
Prevalence of Dementia in Older Adults in Central and Eastern Europe: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
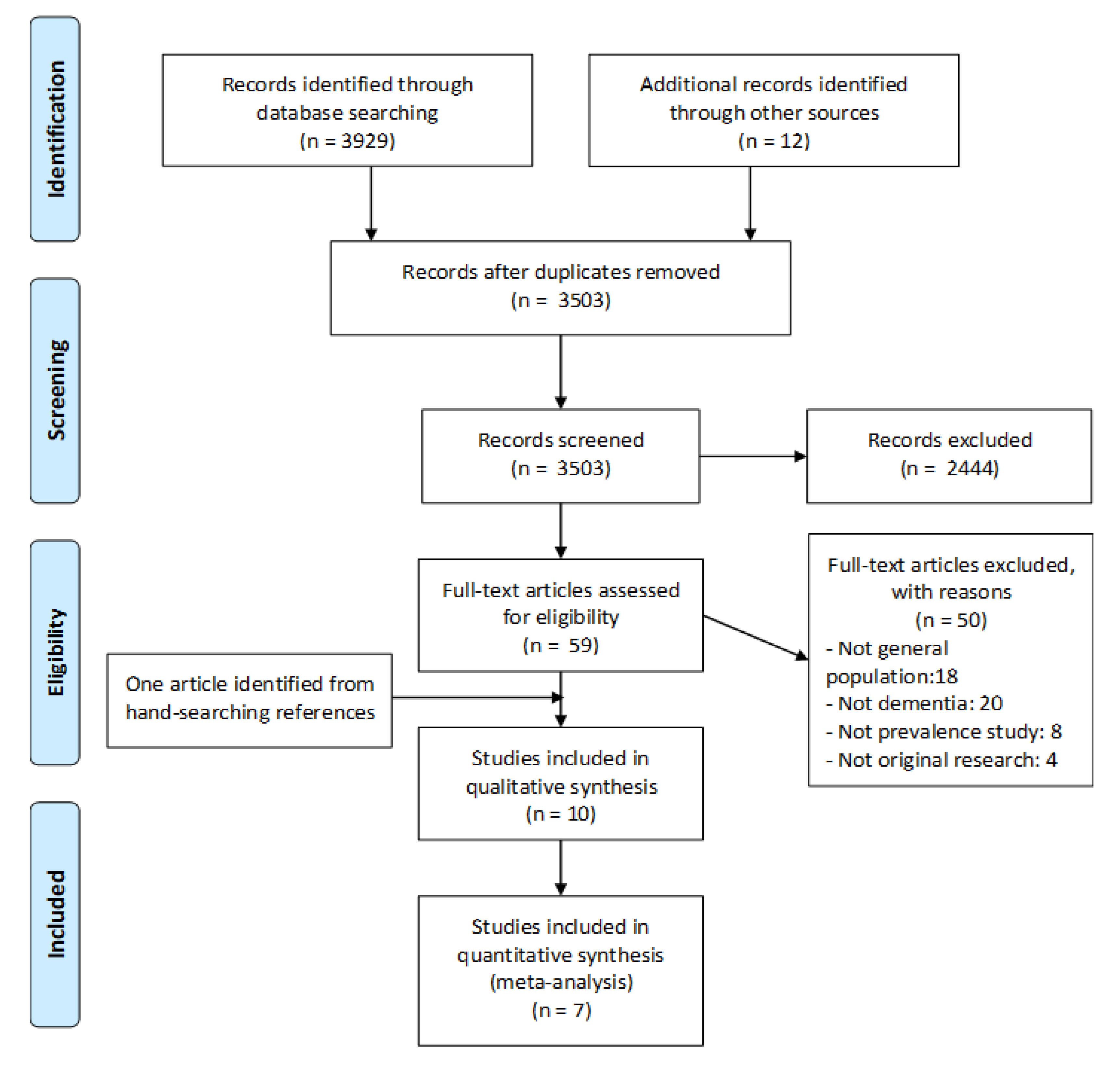
2.1. Search Strategy and Selection Criteria
2.2. Inclusion Criteria
- (1)
- Original research published in peer-reviewed journals or conference abstracts where full data are available.
- (2)
- Population based (i.e., involved a defined “general population”).
- (3)
- Reported prevalence data from Central or Eastern European countries.
- (4)
- Dementia diagnosed by standard criteria such as Diagnostic and Statistical Manual of Mental Disorders (DSM), International Classification of Diseases, Tenth Revision (ICD-10) or clinical interview by trained professionals.
2.3. Exclusion Criteria
- (1)
- Articles about dementia from reversible causes or external causes, or where dementia is a later secondary feature of the disorder, e.g., alcohol or traumatic brain injury, Parkinson’s disease, Huntington’s disease and Creutzfeldt Jakob disease, either sporadic or variant.
- (2)
- Prevalence studies completed in specific populations such as nursing homes, residential care populations, hospital departments or specialist clinics.
- (3)
- Non-original research.
- (4)
- Dementia diagnosed only by cognitive screening instrument.
2.4. Study Selection
2.5. Quality Assessment
2.6. Meta-Analysis
3. Results
3.1. Included Studies
- (a)
- There was no reference to prevalence of dementia reported.
- (b)
- They were not population-based studies.
- (c)
- They were studies about other dementias (secondary or other neurodegenerative conditions).
3.2. Countries
3.3. Sampling Frame
3.4. Diagnostic Procedures
3.5. Quality of Included Papers
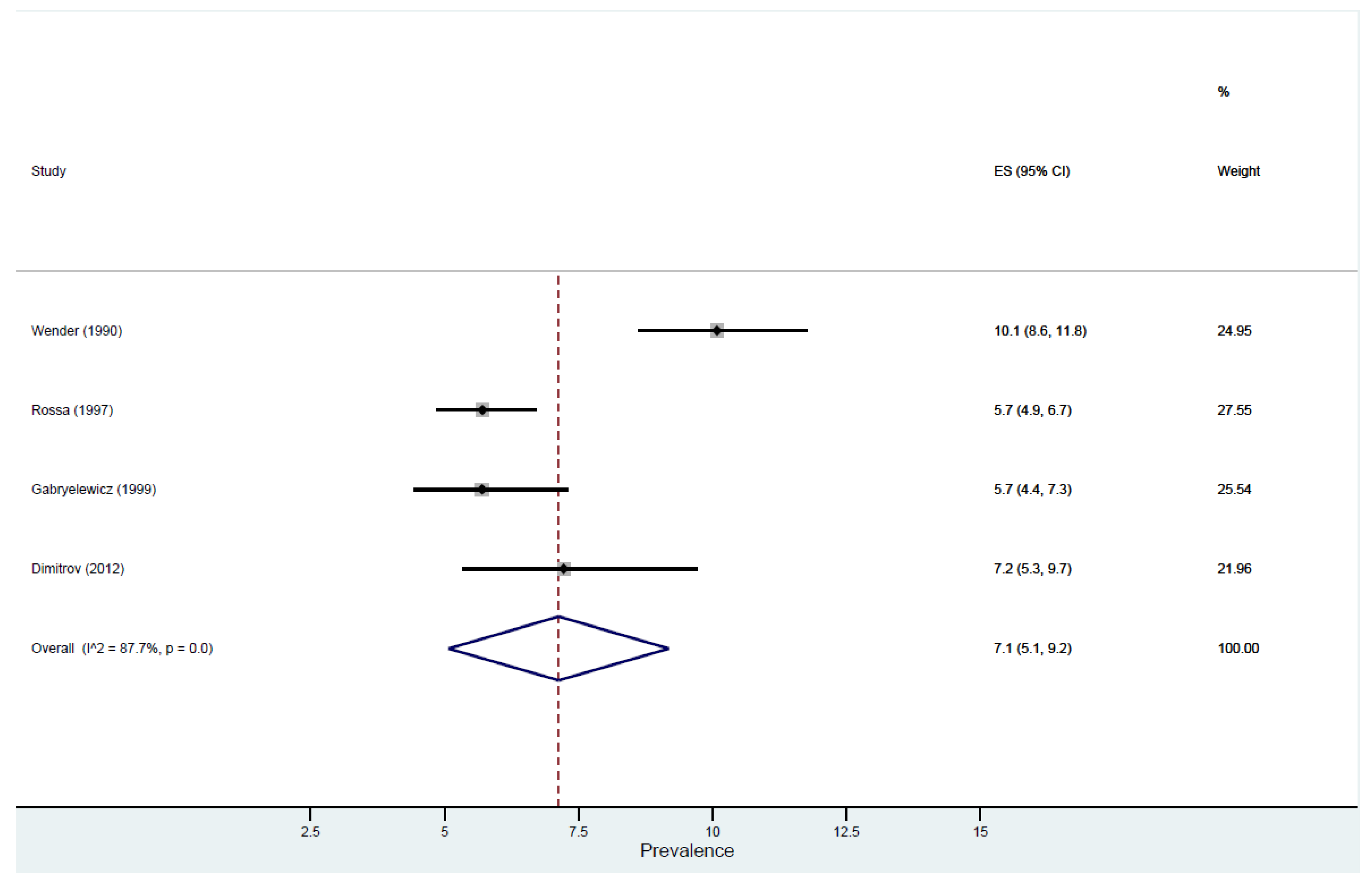
3.6. Prevalence of Dementia
4. Discussion
Strengths and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Terms
- exp *Dementia/or exp *Dementia, Vascular/or exp *Dementia, Multi-Infarct/
- exp *Cognition Disorders/or exp *Dementia/or exp *Alzheimer Disease/
- exp *Cognition Disorders/or exp *Alzheimer Disease/or exp *Dementia/
- exp *Cognition Disorders/or exp *Alzheimer Disease/or exp *Dementia/
- exp *Alzheimer Disease/
- exp *Dementia, Vascular/
- exp *Cognitive Dysfunction/
- 1 or 2 or 3 or 4 or 5 or 6 or 7
- (frequenc* or prevalen* or epidemiolog*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
- 8 and 9
- limit 10 to (abstracts and humans)
- Albania.mp.
- Bosnia.mp. or “Bosnia and Herzegovina”/
- exp *”Bosnia and Herzegovina”/or Herzegovina.mp.
- Bulgaria.mp.
- Croatia.mp.
- Czech republic.mp.
- Hungary.mp.
- exp *”Macedonia (Republic)”/or Macedonia.mp.
- Montenegro.mp.
- Poland.mp.
- Romania.mp.
- Serbia.mp. or exp *Yugoslavia/
- Slovakia.mp. or exp *Czechoslovakia/
- Slovenia.mp.
- Belarus.mp. or exp *”Republic of Belarus”/
- estonia.mp.
- Latvia.mp.
- Lithuania.mp.
- Moldova.mp.
- Russia.mp.
- Russian federation.mp.
- Ukraine.mp.
- 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33
- 8 and 11 and 34
- dementia.mp.
- alzheimer.mp.
- “Alzheimer’s disease”.mp.
- “Alzheimer disease”.mp.
- “Alzheimer dementia”.mp.
- “Vascular Dementia”.mp.
- “Cognitive impairment”.mp.
- “Mixed Dementia”.mp.
- VaD.mp.
- AD.mp.
- 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45
- 9 and 34 and 46
- limit 47 to abstracts
- exp *Dementia/or exp *Dementia, Vascular/or exp *Dementia, Multi-Infarct/
- exp *Cognition Disorders/or exp *Dementia/or exp *Alzheimer Disease/
- exp *Cognition Disorders/or exp *Alzheimer Disease/or exp *Dementia/
- exp *Cognition Disorders/or exp *Alzheimer Disease/or exp *Dementia/
- exp *Alzheimer Disease/
- exp *Dementia, Vascular/
- exp *Cognitive Dysfunction/
- 49 or 50 or 51 or 52 or 53 or 54 or 55
- (frequenc* or prevalen* or epidemiolog*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (
- 56 and 57
- limit 58 to (abstracts and humans)
Appendix B. Prevalence Critical Appraisal Instrument. (Munn at al., 2014)
- Was the Sample Representative of the Target Population?
- 2.
- Were Study Participants Recruited in an Appropriate Way?
- 3.
- Was the Sample Size Adequate?
- n = sample size
- Z = Z statistic for a level of confidence
- p = Expected prevalence or proportion (in proportion of one; if 20%, P = 0.2)
- d = precision (in proportion of one; if 5%, d = 0.05)
- 4.
- Were the Study Subjects and Setting Described in Detail?
- 5.
- Is the Data Analysis Conducted with Sufficient Coverage of the Identified Sample?
- -
- Did the authors describe the reasons for non-response and compare persons in the study to those not in the study, particularly with regards to their socio-demographic characteristics?
- -
- Could the not-responders have led to an underestimate of prevalence of the disease or condition under investigation?—If reasons for non-response appear to be unrelated to the outcome measured and the characteristics of non-responders are comparable to those in the study, the researchers may be able to justify a more modest response rate.
- -
- Did the means of assessment or measurement negatively affect the response rate (measurement should be easily accessible, conveniently timed for participants, acceptable in length, and suitable in content).
- 6.
- Were Objective, Standard Criteria Used for Measurement of the Condition?
- 7.
- Was the Condition Measured Reliably?
- -
- Has the researcher justified the methods chosen?
- -
- Has the researcher made the methods explicit? (For interview method, how were interviews conducted?)
- 8.
- Was There Appropriate Statistical Analysis?
- 9.
- Are All Important Confounding Factors/Subgroups/Differences Identified and Accounted for?
- 10.
- Were Subpopulations Identified Using Objective Criteria?
Appendix C. Table of Studies Excluded with Reason
| Author | Study | Reason for Exclusion |
| Auer, S., Linsmayer, E., Berankova, A., Pascher, P., Firlinger, B., Prischl, D., … Holmerova, I. (2017) | DEMDATA: The Austrian-Czech institutional long-term care project—design and protocol of a two-centre cross sectional study. | Not General Population |
| Auer, S. R., Hofler, M., Linsmayer, E., Berankova, A., Prieschl, D., Ratajczak, P., … Holmerova, I. (2018) | Cross-sectional study of prevalence of dementia, behavioural symptoms, mobility, pain and other health parameters in nursing homes in Austria and the Czech Republic: results from the DEMDATA project. | Not General Population |
| Kijowska, V., & Szczerbinska, K. (2018) | Prevalence of cognitive impairment among long-term care residents: a comparison between nursing homes and residential homes in Poland. | Not General Population |
| Dobrzyn-Matusiak, D., Marcisz, C., Bak, E., Kulik, H., & Marcisz, E. (2014) | Physical and mental health aspects of elderly in social care in Poland | Not General Population |
| Sutovsky, S., Klobucnikova, K., Volarikova, V., & Turcani, P. (2012). | The ussian assisted living study: Prevalence, recognition and treatment of dementia, parkinsonism and depression in the assisted living population | Not General Population |
| Sutovsky, S., Kralova, M., Siarnik, P., & Turcani, P. (2018) | Prevalence, Recognition, and Treatment of Dementia in Assisted Living Facilities | Not General Population |
| Sutovsky, S., & Turcani, P. (2015) | Prevalence, recognition and treatment of parkinsonism, dementia and depression in the assisted living population of Slovakia. | Not General Population |
| Trifonov, E. G., & Ognev, A. E. (1997). | The geriatric psychiatric day hospital: an analysis of 5 years of activities. | Not General Population |
| Turcani, P., & Sutovsky, S. (2014). | The Slovakia assisted living study: Two cross-sectional studies of prevalence, recognition, and treatment of dementia and depression in the assisted living population of Slovakia. | Not General Population |
| Bidzan, L., & Turczynski, J. (2005). | Environment and cognitive functions in a population 60 years and older. | Studies on Cognitive Decline |
| Bidzan, L., Turczynski, J., & Szabert, K. (2009) | Prevalence of MCI in a population from area near Gdansk. | Studies on Cognitive Decline |
| Formanek, T., Kagstrom, A., Winkler, P., & Cermakova, P. (2019). | Differences in cognitive performance and cognitive decline across European regions: a population-based prospective cohort study. | Studies on Cognitive Decline |
| Gabryelewicz, T., Styczynska, M., Luczywek, E., Barczak, A., Pfeffer, A., Androsiuk, W., … Barcikowska, M. (2007). | The rate of conversion of mild cognitive impairment to dementia: predictive role of depression. | Studies on Cognitive Decline |
| Gurgu, M., Zamfirescu, A., Stroie, A. M., & Aurel, R. (2012). | Cognitive impairment prevalence and correlations with subjective memory impairment: Findings from Brasov, Romania. | Studies on Cognitive Decline |
| Gurina, N., Frolov, E., Isaeva, T., Korystina, E., Zelenukha, D., Tadjibaev, P., & Degryse, J. (2010). | Aging in Russia: The results of crystal project in the St-Petersburg district. | Studies on Cognitive Decline |
| Gurina, N. A., Frolova, E. V., & Degryse, J. M. (2011). | A roadmap of aging in Russia: the prevalence of frailty in community-dwelling older adults in the St. Petersburg district—the “Crystal” study. | Studies on Cognitive Decline |
| Knasiene, J., Legotaite, G., & Damuleviciene, G. (2016) | Characteristics of cognitive disorders of the older patients visiting the Memory clinic for the first time | Studies on Cognitive Decline |
| Klich-Rączka, A., Piotrowicz, K., Mossakowska, M., Skalska, A., Wizner, B., Broczek, K.,... & Grodzicki, T. (2014). | The assessment of cognitive impairment suspected of dementia in Polish elderly people: results of the population based PolSenior Study. | Studies on Cognitive Decline |
| Makeeva, O. A., Romero, H. R., Markova, V. V., Melikyan, Z. A., Zhukova, I. A., Minaycheva, L. I., … Welsh-Bohmer, K. (2015). | Ascular risk factors confer domainspecific deficits in cognitive performance within an elderly ussian population. | Studies on Cognitive Decline |
| Motyl, R., Slowik, A., Turaj, W., Szczudlik, A., & Pajak, A. (1998). | Cognitive impairment and cardiovascular disease risk factors. Project CASCADE Krakow. VI. Magnetic resonance imaging of the aging brain in elderly persons (65–78 years old). | Studies on Cognitive Decline |
| Pomykalska, E., Pajak, A., & Szczudlik, A. (1998). | Cognitive impairment and cardiovascular disease risk factors. Project CASCADE Krakow. II. Agreement of Mini-Mental State Examination (MMSE) obtained by nurses and by psychologists from the same persons at age 67-78 years of age. | Studies on Cognitive Decline |
| Orlowiejska-Gillert, M., Pajak, A., Szczudlik, A., Kawalec, E., & Pomykalska, E. (1998). | Cognitive impairment and cardiovascular disease risk factors. Project CASCADE Krakow. III. Assessment of cognitive function in elderly women and men (65–78 years old). | Studies on Cognitive Decline |
| Pajak, A., Kawalec, E., Pomykalska, E., Topor-Madry, R., Orlowiejska-Gillert, M., & Szczudlik, A. (1998). | Cognitive impairment and cardiovascular disease risk factors. Project CASCADE Krakow. IV. Prevalence of cognitive impairment in relation to age, sex, education and history of myocardial infarction in men and women at age 65–78, residents of a rural province in Poland | Studies on Cognitive Decline |
| Parnowski T, Gabryelewicz T, Matuszewska E, Jarkiewicz J. 1993. | Prevalence of the dementia syndrome among elderly people in an urban area. A pilot study. | Study on Cognitive Decline |
| Sipos, K., Bodo, M., May, Z., Lendvai, B., Piros, A., Spitzer, N., … Banyasz, A. (2008). | Risk of mental disorders, their changes and somatic consideration in rural Hungary. | Studies on Cognitive Decline |
| Szczudlik, A., Slowik, A., Turaj, W., Orlowiejska-Gillert, M., Motyl, R., Topor-Madry, R., & Pajak, A. (1998). | Cognitive impairment and cardiovascular disease risk factors. Project CASCADE Krakow. V. Disorders of higher cerebral functions in elderly people (65–78 years old). | Studies on Cognitive Decline |
| Tkacheva, O. N., Runikhina, N. K., Ostapenko, V. S., Sharashkina, N. V., Mkhitaryan, E. A., Onuchina, J. S., … Press, Y. (2018). | Prevalence of geriatric syndromes among people aged 65 years and older at four community clinics in Moscow | Studies on Cognitive Decline |
| Tkacheva, O. N., Runikhina, N. K., Yakhno, N. N., Mkhitaryan, E. A., Ostapenko, V. S., Shrashkina, N. V., & Savushkina, I. Y. (2016). | High prevalence of cognitive impairment in elderly subjects in primary care. | Studies on Cognitive Decline |
| Gavrilov, S. I., & Kirzhanova, V. V. (1983) | Incidence of mental disorders among the late middle-aged and elderly population (according to the primary registration data of the psychoneurologic institutions of Moscow). | Incidence Study |
| Cornutiu, G. (2010). | The incidence and prevalence of Alzheimer’s disease | Literature Review |
| Gavrilova, S. I., & Bratsun, A. L. (1999). | Epidemiology and risk factors of Alzheimer’s disease. | Literature Review |
| Kiejna, A., Frydecka, D., Adamowski, T., Bickel, H., Reynish, E., Prince, M., … Georges, J. (2011). | Epidemiological studies of cognitive impairment and dementia across Eastern and Middle European countries (Epidemiology of Dementia in Eastern and Middle European Countries). | Literature Rivew |
| Ersek, K., Karpati, K., Kovacs, T., Csillik, G., Gulacsi, A. L., & Gulacsi, L. (2010). | [Epidemiology of dementia in Hungary]. | Literature Review |
| Leel-Ossy, L. (1995). | Incidence of Alzheimer’s dementia in homes for the elderly. | Incidence Study |
| Trascu, R. I., & Spiru, L. (2011). | Is Alzheimer’s crisis adequately perceived in Romania? | No Prevalence Study |
| Sova, M. R., Dobrin, R. P., & Chirita, V. (2009) | Aspects regarding the incidence and prevalence of vascular dementia forms]. | No Prevalence Study |
| Iova, A., Mihancea, P., & Sabau, M. (2009). | General aspects of the morbidity in Alzheimer’s dementia during 2003-2005 at the Neurology and Psychiatry Clinical Hospital Oradea. | Not General Population |
| Klich-Raczka, A., Dubiel, M., Sulicka, J., Zyczkowska, J., & Pitucha, M. (2006). | Comprehensive geriatric assessment in hospitalized patients aged 80 years and more. | Not General Population |
| Klimkowicz, A., Dziedzic, T., Slowik, A., & Szczudlik, A. (2002). | Incidence of pre- and poststroke dementia: cracow stroke registry. | Not General Population |
| Klimkowicz-Mrowiec, A., Dziedzic, T., Stowik, A., & Szczudlik, A. (2006). | Predictors of Poststroke Dementia: Results of a Hospital-Based Study in Poland. | Not General Population |
| Kovacs, G. G., Kovari, V., & Nagy, Z. (2008). | Frequency of different forms of dementia at the Department of Neuropathology of the Hungarian National Institute of Psychiatry and Neurology during a 3-year period. | Not General Population |
| Dumitru, M. M., Chirita, V., & Chirita, R. (2014). | Characteristics of early onset dementia in a hospital setting from Romania. | Not General Population |
| Dimitrov, I., Kaprelyan, A., Usheva, N., & Ivanov, B. (2015). | Alzheimer’s disease outpatient referrals to a dementia centre: Diagnostic challenges. | Not General Population |
| Catipovic, V., Drobac, R., & Slijepcevic, M. K. (2004). | [Epidemiological study of psychiatric hospitalizations in Bjelovar General Hospital]. | Not General Population |
| Pecotic, Z., & Pandzic, M. (2000). | The age and sex of hospitalized demented patients. | Not General Population |
| Togoj, A. (2008). | Care for people with dementia in Slovenia | No Prevalence Study |
| Bartos, A., & Raisova, M. (2016) | The Mini-Mental State Examination: Czech Norms and Cutoffs for Mild Dementia and Mild Cognitive Impairment due to Alzheimer’s Disease | No Prevalence Studies |
| Gabryelewicz, T., Kotapka-Minc, S., Maczka, M., Motyl, R., Sobow, T., Szczudlik, A., … Barcikowska, M. (2006) | The characteristic of Polish population Alzheimer’s disease patients and their caregivers: Results from observation EX-ON study | No Prevalence Studies |
| Macijauskiene, J., & Engedal, K. (2005) | Medico social care for persons suffering from Alzheimer’s disease and related disorders | No Prevalence Studies |
References
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.C.; Wu, Y.T.; Prina, M. World Alzheimer Report 2015. In The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost & Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Wortmann, M. Dementia: A global health priority-highlights from an ADI and World Health Organization report. Alzheimer’s Res. Ther. 2012, 4, 40. [Google Scholar] [CrossRef] [Green Version]
- Sousa, R.M.; Ferri, C.P.; Acosta, D.; Albanese, E.; Guerra, M.; Huang, Y.; Jacob, K.S.; Jotheeswaran, A.T.; Rodriguez, J.J.L.; Pichardo, G.R.; et al. Contribution of chronic diseases to disability in elderly people in countries with low and middle incomes: A 10/66 Dementia Research Group population-based survey. Lancet 2009, 374, 1821–1830. [Google Scholar] [CrossRef] [Green Version]
- Wimo, A.; Jönsson, L.; Bond, J.; Prince, M.; Winblad, B.; International, A.D. The worldwide economic impact of dementia 2010. Alzheimer’s Dement. 2013, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Suh, G.H.; Shah, A. A review of the epidemiological transition in dementia-cross-national comparisons of the indices related to Alzheimer’s disease and vascular dementia. Acta Psychiatr. Scand. 2001, 104, 4–11. [Google Scholar] [CrossRef]
- Hofman, A.; Rocca, W.A.; Brayne, C.; Breteler, M.M.B.; Clarke, M.; Cooper, B.; Copeland, J.R.M.; Dartigues, J.F.; Droux, A.D.S.; Hagnell, O.; et al. The prevalence of dementia in Europe: A collaborative study of 1980–1990 findings. Int. J. Epidemiol. 1991, 20, 736–748. [Google Scholar] [CrossRef] [PubMed]
- Lobo, A.; Launer, L.J.; Fratiglioni, L.; Andersen, K.; Di Carlo, A.; Breteler, M.M.B.; Copeland, J.R.M.; Dartigues, J.F.; Jagger, C.; Martinez-Lage, J.; et al. Prevalence of dementia and major subtypes in Europe: A collaborative study of population-based cohorts. Neurology 2000, 54, S4. [Google Scholar]
- Reynish, E.; Fratiglioni, L.; Prince, M.; Bickel, H.; Kiejna, A.; Georges, J. EUROCODE: Report of WP7 2006. Prevalence of Dementia in Europe. Alzheimer Eur. 2006. [Google Scholar]
- Bacigalupo, I.; Mayer, F.; Lacorte, E.; Di Pucchio, A.; Marzolini, F.; Canevelli, M.; Di Fiandra, T.; Vanacore, N. A systematic review and meta-analysis on the prevalence of dementia in Europe: Estimates from the highest-quality studies adopting the DSM IV diagnostic criteria. J. Alzheimer’s Dis. 2018, 66, 1471–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galeotti, F.; Giusti, A.; Meduri, F.; Raschetti, R.; Scardetti, P.; Vanacore, N. Epidemiological data on dementia. In ALCOVE (Alzheimer Cooperative Valuation in EUROPE) Synthesis Report; ALCOVE: Rome, Italy, 2013. [Google Scholar]
- Kiejna, A.; Frydecka, D.; Adamowski, T.; Bickel, H.; Reynish, E.; Prince, M.; Caracciolo, B.; Fratiglioni, L.; Georges, J. Epidemiological studies of cognitive impairment and dementia across Eastern and Middle European countries (epidemiology of dementia in Eastern and Middle European Countries). Int. J. Geriatr. Psychiatry 2011, 26, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Bank, T.W. Gross Domestic Product 2018. Available online: https://databank.worldbank.org/data/download/GDP.pdf (accessed on 14 October 2020).
- Eurostat. Quality of life in Europe-Facts and Views-Health. Available online: https://ec.europa.eu/eurostat/statistics-explained/pdfscache/39269.pdf (accessed on 14 October 2020).
- Busse, R.; Blümel, M. Tackling Chronic Disease in Europe: Strategies, Interventions and Challenges; WHO Regional Office Europe: Copenhagen, Denmark, 2010. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Moola, S.; Riitano, D.; Lisy, K. The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int. J. Health Policy Manag. 2014, 3, 123. [Google Scholar] [CrossRef] [Green Version]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bdzan, L.; Turczyński, J.; Szabert, K. Prevalence of dementia in a rural population. Psychiatr. Pol. 2007, 41, 181–188. [Google Scholar] [PubMed]
- Bidzan, L.; Turczyński, J. Environment and cognitive functions in a population 60 years and older. Psychiatr. Pol. 2005, 39, 1211–1218. [Google Scholar] [PubMed]
- Gavrilova, S.; Sudareva, L.; Kalyn, I. Epidemiology of dementias in the middle-aged and elderly. Zhurnal Nevropatologii Psikhiatrii Imeni SS Korsakova (Moscow, Russia, 1952) 1987, 87, 1345–1352. [Google Scholar]
- Wender, M.; Mularczyk, J.; Modestowicz, R. Epidemiology of Alzheimer’s disease in the selected region of Wielkopolska (town and commune Steszew). Prz. Epidemiol. 1990, 44, 215–221. [Google Scholar]
- Rossa, G. The prevalence of Alzheimer’s type dementia and vascular dementia in the district of Swiebodzin. Psychiatr. Pol. 1997, 31, 121–134. [Google Scholar]
- Gabryelewicz, T. The prevalence of dementia in the population of the Warsaw district of Mokotow from 65 to 84 years of age. Psychiatr. Pol. 1999, 33, 353–366. [Google Scholar]
- Kruja, J.; Rakacolli, M.; Prifti, V.; Buda, L.; Agolli, D. Epidemiology of dementia in Tirana, Albania. In Proceedings of the 6th congress of the European Federation of Neurological Societies, Vienna, Austria, 26–30 October 2002; Volume 9, p. 161. [Google Scholar]
- Stefanova, E.; Pekmezovic, T.; Nalic, D.; Kostic, V.S. The diagnosis of dementia is unspecified–report of a pilot survey of dementia in Belgrade. Gerontology 2004, 50, 260–261. [Google Scholar] [CrossRef]
- Pfeffer, A.; Chodakowska, M.; Czyżewski, K.; Gabryelewicz, T.; Łuczywek, E.; Mossakowska, M.; Broczek, K.; Barcikowska, M. The prevalence of Dementia in Warsaw centenarians: A population–based study. Postępy Nauk Med. 2011, 25, 28–33. [Google Scholar]
- Dimitrov, I.; Tzourio, C.; Milanov, I.; Deleva, N.; Traykov, L. Prevalence of dementia and mild cognitive impairment in a Bulgarian urban population. Am. J. Alzheimer’s Dis. Other Dement. 2012, 27, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Kruja, J.; Beghi, E.; Zerbi, D.; Dobi, D.; Kuqo, A.; Zekja, I.; Mijo, S.; Kapisyzi, M.; Messina, P. High prevalence of major neurological disorders in two Albanian communities: Results of a door-to-door survey. Neuroepidemiology 2012, 38, 138–147. [Google Scholar] [CrossRef]
- Niu, H.; Álvarez-Álvarez, I.; Guillén-Grima, F.; Aguinaga-Ontoso, I. Prevalence and incidence of Alzheimer’s disease in Europe: A meta-analysis. Neurología (Engl. Ed.) 2017, 32, 523–532. [Google Scholar] [CrossRef]
- Fiest, K.M.; Roberts, J.I.; Maxwell, C.J.; Hogan, D.B.; Smith, E.E.; Frolkis, A.; Cohen, A.; Kirk, A.; Pearson, D.; Pringsheim, T. The prevalence and incidence of dementia due to Alzheimer’s disease: A systematic review and meta-analysis. Can. J. Neurol. Sci. 2016, 43, S51–S82. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimer’s Dement. 2013, 9, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.T.; Beiser, A.S.; Breteler, M.M.; Fratiglioni, L.; Helmer, C.; Hendrie, H.C.; Honda, H.; Ikram, M.A.; Langa, K.M.; Lobo, A. The changing prevalence and incidence of dementia over time: Current evidence. Nat. Rev. Neurol. 2017. [Google Scholar] [CrossRef] [Green Version]
- Naing, L.; Winn, T.; Rusli, B.N. Practical issues in calculating the sample size for prevalence studies. Arch. Orofac. Sci. 2006, 1, 9–14. [Google Scholar] [CrossRef]
- Daniel, W.W. Biostatistics: A Foundation for Analysis in the Health Sciences, 7th ed.; John Wiley & Sons: New York, NY, USA, 1999. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Author/Year of Publication | Country (Region) | Age Range | Sample Size | Sampling Frame/Design | Screening and Diagnostic Procedures | Dementia Prevalence (M-Males/F-Females) | Dementia Subtypes | Quality Score |
|---|---|---|---|---|---|---|---|---|
| Bdzan and Turczynski, 2005; Bdzan et al., 2007 [18] | POLAND (rural communities) | ≥60 | 1000 | Random selection from city registers Two-phase study | Screening: MMSE Diagnostic criteria: ICD-10 | All-cause dementia 6.7% (M: 3.0%/F: 8.8%) | AD 44.8% VaD: 44.8% | 9 |
| Gavrilova et al., 1987 [20] | RUSSIA | ≥60 | 2097 | Unclear sampling One-phase study | Clinical interview | All-cause dementia 5.5% | - | 1 |
| Wender et al., 1990 [21] | POLAND (Town and commune Steszew) | ≥45 | Total = 3741 <65: n = 2323 ≥65: n = 1418 | Patients from GP registers Two-phase study | Screening: MMSE, MSQ, SPMSQ Diagnostic criteria: DSM–III–R | Probable Alzheimer’s Dementia: ≥65: 1.1% ≥65: 10.1% | - | 3 |
| Rossa, 1997 [22] | POLAND (District Swiebodzin) | ≥45 | 7417 <65: n = 4999 ≥65: n = 2418 | Municipal registers Two-phase study | Screening: CAMDEX Diagnostic criteria: DSM–III–R | All-cause dementia ≥45 3.6% (M: 2.3%/F: 4.5%) All-cause dementia ≥65 5.7% (M: 3.4%/F:7.0%) * | AD ≥65: 56.1% | 5 |
| Gabryelewicz, 1999 [23] | POLAND (Warsaw district Mokotow) | 65–84 | 1000 | Random selection from city registers Two-phase study | GDS ICD-10: for diagnosis of dementia and for differential diagnosis, DSM-IV: for mixed dementia MMSE | All-cause dementia 5.7% (M: 4.3%/F: 6.6%) 65–69: 1.9% 70–74: 5.8% 75–79: 8.6% 80–84: 16.5% | - | 8 |
| Kruja, 2002 [24] | ALBANIA (Tirana City) | ≥60 | 3521 | Random selection from city registers Two-phase study | Screening: MMSE Diagnostic criteria: ICD-10 | All-cause dementia 7.8% (M: 4.8%/F: 11.5%) 60–64: 2.1% 65–69: 6.3% 70–74: 7.2% 74–79: 12.5% 80–85: 36.4% >85: 45.2% | - | 7 |
| Stefanova et al., 2004 [25] | SERBIA (data from 16 public health centres) | - | 1000 | GP record survey One-phase study | ICD-10 | All-cause dementia 6.7% (M: 2.8%/F: 3.9%) | - | 4 |
| Pffefer et al., 2012 [26] | POLAND (Warsaw) | >100 | 83 | Municipal registers Two-phase study | Screening: MMSE, 6-CIT, GDS, BCRS Diagnostic criteria: DSM-IV | All-cause dementia 66.3% (M:50%, F:69%) | AD 74.5% VaD 18.1% | 6 |
| Dimitrov et al., 2012 [27] | BULGARIA (Varna city) | ≥65 | 540 | Random sample of patients on GP registers Two-phase study | Screening: MMSE, MIS, IADL Diagnostic criteria: DSM-IV | All-cause dementia 7.2% (95% CI 5.0–9.4) | AD 43.1% VaD 27.8% Mixed 18.1% DLB 5.6% | 9 |
| Kruja et al., 2012 [28] | ALBANIA (Cities of Tirana and Saranda | 1–91 | 9869 | Random selection from city registers Two-phase study | Screening: MMSE Diagnostic criteria: DSM-IV | All-cause dementia 1.0% (95% CI 0.8–1.2) (M:0.8%, F: 1.1%) | - | 7 |
| Study Author and Year | Q1 Was the Sample Representative of Target Population? | Q2 Were Study Participants Recruited in an Appropriate Way? | Q3 Was the Sample Size Adequate? | Q4 Were the Study Subjects and Setting Described in Detail? | Q5 Is the Data Analysis Conducted with Sufficient Coverage of the Identified Sample? | Q6 Were Objective, Standard Criteria Used for Measurement of the Condition? | Q7 Was the Condition Measured Reliably? | Q8 Was There Appropriate Statistical Analysis? | Q9 Are All Important Confounding Factors/Subgroups/Differences Identified and Accounted for? | Q10 Were Subpopulations Identified Using Objective Criteria? | Scoring |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bidzan (2007) [18] | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 9 |
| Gavrilova (1987) [20] | Yes | Not clear | No | No | No | Not clear | No | No | No | No | 1 |
| Wender (1990) [21] | No | No | No | Yes | No | Yes | Yes | Not clear | No | No | 3 |
| Rossa (1997) [22] | Yes | Yes | No | No | No | Yes | Yes | Yes | No | No | 5 |
| Gabryelewicz (1999) [23] | Yes | Yes | No | Yes | Not clear | Yes | Yes | Yes | Yes | Yes | 8 |
| Kruja (2002) [24] | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | No | 7 |
| Stefanova (2004) [25] | Yes | Yes | No | No | No | Yes | Yes | No | No | No | 4 |
| Pfeffer (2012) [26] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | No | 6 |
| Dimitrov (2012) [27] | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 9 |
| Kruja (2012) [28] | Yes | Yes | No | No | Yes | Yes | Yes | Yes | No | Yes | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cenko, B.; Ozgo, E.; Rapaport, P.; Mukadam, N. Prevalence of Dementia in Older Adults in Central and Eastern Europe: A Systematic Review and Meta-Analysis. Psychiatry Int. 2021, 2, 191-210. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2020015
Cenko B, Ozgo E, Rapaport P, Mukadam N. Prevalence of Dementia in Older Adults in Central and Eastern Europe: A Systematic Review and Meta-Analysis. Psychiatry International. 2021; 2(2):191-210. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2020015
Chicago/Turabian StyleCenko, Blerta, Emilia Ozgo, Penny Rapaport, and Naaheed Mukadam. 2021. "Prevalence of Dementia in Older Adults in Central and Eastern Europe: A Systematic Review and Meta-Analysis" Psychiatry International 2, no. 2: 191-210. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2020015