Is the Cerebro-Placental Ratio Sufficient to Predict Adverse Neonatal Outcome in Small for Gestational Age Fetuses > 34 Weeks of Gestation?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Neonatal Outcome
2.5. Standard Clinical Management
2.6. Stasticial Analysis
3. Results
3.1. Demographic Data
3.2. Ultrasound Parameters
3.3. Neonatal Outcome
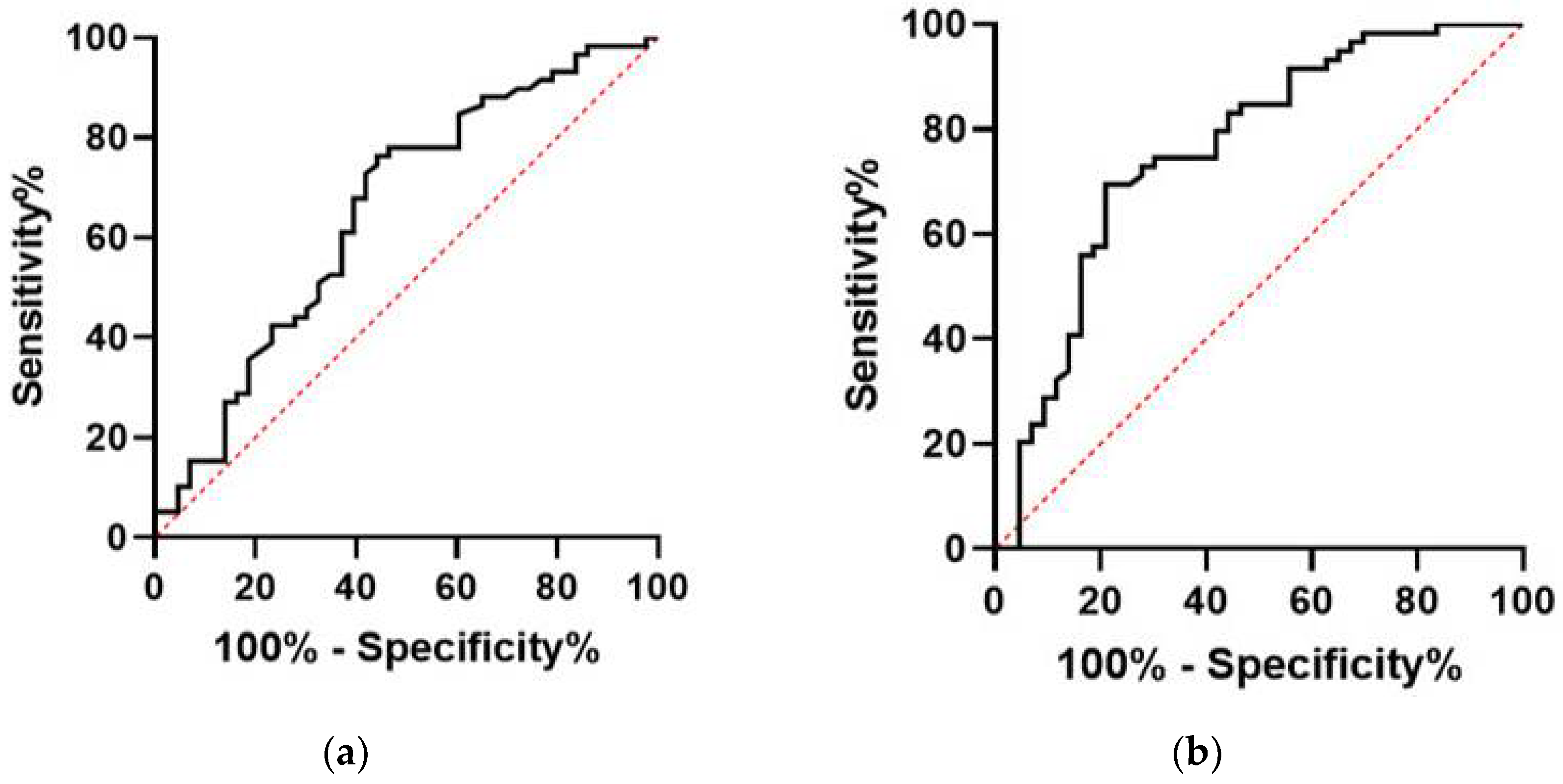
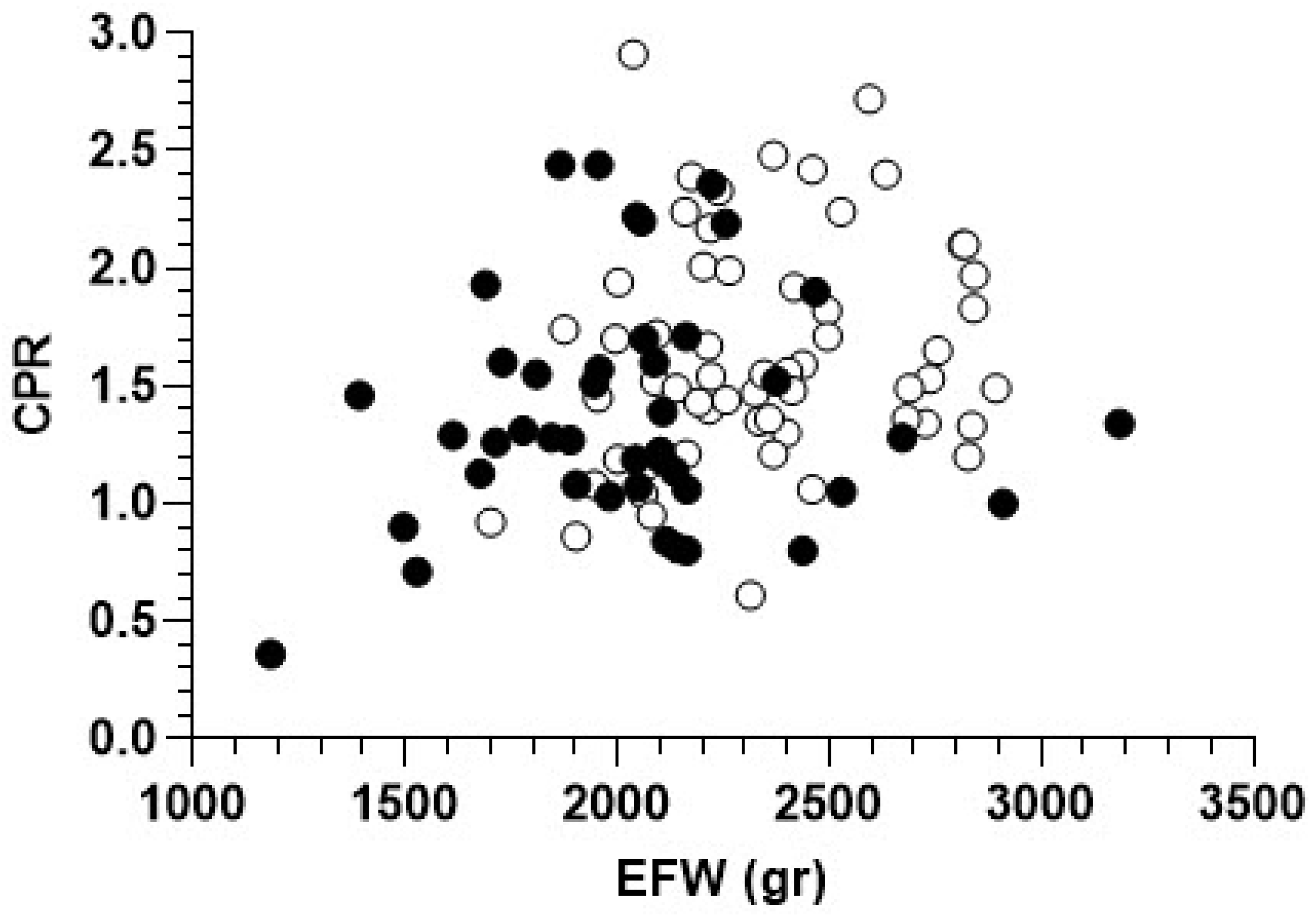
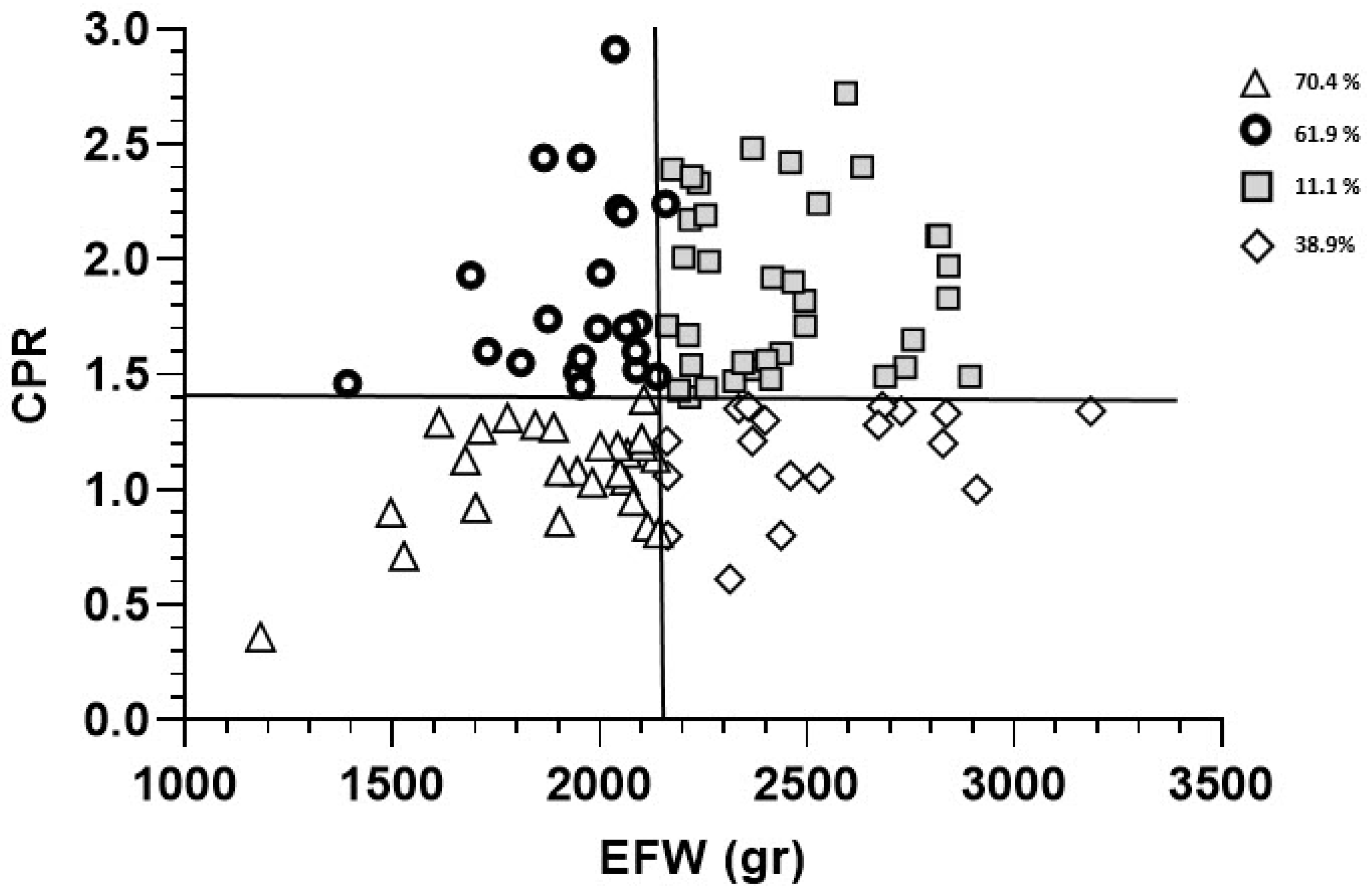
3.4. CPR Cutoff Value and EFW
3.5. Umbilical Artery PI
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeVore, G.R. The importance of the cerebroplacental ratio in the evaluation of fetal well-being in SGA and AGA fetuses. Am. J. Obstet. Gynecol. 2015, 213, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Figueras, F.; Savchev, S.; Triunfo, S.; Crovetto, F.; Gratacos, E. An integrated model with classification criteria to predict small-for-gestational-age fetuses at risk of adverse perinatal outcome. Ultrasound Obstet. Gynecol. 2015, 45, 279–285. [Google Scholar] [CrossRef] [PubMed]
- ACOG Practice bulletin no. 134: Fetal growth restriction. Obstet. Gynecol. 2013, 121, 1122–1133. [CrossRef] [PubMed]
- Garite, T.J.; Clark, R.; Thorp, J.A. Intrauterine growth restriction increases morbidity and mortality among premature neonates. Am. J. Obstet. Gynecol. 2004, 191, 481–487. [Google Scholar] [CrossRef]
- Lees, C.; Marlow, N.; Arabin, B.; Bilardo, C.M.; Brezinka, C.; Derks, J.B.; Duvekot, J.; Frusca, T.; Diemert, A.; Ferrazzi, E.; et al. Perinatal morbidity and mortality in early-onset fetal growth restriction: Cohort outcomes of the trial of randomized umbilical and fetal flow in Europe (TRUFFLE). Ultrasound Obstet. Gynecol. 2013, 42, 400–408. [Google Scholar] [CrossRef]
- Bouchet, N.; Gayet-Ageron, A.; Lumbreras Areta, M.; Pfister, R.E.; de Tejada, B.M. Avoiding late preterm deliveries to reduce neonatal complications: An 11-year cohort study. BMC Pregnancy Childbirth 2018, 18, 17. [Google Scholar] [CrossRef] [Green Version]
- Conde-Agudelo, A.; Villar, J.; Kennedy, S.H.; Papageorghiou, A.T. Predictive accuracy of cerebroplacental ratio for adverse perinatal and neurodevelopmental outcomes in suspected fetal growth restriction: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2018, 52, 430–441. [Google Scholar] [CrossRef]
- Cruz-Martinez, R.; Figueras, F.; Hernandez-Andrade, E.; Oros, D.; Gratacos, E. Fetal brain Doppler to predict cesarean delivery for nonreassuring fetal status in term small-for-gestational-age fetuses. Obstet. Gynecol. 2011, 117, 618–626. [Google Scholar] [CrossRef]
- Khalil, A.; Morales-Rosello, J.; Khan, N.; Nath, M.; Agarwal, P.; Bhide, A.; Papageorghiou, A.; Thilaganathan, B. Is cerebroplacental ratio a marker of impaired fetal growth velocity and adverse pregnancy outcome? Am. J. Obstet. Gynecol. 2017, 216, 606.e1–606.e10. [Google Scholar] [CrossRef] [Green Version]
- Khalil, A.A.; Morales-Rosello, J.; Elsaddig, M.; Khan, N.; Papageorghiou, A.; Bhide, A.; Thilaganathan, B. The association between fetal Doppler and admission to neonatal unit at term. Am. J. Obstet. Gynecol. 2015, 213, 57.e1–57.e7. [Google Scholar] [CrossRef]
- Morales-Rosello, J.; Khalil, A. Fetal cerebroplacental ratio and adverse perinatal outcome. J. Perinat. Med. 2016, 44, 355. [Google Scholar] [CrossRef] [PubMed]
- Flood, K.; Unterscheider, J.; Daly, S.; Geary, M.P.; Kennelly, M.M.; McAuliffe, F.M.; O’Donoghue, K.; Hunter, A.; Morrison, J.J.; Burke, G.; et al. The role of brain sparing in the prediction of adverse outcomes in intrauterine growth restriction: Results of the multicenter PORTO Study. Am. J. Obstet. Gynecol. 2014, 211, 288.e1–288.e5. [Google Scholar] [CrossRef] [PubMed]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus definition of fetal growth restriction: A Delphi procedure. Ultrasound Obstet. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Lees, C.C.; Stampalija, T.; Baschat, A.; da Silva Costa, F.; Ferrazzi, E.; Figueras, F.; Hecher, K.; Kingdom, J.; Poon, L.C.; Salomon, L.J.; et al. ISUOG Practice Guidelines: Diagnosis and management of small-for-gestational-age fetus and fetal growth restriction. Ultrasound Obstet. Gynecol. 2020, 56, 298–312. [Google Scholar] [CrossRef] [PubMed]
- Figueras, F.; Gratacós, E. Update on the diagnosis and classification of fetal growth restriction and proposal of a stage-based management protocol. Fetal Diagn. Ther. 2014, 36, 86–98. [Google Scholar] [CrossRef] [PubMed]
- RCOG. The Investigation and Management of the Small-for-Gestational-Age Fetus (Green-Top Guideline No. 31); Royal College of Obstetricians and Gynaecologists: London, UK, 2013. [Google Scholar]
- Kehl, S.; Dotsch, J.; Hecher, K.; Schlembach, D.; Schmitz, D.; Stepan, H.; Gembruch, U. Intrauterine Growth Restriction. Guideline of the German Society of Gynecology and Obstetrics (S2k-Level, AWMF Registry No. 015/080, October 2016). Geburtshilfe Frauenheilkd 2017, 77, 1157–1173. [Google Scholar] [CrossRef] [Green Version]
- Hadlock, F.P.; Harrist, R.B.; Sharman, R.S.; Deter, R.L.; Park, S.K. Estimation of fetal weight with the use of head, body, and femur measurements--a prospective study. Am. J. Obstet. Gynecol. 1985, 151, 333–337. [Google Scholar] [CrossRef]
- Kagan, K.O.; Wright, D.; Maiz, N.; Pandeva, I.; Nicolaides, K.H. Screening for trisomy 18 by maternal age, fetal nuchal translucency, free beta-human chorionic gonadotropin and pregnancy-associated plasma protein-A. Ultrasound Obstet. Gynecol. 2008, 32, 488–492. [Google Scholar] [CrossRef]
- Kagan, K.O.; Wright, D.; Spencer, K.; Molina, F.S.; Nicolaides, K.H. First-trimester screening for trisomy 21 by free beta-human chorionic gonadotropin and pregnancy-associated plasma protein-A: Impact of maternal and pregnancy characteristics. Ultrasound Obstet. Gynecol. 2008, 31, 493–502. [Google Scholar] [CrossRef]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018, 13, 291–310. [Google Scholar]
- Morales-Roselló, J.; Khalil, A.; Morlando, M.; Bhide, A.; Papageorghiou, A.; Thilaganathan, B. Poor neonatal acid-base status in term fetuses with low cerebroplacental ratio. Ultrasound Obstet. Gynecol. 2015, 45, 156–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GRIT Study Group. A randomised trial of timed delivery for the compromised preterm fetus: Short term outcomes and Bayesian interpretation. BJOG 2003, 110, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Ciobanu, A.; Wright, A.; Syngelaki, A.; Wright, D.; Akolekar, R.; Nicolaides, K.H. Fetal Medicine Foundation reference ranges for umbilical artery and middle cerebral artery pulsatility index and cerebroplacental ratio. Ultrasound Obstet. Gynecol. 2019, 53, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Boers, K.E.; Vijgen, S.M.; Bijlenga, D.; van der Post, J.A.; Bekedam, D.J.; Kwee, A.; van der Salm, P.C.; van Pampus, M.G.; Spaanderman, M.E.; de Boer, K.; et al. Induction versus expectant monitoring for intrauterine growth restriction at term: Randomised equivalence trial (DIGITAT). BMJ 2010, 341, c7087. [Google Scholar] [CrossRef] [Green Version]
- Stampalija, T.; Thornton, J.; Marlow, N.; Napolitano, R.; Bhide, A.; Pickles, T.; Bilardo, C.M.; Gordijn, S.J.; Gyselaers, W.; Valensise, H.; et al. Fetal cerebral Doppler changes and outcome in late preterm fetal growth restriction: Prospective cohort study. Ultrasound Obstet. Gynecol. 2020, 56, 173–181. [Google Scholar] [CrossRef]
- Morales-Rosello, J.; Khalil, A.; Morlando, M.; Papageorghiou, A.; Bhide, A.; Thilaganathan, B. Changes in fetal Doppler indices as a marker of failure to reach growth potential at term. Ultrasound Obstet. Gynecol. 2014, 43, 303–310. [Google Scholar] [CrossRef]
- Molina, L.C.G.; Odibo, L.; Zientara, S.; Običan, S.G.; Rodriguez, A.; Stout, M.; Odibo, A.O. Validation of Delphi procedure consensus criteria for defining fetal growth restriction. Ultrasound Obstet. Gynecol. 2020, 56, 61–66. [Google Scholar] [CrossRef]
- Baschat, A.A. Neurodevelopment after fetal growth restriction. Fetal Diagn. Ther. 2014, 36, 136–142. [Google Scholar] [CrossRef]
- Murray, E.; Fernandes, M.; Fazel, M.; Kennedy, S.H.; Villar, J.; Stein, A. Differential effect of intrauterine growth restriction on childhood neurodevelopment: A systematic review. BJOG 2015, 122, 1062–1072. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | N (%) |
|---|---|
| Age (years) | 34 ± 6.8 |
| Ethnicity (white) | 86 (84.3%) |
| Primiparity | 60 (58.8%) |
| Assisted reproductive technology | 3 (2.9%) |
| Body mass index (BMI) ≥ 30kg/m2 | 5 (4.9%) |
| Smoking | 23 (22.5%) |
| Pre-gestational and gestational diabetes | 12 (11.8%) |
| Hypertension (chronic and gestational) | 12 (11.7%) |
| Renal disease | 2 (2%) |
| Autoimmune disease | 3 (3%) |
| Prophylactic aspirin intake | 8 (7.8%) |
| Previous PE/HELLP | 6 (5.9%) |
| Prior delivery with BW below the 10th centile and IUFD | 2 (1.9%) |
| Prior delivery with BW below the 10th centile | 23 (22.5%) |
| PE/HELLP in current pregnancy | 10 (9.8%) |
| GA at birth (weeks ± days) | 37.6 ± 11.3 |
| Delivery ≥ 37 weeks of gestation | 71 (70%) |
| Mode of delivery | |
| Spontaneous vaginal delivery | 34 (33.3%) |
| Instrumental vaginal delivery | 9 (8.8%) |
| Cesarean section | 59 (57.8%) |
| Predicted/confirmed BW below 10th percentile | 90 (88%) |
| Birth weight (g) | 2281 ± 388 |
| Variables | N (%) |
|---|---|
| GA at diagnosis (weeks ± days) | 36.0 ± 1.1 |
| GA at last ultrasound before delivery (weeks ± days) | 37.0 ± 1.4 |
| EFW (g) | 2209 ± 366 |
| EFW < 3rd percentile | 90 (88%) |
| EFW < 10th and ≥ 3rd percentile | 9 (8.8%) |
| EFW > 10th percentile CPR at last ultrasound before delivery | 3 (2.9%) 1.53 ± 0.5 |
| Middle cerebral artery PI | 1.44 ± 0.3 |
| Umbilical artery PI | 1.0 ± 0.3 |
| Time interval between last ultrasound and delivery (days) | 3.31 ± 3.4 |
| Variables | Adverse Outcome N = 43 | Good Outcome N = 59 | p Value |
|---|---|---|---|
| GA at last ultrasound (weeks ± days) | 36.1 ± 8.8 | 37.4 ± 8.5 | <0.001 |
| Time interval last ultrasound to delivery (days) | 2.4 ± 2.8 | 4.0 ± 3.6 | 0.017 |
| CPR at last ultrasound | 1.4 (0.49) | 1.6 (0.48) | 0.014 |
| GA at delivery (weeks ± days) | 36.6 ± 10.0 | 38.4 ± 9.6 | <0.001 |
| Preterm delivery (<37 weeks) | 24 (56%) | 7 (12%) | <0.001 |
| Female gender | 21 (49%) | 36 (61%) | 0.23 |
| Birth weight (g) | 2059 ± 361 | 2443 ± 325 | <0.001 |
| Birth weight percentile groups (FGR) | |||
| <3rd centile | 22 (51%) | 26 (44%) | |
| <10th and ≥3rd percentile ≥10th percentile | 17 (40%) 4 (9.3%) | 28 (47%) 5 (8.5%) | |
| Predicted/confirmed birth weight < 10th percentile | 38 (88%) | 52 (88%) | 1.00 |
| Mode of delivery | |||
| Spontaneous vaginal delivery | 9 (21%) | 25 (42%) | 0.033 |
| Instrumental vaginal delivery | 4 (9.3%) | 5 (8.5%) | 1.00 |
| Cesarean section | 30 (70%) | 29 (49%) | 0.044 |
| Arterial cord pH | |||
| pH < 7.15 | 6 (14%) | 0 (0.00%) | 0.005 |
| Apgar at 5 min < 7 | 3 (7.0%) | 0 (0.00%) | 0.07 |
| NICU admission | 34 (79%) | 0 (0.00%) | <0.001 |
| Duration of NICU hospitalization | 10 (0–88) * | 0 | |
| Neonatal morbidity (overall) | 32 (74%) | 0 (0.00%) | <0.001 |
| Hypoglycemia | 15 (35%) | 0 (0.00%) | <0.001 |
| Hyperbilirubinemia | 13 (30%) | 0 (0.00%) | <0.001 |
| Respiratory distress syndrome | 8 (19%) | 0 (0.00%) | <0.001 |
| Apnea-bradycardia | 7 (16%) | 0 (0.00%) | 0.002 |
| Hypothermia | 2 (4.7%) | 0 (0.00%) | 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zdanowicz, J.A.; Disler, M.; Gerull, R.; Raio, L.; Surbek, D. Is the Cerebro-Placental Ratio Sufficient to Predict Adverse Neonatal Outcome in Small for Gestational Age Fetuses > 34 Weeks of Gestation? Reprod. Med. 2021, 2, 2-11. https://0-doi-org.brum.beds.ac.uk/10.3390/reprodmed2010002
Zdanowicz JA, Disler M, Gerull R, Raio L, Surbek D. Is the Cerebro-Placental Ratio Sufficient to Predict Adverse Neonatal Outcome in Small for Gestational Age Fetuses > 34 Weeks of Gestation? Reproductive Medicine. 2021; 2(1):2-11. https://0-doi-org.brum.beds.ac.uk/10.3390/reprodmed2010002
Chicago/Turabian StyleZdanowicz, Jarmila A., Muriel Disler, Roland Gerull, Luigi Raio, and Daniel Surbek. 2021. "Is the Cerebro-Placental Ratio Sufficient to Predict Adverse Neonatal Outcome in Small for Gestational Age Fetuses > 34 Weeks of Gestation?" Reproductive Medicine 2, no. 1: 2-11. https://0-doi-org.brum.beds.ac.uk/10.3390/reprodmed2010002