Antibacterial-Integrated Collagen Wound Dressing for Diabetes-Related Foot Ulcers: An Evidence-Based Review of Clinical Studies

 ,
,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Study Selection
2.5. Data Extraction and Management
2.6. Risk of Bias Assessment
3. Results
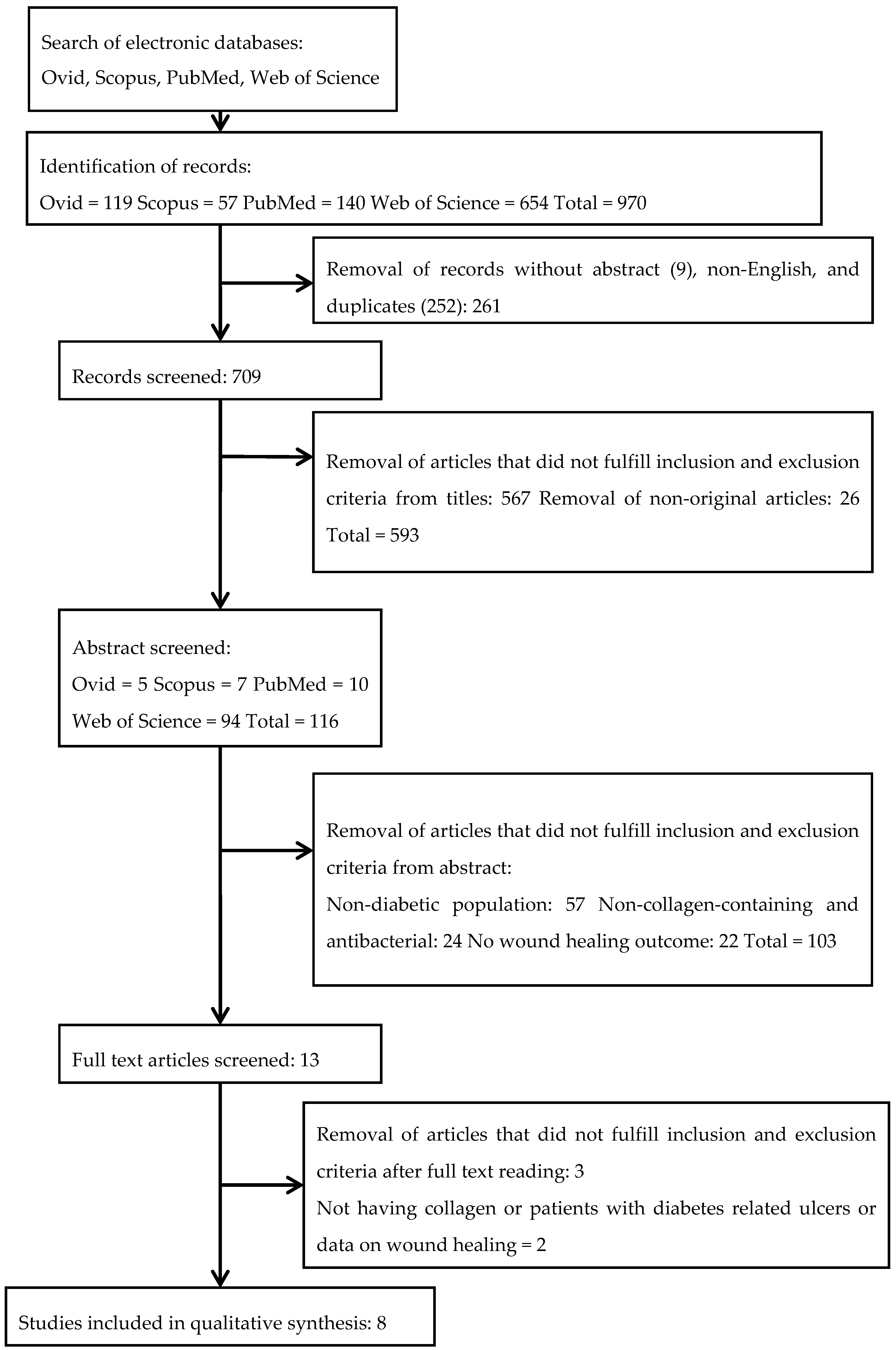
3.1. Search Results
3.2. Study Characteristics
3.3. Gentamicin on Collagen Dressing
3.4. Collagen with Polyhexamethylene Biguanide
3.5. Hybrid Collagen-Cellulose Integrated with Silver
3.6. Collagen Dressing Gentian with Violet/Methylene Blue
3.7. Collagen Integrated with Silver
3.8. Quality of Articles Methodology
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Fernandes, J.D.R.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.J.; Lee, K.M.; Park, M.S.; Choi, S.H.; Park, J.I.; Cho, J.H.; Park, K.H.; Woo, S.J. Association between diabetic foot ulcer and diabetic retinopathy. PLoS ONE 2017, 12, e0175270. [Google Scholar] [CrossRef] [Green Version]
- Tan, W.S.; Arulselvan, P.; Ng, S.F.; Taib, C.N.M.; Sarian, M.N.; Fakurazi, S. Improvement of diabetic wound healing by topical application of Vicenin-2 hydrocolloid film on Sprague Dawley rats 11 Medical and Health Sciences 1103 Clinical Sciences. BMC Complement. Altern. Med. 2019, 19, 20. [Google Scholar] [CrossRef]
- Ayuk, S.M.; Abrahamse, H.; Houreld, N.N. The Role of Matrix Metalloproteinases in Diabetic Wound Healing in relation to Photobiomodulation. J. Diabetes Res. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahiru, I.; Amaefule, K.; Okpe, I.; Ibrahim, A.; Muazu, S. An overview of diabetic foot disease. Niger. J. Basic Clin. Sci. 2016, 13, 1. [Google Scholar] [CrossRef]
- Percival, S.L.; Vuotto, C.; Donelli, G.; Lipsky, B.A. Biofilms and Wounds: An Identification Algorithm and Potential Treatment Options. Adv. Wound Care 2015, 4, 389–397. [Google Scholar] [CrossRef]
- Kim, P.J.; Attinger, C.E.; Bigham, T.; Hagerty, R.; Platt, S.; Anghel, E.; Steinberg, J.S.; Evans, K.K. Clinic-based Debridement of Chronic Ulcers Has Minimal Impact on Bacteria. Wounds Compend. Clin. Res. Pract. 2018, 30, 114–119. [Google Scholar]
- Messenger, G.; Masoetsa, R.; Hussain, I. A Narrative Review of the Benefits and Risks of Total Contact Casts in the Management of Diabetic Foot Ulcers. J. Am. Coll. Clin. Wound Spec. 2017, 9, 19–23. [Google Scholar] [CrossRef]
- Alternatives to the Total Contact Cast for the Treatment of Diabetic|WoundSOurce Foot Wounds. Available online: https://www.woundsource.com/blog/alternatives-total-contact-cast-in-managing-diabetic-foot-ulcers (accessed on 7 April 2020).
- Smith-Strøm, H.; Iversen, M.M.; Igland, J.; Østbye, T.; Graue, M.; Skeie, S.; Wu, B.; Rokne, B. Severity and duration of diabetic foot ulcer (DFU) before seeking care as predictors of healing time: A retrospective cohort study. PLoS ONE 2017, 12, e0177176. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, P.P.; Ray, S.; Biswas, D.; Baidya, A.; Bhattacharjee, R.; Mukhopadhyay, P.; Ghosh, S.; Mukhopadhyay, S.; Chowdhury, S. A comparative study between total contact cast and pressure-relieving ankle foot orthosis in diabetic neuropathic foot ulcers. J. Diabetes Sci. Technol. 2015, 9, 302–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cullum, N.; Davies, M.; Harrison, M.; Howers, L.M.; Murphy, S.; Walters, B. Chronic Wounds: Advanced Wound Dressings and Antimicrobial Dressings; Nice: London, UK, 2016; pp. 1–43. ISBN 978-1-4731-1781-5. [Google Scholar]
- Hurlow, J.; Couch, K.; Laforet, K.; Bolton, L.; Metcalf, D.; Bowler, P. Clinical Biofilms: A Challenging Frontier in Wound Care. Adv. Wound Care 2015, 4, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malone, M.; Bjarnsholt, T.; McBain, A.J.; James, G.A.; Stoodley, P.; Leaper, D.; Tachi, M.; Schultz, G.; Swanson, T.; Wolcott, R.D. The prevalence of biofilms in chronic wounds: A systematic review and meta-analysis of published data. J. Wound Care 2017, 26, 20–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpenter, S.; Davis, S.; Fitzgerald, R.; Gehling, M.; Kapp, D.; Karr, J.; Samies, J.; Shultz, G.; Teichman, A.; Weir, D. Expert Recommendations for Optimizing Outcomes in the Management of Biofilm to Promote Healing of Chronic Wounds; HMP Communications LLC: Malvern, PA, USA, 2016. [Google Scholar]
- Barker, J.C.; Khansa, I.; Gordillo, G.M. A Formidable Foe Is Sabotaging Your Results. Plast. Reconstr. Surg. 2017, 139, 1184e–1194e. [Google Scholar] [CrossRef]
- Seth, A.K.; Geringer, M.R.; Hong, S.J.; Leung, K.P.; Mustoe, T.A.; Galiano, R.D. In vivo modeling of biofilm-infected wounds: A review. J. Surg. Res. 2012, 178, 330–338. [Google Scholar] [CrossRef]
- Misic, A.M.; Gardner, S.E.; Grice, E.A. The Wound Microbiome: Modern Approaches to Examining the Role of Microorganisms in Impaired Chronic Wound Healing. Adv. Wound Care 2014, 3, 502–510. [Google Scholar] [CrossRef] [Green Version]
- Abbas, M.; Uçkay, I.; Lipsky, B.A. In diabetic foot infections antibiotics are to treat infection, not to heal wounds. Expert Opin. Pharmacother. 2015, 16, 821–832. [Google Scholar] [CrossRef]
- Kramer, A.; Dissemond, J.; Kim, S.; Willy, C.; Mayer, D.; Papke, R.; Tuchmann, F.; Assadian, O. Consensus on Wound Antisepsis: Update 2018. Skin Pharmacol. Physiol. 2018, 31, 28–58. [Google Scholar] [CrossRef]
- Nelson, E.A.; O’Meara, S.; Golder, S.; Dalton, J.; Craig, D.; Iglesias, C. Systematic review of antimicrobial treatments for diabetic foot ulcers. Diabet. Med. 2006, 23, 348–359. [Google Scholar] [CrossRef]
- Landsman, A.; Blume, P.A.; Jordan, D.A.; Vayser, D.; Gutierrez, A. An Open-label, Three-arm Pilot Study of the Safety and Efficacy of Topical Microcyn Rx Wound Care versus Oral Levofloxacin versus Combined Therapy for Mild Diabetic Foot Infections. J. Am. Podiatr. Med. Assoc. 2011, 101, 484–496. [Google Scholar] [CrossRef]
- Perde-Schrepler, M.; Florea, A.; Brie, I.; Virag, P.; Fischer-Fodor, E.; Vâlcan, A.; Gurzău, E.; Lisencu, C.; Maniu, A. Size-Dependent Cytotoxicity and Genotoxicity of Silver Nanoparticles in Cochlear Cells In Vitro. J. Nanomater. 2019, 2019, 6090259. [Google Scholar] [CrossRef] [Green Version]
- O’Meara, S.; Cullum, N.; Majid, M.; Sheldon, T. Systematic reviews of wound care management: (3) Antimicrobial agents for chronic wounds; (4) diabetic foot ulceration. Health Technol. Assess. (Rockv) 2000, 4, 1–3. [Google Scholar] [CrossRef]
- Moura, L.I.F.; Dias, A.M.A.; Carvalho, E.; De Sousa, H.C. Recent advances on the development of wound dressings for diabetic foot ulcer treatment-A review. Acta Biomater. 2013, 9, 7093–7114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, Z.; Thu, H.E.; Shuid, A.N.; Katas, H.; Hussain, F. Recent Advances in Polymer-based Wound Dressings for the Treatment of Diabetic Foot Ulcer: An Overview of State-of-the-art. Curr. Drug Targets 2017, 19, 527–550. [Google Scholar] [CrossRef]
- Wu, L.; Norman, G.; Dumville, J.C.; O’Meara, S.; Bell-Syer, S.E.M. Dressings for treating foot ulcers in people with diabetes: An overview of systematic reviews. Cochrane Database Syst. Rev. 2015, CD010471. [Google Scholar] [CrossRef] [Green Version]
- Gianino, E.; Miller, C.; Gilmore, J. Smart Wound Dressings for Diabetic Chronic Wounds. Bioengineering 2018, 5, 51. [Google Scholar] [CrossRef] [Green Version]
- Djavid, G.E.; Tabaie, S.M.; Tajali, S.B.; Totounchi, M.; Farhoud, A.; Fateh, M.; Ghafghazi, M.; Koosha, M.; Taghizadeh, S. Application of a collagen matrix dressing on a neuropathic diabetic foot ulcer: A randomised control trial. J. Wound Care 2020, 29, S13–S18. [Google Scholar] [CrossRef]
- Killat, J.; Reimers, K.; Choi, C.Y.; Jahn, S.; Vogt, P.M.; Radtke, C. Cultivation of keratinocytes and fibroblasts in a three-dimensional bovine collagen-elastin matrix (Matriderm®) and application for full thickness wound coverage in vivo. Int. J. Mol. Sci. 2013, 14, 14460–14474. [Google Scholar] [CrossRef]
- O’Brien, F.J. Biomaterials & scaffolds for tissue engineering. Mater. Today 2011, 14, 88–95. [Google Scholar] [CrossRef]
- Rangaraj, A.; Harding, K.; Leaper, D.; Rangaraj, A.; Harding, K. David Leaper Role of collagen in wound management. Wounds UK 2011, 7, 54–63. [Google Scholar]
- Parenteau-Bareil, R.; Gauvin, R.; Berthod, F. Collagen-based biomaterials for tissue engineering applications. Materials 2010, 3, 1863–1887. [Google Scholar] [CrossRef] [Green Version]
- Chattopadhyay, S.; Raines, R.T. Collagen-based biomaterials for wound healing. Biopolymers 2014, 101, 821–833. [Google Scholar] [CrossRef] [Green Version]
- Holmes, C.; Wrobel, J.S.; Maceachern, M.P.; Boles, B.R. Collagen-based wound dressings for the treatment of diabetes-related foot ulcers: A systematic review. Diabetes Metab. Syndr. Obes. Targets Ther. 2013, 6, 17–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loh, E.Y.X.; Fauzi, M.B.; Ng, M.H.; Ng, P.Y.; Ng, S.F.; Ariffin, H.; Amin, M.C.I.M. Cellular and Molecular Interaction of Human Dermal Fibroblasts with Bacterial Nanocellulose Composite Hydrogel for Tissue Regeneration. ACS Appl. Mater. Interfaces 2018, 10, 39532–39543. [Google Scholar] [CrossRef] [PubMed]
- Fauzi, M.B.; Lokanathan, Y.; Aminuddin, B.S.; Ruszymah, B.H.I.; Chowdhury, S.R. Ovine tendon collagen: Extraction, characterisation and fabrication of thin films for tissue engineering applications. Mater. Sci. Eng. C 2016, 68, 163–171. [Google Scholar] [CrossRef]
- Fauzi, M.B.; Lokanathan, Y.; Nadzir, M.M.; Aminuddin, S.; Ruszymah, B.H.I.; Chowdhury, S.R.; Ramanauskiene, K.; Stelmakiene, A.; Briedis, V.; Ivanauskas, L.; et al. Attachment, proliferation, and morphological properties of human dermal fibroblasts on ovine tendon collagen scaffolds: A comparative study. Malays. J. Med. Sci. 2017, 24, 33–43. [Google Scholar] [CrossRef]
- Busra, F.M.; Chowdhury, S.R.; Saim, A.B.; Idrus, R.B. Genotoxicity and cytotoxicity of ovine collagen on human dermal fibroblasts. Saudi Med. J. 2011, 32, 1311–1312. [Google Scholar]
- Bohn, G.; Liden, B.; Schultz, G.; Yang, Q.; Gibson, D.J. Ovine-Based Collagen Matrix Dressing: Next-Generation Collagen Dressing for Wound Care. Adv. Wound Care 2016, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Busra, F.M.; Rajab, N.F.; Tabata, Y.; Saim, A.B.; Idrus, R.B.H.; Chowdhury, S.R. Rapid treatment of full-thickness skin loss using ovine tendon collagen type I scaffold with skin cells. J. Tissue Eng. Regen. Med. 2019, 13, 874–891. [Google Scholar] [CrossRef]
- Ge, L.; Xu, Y.; Li, X.; Yuan, L.; Tan, H.; Li, D.; Mu, C. Fabrication of Antibacterial Collagen-Based Composite Wound Dressing. ACS Sustain. Chem. Eng. 2018, 6, 9153–9166. [Google Scholar] [CrossRef]
- Hixon, K.R.; Lu, T.; McBride-Gagyi, S.H.; Janowiak, B.E.; Sell, S.A. A Comparison of Tissue Engineering Scaffolds Incorporated with Manuka Honey of Varying UMF. Biomed Res. Int. 2017, 2017, 4843065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalil, M.A.A.; Kasmuri, A.R.; Hadi, H. Stingless bee honey, the natural wound healer: A review. Skin Pharmacol. Physiol. 2017, 30, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.M.; Chou, Y.T.; Wen, Z.H.; Wang, Z.R.; Chen, C.H.; Ho, M.L. Novel Biodegradable Porous Scaffold Applied to Skin Regeneration. PLoS ONE 2013, 8, e56330. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Checklists and Notes. Available online: https://www.sign.ac.uk/checklists-and-notes (accessed on 4 April 2020).
- De Oliveira, N.K.; Miguita, L.; Salles, T.H.C.; d’Ávila, M.A.; Marques, M.M.; Deboni, M.C.Z. Can porous polymeric scaffolds be functionalized by stem cells leading to osteogenic differentiation? A systematic review of in vitro studies. J. Mater. Sci. 2018, 53, 15757–15768. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Kuss, M.; Edmonds, M.; Reyzelman, A.; Sigal, F. Topical application of a gentamicin-collagen sponge combined with systemic antibiotic therapy for the treatment of diabetic foot infections of moderate severity a randomized, controlled, multicenter clinical trial. J. Am. Podiatr. Med. Assoc. 2012, 102, 223–232. [Google Scholar] [CrossRef]
- Uçkay, I.; Kressmann, B.; Malacarne, S.; Toumanova, A.; Jaafar, J.; Lew, D.; Lipsky, B.A. A randomized, controlled study to investigate the efficacy and safety of a topical gentamicin-collagen sponge in combination with systemic antibiotic therapy in diabetic patients with a moderate or severe foot ulcer infection. BMC Infect. Dis. 2018, 18, 361. [Google Scholar] [CrossRef] [Green Version]
- Uçkay, I.; Kressmann, B.; Di Tommaso, S.; Portela, M.; Alwan, H.; Vuagnat, H.; Maître, S.; Paoli, C.; Lipsky, B.A. A randomized controlled trial of the safety and efficacy of a topical gentamicin–collagen sponge in diabetic patients with a mild foot ulcer infection. SAGE Open Med. 2018, 6. [Google Scholar] [CrossRef] [Green Version]
- Varga, M.; Sixta, B.; Bem, R.; Matia, I.; Jirkovska, A.; Adamec, M. Application of gentamicin-collagen sponge shortened wound healing time after minor amputations in diabetic patients—A prospective, randomised trial. Arch. Med. Sci. 2014, 2, 283–287. [Google Scholar] [CrossRef] [Green Version]
- Bain, M.A.; Thibodeaux, K.T.; Speyrer, M.S.; Carlson, E.; Koullias, G.J. Effect of Native Type I Collagen with Polyhexamethylene Biguanide Antimicrobial on Wounds: Interim Registry Results. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2251. [Google Scholar] [CrossRef]
- Oropallo, A.R. Use of native type i collagen matrix plus polyhexamethylene biguanide for chronic wound treatment. Plast. Reconstr. Surg. Glob. Open 2019, 7, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gottrup, F.; Cullen, B.M.; Karlsmark, T.; Bischoff-Mikkelsen, M.; Nisbet, L.; Gibson, M.C. Randomized controlled trial on collagen/oxidized regenerated cellulose/silver treatment. Wound Repair Regen. 2013, 21, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Lullove, E.L. Use of Ovine-based Collagen Extracellular Matrix and Gentian Violet/Methylene Blue Antibacterial Foam Dressings to Help Improve Clinical Outcomes in Lower Extremity Wounds: A Retrospective Cohort Study. Wounds 2017, 29, 107–114. [Google Scholar] [PubMed]
- Manizate, F.; Fuller, A.; Gendics, C.; Lantis, J.C. A prospective, single-center, nonblinded, comparative, postmarket clinical evaluation of a bovine-derived collagen with ionic silver dressing versus a carboxymethylcellulose and ionic silver dressing for the reduction of bioburden in variable-etiology, bi. Adv. Ski. Wound Care 2012, 25, 220–225. [Google Scholar] [CrossRef]
- Maczynska, B.; Secewicz, A.; Smutnicka, D.; Szymczyk, P.; Dudek-Wicher, R.; Junka, A.; Bartoszewicz, M. In vitro efficacy of gentamicin released from collagen sponge in eradication of bacterial biofilm preformed on hydroxyapatite surface. PLoS ONE 2019, 14, e0217769. [Google Scholar] [CrossRef]
- Mishra, P.K.; Ashoub, A.; Salhiyyah, K.; Aktuerk, D.; Ohri, S.; Raja, S.G.; Luckraz, H. Role of topical application of gentamicin containing collagen implants in cardiac surgery. J. Cardiothorac. Surg. 2014, 9, 122. [Google Scholar] [CrossRef] [Green Version]
- Dumville, J.C.; Lipsky, B.A.; Hoey, C.; Cruciani, M.; Fiscon, M.; Xia, J. Topical antimicrobial agents for treating foot ulcers in people with diabetes. Cochrane Database Syst. Rev. 2017, Issue 6, CD011038. [Google Scholar] [CrossRef]
- Schimmer, C.; Özkur, M.; Sinha, B.; Hain, J.; Gorski, A.; Hager, B.; Leyh, R. Gentamicin-collagen sponge reduces sternal wound complications after heart surgery: A controlled, prospectively randomized, double-blind study. J. Thorac. Cardiovasc. Surg. 2012, 143, 194–200. [Google Scholar] [CrossRef] [Green Version]
- Hübner, N.O.; Kramer, A. Review on the efficacy, safety and clinical applications of polihexanide, a modern wound antiseptic. Skin Pharmacol. Physiol. 2010, 23, 17–27. [Google Scholar] [CrossRef]
- Lenselink, E.; Andriessen, A. A cohort study on the efficacy of a polyhexanide-containing biocellulose dressing in the treatment of biofilms in wounds. J. Wound Care 2011, 20, 534–539. [Google Scholar] [CrossRef]
- Kaehn, K. Polihexanide: A Safe and Highly Effective Biocide. Skin Pharmacol. Physiol. 2010, 23, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Müller, G.; Kramer, A. Biocompatibility index of antiseptic agents by parallel assessment of antimicrobial activity and cellular cytotoxicity. J. Antimicrob. Chemother. 2008, 61, 1281–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lintzeris, D.; Vernon, K.; Percise, H.; Strickland, A.; Yarrow, K.; White, A.; Gurganus, M.; Sherrod, S.; Vergin, K.; Johnson, L. Effect of a New Purified Collagen Matrix With Polyhexamethylene Biguanide on Recalcitrant Wounds of Various Etiologies: A Case Series. Wounds Compend. Clin. Res. Pract. 2018, 30, 72–78. [Google Scholar]
- Wu, S.; Applewhite, A.J.; Niezgoda, J.; Snyder, R.; Shah, J.; Cullen, B.; Schultz, G.; Harrison, J.; Hill, R.; Howell, M.; et al. Oxidized Regenerated Cellulose/Collagen Dressings: Review of Evidence and Recommendations. Adv. Skin Wound Care 2017, 30, S1–S18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grothier, L. Products & technology Understanding the use of collagen/ oxidised regenerated cellulose dressings. Wounds Int. 2015, 6, 34–40. [Google Scholar]
- Keller, U.A.D.; Sabino, F. Matrix metalloproteinases in impaired wound healing. Met. Med. 2015, 2, 8. [Google Scholar] [CrossRef] [Green Version]
- Sim, W.; Barnard, R.T.; Blaskovich, M.A.T.; Ziora, Z.M. Antimicrobial Silver in Medicinal and Consumer Applications: A Patent Review of the Past Decade (2007–2017). Antibiotics 2018, 7, 93. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, D.; Smeets, R.; Unglaub, F.; Wöltje, M.; Pallua, N. Effect of oxidized regenerated cellulose/collagen matrix on proteases in wound exudate of patients with diabetic foot ulcers. J. Wound Ostomy Cont. Nurs. 2011, 38, 522–528. [Google Scholar] [CrossRef]
- Edwards, K. New Twist on an Old Favorite: Gentian Violet and Methylene Blue Antibacterial Foams. Adv. Wound Care 2016, 5, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Pandian, S.R.K.; Deepak, V.; Kalishwaralal, K.; Viswanathan, P.; Gurunathan, S. Mechanism of bactericidal activity of silver nitrate-a concentration dependent bi-functional molecule. Braz. J. Microbiol. 2010, 41, 805–809. [Google Scholar] [CrossRef] [Green Version]
- Dumville, J.C.; Deshpande, S.; O’Meara, S.; Speak, K. Foam dressings for healing diabetic foot ulcers. Cochrane Database Syst. Rev. 2013, CD009111. [Google Scholar] [CrossRef] [PubMed]
- Nussbaum, S.R.; Carter, M.J.; Fife, C.E.; DaVanzo, J.; Haught, R.; Nusgart, M.; Cartwright, D. An Economic Evaluation of the Impact, Cost, and Medicare Policy Implications of Chronic Nonhealing Wounds. Value Health 2018, 21, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fife, C.E.; Carter, M.J. Wound Care Outcomes and Associated Cost Among Patients Treated in US Outpatient Wound Centers: Data From the US Wound Registry. Wounds Compend. Clin. Res. Pract. 2012, 24, 10–17. [Google Scholar]


{kind=link}
{kind=link}
| No | Keywords |
|---|---|
| 1 | collagen |
| 2 | foam |
| 3 | sponge |
| 4 | matrix |
| 5 | por*s |
| 6 | antib* |
| 7 | antimic* |
| 8 | diabetic |
| 9 | foot |
| 10 | ulcer |
| 11 | lower extremity |
| 12 | chronic |
| 13 | wound |
| 14 | Or/2–5 |
| 15 | Or/6–7 |
| 16 | Or/8–13 |
| 17 | 1 and 14 and 15 and 16 |
| 18 | Limit 17 to yr. = “2010–2020” |
| Study | Aim | Product | Study Design | Total Sample Population (DFU) | Time | Results | Conclusion |
|---|---|---|---|---|---|---|---|
| Bain et al. 2019 [54] | Native type I Collagen with Polyhexamethylene Biguanide (PHMB) antimicrobial | PuraPly AM, Organogenesis | Prospective, Registry, post-market clinical evaluation | 63 (6) | Weekly for 24 weeks | 66.7% diabetic patients showed complete closure by week 8 No hypersensitivity issues, antimicrobial component biocompatible Positive influence on healthcare costs | Porcine collagen matrix with PHMB (PCMP) positively impact wound healing various types of lesions, including DU as adjunct therapy |
| Oropallo, AR. 2019 [55] | Native type I Collagen Matrix with Polyhexamethylene Biguanide (PCMP) ability to close DFU wounds over 12 weeks. | PuraPly AM, Organogenesis | Prospective | 41 (4) | Weekly (if necessary) for 12 weeks | 25% of DFU achieved complete closure. The mean wound closure for DFU were 43% at week 4 and 50% at week 12. | PCMP treatment responds positively to nonhealing chronic wounds including diabetic ulcers. |
| Uckay et al. 2018 [52] | Patients with mild-DFU treated with topical gentamicin and collagen sponge | Garamycin, Innocoll Pharmaceuticals Ltd.) | Randomized controlled trial | 24 (22) | 14 different days over 24 days | 91% cured clinically 56% had pathogen eradication at end of study Most frequent isolated pathogens were S. aureus, P. aeruginosa, and S. epidermis. 36% patients had polymicrobial infection. | There was no difference between the treatment and control for treating mild diabetic ulcers, but it was well tolerated. |
| Uckay et al. 2018 (1) [51] | Patients with moderate or severe DFU infection treated with topical gentamicin and collagen sponge and systemic antibiotic therapy | Garamycin, Innocoll Pharmaceuticals Ltd. | Randomized controlled trial | 88 (68) | Weekly for 14–28 days | 73% were cured clinically 15% improved significantly 52% had total pathogen eradication | There was no significance in the overall cure compared to control although the sponge was well tolerated. |
| Gottrup et al. 2013 [56] | Collagen/oxidized regenerated cellulose (ORC)/silver treatment compared to standard | Promogran Prisma, Systagenix | Randomized controlled trial | 39 (36) | Every 2 weeks for 14 weeks | 79% had ≥50% reduction in wound area by week 4 compared to standard (43%) Levels of elastase decreased significantly MMP-9 reduced Lower MMP-9-TIMP-1 trend Improved healing rates | Collagen/ORC/silver increased healing rates and decreased levels of infection significantly. |
| Lullove, EJ. 2017 [57] | To improve chornic wounds in the lower extremity using ovine-based collagen matrix with gentian violet/methylene blue antibacterial dressings | Hydrofera Blue, Hollister | Retrospective case series | 53 (22) | Twice weekly for 4 weeks then weekly until closure 24 weeks | 76.5% average wound closure by 8 weeks 50% DFU patients had more than 40% wound closure in 4 weeks Average 10.6 weeks to closure 100% Re-epithelisation of all wounds at week 20 except 1 case achieved at week 24. Absence of re-infection on wounds Average cost for single wound to closure is $2749.49 | Using collagen-based matrix with antibacterial foam healed more than 40% of chronic wounds within 4 weeks with absence of infection and adverse effects. |
| Manizate et al. 2012 [58] | Treat infected DFU with bovine-derived collagen and ionic silver (Ag) dressing hybrid (BDC) compared to carboxymethylcellulose and Ag dressing (CMC) | Aquacel Ag, Medline | Prospective; post-market clinical evaluation | 10 (1) | Changed daily and checked at week 1 and 4 for 8 weeks | The absolute wound closure rate of BDC were higher than CMC but percentage of closed wounds were not significant S aureus accounts for 50% of wounds with most frequency Initial bacterial load did not have any significant effect on the closure rate | There were no statistically significant differences in terms of efficacy and effect of bioburden between the two dressings, but both showed positive trend for wound healing, with BDC more preferred by patients and more superior absolute wound closure. |
| Varga et al. 2014 [53] | Treat minor amputated diabetic patients with gentamicin collagen sponge | Collatamp®EG; Syntacoll | Prospective, randomized trial | 50 (22) | Regular follow up with patients until wounds fully heal up to 20 weeks | Using the gentamicin collagen sponge shortened wound healing duration significantly by close to 2 weeks compared to those without the treatment General reduction of microbial findings in treatment group but no significant differences of bacterial loading between treated and non-treated group. | Although wound healing improved significantly with the gentamicin collagen sponge, there were no improvements to shortening the length of hospital stay, revision for wound breakdown or re-amputations. |
| Study | Bain et al. [54] | Oropallo [55] | Uckay et al. [52] | Uckay et al. (1) [51] | Gottrup et al. [56] | Lullove [57] | Manizate et al. [58] | Varga et al. [53] |
|---|---|---|---|---|---|---|---|---|
| Clinical Trials (Randomized and Cohort) Methodology | ||||||||
| Does the study have a focused question? | Y | Y | Y | Y | Y | Y | Y | Y |
| Is the study randomized with appropriate concealment method? | X | X | Y | Y | Y | X | X | Y |
| Was there some recognition that assessment of outcome could have been influenced by exposure status when blinding was not possible? | X | Y | Y | Y | Y | X | Y | X |
| Groups being studied (same or different sites) are selected from comparable source populations in all respects other than the investigated factor? | Y | X | Y | Y | Y | X | X | Y |
| Was blinding about treatment allocation performed for subjects and investigators? | X | X | Y | Y | Y | X | X | X |
| Was the only difference found is between groups the investigated treatment, i.e., large variables | X | X | Y | X | Y | X | X | X |
| How many percentage (Not more than 20%) of participants or clusters in each arm of study dropped out before study completion? | 7.9% | 0% | 8.3% | 23% | 7.7% | 0% | 0% | 10% |
| Was there a comparison made between participants throughout the entire study and those that were lost to follow up or dropped out (by exposure status)? | Y | N/A | N/A | Y | X | N/A | N/A | N/A |
| Other sources was used as evidence to demonstrate valid and reliable method of outcome assessment. | Y | Y | Y | Y | Y | X | X | Y |
| All relevant outcomes were clearly defined, are measured in a reliable, standard, and valid way | Y | Y | Y | Y | Y | Y | Y | Y |
| How well was the study done to minimise bias? | X | X | Y | Y | Y | X | X | X |
| Clinical Trials Selection of Subjects | ||||||||
| Does the study have inclusion/exclusion criteria? | Y | Y | Y | Y | Y | Y | Y | Y |
| Number of samples | Y | Y | Y | Y | Y | Y | Y | Y |
| Age (mean or median)? | 76 | 62 | 70 | 71 | 60 | 75.9 | X | 62 |
| Sex of DU patients? | ? | ? | Y | Y | Y | ? | X | Y |
| Control or comparison with another treatment or standard of care? | X | X | Y | Y | Y | X | Y | Y |
| Was there a baseline wound condition for selection? | Y | Y | Y | Y | Y | Y | Y | Y |
| Type of diabetes | X | Y | X | Y | X | X | X | Y |
| Was ankle brachial index measured and reported before selection? | X | X | Y | Y | Y | Y | Y | X |
| Was the HbA1c measured and reported? | X | X | Y | Y | Y | X | Y | Y |
| What was the median baseline wound area? | 6.5 cm2 | 7.2 cm2 | Y | Y | 4.3 cm2 | 6.4 | 14.9 | X |
| Minimum wound duration? | 4 months | 24 months | X | X | 1 month | 1 month | X | N/A |
| Outcomes Criteria | ||||||||
| Wound closure analysis? | Y | Y | ? | ? | Y | Y | Y | ? |
| Time to complete wound closure were measured appropriately? | Y | Y | X | X | X | Y | Y | Y |
| Did the study report data on either tissue granulation or exudates? | X | X | ? | ? | Y | X | X | X |
| Were there any results pertaining microbiological, pathogen, or biofilm data? | X | X | Y | Y | X | X | Y | Y |
| Does the study include an inferential statistical analysis? | X | Y | Y | Y | Y | X | Y | Y |
| Other Integrity Criteria | ||||||||
| Was there Institutional Ethical consideration? | Y | Y | Y | Y | Y | Y | Y | Y |
| Where there mentions of funding? | ? | Y | Y | Y | Y | Y | Y | X |
| Location of Site (clinical) mentioned | X | Y | Y | Y | Y | Y | X | Y |
| Year of data collection (clinical) | X | N | Y | Y | Y | Y | X | Y |
| Did authors declare/disclosure conflict of interest? | Y | Y | Y | Y | Y | Y | Y | X |
| Ratio | 16/32 (50%) | 19/32 (59%) | 25/32 (78%) | 27/32 (84%) | 29/32 (91%) | 17/32 (53%) | 18/32 (56%) | 19/32 (59%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
N. Amirrah, I.; Mohd Razip Wee, M.F.; Tabata, Y.; Bt Hj Idrus, R.; Nordin, A.; Fauzi, M.B. Antibacterial-Integrated Collagen Wound Dressing for Diabetes-Related Foot Ulcers: An Evidence-Based Review of Clinical Studies. Polymers 2020, 12, 2168. https://0-doi-org.brum.beds.ac.uk/10.3390/polym12092168
N. Amirrah I, Mohd Razip Wee MF, Tabata Y, Bt Hj Idrus R, Nordin A, Fauzi MB. Antibacterial-Integrated Collagen Wound Dressing for Diabetes-Related Foot Ulcers: An Evidence-Based Review of Clinical Studies. Polymers. 2020; 12(9):2168. https://0-doi-org.brum.beds.ac.uk/10.3390/polym12092168
Chicago/Turabian StyleN. Amirrah, Ibrahim, Mohd Farhanulhakim Mohd Razip Wee, Yasuhiko Tabata, Ruszymah Bt Hj Idrus, Abid Nordin, and Mh Busra Fauzi. 2020. "Antibacterial-Integrated Collagen Wound Dressing for Diabetes-Related Foot Ulcers: An Evidence-Based Review of Clinical Studies" Polymers 12, no. 9: 2168. https://0-doi-org.brum.beds.ac.uk/10.3390/polym12092168