1. Introduction
At the completion of residency training in obstetrics and gynecology (Ob/Gyn), each resident is expected to have a comprehensive knowledge base of core Ob/Gyn topics sufficient for independent practice. The Accreditation Council for Graduate Medical Education (ACGME) requires each Ob/Gyn residency program to maintain an education curriculum to help each resident achieve designated competencies [
1]. A national resident assessment of knowledge is completed annually by the Council on Resident Education in Obstetrics and Gynecology (CREOG) In-Training Exam. At the completion of residency, all Ob/Gyn graduates may sit for the qualifying examination given by the American Board of Obstetrics and Gynecology (ABOG), the first step towards Board Certification.
In Ob/Gyn, while there are readily available educational resources created by various credible organizations including the American College of Obstetricians and Gynecologists (ACOG), CREOG, and many others, they are not currently co-located, integrated, or structured into a format that can serve as a comprehensive curriculum for Ob/Gyn residency. In 2020, CREOG published the CREOG 12th Edition of Educational Objectives, which consists of a comprehensive list of learning objectives [
2]. While CREOG has associated ACOG resources with these objectives, this still will not serve as a platform that functions as a residency education curriculum. A curriculum would not only require topics with associated objectives and resources, but also a platform with a structured timeline for implementation of these topics at residency programs. Additionally, the curriculum would need to cycle. As no standardized curriculum currently exists, each residency program develops its own didactic education curriculum, which requires a significant amount of time and effort and leads to variability in curriculum quality and content. This may lead to a wide range in resident and faculty satisfaction, resident performance on the annual CREOG and ABOG Exams, and clinical competency upon completion of residency training.
Meanwhile, there are other specialties such as general surgery who have implemented a successful standardized, national residency education curriculum for their residents. In general surgery, this national curriculum has shown significant improvement in outcomes of residency training, including resident and program leadership satisfaction as well as In-Training and Board Exam scores [
3,
4,
5,
6]. In 2004, general surgery formed the Surgical Council on Resident Education (SCORE, the correlate to CREOG) and with the support of the American Board of Surgery (ABS), American College of Surgeons, and ACGME in 2008 developed the SCORE Portal, a web-based national education curriculum [
3]. The principal goal of SCORE is to provide general surgery residents across the country with equal access to a common knowledge base through a national curriculum and educational resources and, thus, to standardize and improve the education of residents in general surgery and related specialties [
7,
8]. The SCORE Portal includes This Week in SCORE (TWIS), which is a standardized two-year general surgery curriculum comprised of weekly topics with online modules, associated readings, and multiple-choice quizzes, and provides a systematic way for residents and programs to cover content and track performance [
3]. The portal is updated and maintained by the SCORE. As of 2018, the SCORE curriculum is used by 97% of general surgery programs nationally [
9].
There is substantial data showing the positive impact of the SCORE Portal on outcomes of residency training. Residents who participate in the TWIS weekly curriculum have shown a considerable improvement in general surgery In-Training Exam performance. Winer et al. noted a 12% increase in median score, and 90% of residents felt that this structured curriculum improved the culture of education at their program [
4]. Chang et al. demonstrated that residents who completed more review questions using the SCORE curriculum performed higher on the In-Training Exam [
5]. Residents in programs who subscribe to SCORE have demonstrated an improvement in mean board scores and, ultimately, a higher pass rate on the ABS Qualifying Exam [
6]. Other surgical subspecialties, including Vascular Surgery, Pediatric Surgery, Oral and Maxillofacial Surgery, and Oncologic Surgery, as well as Critical Care, have added their sub-specialty curriculum content to the SCORE platform for their residents.
We hypothesize that there is a need for a standardized residency education curriculum in the field of Ob/Gyn. With this study, we sought to determine the perceptions Ob/Gyn residents, program directors (PDs), and assistant program directors (APDs) at three diverse institutions have of the need for a standardized Ob/Gyn residency education curriculum.
2. Materials and Methods
Participants were recruited from three sites: Temple Health, Virginia Commonwealth University Health, and Einstein Healthcare Network. Temple Health is a university-based program in Philadelphia, Pennsylvania, with five residents per year (with the exception of six first-year positions). Virginia Commonwealth University Health is a university-based program in Richmond, Virginia with six residents per year. Einstein Healthcare Network is a community-based program with five residents per year [
10]. All Ob/Gyn residents from postgraduate years 1–4, program directors, and assistant program directors from the three sites were invited to participate. This included a total of 73 eligible participants (three PDs, five APDs, and 65 residents). Participants were recruited by distributing the survey via email.
A twelve-item web-based survey was developed on the SurveyMonkey platform. The survey questions were designed to obtain pertinent demographic information, assess the current state of and satisfaction with didactic resident education, and to assess the main outcomes of the study—the perceptions that residents and program leadership have regarding centralization and accessibility of resident didactic education and the need for a standardized Ob/Gyn residency education curriculum.
Respondents were queried about individual and program demographic information, current use of Ob/Gyn educational resources, and program-specific didactic education curriculum information. Respondents were additionally queried about their perceptions regarding the need for centralization and standardization of Ob/Gyn residency education and the need for a national Ob/Gyn residency education curriculum on a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neither disagree nor agree, 4 = agree, 5 = strongly agree). Lastly, respondents were queried to select which components they believe should be included if a national curriculum were to be developed. See
Appendix A for survey questions.
In March 2019, the survey was distributed via email to the participating institutions. Program directors and assistant program directors were contacted directly via email to participate and were asked to distribute the survey study via email to residents at their respective institutions for participation. Responses were collected on the SurveyMonkey platform, a secure web-based application. Participant responses were anonymous, and participants provided electronic informed consent. Participants were given the option to participate in a raffle for an Amazon gift card. Each participant was limited to one response through the survey platform. The survey was open for participants to complete for four weeks, from March to April 2019. Two reminder emails were sent to complete the survey, one to two weeks apart. We performed descriptive statistics using Microsoft Excel 2019. Descriptive statistics were reported using means and standard deviations for continuous variables and counts and percentages for categorical variables. This study was approved by the Temple University Institutional Review Board.
3. Results
3.1. Participants
A total of 50 out of 73 respondents completed the survey, representing an overall survey response rate of 68%. Response rates in each respective group of PDs, APDs, and residents included the following: 3/3 (100%), 5/5 (100%), and 42/65 (65%).
Current State of Resident Education
Of participants, 100% responded that their residency program has a didactic education curriculum, defined as scheduled learning sessions, with or without associated readings. The educational resources most commonly cited, both as part of the didactic education curriculum and for independent learning, included ACOG Practice Bulletins, ACOG Committee Opinions, and Ob/Gyn textbooks. The educational materials that respondents found to be the most useful for the CREOG In-Training Exam included ACOG Practice Bulletins, ACOG Committee Opinions, and Personal Review of Learning in Obstetrics and Gynecology (PROLOG). No participants listed “other” as a response to educational materials used (
Table 1). The majority of participants reported that their didactic education curriculum cycles, with a two-year cycle, reported most commonly.
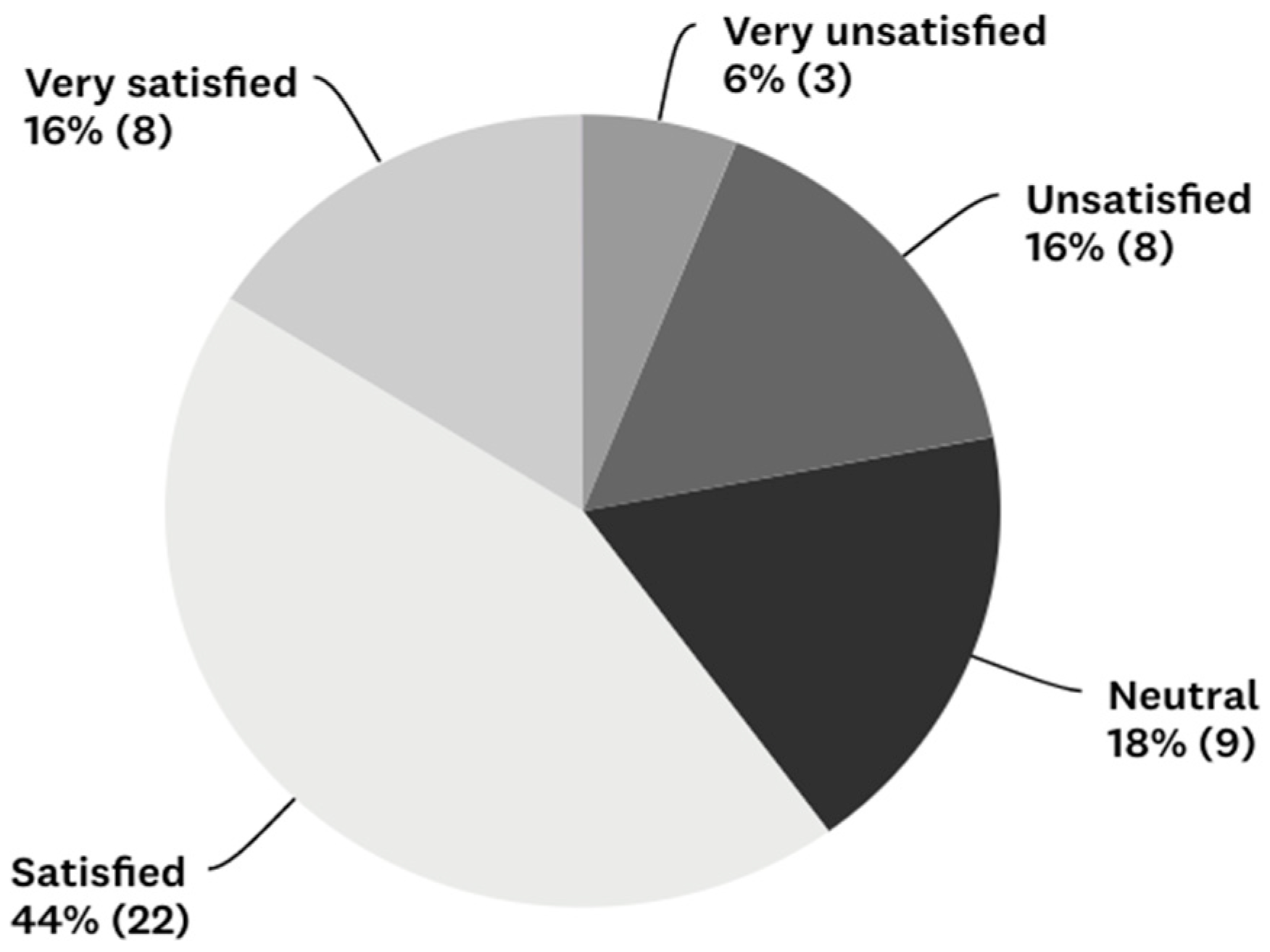
The most common struggles reported with programs’ didactic education curricula included low resident participation, lack of sufficient didactic time, lack of curriculum structure, lack of fully protected education time, and frequent curriculum turnover. Of note, although “low faculty participation” was not a specific option for this question, four participants individually selected “other” and reported this as an issue. Regarding satisfaction with their current didactic education curriculum at their residency program, 40% of respondents were very unsatisfied, unsatisfied, or neutral (
Figure 1).
Perceptions Regarding Centralization and Standardization of Residency Education
Of all participants, 78% (and 100% of PDs and APDs) agreed or strongly agreed that the didactic education curriculum at their residency program could be improved. The majority of respondents (72%) agreed or strongly agreed that all Ob/Gyn residents across the country should learn the same content through their didactic education curriculum. Almost all participants (94%) agreed or strongly agreed that residents nationwide should have equal access to high-quality Ob/Gyn educational resources during their training. A significant majority of respondents (92%) agreed or strongly agreed that core Ob/Gyn educational resources should be centrally located. Of participants, 80% agreed or strongly agreed that they would like to have a curriculum of core education topics for Ob/Gyn residency that is developed and implemented on a national level.
A significant majority (76% total, with 76% of residents, 66% of PDs, and 80% of APDs) agreed or strongly agreed that there is a need for a national Ob/Gyn residency education curriculum. The majority of participants (72%) agreed or strongly agreed that a national Ob/Gyn residency education curriculum would improve resident performance on the CREOG In-Training Exam (
Table 2).
Curriculum Components
If a national Ob/Gyn residency education curriculum were developed, the majority of respondents agreed or strongly agreed that it should include core learning topics (92%), learning objectives (78%), core readings (88%), additional high yield resources (94%), and quiz questions (90%).
4. Discussion
The principal finding of this study of diverse Ob/Gyn residency programs is a perceived need among residents and program leadership for a centrally located, standardized Ob/Gyn residency education curriculum.
Additionally, our findings demonstrate that Ob/Gyn residents and programs at the three residency programs surveyed are using similar education resources for resident didactics, independent learning, and CREOG In-Training Exam preparation. Our results reveal that residents and program leadership at these three institutions report similar challenges with and desire improvement of resident didactic education. Lastly, residents and program leadership at these institutions desire centralization, equal accessibility, and standardization of resident didactic education content.
This survey study demonstrates a perceived need for a centrally located, structured, standardized residency education curriculum in the field of Ob/Gyn. The benefits of standardization of medical education have been reviewed in the literature. Standardization offers many rewards, including the promotion of patient safety, fostering continuous quality improvement, and enabling the spread of best practices. Standardization may also contribute to greater fairness, equity, reliability, and validity [
11]. Furthermore, there has been research on best practice in medical education that highlights that medical education at all levels should be designed to equip physicians with the knowledge, clinical skills, and professionalism that are required to deliver quality patient care with the ultimate outcome being the health of individual patients and society. Improvement in patient outcomes has been linked to educational efforts, and this emphasizes the importance of research in the arena of medical education, such as this study [
12].
We anticipate that standardizing the material that Ob/Gyn residents learn nationwide through the creation of a centralized curriculum would improve outcomes of residency training in our field and have multiple positive clinical implications. First, a standardized curriculum created with CREOG objectives and ACOG resources would align teaching and learning with essential core content as already determined by the education organizations in our field. Second, central regulation would allow individuals and programs to spend less time developing and modifying curricula and more time teaching and learning. Third, a standardized curriculum would reduce variability in didactic content and allow residents from all types of programs to have access to the same knowledge base. This would likely lead not only to improvement in Ob/Gyn resident and program leadership satisfaction with their education curriculum and improvement in exam scores on the CREOG In-Training Exam and on the ABOG Exam, but more importantly, more uniform acquisition of clinical knowledge that may transfer to improved clinical practice upon completion of training. This would optimize the care that we provide for our patients in our field. Additionally, by providing all residents in a field with the standardized knowledge base that they are expected to have upon completion of training leads the field to ultimately be more accountable for providing uniform, evidence-based clinical care.
There were several strengths to this study. An important strength of this study is the high response rate of 68%. Additionally, this study was the first to assess the current state of Ob/Gyn resident didactic education. Our study was also the first to evaluate the need for a standardized Ob/Gyn residency education curriculum, with a majority of respondents indicating a desire for a standardized curriculum effort. Additional strengths include the anonymity of the study and a timely assessment of a topic relevant to not only Ob/Gyn, but also other related specialties. Most importantly, these results pave the way for residents at all programs to have equal access to high-quality education content in the form of a standardized curriculum.
There were several limitations to our study. One limitation is the risk of nonresponse bias, which was minimized by the high response rate. An additional limitation is that the survey data could have been collected in a fashion to allow for more advanced statistical analysis. Furthermore, this study was conducted at three institutions and thus cannot be directly generalized to all residents and program leadership nationally.
Future directions include conducting a national survey of all Ob/Gyn programs to confirm the findings of this multi-institution study and, ultimately, designing and implementing a standardized residency education curriculum in Ob/Gyn that integrates existing resources, modeled after successful national curricula in other specialties.
5. Conclusions
This study demonstrates a perceived need for a centrally located, structured Ob/Gyn residency education curriculum to promote standardization of the knowledge that residents have upon completion of their residency training. Other specialties such as general surgery have created such curricula with tremendous success and almost ubiquitous use. Similar to other specialties, a standardized Ob/Gyn residency education curriculum would likely lead to an improvement in Ob/Gyn resident and program leadership satisfaction with their education curriculum and improvement in exam scores on the CREOG In-Training and ABOG Exams. Most importantly, a standardized curriculum may increase and help standardize resident clinical competency upon completion of residency training and, thus ultimately, improve the care that we provide to patients in our field.
Author Contributions
Conceptualization, O.M., J.H., S.J., D.J. and M.R.; methodology, O.M., J.H. and M.R.; software, O.M.; validation, O.M., J.H., D.J. and M.R.; formal analysis, O.M.; investigation, O.M.; resources, O.M.; data curation, O.M.; writing — original draft preparation, O.M.; writing — review and editing, O.M., J.H., S.J., D.J. and M.R.; visualization, O.M.; supervision, J.H., S.J., D.J. and M.R.; project administration, O.M.; funding acquisition, O.M., J.H., D.J. and M.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Council on Resident Education in Obstetrics and Gynecology (CREOG) Empower Award. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Acknowledgments
The authors would like to thank the CREOG Empower Award for funding this study, the SurveyMonkey online survey software for providing a platform to develop and distribute the needs assessment survey, and all participants, including residents and program leadership who participated in the survey study.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Appendix A. Needs Assessment Survey
![Reprodmed 01 00015 i001]()
![Reprodmed 01 00015 i002]()
![Reprodmed 01 00015 i003]()
References
- Accreditation Council for Graduate Medical Education (ACGME). ACGME Program Requirements for Graduate Medical Education in Obstetrics and Gynecology; ACGME: Chicago, IL, USA, 2019. [Google Scholar]
- CREOG Education Committee. Council on Resident Education in Obstetrics and Gynecology Educational Objectives: Core Curriculum in Obstetrics and Gynecology, 12th ed.; The American College of Obstetricians and Gynecologists: Washington, DC, USA, 2020. [Google Scholar]
- Web Site: SCORE|General Surgery Resident Curriculum Portal. Available online: https://www.surgicalcore.org/ (accessed on 20 September 2019).
- Winer, L.K.; Cortez, A.R.; Kassam, A.; Quillin, R.C.; Goodman, M.D.; Makley, A.T.; Sussman, J.J.; Kuethe, J.W. The Impact of a Comprehensive Resident Curriculum and Required Participation in “This week in SCORE” on General Surgery ABSITE Performance and Well-Being. J. Surg. Educ. 2019, 76, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.; Kenel-Pierre, S.; Basa, J.; Schwartzman, A.; Dresner, L.; Alfonso, A.E.; Sugiyama, G. Study habits centered on completing review questions result in quantitatively higher American Board of Surgery In-Training Exam scores. J. Surg. Educ. 2014, 71, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Klingensmith, M.E.; Jones, A.T.; Smiley, W.; Biester, T.W.; Malangoni, M.A. Subscription to the Surgical Council on Resident Education Web Portal and Qualifying Examination Performance. J. Am. Coll. Surg. 2014, 218, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, A.K.; Bell, R.H., Jr.; Britt, L.D.; Tarpley, J.L.; Blair, P.G.; Tarpley, M.J. National efforts to reform residency education in surgery. Acad. Med. 2007, 82, 1200–1210. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.H. Surgical council on resident education: A new organization devoted to graduate surgical education. J. Am. Coll. Surg. 2007, 204, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.R.T.; Salami, A.; Hickey, M.; Barrett, K.B.; Klingensmith, M.E.; Malangoni, M.A. What Can SCORE Web Portal Usage Analytics Tell Us About How Surgical Residents Learn? J. Surg. Educ. 2017, 74, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Web Site: American Medical Association|FREIDA. Available online: https://freida.ama-assn.org/ (accessed on 13 September 2020).
- Bates, J.; Schrewe, B.; Ellaway, R.H.; Teunissen, P.W.; Watling, C. Embracing standardisation and contextualisation in medical education. Med. Educ. 2019, 53, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed, S.; Shell, R.; Kassis, K.; Tartaglia, K.; Wallihan, R.; Smith, K.; Hurtubise, L.; Martin, B.; Ledford, C.; Bradbury, S.; et al. Applying adult learning practices in medical education. Curr. Probl. Pediatr. Adolesc. Health Care 2014, 44, 170–181. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).







{kind=link}