4.1. Semi-Parametric Models for Multidimensional Latent Traits
IRT models above discussed assume, in their original formulation, (i) the presence of a single latent variable (unidimensionality assumption), (ii) parametric, usually normal, distribution of the latent variable, and (iii) no effect of individual characteristics on the latent variable. Often, these assumptions are restrictive and, thus, generalised versions of IRT models can be considered to allow for:
For both these reasons, the following analysis is carried out relying on the multidimensional extension of IRT models described in
Section 3.1 based on multiple latent traits with a discrete distribution, as implemented in the class of multidimensional Latent Class IRT models (LC-IRT) [
18,
39,
40]. This type of model belongs to the wide class of mixture IRT models (for a review see [
41,
42], and reference therein) that, in turn, are an example of mixture models [
43].
Furthermore, to account for the possible effect of individual characteristics on the latent variables we adopt a concomitant variable approach [
44,
45], based on the assumption that certain individual observable covariates may affect the clustering of individuals.
Let
be the item response configuration of individual
i and
be the vector of
D latent variables that drive the response process (in our context,
, being Limitations and Dysphoria the two latent variables involved in the analysis). The latter is assumed to have a discrete distribution with
k support points (i.e., components)
. Each support point
is referred to a latent class
u of individuals who share common levels of the latent traits. Let
be the possible realisation of
with
and let
(
) the weights for each component denoting the prior probability of belonging to latent class
u. Here, to make easier the interpretation of the latent classes and to improve the parsimony of the model (see [
18] for details), the number
k of mixture components is assumed the same for all the latent traits. This implies that individuals belonging to the same latent class are characterised by a class-specific profile in terms of the
D latent variables (i.e., Limitations and Dysphoria), being possible that a class may have high levels on all the
D dimensions, another class low levels on all the
D dimensions, and some other class high levels on some dimensions and low levels on some other ones. Thus, the dependency among the
D dimensions (i.e., between Limitations and Dysphoria) emerges as a consequence of aggregating the dimensions across the latent classes.
The manifest distribution of the individual’s response vector
follows the Latent Class (LC) model [
37,
38]. Thus, extending the formula in (
1) we obtain
where
is specified in accordance with IRT parameterisation, that is
with
indicator variable yielding 1 if item
j measures latent trait
. Same extension may be pursued starting from Equation (
3). As in the unidimensional model, the discriminating parameters
measure the capacity of the item to discern between individuals with different levels of latent traits. The difficulty parameters
are specific of each pair of consecutive item response categories and measure, for each item, the difficulty of answering
r or more. In the context at issue, high values of
(
) denote a general tendency to disagree with item
j or, in other words, only individuals belonging to latent classes with high levels of the latent traits are expected to choose high values of
r for item
j. On the opposite, low values of
characterise items for which respondents generally agree.
Notice that
and
are constant among the latent classes. Alternative formulations of mixture IRT models that remove these constraints are represented, for instance, by the diagnostic model [
40], characterised by fixed rather than free latent traits, and the mixed Rasch-type models [
46,
47] that rely on a mixture of separate Rasch models with class-specific person and item parameters. Anyway, alternative constraints have to be imposed to allow for free item parameters among classes. In addition, the estimation process related with these alternative formulations turns out to be computationally demanding without providing an effective advantage in terms of interpretation of parameters, which results quite complex.
To ensure the identification of the proposed model, some further constraints have to be considered on the model parameters. As usual in the IRT approach, one item discriminating parameter must be constrained to 1 for each latent trait and one item threshold difficulty parameter to 0 for each latent trait. Alternatively, we may constraint the weighted sum of mixture components to be equal to 0 for each latent trait. In addition, one latent class weight must be obtained as the complement to 1 of the remaining weights. Taking into account these aspects the number of free parameters is
The model may be extended to account for the effect of individual characteristics on the latent class membership. Following the concomitant variable approach [
44,
45], the individual-constant weights
are replaced with individual-specific weights
generally modelled through a multinomial logit formulation
with
class-specific constant term and
class-specific vector of regression coefficients that describe the effect of covariates on the prior probability of belonging to class
u with respect to the reference class (e.g. class 1). Alternatively, whenever latent classes are ordered with respect to latent traits the
holds, that is,
In such a case, regression coefficients collected in vector are common to all the latent classes and their interpretation is easier. Furthermore, when covariates are considered the number of free model parameters is equal to under the multinomial logit formulation because of the presence of regression coefficients and thresholds (constant terms), whereas it becomes under the due to p regression coefficients and thresholds.
Different from alternative approaches based on multi-steps strategies (tipically, estimation of the IRT model followed by estimation of the covariates effect), the concomitant variable approach here adopted has the advantage of providing consistent estimates and predicting the most likely latent class for those individuals who have not yet answered the test items.
Inference for this class of models follows and generalises the main content summarised in
Section 3.1. EM algorithm is provided in [
34], to which we refer for details. We outline that, as usual in the mixture and latent class type models, the number
k of mixture components is not a model parameter but it has a constant value that has to be a priori fixed. Whenever theoretical reasons do not exist to support a given value of
k, the choice is usually based on the comparison among alternative models through the BIC index.
The selection of dimensions may be performed by a LR statistic used to test the unidimensionality of a set of items against a specific multidimensional alternative. Details are in [
18].
4.2. Results-II
In this section results based on the application of multidimensional latent class IRT models for ordinal polytomous item responses were described following the steps proposed in [
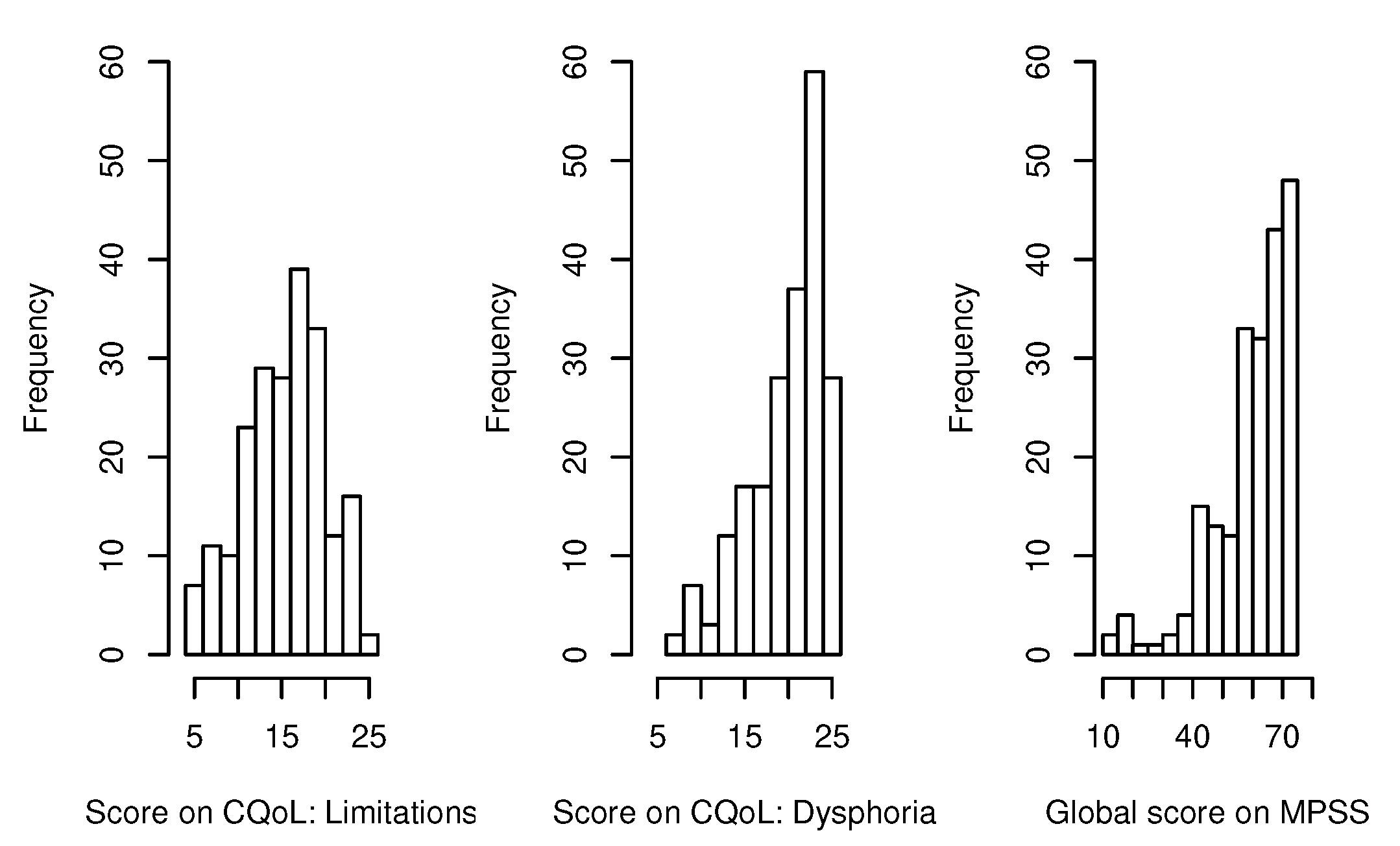
18]. The dimensionality structure of the model was defined according to the two considered dimensions of CQoL
Limitations and
Dysphoria, with items 1 to 5 loading on
Limitations and items 6 to 10 loading on
Dysphoria. Firstly, we carried out the standard LC model without covariates for different values of
k to detect the best number of latent classes. Given
k, we selected the most appropriate link function by estimating a bidimensional model both with global and local logit, again without covariates. In the third step, we compared the model selected at the previous step with its constrained versions to choose suitable constraints on the item parameters. In the end, we added several individual covariates, reaching the final model, whose results were described in depth. In what follows, we report details about each of the mentioned steps.
Number of latent classes. In order to select the optimal number of classes, we carried out the standard LC model with
number of classes not including any covariates. The BIC was used to choose the best model. Results displayed in
Table 5 led us to consider
latent classes.
Type of link function. We chose the most appropriare link function by estimating a bidimensional LC-IRT model both with global and local logit (GRM and GPCM, respectively), keeping the number of classes (
) previously selected. Again, the BIC was used as selection criteria. Results in
Table 6 show that global logit link (GRM) is better, thus confirming what obtained with the unidimensional IRT models (
Table 4).
Constraints on the item parameters. In order to select the constraints on item parameters, we compared the bidimensional LC GRM with its constrained versions, namely bidimensional LC RS-GRM, 1P-GRM and 1P-RS-GRM, through the BIC index. Also in this step, we considered models without covariates. BIC index showed that the graded response models with constrained parameters (i.e., rating scale parameterisation) have a better fit. In particular, the comparison between the bidimensional LC RS-GRM and the bidimensional LC 1P-RS-GRM, based on BIC, led to prefer the 1P-RS-GRM. This model consists in the graded response type model with constraints on both cutoff points (, for all ) and discrimination parameters (, for all ).
Details of the model selection are displayed in
Table 7.
Latent classes and effect of covariates on the class membership. Once the best model was selected, we added individual covariates to understand how individual and disease-related characteristics impact on class membership. The estimated support points for the bidimensional LC 1P-RS-GRM with covariates (see
Table 8) indicated that the latent classes are increasing ordered according to the levels of both
Limitations and
Dysphoria (i.e., estimated support points of the two dimensions increase from class 1 to class 3). Thus, we can interpret the three latent classes in terms of different degrees of CQoL perceived by participants. In particular, Class 1 included subjects who report low levels of both perceived limitations and dysphoria. On the other hand, patients in Class 2 and Class 3 are characterised by medium and high levels of perceived limitations and dysphoria, respectively. Thus, subjects with the highest level of CQoL are located in Class 1, whereas Class 3 includes patients with the lowest level of CQoL. The average of individual-specific weights
is reported in
Table 8 for each class
u (
). Moreover, the differences between the maximum and the minimum value estimated for the support points in each dimension showed that
Dysphoria is the dimension that better discriminates among subjects (i.e., the dimension with the biggest difference equal to 5.79).
In the final selected model, class weights are influenced by individual covariates. Because the support points were increasingly ordered for both the two considered dimensions, we adopted the more parsimonious global logit specification according to Equation (
7) to estimate the effect of covariates on class weights. According to the literature, we added the following variables as covariates: age, social support, age at diagnosis, type of celiac disease, and marital status. Because the type of celiac disease did not result to be significant even for
, it was removed from the final model, whose results are summarised in
Table 9.
We can conclude that the most relevant covariates are social support and age at diagnosis. In particular, for a unit increase in the perceived social support the odds of the latent trait levels (i.e., Limitations and Dysphoria) decrease by 0.95. Moreover, receiving a CD diagnosis in adolescence or adult age rather than in childhood leads to higher levels of perceived limitations due to the CD and dysphoria. About that, odds ratios indicate an increase of 3.53 and 2.64 for adolescence and adult age (vs childhood), respectively. In addition, a weaker impact is associated to age and marital status covariates: older patients present lower levels of perceived limitations and dysphoria (OR = 0.98), and participants who are married or cohabiting report higher latent trait levels (OR = 0.63).
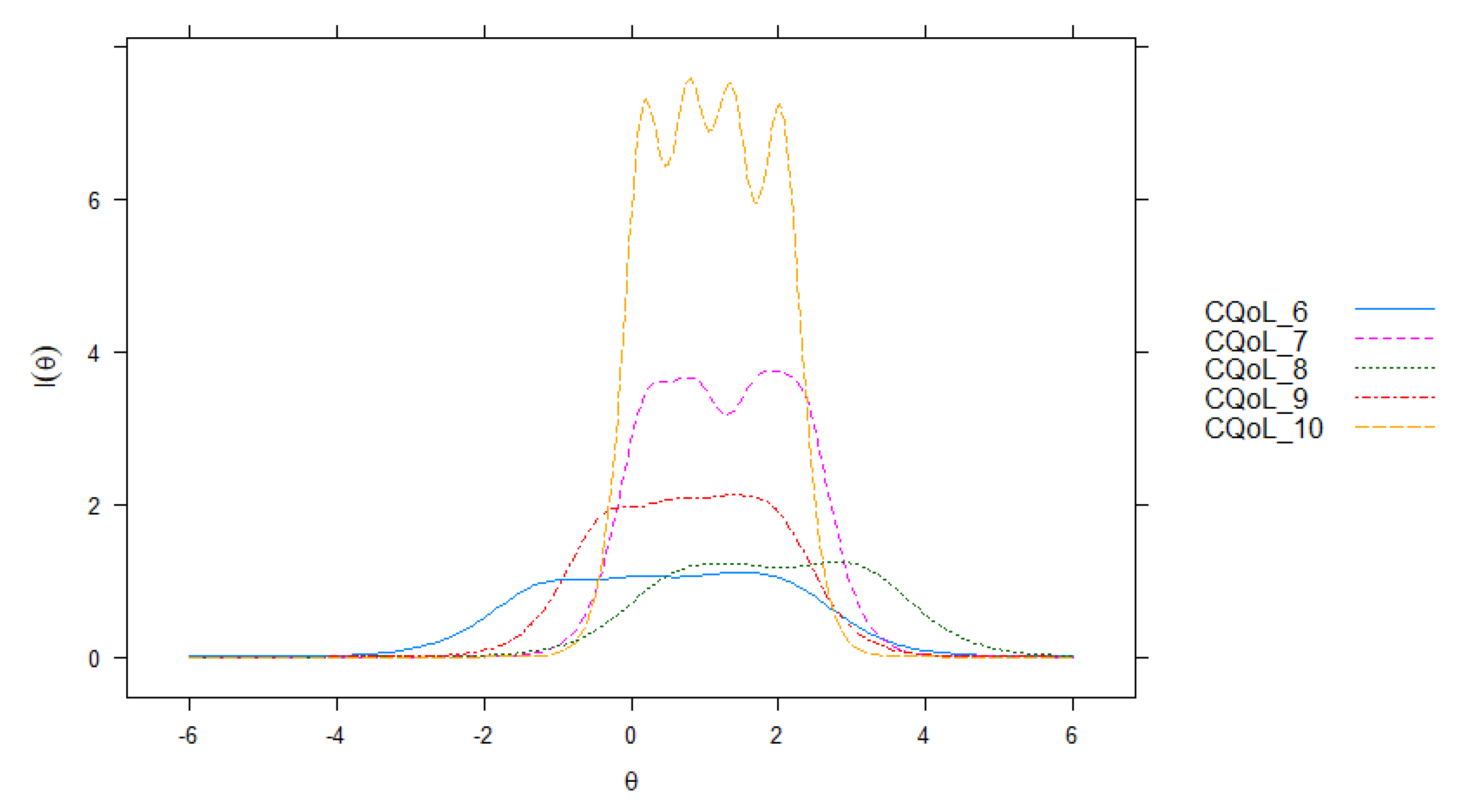
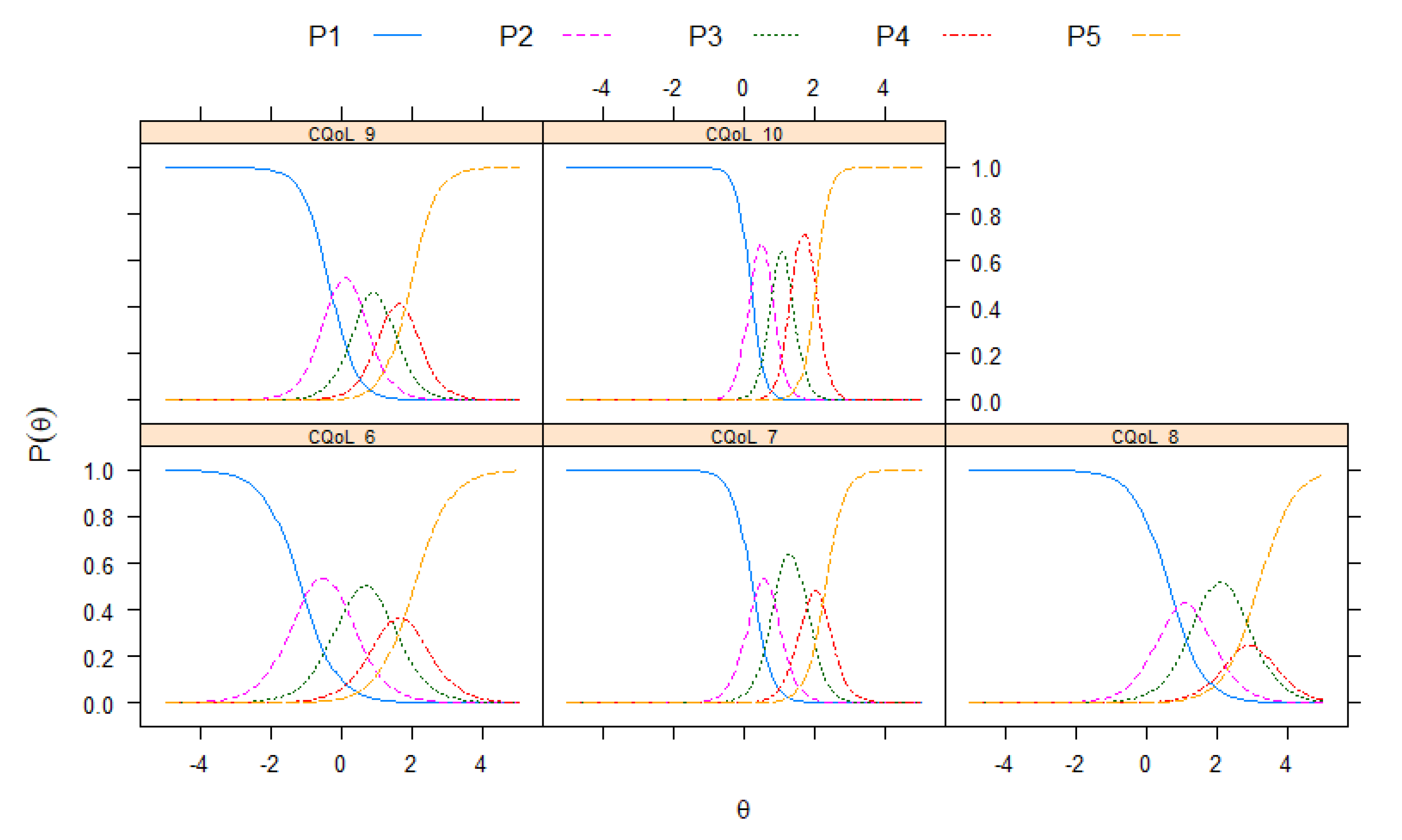
Item difficulties. In
Table 10, we illustrate results regarding the item difficulty parameters. It is worth noting that in the specific context of CQoL, easy items represent the most critical CD-related aspects to be taken into account in support programmes. Indeed, these items are more easily endorsed even for low levels of perceived
Limitations and
Dysphoria. On the other hand, difficult items refer to CD impacts that require high levels of
Limitations and
Dysphoria to be observed.
Concerning dimension Limitations, the easiest items to endorse were CQoL_1 (feeling limited in eating with coworkers) and CQoL_3 (difficulty traveling or taking long trip), whereas the most difficult item was CQoL_5 (feeling worried about the increased risk that a family member has the celiac disease). About dimension Dysphoria, the easiest items to endorse were CQoL_6 (feeling socially stigmatised) and CQoL_9 (not being able to live a normal life), whereas the most difficult item was CQoL_8 (trouble socialising due to the celiac disease). Regarding parameters, results showed that higher levels of Dysphoria are needed to choose categories greater than 1 with respect to the dimension Limitations.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}