
A Geminated Mandibular Second Molar—A Case Report


1
Meadow Walk Dental Practice, 1b Meadow Walk, Buckingham MK18 1RS, UK
2
Bristol Dental School, Lower Maudlin Street, Bristol BS1 2LY, UK
*
Author to whom correspondence should be addressed.
Reports 2021, 4(4), 31; https://0-doi-org.brum.beds.ac.uk/10.3390/reports4040031
Submission received: 23 April 2021
/
Revised: 22 September 2021
/
Accepted: 23 September 2021
/
Published: 27 September 2021
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Fusion and gemination are not entirely uncommon dental anomalies that may also be named ‘double teeth’. This is due to their unusual presentation in a twin-like fashion. Teeth with these irregularities may appear clinically similar, presenting as large and bulbous in shape with unusual anatomy and fissure patterns. The exact aetiology of these anomalies is uncertain, but many potential local or systemic disturbances during the morphodifferentiation stage of odontogenesis have been considered. Gemination occurs rarely in the permanent dentition and even less frequently in the posterior region of the oral cavity. This report presents a case of a geminated mandibular second molar and discusses the importance of early recognition and diagnosis of such teeth so that adequate preventative care and treatment can be provided.
1. Introduction
Abnormalities within the human dentition may present in various forms. These include irregularities in the number, size, shape, or structure of teeth, and occur as a result of disturbances during odontogenesis [1,2]. Fusion and gemination are anomalies that can show disparity from the norm within all these domains. Tooth gemination presents as two completely or partially separated crowns stemming from a single shared root (see Figure 1a,b). This occurs as result of the division of a single tooth bud [2,3]. Fusion, however, whilst clinically similar to gemination, consists of the joining of two separate tooth buds during tooth development. This results in a large, conjoined crown deriving from individual roots (see Figure 2a,b).
Teeth that have undergone fusion or gemination present most commonly in primary teeth at a prevalence rate of 0.5%, whilst in the permanent dentition, these anomalies occur at a rate of 0.1%. Anterior teeth are more frequently affected, and the clinical manifestation of this anomaly varies considerably from a minor notch in the incisal edge of an abnormally wide incisor to the appearance of almost two separate crowns. Gemination is more commonly seen the in maxillary arch, whilst fusion is more commonly seen in the mandibular arch. Teeth in the lower jaw are also more commonly affected, whilst incidence levels appear to be equal between the sexes [4].
The irregular structure of these teeth can cause them to be the subject of higher caries and periodontal risks, whilst also posing occlusal, functional, and aesthetic difficulties for patients (especially when anterior teeth are affected) [2]. When affecting the primary dentition, eruptive disturbance of successional teeth can also be problematic [4]. As a result, both fused and geminated teeth can present numerous restorative challenges to the dentist. This can include complex endodontic work, difficulty in recreating intricate and unusual anatomy for direct restorations, difficulty in achieving an aesthetic result acceptable to the patient and hardship in achieving adequate periodontal hygiene for the patient [5]. A multidisciplinary approach may be required for especially complex cases [6].
2. Case Presentation
A 61-year-old woman presented to the primary care dental clinic of one of the authors (A.P.) for a routine examination. Medically, she had suffered from cancer of the womb 5 years previously and subsequently was treated with a hysterectomy. She had no other relevant medical history, no allergies, was a non-smoker and rarely drank alcohol. She complained of a ‘tender’ tooth in her upper left quadrant.
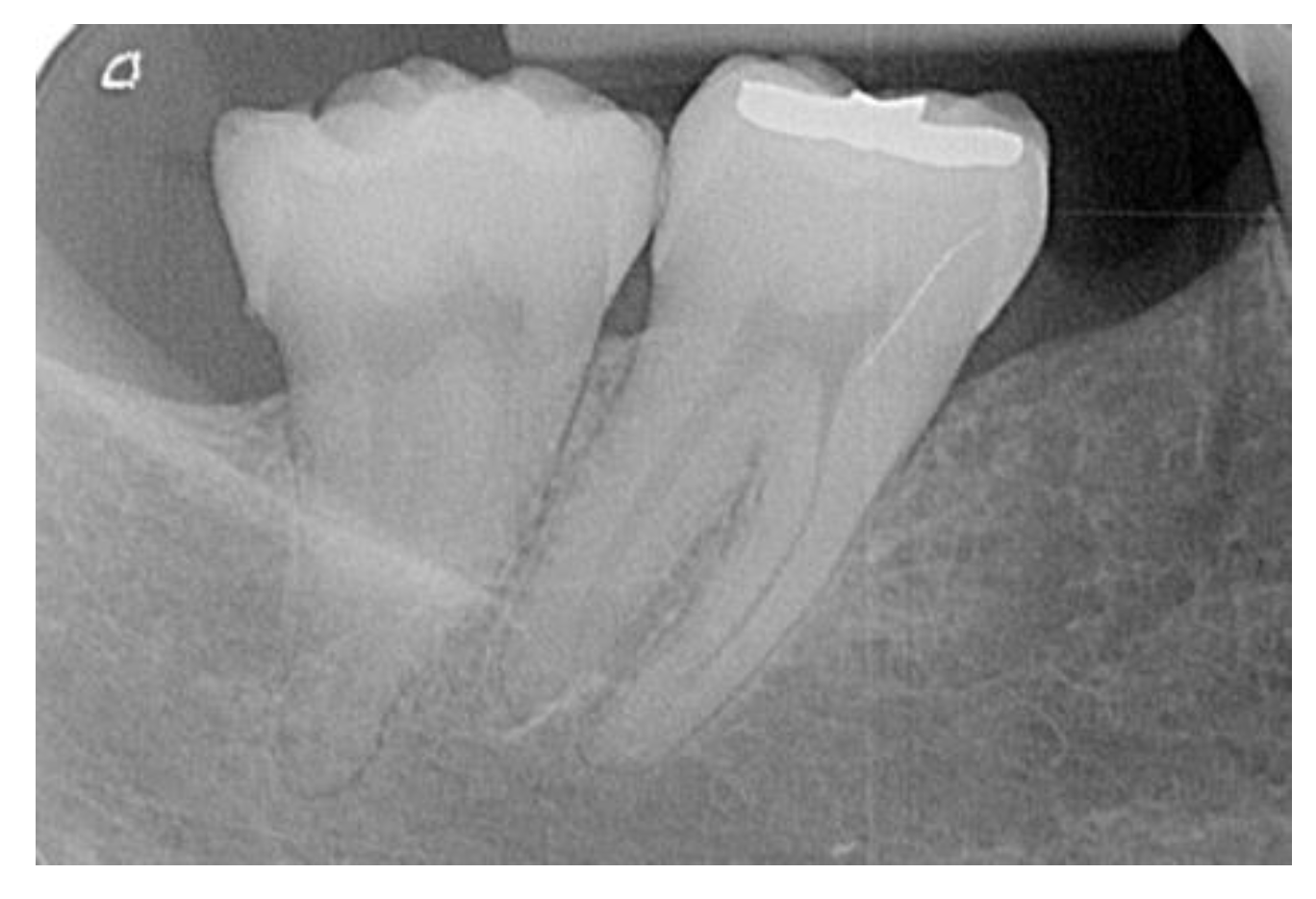
Clinical examination found that she had good oral hygiene and that her intra-oral soft tissues were healthy, apart from a draining sinus above her upper left first molar. She had a partially restored dentition and an incidental finding of a large bifid crown of her lower-right second molar (Figure 3 and Figure 4). This tooth had previously been restored with a small, miscoloured disto-occlusal restoration. The composite restoration had partially fractured disto-lingually, resulting in a 2 mm-wide, slightly carious cavity. A Basic Periodontal Examination (BPE) was carried out, which found false pocketing of the gingiva around the tooth with an overall score of ‘3’ in this sextant, but a score of ‘1’ in all other sextants. An intra-oral periapical radiograph (Figure 5) of the tooth demonstrated a wide crown that appeared to partially diverge, with one half of the crown pointing mesially and the other pointed distally. The crowns converged into a large pulp with three distinguishable pulp horns and two roots.
Treatment for this patient consisted of completion of a plaque index score to observe areas of inadequate cleaning and plaque accumulation. Following the use of this visual special investigation that allowed the patient to observe areas for oral hygiene improvement, the patient was given an ultrasonic subscale as well as instruction on the use of interdental brushes and single tufted brushes to achieve optimal gingival hygiene. The variance in anatomy of this tooth from a typical tooth, and therefore the increased periodontal susceptibility, was explained to the patient. This served to further encourage and highlight the importance of immaculate oral hygiene technique. Six weeks later, on re-instrumentation, there was no gingival inflammation or bleeding on probing and a BPE score of ‘0’ was recorded.
The existing composite restoration as well as the carious pit were removed. The tooth was re-restored with composite resin and adjusted to ensure the patient was content with the occlusal scheme, as morphological differences in the presentation of the bifid crown alter standard occlusion. The unusual anatomy of the tooth presented difficulty in achieving good aesthetic results with the composite. To address the patient’s other complaints that did not concern the geminated tooth, root canal treatment of the upper left first molar was also completed. This case was treated with simple restorative procedures; however, a case can very easily present with more complications when endodontic or surgical procedures in the form of complete removal or hemisection of the double tooth are required for pathological or aesthetic reasons.
3. Discussion
Tooth gemination and fusion are anomalies that occur during the morpho-differentiation stage of odontogenesis [7]. The precise aetiology of geminated teeth is uncertain, but studies show a variety of local and systemic factors to be responsible for the developmental disturbances. These may include hereditary diseases including achondroplasia, chondroectodermal dysplasia, osteopetrosis and focal dermal hypoplasia. Infectious inflammatory processes, endocrine influences, ionising radiation or local traumatic interferences [8,9], as suggested by reports suggesting physical pressure during tooth development can result in close contact between the tooth buds, which may also result in fusion [10]. There are thought to be more than 300 genes responsible for odontogenesis. A defect in any of these genes may result in altered morphology of a tooth, and disturbances affecting these genes may occur pre- or postnatally. Consequently, either dentition may be affected [8].
The clinical differentiation between fusion and gemination can be difficult, but as fusion refers to the joining of two individual tooth buds, in the exception that one tooth bud was that of a supernumerary tooth, the patient would present with one tooth fewer than the norm. Therefore, this may be noticed during a routine dental charting. As gemination is the division of one tooth bud, tooth count is regular and so may just be observed through the presence of a macrodont tooth. Radiographic analysis is used to confirm the diagnosis by assessing the number of roots as well as the outline of the pulp chamber and pulp horns. In this case, the patient presented without a shortage in number of teeth (excluding a previously extracted lower-right second premolar) and the presence of a large singular pulp chamber in the lower-right second molar. Thus, a diagnosis of gemination was made. As this type of anomaly is one that affects the 3D structure of a tooth, the use of cone beam computed tomography (CBCT) would be the most thorough method of assessing this anomaly for a more accurate differentiation between the two conditions [11]. This differentiation becomes significant in managing instances that require complex treatment. CBCT may be used to assess the potentially intricate root canal system of a double tooth, which will vary greatly between fused and geminated teeth. This will allow a specialist to know how to appropriately instrument through the tooth in the event of endodontic pathology or elective endodontic treatment that may occur as a result of pulp exposure during surgical sectioning of a bifid crown [10]. Further to this, specialists will require detail of the structure of the tooth and therefore whether the tooth has been fused or geminated prior to treatment that may include hemi-sectioning, grinding or surgical extraction.
Existing literature shows the majority of teeth affected by fusion or gemination to be that of the deciduous dentition, and most commonly, it is the anterior teeth that are affected. Aesthetic problems are therefore the primary complaint in such presentations.
Gemination occurring not only in the permanent dentition, but in posterior teeth is a rare phenomenon. The irregular morphology of the crown, particularly the presence of a large occlusal table with additional fissures, as well as lingual and labial vertical grooves where the two crowns demarcate, create plaque traps that may be difficult to clean [2]. As well as this, the abnormal shape of the tooth creates oddities in the way the maxillary and mandibular teeth occlude and can cause asymmetry, which interferes with tooth alignment and may result in crowding [2,6]. These features increase the likelihood of caries. In this case, the patient presented with a failing occlusal composite restoration where the disto-occlusal aspect of the composite had fractured off. Fracture of the restoration in this manner may have been due to poor occlusal design of the restoration where ultimately increased occlusal forces directed distally resulted in fracture. Often, the unusual contour of these teeth, as well as the extension of the vertical grooves subgingivally, can cause food and plaque accumulation at the level of, and beneath, the gingivae, leading to gingival inflammation and pocket formation. Periodontal health may therefore be at risk [11], and this is highlighted in this case where initial routine examination indicated a BPE score of ‘3’ in the sextant of the geminated tooth, but a BPE of ‘1’ in all other sextants. In cases where there is crowding of unusually large incisors, accessibility for a patient’s oral hygiene becomes difficult and can lead to further deposits and gingival inflammation [12]. There is strong evidence of the link between periodontal disease and systemic disease and the importance of maintaining excellent periodontal health is especially relevant for patients at risk of cardiovascular disease or diabetes [13], and there is also evidence of a link between periodontal disease and Alzheimer’s disease [14].
It can occasionally be difficult to identify double teeth on conventional radiographs due to superimposition. This can create further complications if extracting an undiagnosed fused or geminated posterior tooth in the maxillary arch. This is due to the higher likelihood of fracture of the maxillary tuberosity in consequence to excessive force application when attempting to remove the large tooth. This is relevant to the general dental practitioner (GDP), who should promptly refer such a case to an oral surgeon should tuberosity fracture occur [13].
Primary aims when treating fusion and gemination cases should be to reduce caries risk, periodontal risk, improve aesthetics and maintain function. Treatment options will be case dependent and vary greatly due to the multitude of ways in which the tooth may present. A multidisciplinary approach with input from orthodontists, prosthodontists, endodontists and oral surgeons may be required [12,15], with treatment decision taking factors including the location of the tooth, the patient’s age, the degree of involvement and the stage of root development into consideration.
Possible treatment options include endodontic treatment proceeded by ‘slicing’ or hemi-sectioning of the tooth and direct restoration with composite resin. This may be followed by orthodontic alignment [10,12], especially for anterior cases where significant spacing may result following hemi-sectioning of the tooth. In some cases, the tooth may be extracted prior to sectioning and then re-implanted. However, this may result in ankylosis due to a lack of periodontal membrane where the tooth has been sectioned. Other cases may simply include reducing the size of the double tooth by selective grinding and complete extraction of the tooth, followed by replacement with either a fixed or removable prosthesis or crowning the tooth [10,11]. When deciduous teeth are affected, treatment options can depend upon the presence of the successor tooth. In some cases, the deciduous tooth may be unrestorable and may simply be left to exfoliate naturally, or it may need to be extracted, depending on the degree of root resorption [16].
As with all patients, consideration must be given to any risks and possible complications that may arise because of treatment. These may include tooth devitalisation in cases that are not endodontically treated, ankylosis, or failure of root treatment where endodontic treatment is provided. Not all patients will require specialist-level care, but GDPs should be aware of the presentation of these teeth so that an early diagnosis can be made, and preventative care implemented. GDPs may seal the fissures and grooves on bifid crowns, improve the aesthetics of affected anterior teeth with direct composite resin restorations, promote the importance of immaculate oral hygiene to prevent periodontal disease, encourage good dietary habits and provide fluoride advice [17]. Early referral of children to a joint paediatric and orthodontic clinic may also be helpful to allow treatment plans and considerations to begin. These implementations may all serve to reduce the clinical necessity of complex treatment.
4. Conclusions
Gemination and fusion are rare occurrences that have the potential to have clinically significant implications for a patient. Although many of these teeth may be asymptomatic, early recognition of their presence and unusual anatomy by general dentists can be important to prevent complications that may require patients to have extensive treatment. Double teeth in the primary dentition may delay the eruption of permanent teeth, and so GDPs should seek specialist advice and carefully monitor these potentially problematic teeth. Successful treatment of patients with fused and geminated teeth should be focused on prevention, improving aesthetics and maintaining function.
Author Contributions
Case treated by A.P.-S.; writing—initial draft preparation, A.P.-S.; writing—review and editing, J.P.; revised draft preparation, A.P.-S.; revised draft review and editing, J.P. Both authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tarim Ertas, E.; Yircali Atici, M.; Arslan, H.; Yasa, B.; Ertas, H. Endodontic treatment and esthetic management of a geminated central incisor bearing a talon cusp. Case Rep. Dent. 2014, 2014, 123681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajesh Ebenezar, A.; Venkatesh, A.; Mary, A.V.; Mohan, A.G. An unusual occurrence of bilaterally geminated mandibular second premolars resulting in premolar molarization: A case report. J. Conserv. Dent. 2013, 16, 582–584. [Google Scholar] [PubMed] [Green Version]
- Rao, P.; Veena, K.; Chatra, L.; Shenai, P. Twin tooth on either side: A case report of bilateral gemination. Ann. Med. Health Sci. Res. 2013, 3, 271–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkatesh, A.M.; Mitthra, S.; Prakash, V.; Prasad, T.S. Gemination or Fusion?—A case report. Biomed. Pharmacol. J. 2016, 9, 1225–1228. [Google Scholar] [CrossRef]
- Rudagi, K.; Rudagi, B.M.; Metgud, S.; Wagle, R. Endodontic management of mandibular second molar fused to a supernumerary tooth, using spiral computed tomography as a diagnostic aid: A case report. Case Rep. Dent. 2012, 2012, 614129. [Google Scholar] [CrossRef] [PubMed]
- Ramamurthy, S.; Satish, R.; Priya, K. Surgical and orthodontic management of fused maxillary central and lateral incisors in early mixed dentition stage. Case Rep. Dent. 2014, 2014, 109301. [Google Scholar] [CrossRef] [PubMed]
- Sandeep, S.; Kumar, G.J.; Potdar, S.; Bhanot, R.; Vathare, A.S.; Tiwari, R.V.; Harshitha, B. Rare case of gemination of mandibular third molar-A case report. J. Family Med. Prim. Care 2020, 9, 2577–2579. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.M.; Marla, V.; Shrestha, S.; Mahrjan, I. Developmental anomalies affecting the morphology of teeth—A review. RSBO 2015, 12, 68–78. [Google Scholar] [CrossRef] [Green Version]
- Grover, P.S.; Lorton, L. Gemination and twinning in the permanent dentition. J. Oral Med. Oral Path. 1985, 59, 313–318. [Google Scholar] [CrossRef]
- Demircioglu Guler, D.; Sen Tunc, E.; Arici, N.; Ozkan, N. Multidisciplinary management of a fused tooth: A case report. Case Rep. Dent. 2013, 2013, 634052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, P.; Gupta, H.; Mathur, H.; Porwal, A. Gemination mandibular third molar—A rare case with use of CBCT in diagnosis and treatment planning. J. Indian Acad. Oral Med. Radiol. 2019, 31, 377–381. [Google Scholar]
- Mahendra, L.; Govindarajan, S.; Jayanandan, M.; Shamsudeen, S.M.; Kumar, N.; Madasamy, R. Complete bilateral gemination of maxillary incisors with separate root canals. Case Rep. Dent. 2014, 2014, 425343. [Google Scholar] [CrossRef] [PubMed]
- Hegde, R.; Awan, K.H. Effects of periodontal disease on systemic health. Dis. Mon. 2019, 65, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Cerajewska, T.; Davies, M.; West, N. Periodontitis: A potential risk factor for Alzheimer’s disease. Br. Dent. J. 2015, 218, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Grammatopoulos, E. Gemination or fusion? Br. Dent. J. 2007, 203, 119–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrivastava, S.; Tijare, M.; Singh, S. Fusion/double teeth. J. Indian Acad. Oral Med. Radiol. 2011, 23, 468–470. [Google Scholar] [CrossRef]
- Ben Salem, M.; Chouchene, F.; Masmoudi, F.; Baaziz, A.; Maatouk, F.; Ghedira, H. Fusion or Gemination? Diagnosis and Management in Primary Teeth: A Report of Two Cases. Case Rep. Dent. 2021, 2021, 6661776. [Google Scholar] [PubMed]
Figure 1.
Diagrammatic representation of geminated teeth with a bifid crown and shared roots and root canal systems: (a) geminated molar tooth; (b) geminated incisor tooth.
Figure 1.
Diagrammatic representation of geminated teeth with a bifid crown and shared roots and root canal systems: (a) geminated molar tooth; (b) geminated incisor tooth.

Figure 2.
Diagrammatic representation of fused teeth with a bifid crown and individual roots and root canal systems: (a) fused molar tooth; (b) fused incisor tooth.
Figure 2.
Diagrammatic representation of fused teeth with a bifid crown and individual roots and root canal systems: (a) fused molar tooth; (b) fused incisor tooth.

Figure 3.
Lower-right intra-oral view showing the large bifid crown of the lower right second molar.
Figure 3.
Lower-right intra-oral view showing the large bifid crown of the lower right second molar.

Figure 4.
Occlusal view of lower-right second molar showing fractured composite restoration and early carious lesion.
Figure 4.
Occlusal view of lower-right second molar showing fractured composite restoration and early carious lesion.

Figure 5.
Intraoral periapical radiograph showing the wide pulp chamber of the lower-right second molar stemming from two roots.
Figure 5.
Intraoral periapical radiograph showing the wide pulp chamber of the lower-right second molar stemming from two roots.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Pandya-Sharpe, A.; Puryer, J. A Geminated Mandibular Second Molar—A Case Report. Reports 2021, 4, 31. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4040031
AMA Style
Pandya-Sharpe A, Puryer J. A Geminated Mandibular Second Molar—A Case Report. Reports. 2021; 4(4):31. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4040031
Chicago/Turabian StylePandya-Sharpe, Asha, and James Puryer. 2021. "A Geminated Mandibular Second Molar—A Case Report" Reports 4, no. 4: 31. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4040031