2.1. GCH System 2.0
In this section, the main components of GCH 2.0 are described, emphasizing the main improvements carried out on the previous prototype [
13].
The core of GCH 2.0 System consists of the coupling of a miniature force sensor, an Exact Sensor Instrument’s EX601D (Shenzhen Exact Sensor Instrument Co., Ltd., Shenzhen, China) [
18], within the distal part of the forearm crutch shaft. Compression load cell features include: cylindrical (in the shape of a coin), diameter of 19 mm, stainless steel measuring element, hermetically sealed (fully welded) and easy installation. Safe load limit = 100 kg, rated output = 0.7198 mV/V, linearity ≤0.05% Full Scale (FS), hysteresis ≤0.05% FS, repeatability ≤0.03% FS, Zero balance ±2% FS and operating temperature range = −20 °C to 60 °C.
The said cell is connected to the electronic board and power batteries housed in this area. The data acquisition card has the function of emitting a radiofrequency signal. The communication protocol used is SimpliciTI, a low-power Radio Frequency (RF) protocol from Texas Instruments Inc. (Dallas, Texas, USA) [
19] at 898 MHz with a period of 80 samples per second. The digital and amplified signal arrives at an ultra low power MSP430 microcontroller also from Texas Instruments (input voltage 2.4 V DC—Direct Current, battery/autonomy 6000 mAh).
GCH 2.0, as opposed to GCH 1.0 [
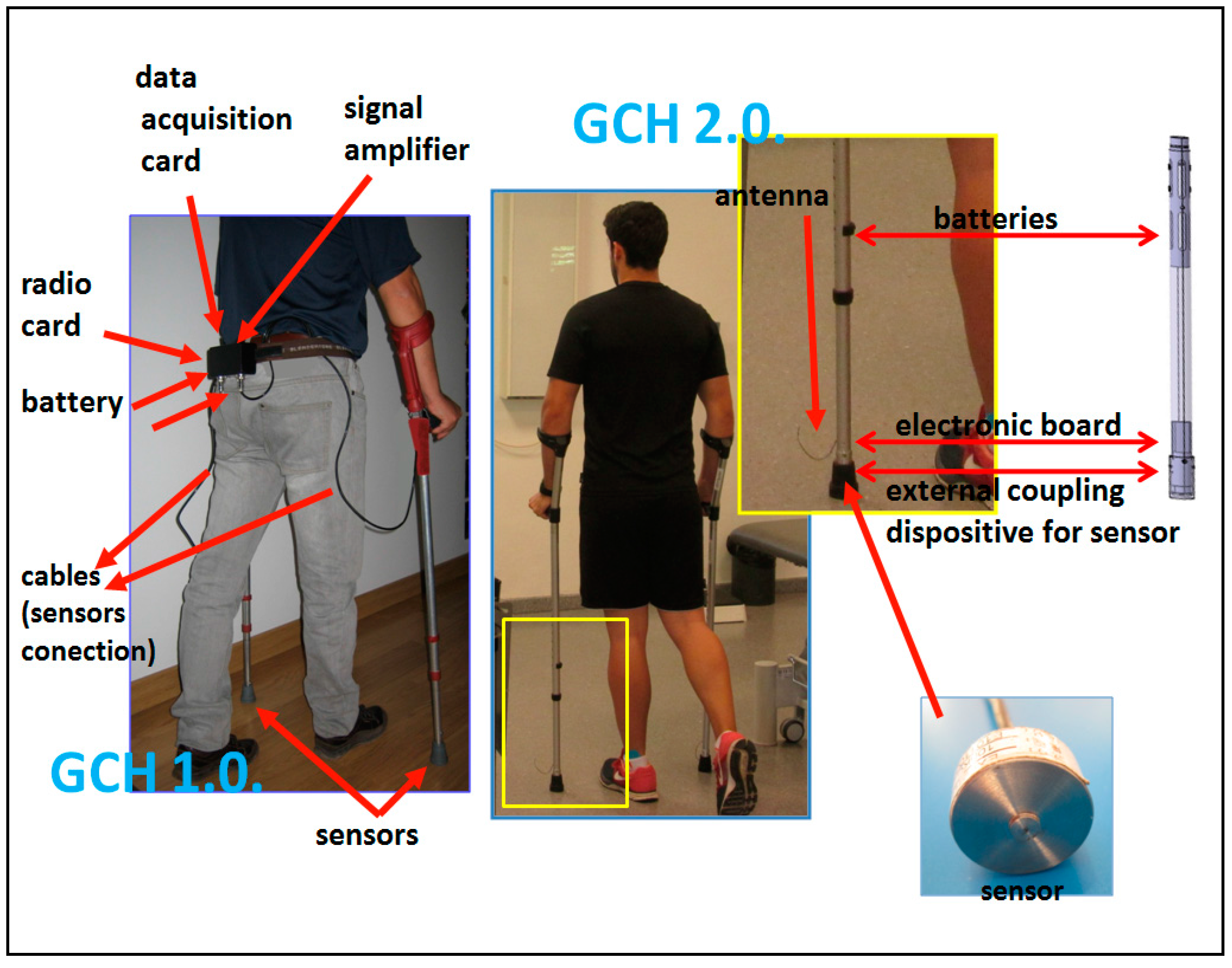
12], introduces a compact design of the system integrating all these elements inside the crutch shaft. The sensor with its coupling mechanism; the data acquisition and radio cards, incorporated in a single printed circuit board (PCB); and the power supply are integrated in the most distal part of the crutch, an independent and extensible pipe to allow for the height adjustment tube (
Figure 1). All external cables are eliminated. Manufacture of the PCB has been conducted with miniature electronic components, as a surface mount device (SMD). This allows us to integrate electronics inside the crutch, unlike the first prototype that wired the sensor installed inside the crutch with an external box that patients had to carry in their belt.
It is worth noting that when the GCH 2.0 crutch is started, the offset process is automatically activated. Once the crutch is on, it is placed vertically on the floor for 5 s, thus its weight is not recorded. This method allows us to exchange or add the usual standard components to the crutches (ergonomic handles, casings, beads, etc.) without the weight difference affecting measurements.
One of our main objectives with this new system is to provide a compact and ready-to-use device that could be used not only in clinical trials or under direct supervision by the physiotherapist, but also during daily life, thus speeding up the patient’s recovery. With this aim in mind, a clock-shaped, portable receiver has been introduced that can be used independently by the patient while performing the aided gait with crutches even outdoors. Thus, not only would they walk on stable ground within a room, but they could also walk on steps, ramps or uneven floors,
i.e., the usual outdoor obstacles and difficulties [
20]. In addition, thanks to the use of a compact force sensor, GCH 2.0 does not require frequent calibrations.
Regarding the batteries, we decided to replace them with double standard AA that, together with an adapter, were also integrated inside the crutch, with a minimum amperage of 3000 mA each to prolong their use. The batteries are directly rechargeable through a connector or by extracting them and using a standard charger. This latter mode allows the user to replace the batteries while the used ones are being charged so that the crutches are available at all times.
The design of a specific program has been another major improvement in the applicability of GCH 2.0 as a measurement tool. The Crossbow sensor of GCH System 1.0 emitted signals that were monitored and recorded by a generic program called Moteview 2.0 (Moog Crossbow, East Aurora, NY, USA) [
21]. This program works at a frequency of 0 to 10 Hz, so that even using the maximum frequency, the curve recorded was not accurate enough. The new GCH 2.0 software (called GCH Control Software 1.0) records data up to 80 Hz, thus obtaining a more optimized curve of weight bearing at each step. The basic application covers one or two modules (one for each crutch), although the system is able to cover more. That is, many patients can be walking with instrumented crutches at the same time. The signal sent by the crutches is detected by a small USB receiver that is connected to a computer (“fixed system”) by means of a virtual COM (Communication) port, or by a receptor incorporated into a watch, mobile phone, pendant or substitute (the “portable system” described before). This portable receiver provides autonomy to the patient in order to perform aided gait outdoors.
The fixed system is used during patient care in the clinic or laboratory as a training or research object, respectively. The software translates the millivolts from the sensor signal into units of force (force kilograms—kg), records the data, analyzes them and allows their numerical and graphical display of the loads that the subject carries out on screen in real-time. Besides specific graphs of weight bearing by each crutch, the unification or overlapping of both are obtained. These graphs can be seen by the patient through a canon projector to perform a visual feedback during gait.
This visual feedback is part of what we call a “self-correcting” mechanism. Thanks to this mechanism, new in GCH 2.0, the patient receives acoustic and/or visual information about the load exerted on the crutches. The visual feedback is based on the above-mentioned projection on a screen of the amount of load exerted, which is directly proportional to the injured lower member unloading. This feature is mainly intended for patient’s training during physiotherapy sessions. On the other hand, the acoustic feedback allows the system to be used without supervision even outdoors. With this self-correcting mechanism, if the amount of load is wrong, the subject is able to increase or reduce the force to improve the accuracy and exactly manage the ideal load recommended by the physiotherapist.
Finally, the program contains a database specifically designed for patients, in which we can record all their data and the applied sessions with our tool. Likewise, the recordings of the loads applied, number of steps, mistakes made, etc., are designed for their posterior analysis within the care or research area.
The System was registered at the Spanish Patent and Trademark Office with number P201031779, and international expansion has been carried out [
22]. A summary of all the improvements is shown in
Table 1.
Basic Functions of the GCH System 2.0
From an operational point of view, the two main functions of GCH 2.0 are:
Load control. The objective measurement of the loads applied to the crutches is the basis of the System. It shows the kilograms exerted on the crutches and the percentage of patient body weight (PPBW). This datum is the most relevant in the clinic, which always requires the subject’s current weight to be entered. The percentages allow researchers to compare intra-subject and inter-subject tests in order to establish treatment protocols.
Feedback mechanism. The feedback information includes, individually, the ideal load exerted on the crutches (directly proportional to the unloading on the injured lower member), PPBW, according to the pathology and the treatment phase, introduced into the software as well as a percentage of error tolerated clinically due to excess or defect load. The fixed system alerts the subject of the mistakes made during gait for immediate self-correction (
Figure 2). Acoustic signals, a continuous whistling, will be used if the recommended load is exceeded or discontinuous if it does not reach it; and visual, by using a projector. The portable system only uses an audible feedback. The fixed system shows only the feedback information useful for the patient’s training in the projector, and additional personalized clinical information (useful for the physiotherapist/researcher) on the computer screen.
The inclusion of the patient’s weight especially benefits the functionality of the program, since it allows us to extrapolate load amounts to PPBW [
9], both in the recommendation of the ideal weight as well as the margins of errors allowed. This offers the possibility of performing intra-subject and inter-subject comparisons. Only in this way can we advance towards the creation of protocols of performance based on scientific evidence [
24].
2.4. Measurements and Participants
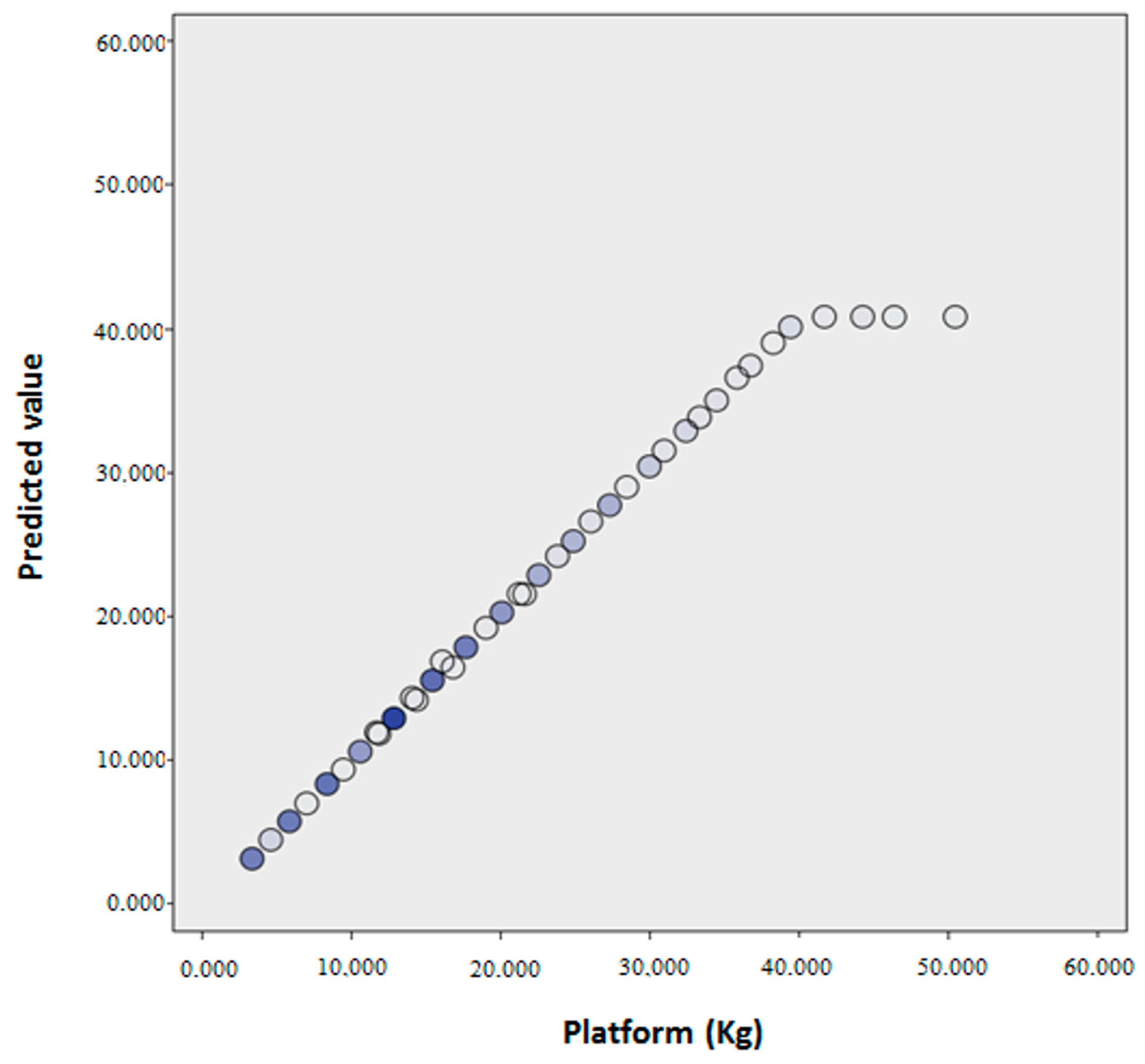
The measurements were made by means of the GCH System 2.0 and the AMTI Platform during the assisted gait carried out by 30 participants, 18 women (66.7%) and 12 men (33.3%), with an age range from 18 to 45 years (mean = 29.87 years; Standard Deviation SD = 7.26).
Different PPBW applied to the crutches were requested in order to obtain heterogeneous measurements during gait. The sampling was considered non-probabilistic due to guidelines provided. We obtained loads between 2.13 kg and 50.60 kg.
For each crutch (2) and participant (30), nine measurements were taken. Of these, three belonged to a requested load on the crutch at 10% of body weight, another three at 25% and three more at 50% or the maximum possible. A total of 540 measurements were taken (270 with each crutch). These values were compared with the 540 measurements undertaken by the force platform. The number of measurements (540) is high enough according to the required sample size when comparing two means in two samples [
27].
Finally, participants were also selected in a non-probabilistic and convenience mode.
Inclusion Criteria
healthy subjects between 18 and 60 years old with previous experience with crutches;
presenting a normal gait, being asymptomatic on walking at free cadence;
overcome a simple test of static equilibrium, consisting of keeping one’s balance on each foot for 30 s without great bodily movements [
26].
Exclusion Criteria
The research protocol was approved by the ethics committee of the University Hospital Virgen Macarena (Seville, Spain). All participants gave written informed consent prior to participation in the study.
2.5. Data Collection
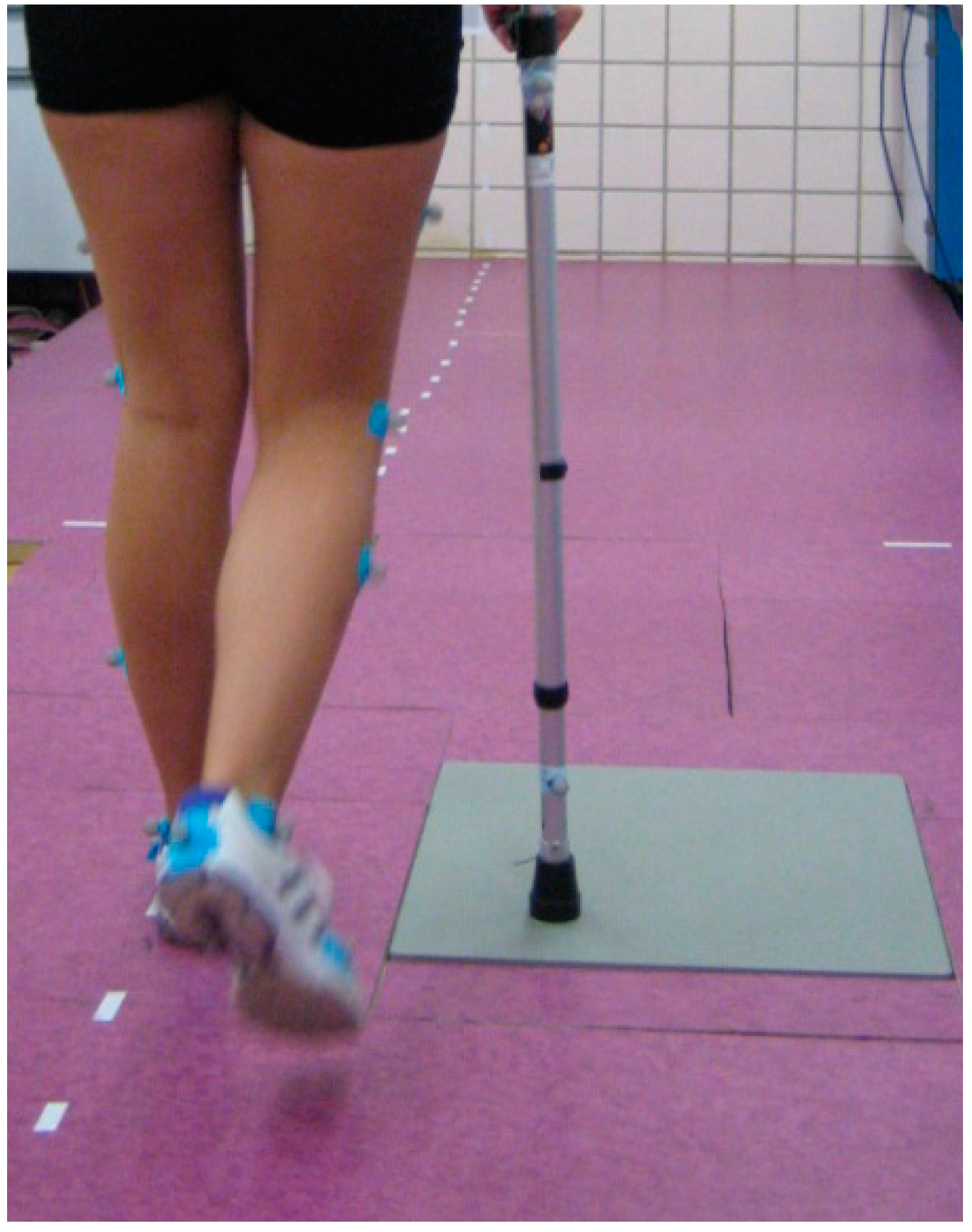
The measurements carried out by the two systems during aided gait were taken simultaneously and under the same conditions. The biomechanics laboratory includes a walking corridor 8.5 m long. The force platform was located halfway along the walk. Laterally, and along this corridor, signals were placed in a straight line that offered: the control of the gait direction and a distracting effect that prevented the subjects from centering their attention on the Platform so as to make the crutches match it (
Figure 3).
To avoid differences among the tests, the laboratory always used the same artificial light (with lowered blinds) and a constant temperature (25 °C). This data is relevant as the subjects were asked to do physical activity and wear special clothes (sports short, short-sleeved T-shirt and sports shoes).
The participants first had a learning and familiarization period followed by them completing an 8.5 m walk, 10 times with each crutch and with each load percentage (10%, 25% and 50% or maximum possible). Aided gait with a partial load was in two stages, with a contra-lateral crutch and simultaneous heel and crutch support. The chosen height of the crutch was associated with an elbow flexion of 20° to 30° [
28,
29]. The required speed was at free cadence.
Data collection was performed 10 times with the right crutch and 10 more with the left in each load modality and every patient. Of the valid measurements, we took the three central ones to conduct our statistical analysis. GCH Control Software was used with the GCH System 2.0 and Vicon Nexus (Vicon, Oxford, UK) with the AMTI Platform, controlled by two researchers who recorded the load applied when a crutch matched the Platform. Subsequently, the timing and scoring reference of this support was recorded to correlate the data from both pieces of software in time.
Both measurement systems started at offset or zero, so the weight of the implemented crutch, 0.720 kg, was subtracted from the values of the Platform.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}