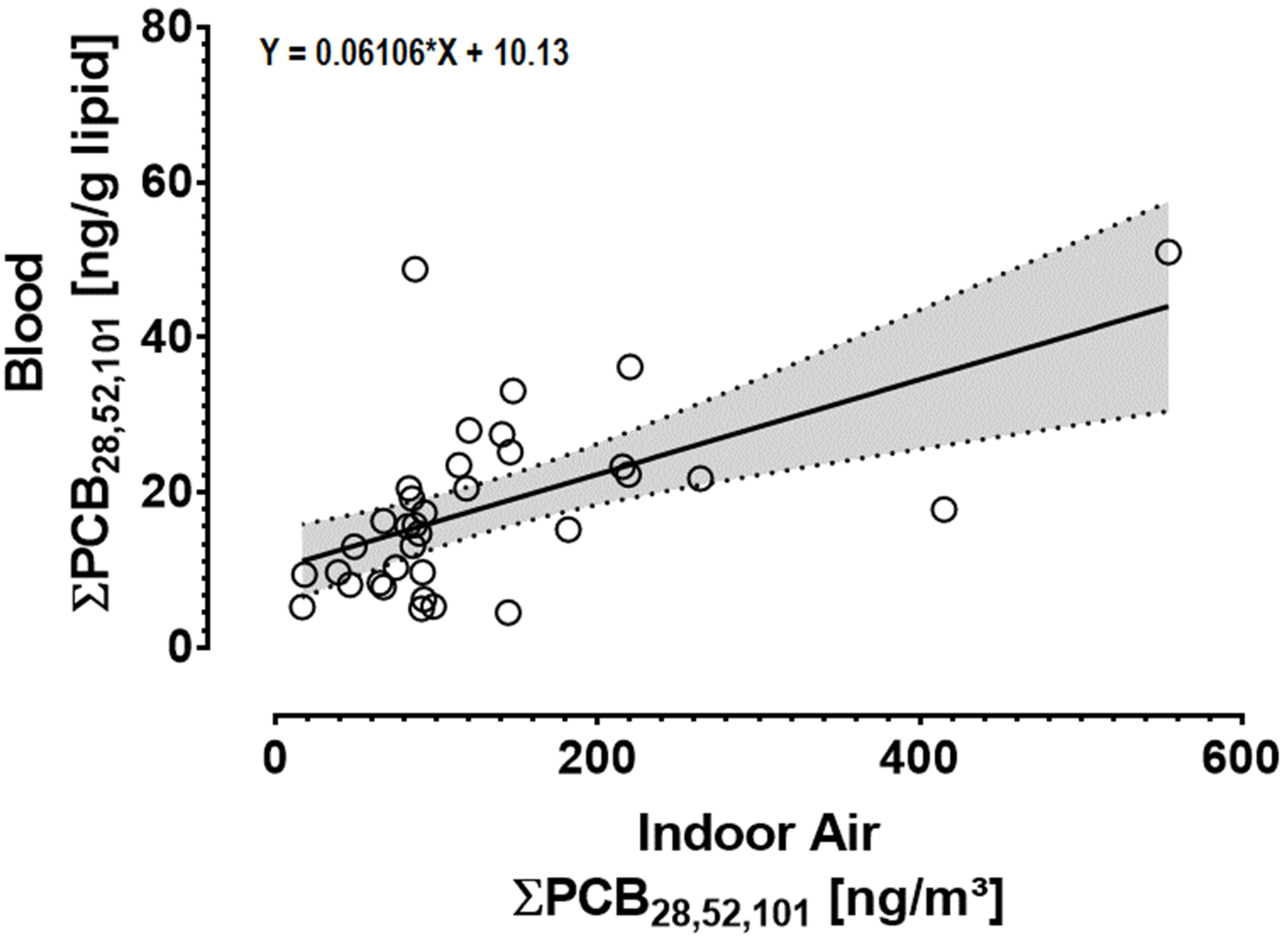
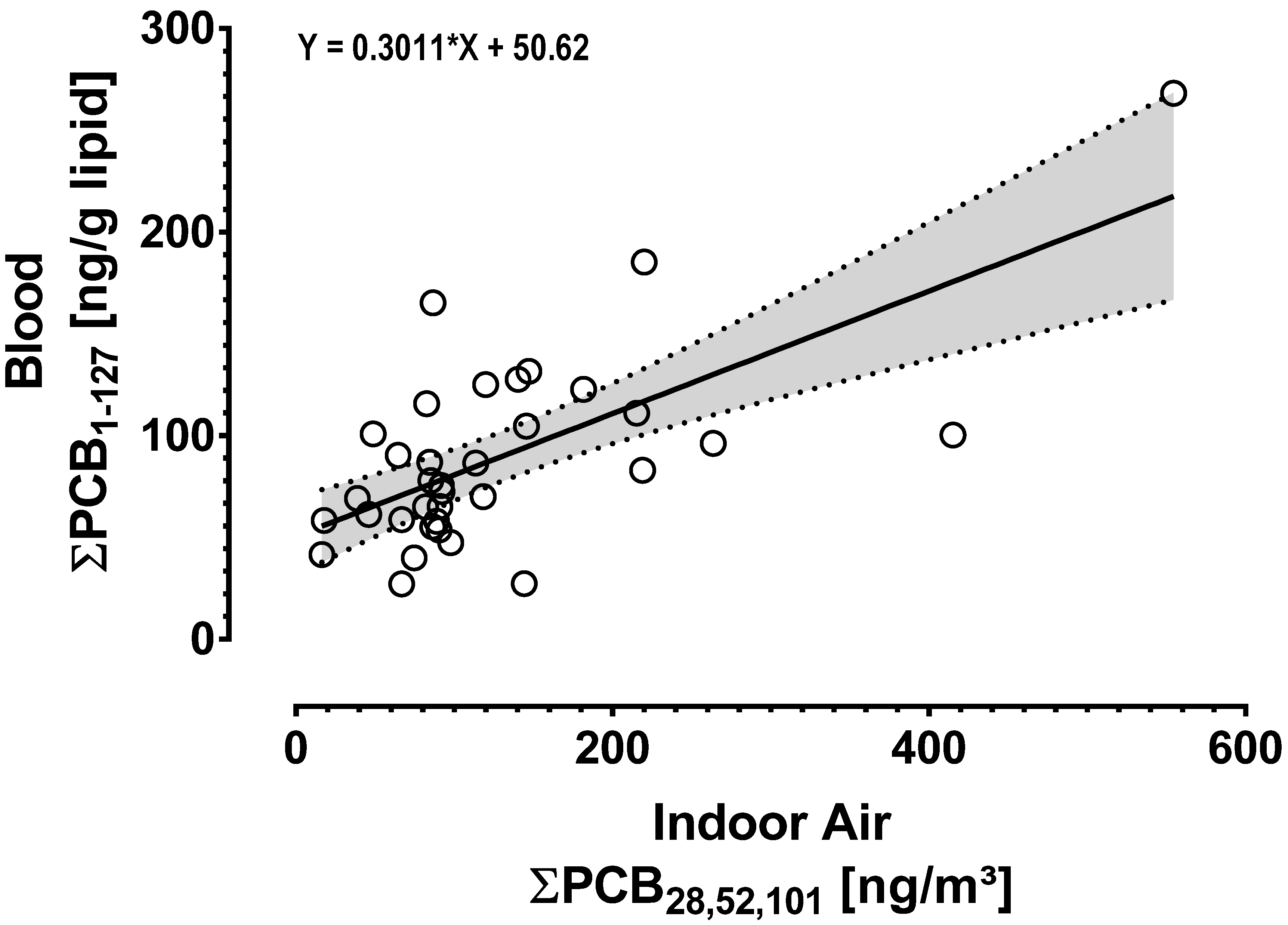
3.4. Correlation between PCBs in Indoor Air and in the Blood of Exposed Individuals
3.5. Quantification of PCBs Absorbed into the Blood from Indoor Air
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Breivik, K.; Sweetman, A.; Pacyna, J.M.; Jones, K.C. Towards a global historical emission inventory for selected PCB congeners—A mass balance approach: 1. Global production and consumption. Sci. Total Environ. 2002, 290, 181–198. [Google Scholar] [CrossRef]
- EFSA–European Food Safety Authority. Update of the monitoring of levels of dioxins and PCBs in food and feed. EFSA J. 2012, 10, 2832. [Google Scholar]
- WHO–World Health Organization. Safety Evaluation of Certain Food Additives and Contaminants: Supplement 1: Non-Dioxin-Like Polychlorinated Biphenyls/Prepared by the Eightieth Meeting of the Joint FAO/WHO Expert Committee on Food Additives (JECFA); World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Grimm, F.A.; Klaren, W.D.; Li, X.; Lehmler, H.-J.; Karmakar, M.; Robertson, L.W.; Chiu, W.A.; Rusyn, I. Cardiovascular effects of polychlorinated biphenyls and their major metabolites. Environ. Health Perspect. 2020, 128, 77008. [Google Scholar] [CrossRef] [PubMed]
- Lauby-Secretan, B.; Loomis, D.; Grosse, Y.; Ghissassi, F.E.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Baan, R.; Mattock, H.; Straif, K. Carcinogenicity of polychlorinated biphenyls and polybrominated biphenyls. Lancet Oncol. 2013, 14, 287–288. [Google Scholar] [CrossRef] [Green Version]
- Malisch, R.; Kotz, A. Dioxins and PCBs in feed and food-review from European perspective. Sci. Total Environ. 2014, 491–492, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Saktrakulkla, P.; Lan, T.; Hua, J.; Marek, R.F.; Thorne, P.S.; Hornbuckle, K.C. Polychlorinated biphenyls in food. Environ. Sci. Technol. 2020, 54, 11443–11452. [Google Scholar] [CrossRef]
- Fattore, E.; Fanelli, R.; Dellatte, E.; Turrini, A.; Di Domenico, A. Assessment of the dietary exposure to non-dioxin-like PCBs of the Italian general population. Chemosphere 2008, 73, S278–S283. [Google Scholar] [CrossRef]
- Cogliano, V.J. Lack of data drives uncertainty in PCB health risk assessments. Environ. Sci. Pollut. Res. 2016, 23, 2212–2219. [Google Scholar] [CrossRef]
- Lehmann, G.M.; Christensen, K.; Maddaloni, M.; Phillips, L.J. Evaluating health risks from inhaled polychlorinated biphenyls: Research needs for addressing uncertainty. Environ. Health Perspect. 2015, 123, 109–113. [Google Scholar] [CrossRef] [Green Version]
- Frederiksen, M.; Meyer, H.W.; Ebbehøj, N.E.; Gunnarsen, L. Polychlorinated biphenyls (PCBs) in indoor air originating from sealants in contaminated and uncontaminated apartments within the same housing estate. Chemosphere 2012, 89, 473–479. [Google Scholar] [CrossRef]
- Marek, R.F.; Thorne, P.S.; Herkert, N.J.; Awad, A.M.; Hornbuckle, K.C. Airborne PCBs and OH-PCBs inside and outside urban and rural U.S. schools. Environ. Sci. Technol. 2017, 51, 7853–7860. [Google Scholar] [CrossRef] [PubMed]
- Kraft, M.; Sievering, S.; Grün, L.; Rauchfuss, K. Mono-, di-, and trichlorinated biphenyls (PCB 1-PCB 39) in the indoor air of office rooms and their relevance on human blood burden. Indoor Air 2018, 28, 441–449. [Google Scholar] [CrossRef]
- Andersen, H.V.; Gunnarsen, L.; Knudsen, L.E.; Frederiksen, M. PCB in air, dust and surface wipes in 73 Danish homes. Int. J. Hyg. Environ. Health 2020, 229, 113429. [Google Scholar] [CrossRef] [PubMed]
- Frederiksen, M.; Andersen, H.V.; Haug, L.S.; Thomsen, C.; Broadwell, S.L.; Egsmose, E.L.; Kolarik, B.; Gunnarsen, L.; Knudsen, L.E. PCB in serum and hand wipes from exposed residents living in contaminated high-rise apartment buildings and a reference group. Int. J. Hyg. Environ. Health 2020, 224, 113430. [Google Scholar] [CrossRef]
- Gabrio, T.; Piechotowski, I.; Wallenhorst, T.; Klett, M.; Cott, L.; Friebel, P.; Link, B.; Schwenk, M. PCB-blood levels in teachers, working in PCB-contaminated schools. Chemosphere 2000, 40, 1055–1062. [Google Scholar] [CrossRef]
- Johansson, N.; Hanberg, A.; Wingfors, H.; Tysklind, M. PCB in building sealant is influencing PCB levels in blood of residents. Organohalogen Compd. 2003, 63, 381–384. [Google Scholar]
- Liebl, B.; Schettgen, T.; Kerscher, G.; Broding, H.-C.; Otto, A.; Angerer, J.; Drexler, H. Evidence for increased internal exposure to lower chlorinated polychlorinated biphenyls (PCB) in pupils attending a contaminated school. Int. J. Hyg. Environ. Health 2004, 207, 315–324. [Google Scholar] [CrossRef]
- Schettgen, T.; Alt, A.; Preim, D.; Keller, D.; Kraus, T. Biological monitoring of indoor-exposure to dioxin-like and non-dioxin-like polychlorinated biphenyls (PCB) in a public building. Toxicol. Lett. 2012, 213, 116–121. [Google Scholar] [CrossRef]
- Meyer, H.W.; Frederiksen, M.; Göen, T.; Ebbehøj, N.E.; Gunnarsen, L.; Brauer, C.; Kolarik, B.; Müller, J.; Jacobsen, P. Plasma polychlorinated biphenyls in residents of 91 PCB-contaminated and 108 non-contaminated dwellings-an exposure study. Int. J. Hyg. Environ. Health 2013, 216, 755–762. [Google Scholar] [CrossRef]
- Pedersen, E.B.; Ebbehøj, N.E.; Göen, T.; Meyer, H.W.; Jacobsen, P. Exposure to 27 polychlorinated biphenyls in the indoor environment of a workplace: A controlled bio-monitoring study. Int. Arch. Occup. Environ. Health 2016, 89, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Marek, R.F.; Thorne, P.S.; Wang, K.; DeWall, J.; Hornbuckle, K.C. PCBs and OH-PCBs in serum from children and mothers in urban and rural U.S. communities. Environ. Sci. Technol. 2013, 47, 3353–3361. [Google Scholar] [CrossRef] [PubMed]
- Marek, R.F.; Thorne, P.S.; DeWall, J.; Hornbuckle, K.C. Variability in PCB and OH-PCB serum levels in children and their mothers in urban and rural U.S. communities. Environ. Sci. Technol. 2014, 48, 13459–13467. [Google Scholar] [CrossRef]
- Kraft, M.; Rauchfuss, K.; Sievering, S.; Wöckner, M.; Neugebauer, F.; Fromme, H. Quantification of all 209 PCB congeners in blood-Can indicators be used to calculate the total PCB blood load? Int. J. Hyg. Environ. Health 2017, 220, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Schwenk, M.; Gabrio, T.; Päpke, O.; Wallenhorst, T. Human biomonitoring of polychlorinated biphenyls and polychlorinated dibenzodioxins and dibenzofuranes in teachers working in a PCB-contaminated school. Chemosphere 2002, 47, 229–233. [Google Scholar] [CrossRef]
- Herrick, R.F.; Meeker, J.D.; Altshul, L. Serum PCB levels and congener profiles among teachers in PCB-containing schools: A pilot study. Environ. Health 2011, 10, 56. [Google Scholar] [CrossRef] [Green Version]
- Egsmose, E.L.; Bräuner, E.V.; Frederiksen, M.; Mørck, T.A.; Siersma, V.D.; Hansen, P.W.; Nielsen, F.; Grandjean, P.; Knudsen, L.E. Associations between plasma concentrations of PCB 28 and possible indoor exposure sources in Danish school children and mothers. Environ. Int. 2016, 87, 13–19. [Google Scholar] [CrossRef]
- Fitzgerald, E.F.; Shrestha, S.; Palmer, P.M.; Wilson, L.R.; Belanger, E.E.; Gomez, M.I.; Cayo, M.R.; Hwang, S.-A. Polychlorinated biphenyls (PCBs) in indoor air and in serum among older residents of upper Hudson River communities. Chemosphere 2011, 85, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Ampleman, M.D.; Martinez, A.; DeWall, J.; Rawn, D.F.K.; Hornbuckle, K.C.; Thorne, P.S. Inhalation and dietary exposure to PCBs in urban and rural cohorts via congener-specific measurements. Environ. Sci. Technol. 2015, 49, 1156–1164. [Google Scholar] [CrossRef] [PubMed]
- Fromme, H.; Hilger, B.; Albrecht, M.; Gries, W.; Leng, G.; Völkel, W. Occurrence of chlorinated and brominated dioxins/furans, PCBs, and brominated flame retardants in blood of German adults. Int. J. Hyg. Environ. Health 2016, 219, 380–388. [Google Scholar] [CrossRef]
- Apostoli, P.; Magoni, M.; Bergonzi, R.; Carasi, S.; Indelicato, A.; Scarcella, C.; Donato, F. Assessment of reference values for polychlorinated biphenyl concentration in human blood. Chemosphere 2005, 61, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Schettgen, T.; Alt, A.; Esser, A.; Kraus, T. Current data on the background burden to the persistent organochlorine pollutants HCB, p,p’-DDE as well as PCB 138, PCB 153 and PCB 180 in plasma of the general population in Germany. Int. J. Hyg. Environ. Health 2015, 218, 380–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandow, N.; Conrad, A.; Kolossa-Gehring, M.; Murawski, A.; Sawal, G. Polychlorinated biphenyls (PCB) and organochlorine pesticides (OCP) in blood plasma–Results of the German environmental survey for children and adolescents 2014–2017 (GerES V). Int. J. Hyg. Environ. Health 2020, 224, 113426. [Google Scholar] [CrossRef] [PubMed]
- Mørck, T.A.; Erdmann, S.E.; Long, M.; Mathiesen, L.; Nielsen, F.; Siersma, V.D.; Bonefeld-Jørgensen, E.C.; Knudsen, L.E. PCB concentrations and dioxin-like activity in blood samples from Danish school children and their mothers living in urban and rural areas. Basic Clin. Pharmacol. Toxicol. 2014, 115, 134–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n > LOQ | Minimum | 25th Percentile | Median | 75th Percentile | 95th Percentile | Maximum | Mean | |
|---|---|---|---|---|---|---|---|---|
| [ng/g l.w.] | [ng/g l.w.] | [ng/g l.w.] | [ng/g l.w.] | [ng/g l.w.] | [ng/g l.w.] | [ng/g l.w.] | ||
| PCB 28 | 35 | 2.2 | 5.9 | 12 | 16 | 37 | 39 | 13 |
| PCB 52 | 35 | 0.35 | 1.2 | 2.3 | 4.3 | 8.7 | 8.9 | 3.0 |
| PCB 101 | 35 | 0.39 | 0.7 | 1.6 | 2.9 | 4.5 | 4.7 | 1.9 |
| PCB 138 | 35 | 8.8 | 28 | 47 | 64 | 129 | 196 | 52 |
| PCB 153 | 35 | 19 | 74 | 136 | 168 | 311 | 531 | 143 |
| PCB 180 | 35 | 11 | 59 | 78 | 128 | 367 | 370 | 112 |
| ∑PCB1–209 | 119 | 385 | 559 | 750 | 1600 | 2152 | 632 |
| Indoor Air | Blood | Spearman’s Coefficient (Rho) of Correlation | p Value |
|---|---|---|---|
| PCB28 | PCB28 | 0.534 | <0.001 |
| PCB52 | PCB52 | 0.564 | <0.001 |
| PCB101 | PCB101 | 0.686 | <0.001 |
| ∑PCB28,52,101 | ∑PCB28,52,101 | 0.587 | <0.001 |
| ∑PCB28,52,101 | ∑PCB1–127 (mono-penta) | 0.535 | 0.001 |
| ∑PCB28,52,101,138,153,180x5 | ∑PCB1–39 (mono-tri) | 0.462 | 0.005 |
| ∑PCB28,52,101,138,153,180x5 | ∑PCB1–81 (mono-tetra) | 0.551 | 0.001 |
| ∑PCB28,52,101,138,153,180x5 | ∑PCB1–127 (mono-penta) | 0.542 | 0.001 |
| ∑PCB28,52,101,138,153,180x5 | ∑PCB1–169 (mono-hexa) | (0.130) | (0.455) |
| ∑PCB28,52,101,138,153,180x5 | ∑PCB1–209 (mono-deca) | (0.050) | (0.775) |
| Indoor Air [ng/m3] | Blood [ng/g l.w.] | ||
|---|---|---|---|
| ∑PCB28,52,101 | 100 | ∑PCB28,52,101 | 16 (95% CI 13–20) |
| 300 | 29 (95% CI 22–35) | ||
| ∑PCB28,52,101 | 100 | ∑PCB1–127 | 81 (95% CI 68–93) |
| 300 | 141 (95% CI 118–164) | ||
| Indoor Air [ng/m3] | Blood [ng/g l.w.] | ||
|---|---|---|---|
| ∑PCB28,52,101 | ∑PCB28,52,101,138,153,180×5 | ∑PCB1–127 | |
| room A | 92 | 479 | 78 (95% CI 65–91) |
| room B | 555 | 2797 | 218 (95% CI 167–269) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kraft, M.; Rauchfuss, K.; Fromme, H.; Grün, L.; Sievering, S.; Köllner, B.; Chovolou, Y. Inhalation Exposure to PCB from Contaminated Indoor Air—How Much Is Absorbed into the Blood? Pollutants 2021, 1, 181-193. https://0-doi-org.brum.beds.ac.uk/10.3390/pollutants1030015
Kraft M, Rauchfuss K, Fromme H, Grün L, Sievering S, Köllner B, Chovolou Y. Inhalation Exposure to PCB from Contaminated Indoor Air—How Much Is Absorbed into the Blood? Pollutants. 2021; 1(3):181-193. https://0-doi-org.brum.beds.ac.uk/10.3390/pollutants1030015
Chicago/Turabian StyleKraft, Martin, Knut Rauchfuss, Hermann Fromme, Lothar Grün, Silvia Sievering, Barbara Köllner, and Yvonni Chovolou. 2021. "Inhalation Exposure to PCB from Contaminated Indoor Air—How Much Is Absorbed into the Blood?" Pollutants 1, no. 3: 181-193. https://0-doi-org.brum.beds.ac.uk/10.3390/pollutants1030015