Machine Learning Methods Applied to Predict Ventilator-Associated Pneumonia with Pseudomonas aeruginosa Infection via Sensor Array of Electronic Nose in Intensive Care Unit


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
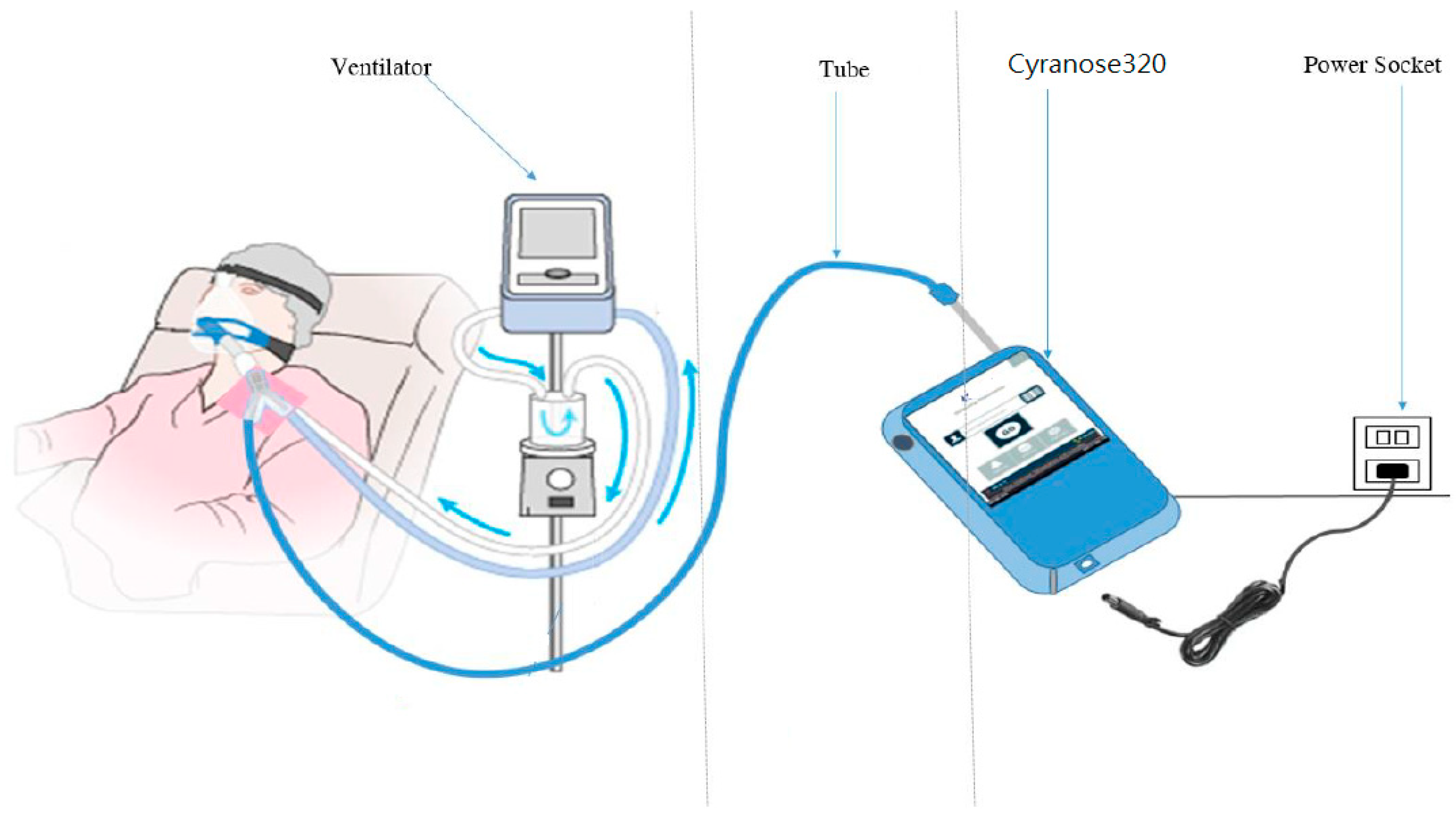
2.1. Database
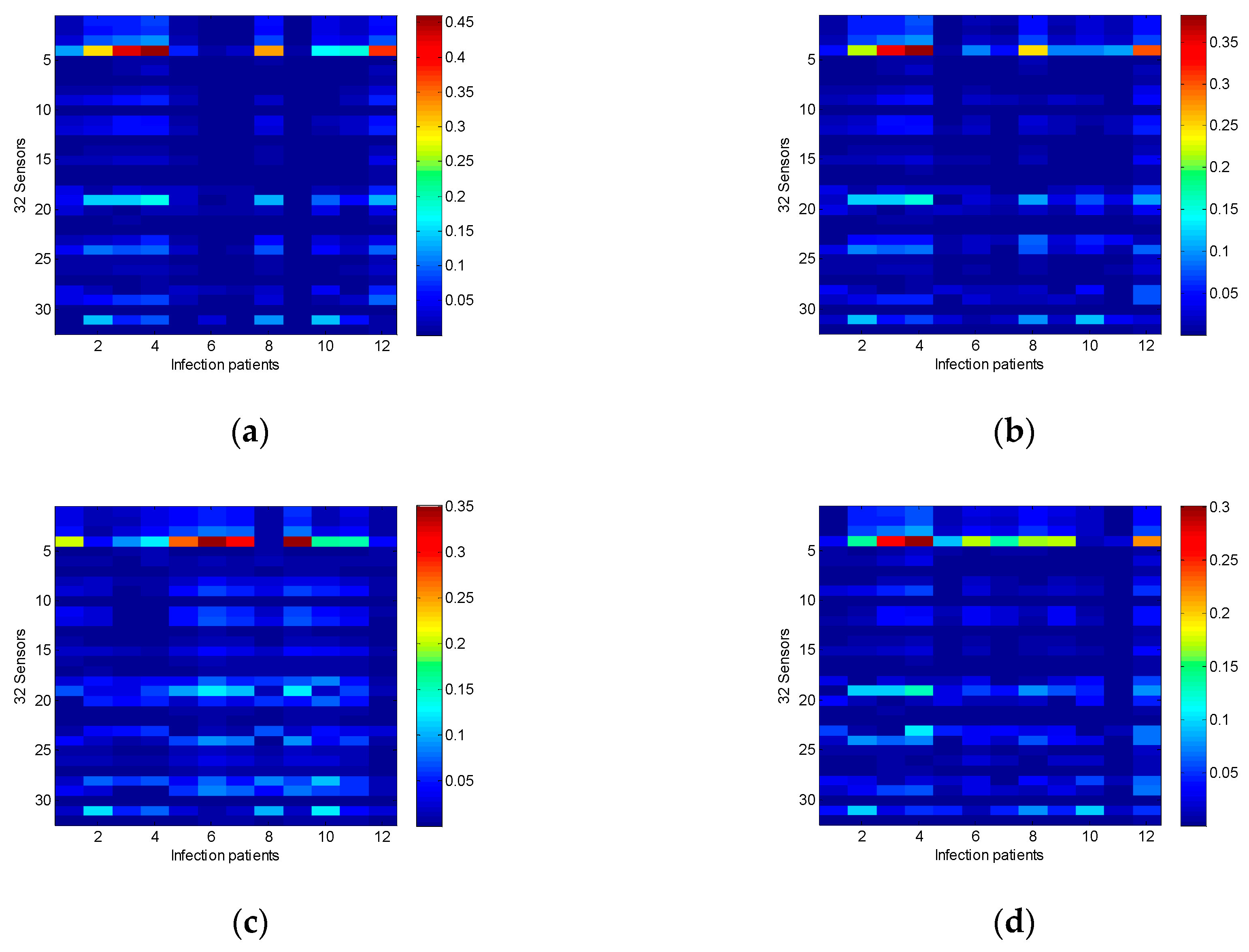
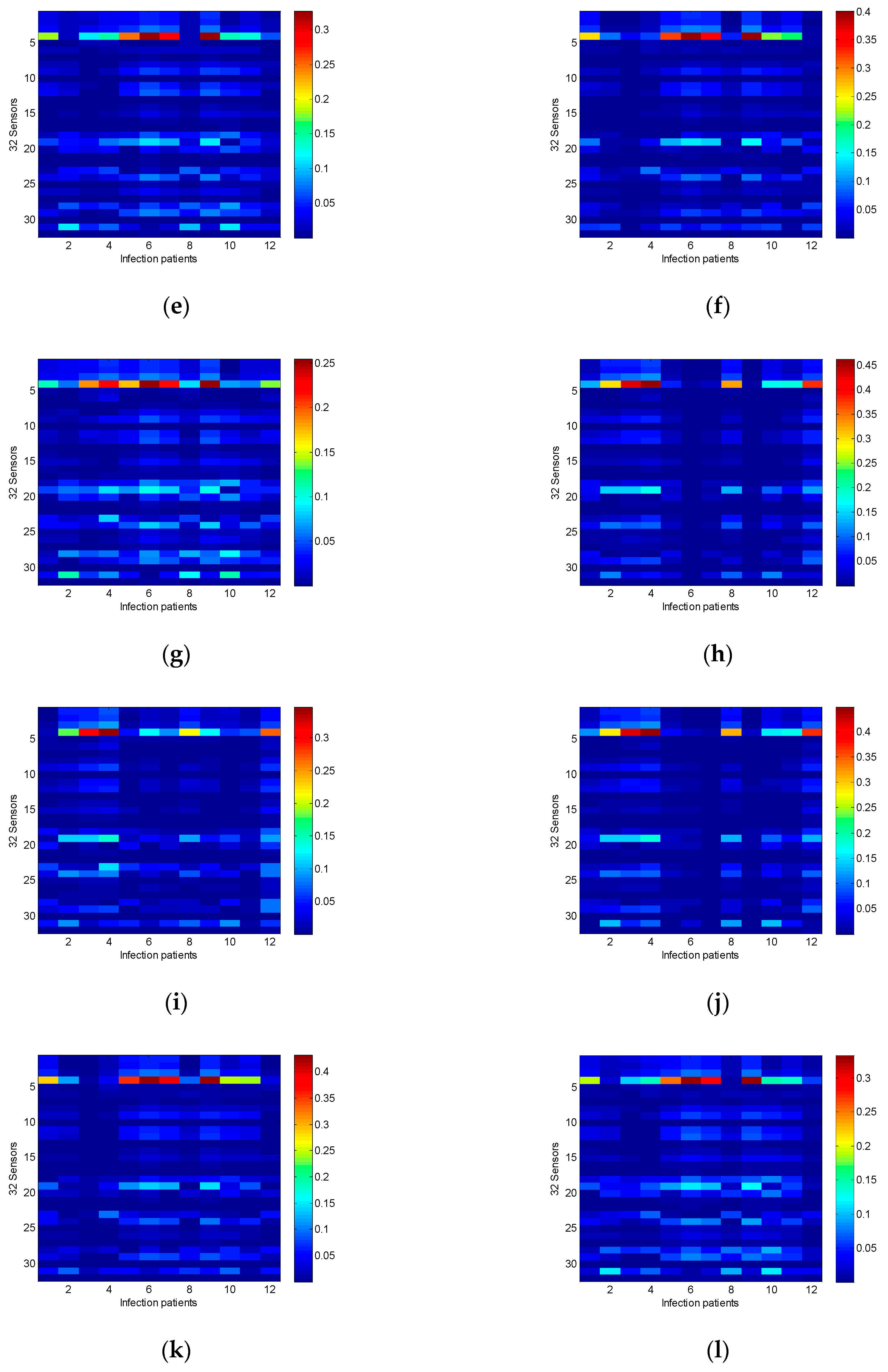
2.2. Sensor Array Sensitivity Analysis
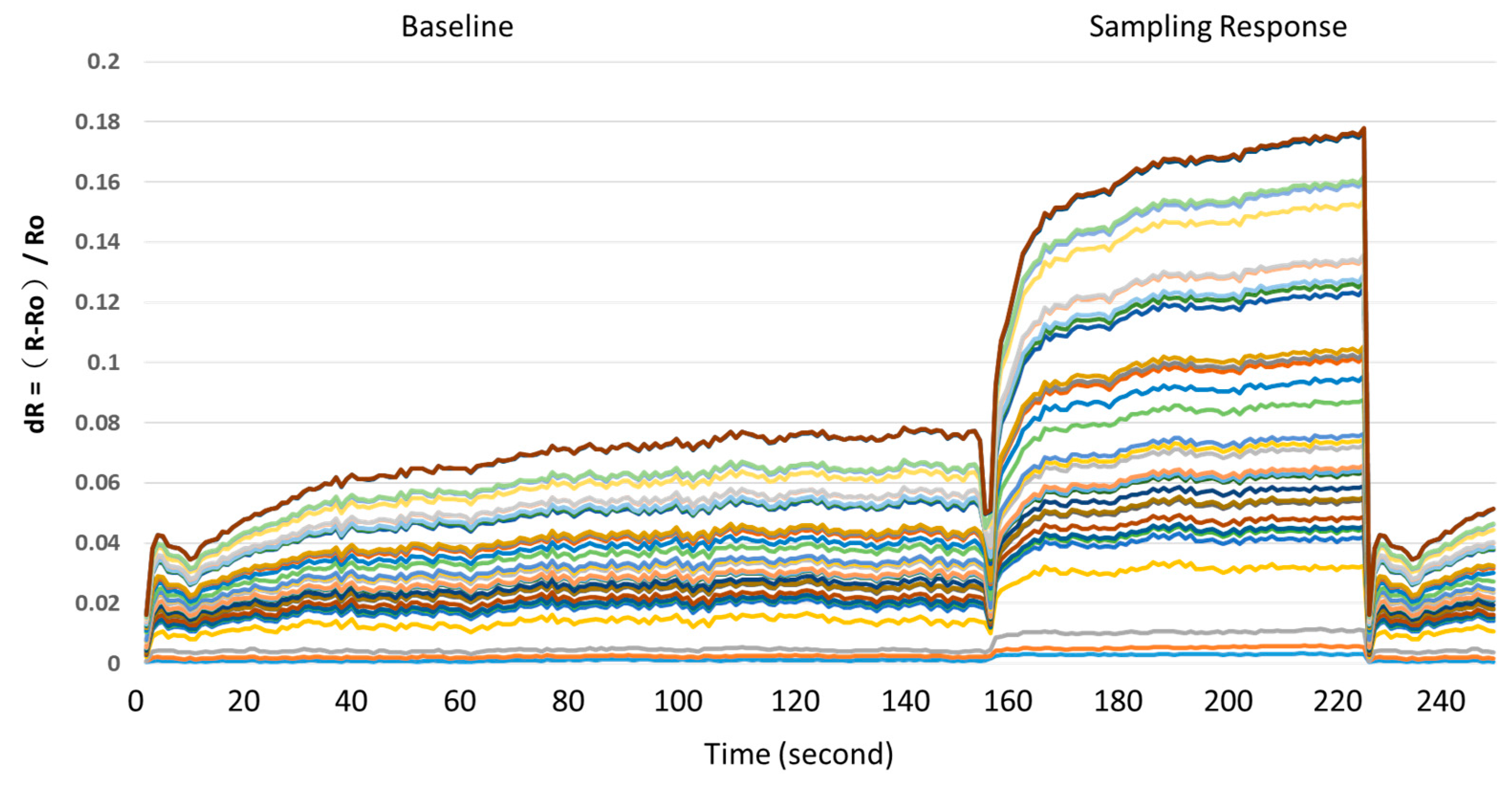
2.3. Data Preprocess
2.4. Architecture of Ensemble Neural Networks
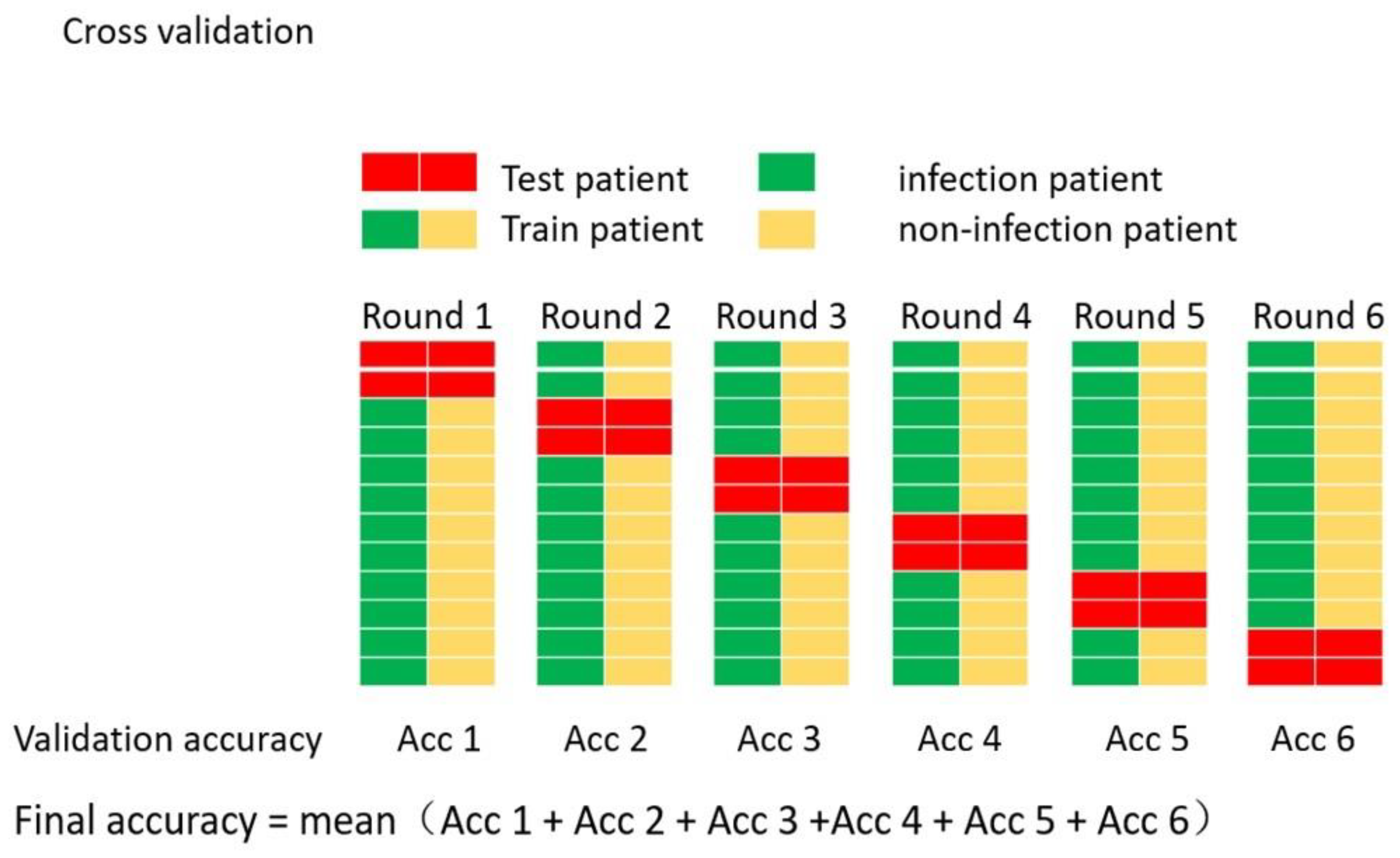
- First, randomly select four cases from the database as the testing dataset, including two infection cases and two non-infection cases. Each case includes 140 patients’ data.
- The rest of the database was divided into five segments (dataset1, dataset2, ..., dataset5). Each dataset includes two infection cases and two non-infection cases. Randomly select four datasets as the training datasets, the remaining dataset is the validation dataset to check the model for over-fitting. This step is repeated five times such that five different training datasets and one validation dataset are produced. Each training and validation dataset were used to train 10 networks with different initial weights.
- After the training process is finalized, the testing dataset is applied to test the classification accuracy and generalization of the ANN classifier, then the best network in each training and validation datasets are selected to be combined into the ensemble model.
- Finally, an ENN model constructed by five networks is established. The output of the ENN model is the average of five best networks.
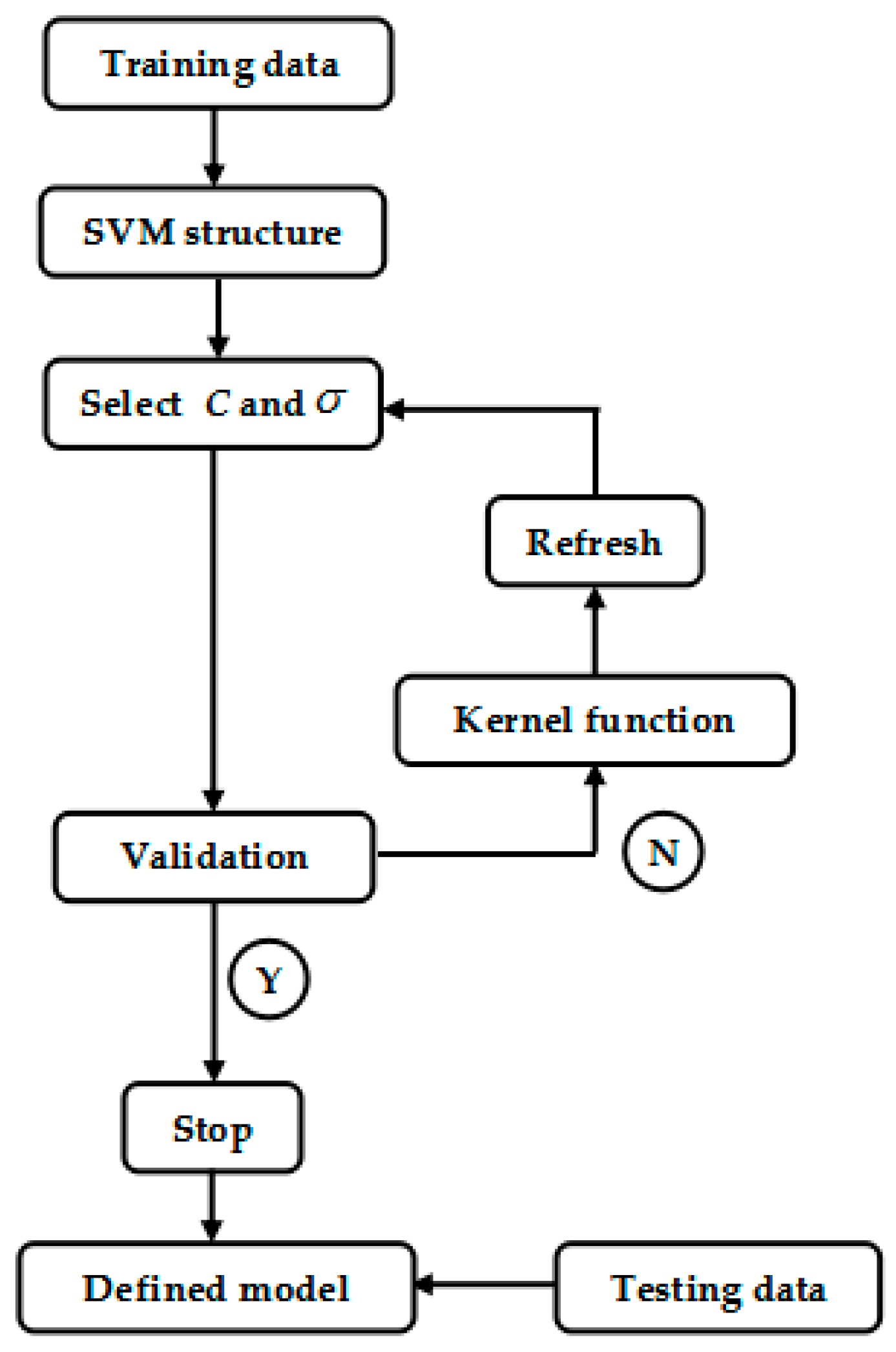
2.5. Architecture of SVM
2.6. Evaluate the SVM Predictive Performance
3. Results
3.1. Prediction Ability of the ENN Model
3.2. Prediction Ability of the SVM Model
3.3. ROC Curve Analysis
4. Conclusions and Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Chastre, J.; Fagon, J. Ventilator-associated pneumonia. Am. J. Resp. Crit. Care Med. 2002, 165, 867–903. [Google Scholar] [CrossRef]
- Morehead, R.; Pinto, S. Ventilator-associated pneumonia. Arch. Intern. Med. 2000, 160, 1926–1936. [Google Scholar] [CrossRef] [PubMed]
- Torres, A. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [PubMed]
- Disease Control Bureau, Ministry of Health and Welfare, Taipei. Statistical Report on the Cause of Death; Disease Control Bureau, Ministry of Health and Welfare: Taipei, Taiwan, 2017.
- Di Francesco, F.; Fuoco, R.; Trivella, M.G.; Ceccarini, A. Breath analysis: Trends in techniques and clinical applications. Microchem. J. 2005, 79, 405–410. [Google Scholar] [CrossRef]
- Dweik, R.A.; Amann, A. Exhaled breath analysis: The new frontier in medical testing. J. Breath Res. 2008, 2, 030301. [Google Scholar] [CrossRef]
- Bikov, A.; Lazar, Z.; Horváth, I. Established methodological issues in electronic nose research: How far are we from using these instruments in clinical settings of breath analysis? J. Breath Res. 2015, 9, 34001. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.-R.; Chang, Y.-H.; Kao, M.-T.; Wang, H.-H.; Hong, R.-I.; Lin, Y.-J. Application of the electronic nose for uremia diagnosis. Sens. Actuators B Chem. 2001, 76, 177–180. [Google Scholar]
- Voss, A.; Baier, V.; Reisch, R.; Von Roda, K.; Elsner, P.; Ahlers, H.; Stein, G. Smelling Renal Dysfunction via Electronic Nose. Ann. Biomed. Eng. 2005, 33, 656–660. [Google Scholar] [CrossRef]
- Tang, K.-T.; Chiu, S.-W.; Chang, M.-F.; Hsieh, C.-C.; Shyu, J.-M. A Low-Power Electronic Nose Signal-Processing Chip for a Portable Artificial Olfaction System. IEEE Trans. Biomed. Circuits Syst. 2011, 5, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Bono, R.; Pennazza, G.; Santonico, M.; Mantini, G.; Bernabei, M.; Zarlenga, M.; Roscioni, C.; Martinelli, E.; Paolesse, R.; Di Natale, C.; et al. Identification of melanoma with a gas sensor array. Ski. Res. Technol. 2008, 14, 226–236. [Google Scholar]
- Yu, J.; Byun, H.; So, M.; Huh, J. Analysis of diabetic patient’s breath with conducting polymer sensor array. Sens. Actuators B. Chem. 2005, 108, 305–308. [Google Scholar] [CrossRef]
- Dalton, P.; Gelperin, A.; Preti, G. Volatile Metabolic Monitoring of Glycemic Status in Diabetes Using Electronic Olfaction. Technol. Ther. 2004, 6, 534–544. [Google Scholar] [CrossRef] [PubMed]
- Blatt, R.; Bonarini, A.; Calabrò, E.; Della Torre, M.; Matteucci, M.; Pastorino, U. Lung Cancer Identification by an Electronic Nose based on an Array of MOS Sensors. In Proceedings of the 2007 International Joint Conference on Neural Networks, Orlando, FL, USA, 12–17 August 2007; pp. 1423–1428. [Google Scholar]
- Di Natale, C.; Macagnano, A.; Martinelli, E.; Paolesse, R.; D’Arcangelo, G.; Roscioni, C.; Finazzi-Agrò, A.; D’Amico, A. Lung cancer identification by the analysis of breath by means of an array of non-selective gas sensors. Biosens. Bioelectron. 2003, 18, 1209–1218. [Google Scholar] [CrossRef]
- Dragonieri, S.; Schot, R.; Mertens, B.J.; Le Cessie, S.; Gauw, S.A.; Spanevello, A.; Resta, O.; Willard, N.P.; Vink, T.J.; Rabe, K.F.; et al. An electronic nose in the discrimination of patients with asthma and controls. J. Clin. Immunol. 2007, 120, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Kunos, L.; Bikov, A.; Lazar, Z.; Korosi, B.Z.; Benedek, P.; Losonczy, G.; Horvath, I. Evening and morning exhaled volatile compound patterns are different in obstructive sleep apnoea assessed with electronic nose. Sleep Breath 2015, 19, 247–253. [Google Scholar] [CrossRef]
- Phillips, M. Method for the Collection and Assay of Volatile Organic Compounds in Breath. Anal. Biochem. 1997, 247, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Thaler, E.R.; Hanson, C.W. Medical applications of electronic nose technology. Rev. Med Devices 2005, 2, 559–566. [Google Scholar] [CrossRef]
- Davis, K.A. Ventilator-Associated Pneumonia: A Review. J. Intensiv. Care Med. 2006, 21, 211–226. [Google Scholar] [CrossRef]
- Geraldes, L.; Todo-Bom, A.; Loureiro, C. Airways inflammation evaluation. Upper and lower airways. Rev. Port. Pneumol. 2009, 15, 443–460. [Google Scholar] [CrossRef]
- Boots, A.W.; Van Berkel, J.J.B.N.; Dallinga, J.W.; Smolinska, A.; Wouters, E.F.; Van Schooten, F.J. The versatile use of exhaled volatile organic compounds in human health and disease. J. Breath Res. 2012, 6, 27108. [Google Scholar] [CrossRef]
- Bos, L.D.J.; Sterk, P.J.; Schultz, M.J. Volatile Metabolites of Pathogens: A Systematic Review. PLoS Pathog. 2013, 9, e1003311. [Google Scholar] [CrossRef]
- Schnabel, R.; Boumans, M.; Smolinska, A.; Stobberingh, E.; Kaufmann, R.; Roekaerts, P.; Bergmans, D. Electronic nose analysis of exhaled breath to diagnose ventilator-associated pneumonia. Respir. Med. 2015, 109, 1454–1459. [Google Scholar] [CrossRef] [PubMed]
- Wong, M. Detection of Electronic Nasal Pneumonia Using Pattern Recognition; National Tsinghua University: Hsinchu, Taiwan, 2013; pp. 20–24. [Google Scholar]
- Scott, S.; James, D.; Ali, Z. Review data analysis for electronic nose systems. Microchim. Acta 2007, 15, 183–207. [Google Scholar]
- Sadrawi, M.; Fan, S.-Z.; Abbod, M.F.; Jen, K.-K.; Shieh, J.-S. Computational Depth of Anesthesia via Multiple Vital Signs Based on Artificial Neural Networks. Biomed Res. Int. 2015, 2015, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Chen, Y.-F.; Fan, S.-Z.; Abbod, M.F.; Shieh, J.-S. EEG Signals Analysis Using Multiscale Entropy for Depth of Anesthesia Monitoring during Surgery through Artificial Neural Networks. Comput. Math. Methods Med. 2015, 2015, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Ma, L.; Chiu, R.-C.; Fan, S.-Z.; Abbod, M.F.; Shieh, J.-S.; Boonstra, T. HRV-derived data similarity and distribution index based on ensemble neural network for measuring depth of anaesthesia. PeerJ 2017, 5, 30. [Google Scholar]
- Chapelle, O.; Vapnik, V. Model selection for support vector machines. In Advances in Neural Information Processing Systems; MIT Press: Cambridge, MA, USA, 2000; Volume 12, pp. 230–236. [Google Scholar]
- Gold, C.; Sollich, P. Model selection for support vector machine classification. Neurocomputing 2003, 55, 221–249. [Google Scholar] [CrossRef]
- Anguita, D.; Ridella, S.; Rivieccio, F. Hyper parameter design criteria for support vector classifiers. Neuro Comput. 2003, 55, 109–134. [Google Scholar]
- Ancona, N.; Cicirelli, G.; Distance, A. Complexity reduction and parameter selection in support vector machines. In Proceedings of the 2002 International Joint Conference on Neural Networks, Honolulu, HI, USA, 12–17 May 2002; pp. 2375–2380. [Google Scholar]
- Amann, A.; Costello, B.D.L.; Miekisch, W.; Schubert, J.; Buszewski, B.; Pleil, J.; Ratcliffe, N.; Risby, T. The human volatilome: Volatile organic compounds (VOCs) in exhaled breath, skin emanations, urine, feces and saliva. J. Breath Res. 2014, 8, 34001. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, R.; Fijten, R.; Smolinska, A.; Dallinga, J.; Boumans, M.-L.; Stobberingh, E.; Boots, A.; Roekaerts, P.; Bergmans, D.; Van Schooten, F.J. Analysis of volatile organic compounds in exhaled breath to diagnose ventilator-associated pneumonia. Sci. Rep. 2015, 5, 17179. [Google Scholar] [CrossRef]
- Laakso, O.; Haapala, M.; Jaakkola, P.; Laaksonen, R.; Luomanmäki, K.; Nieminen, J.; Pettersson, M.; Päivä, H.; Räsänen, M.; Himberg, J.J. FT-IR breath test in the diagnosis and control of treatment of methanol intoxications. J. Anal. Toxicol. 2001, 25, 26–30. [Google Scholar] [CrossRef]
- Van den Velde, S.; Nevens, F.; Van hee, P.; van Steenberghe, D.; Quirynen, M. GC-MS analysis of breath odour compounds in liver patients. J. Chromatogr. B 2008, 875, 344–348. [Google Scholar] [CrossRef]
- Amann, A.; Poupart, G.; Telser, S.; Ledochowski, M.; Schmid, A.; Mechtcheriakov, S. Applications of breath gas analysis in medicine. Int. J. Mass Spectrom. 2004, 239, 227–233. [Google Scholar] [CrossRef]
- Pearce, T.; Schiffman, S.; Nagle, H.; Gardner, J. Handbook of Machine Olfaction: Electronic Nose Technology; Wiley: Hoboken, NJ, USA, 2006. [Google Scholar]
- Gardner, J.; Bartlett, P. Sensors and Sensory Systems for an Electronic Nose; Springer: New York, NY, USA, 1992. [Google Scholar]
- Dutta, R.; Hines, E.L.; Gardner, J.W.; Boilot, P. Bacteria classification using Cyranose 320 electronic nose. Biomed. Eng. 2002, 1, 4. [Google Scholar]
- Hansen, L.; Salam, P. Neural network ensembles. Trans. Pattern Anal. Mach. Intell. 1990, 12, 993–1001. [Google Scholar] [CrossRef]
- Zhou, Z.-H.; Wu, J.; Tang, W. Ensembling neural networks: Many could be better than all. Artif. Intell. 2002, 137, 239–263. [Google Scholar] [CrossRef]
- Bhavsar, H.; Ganatra, A. Increasing Efficiency of Support Vector Machine using the Novel Kernel Function: Combination of Polynomial and Radial Basis Function. Int. J. Adv. Comput. Theory Eng. 2014, 3, 17–24. [Google Scholar]
- Ye, Z.; Li, H. Based on radial basis kernel function of support vector machines for speaker. In Proceedings of the 5th International Congress on Image and Signal Processing, Chongqing, China, 16–18 October 2012. [Google Scholar]
- Ottenbacher, K.J.; Smith, P.M.; Illig, S.B.; Linn, R.T.; Fiedler, R.C.; Granger, C.V. Comparison of logistic regression and neural networks to predict rehospitalization in patients with stroke. J. Clin. Epidemiol. 2001, 54, 1159–1165. [Google Scholar] [CrossRef]
- Yeh, J.-R.; Fan, S.-Z.; Shieh, J.-S. Human heart beat analysis using a modified algorithm of detrended fluctuation analysis based on empirical mode decomposition. Med. Eng. Phys. 2009, 31, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.; Shpanskaya, K.; et al. CheXNet: Radiologist-Level Pneumonia Detection on Chest X-Rays with Deep Learning. arXiv 2017, arXiv:1711.05225v1. [Google Scholar]
- De Fauw, J.; Ledsam, J.R.; Romera-Paredes, B.; Nikolov, S.; Tomasev, N.; Blackwell, S.; Askham, H.; Glorot, X.; O’Donoghue, B.; Visentin, D.; et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat. Med. 2018, 24, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q. Flexible gas sensor based on graphene/ethyl cellulose nanocomposite with ultra-low strain response for volatile organic compounds rapid detection. Nanotechnology 2018, 29, 285501. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y. 3D Architectured Graphene/Metal Oxide Hybrids for Gas Sensors: A Review. Sensors 2018, 18, 1456. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Common Disease | Indicator Gases |
|---|---|
| Renal disease | Ammonia, Mono-methylamine, Dimethylamine, Trimethylamine |
| Skin Disease | Melanoma biomarkers, Fatty acids |
| Diabetes | Glyceria, Acetone |
| Lung Cancer | Styrene, Decane, Isoprene, Benzene, Undecane, 1-hexene, Hexanal, Propyl |
| Asthma | Nitric Oxide (NO) |
| No. | Sex | Age | WBC | PLT | Seg | CRP | Sputum | No. | Sex | Age | WBC | PLT | Seg | CRP | Sputum |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | male | 87 | 7.38 | 120 | 61.4 | 2.07 | Pseudomonas aeruginosa | 1 | male | 87 | 5.27 | 146 | 58 | N/A | X |
| 2 | male | 90 | 10.23 | 363 | 70.8 | N/A | Pseudomonas aeruginosa | 2 | male | 83 | 6.18 | 11 | 86.1 | N/A | X |
| 3 | female | 80 | 13.73 | 258 | 83.1 | 7.09 | Pseudomonas aeruginosa | 3 | male | 44 | 20.95 | 194 | 90.4 | N/A | X |
| 4 | male | 63 | 12.05 | 39 | 91.1 | 21.93 | Pseudomonas aeruginosa | 4 | female | 51 | 16.25 | 352 | 89.2 | 3.52 | X |
| 5 | male | 80 | 31.8 | 286 | 93.5 | 29.12 | Pseudomonas aeruginosa | 5 | female | 68 | 9.7 | 191 | 83.9 | 13.05 | X |
| 6 | male | 54 | 3.25 | 75 | 93 | 11.43 | Pseudomonas aeruginosa | 6 | male | 51 | 6.75 | 178 | 77.3 | N/A | X |
| 7 | male | 59 | 10.62 | 342 | 75.2 | 5.99 | Pseudomonas aeruginosa | 7 | female | 53 | 20.56 | 204 | 93.6 | 0.64 | X |
| 8 | male | 57 | 9.11 | 154 | 82.8 | N/A | Pseudomonas aeruginosa | 8 | male | 49 | 17.59 | 309 | 80.7 | N/A | X |
| 9 | male | 49 | 13.23 | 170 | 82.8 | N/A | Pseudomonas aeruginosa | 9 | male | 49 | 13.15 | 438 | 80.5 | N/A | X |
| 10 | male | 83 | 12.58 | 142 | 88.7 | 8.61 | Pseudomonas aeruginosa | 10 | male | 84 | 25.82 | 274 | 85.5 | 7.86 | X |
| 11 | male | 79 | 8.98 | 301 | 73.4 | N/A | Pseudomonas aeruginosa | 11 | female | 70 | 6.86 | 306 | 40.2 | N/A | X |
| 12 | female | 61 | 10.8 | 174 | 83.6 | 12.47 | Pseudomonas aeruginosa | 12 | female | 78 | 23.31 | 206 | 89.6 | N/A | X |
| Dataset | Model Type | AUC | ACC | SEN | PPV |
|---|---|---|---|---|---|
| At Best Threshold | |||||
| 1 | ENN Model | 0.9815 | 0.9304 | 0.9929 | 0.8825 |
| 2 | ENN Model | 0.9801 | 0.9518 | 0.9571 | 0.9470 |
| 3 | ENN Model | 0.9925 | 0.9375 | 0.9679 | 0.9125 |
| 4 | ENN Model | 0.9790 | 0.9625 | 0.9714 | 0.9544 |
| 5 | ENN Model | 0.9879 | 0.9571 | 0.9679 | 0.9476 |
| Average | ENN Model | 0.9842 ± 0.0058 | 0.9479 ± 0.0135 | 0.9714 ± 0.0131 | 0.9288 ± 0.0306 |
| 0.500 | 0.500 | 0.500 | 0.500 | 0.671 | 0.288 | 0.361 | 0.500 | 0.584 | 0.500 | 0.486 | ||
| 0.500 | 0.500 | 0.500 | 0.500 | 0.716 | 0.280 | 0.396 | 0.500 | 0.500 | 0.500 | 0.443 | ||
| 0.500 | 0.500 | 0.500 | 0.500 | 0.254 | 0.282 | 0.500 | 0.500 | 0.500 | 0.661 | 0.500 | ||
| 0.500 | 0.500 | 0.500 | 0.500 | 0.286 | 0.305 | 0.352 | 0.513 | 0.682 | 0.679 | 0.548 | ||
| 0.500 | 0.500 | 0.500 | 0.500 | 0.346 | 0.500 | 0.363 | 0.671 | 0.500 | 0.500 | 0.679 | ||
| 0.500 | 0.500 | 0.500 | 0.500 | 0.318 | 0.461 | 0.500 | 0.500 | 0.500 | 0.711 | 0.500 | ||
| 0.500 | 0.500 | 0.500 | 0.500 | 0.305 | 0.500 | 0.500 | 0.500 | 0.500 | 0.500 | 0.500 | ||
| 0.500 | 0.500 | 0.500 | 0.500 | 0.695 | 0.471 | 0.500 | 0.500 | 0.846 | 0.500 | 0.707 | ||
| 0.500 | 0.500 | 0.500 | 0.500 | 0.695 | 0.500 | 0.500 | 0.575 | 0.500 | 0.500 | 0.730 | ||
| 0.500 | 0.500 | 0.500 | 0.500 | 0.695 | 0.500 | 0.500 | 0.546 | 0.755 | 0.500 | 0.786 | ||
| 0.500 | 0.500 | 0.500 | 0.500 | 0.695 | 0.500 | 0.500 | 0.500 | 0.743 | 0.500 | 0.8250 | ||
| Dataset | Model Type | AUC | ACC | SEN | PPV |
|---|---|---|---|---|---|
| At Best Parameters | |||||
| 1 | SVM Model | 0.9524 | 0.8786 | 0.8786 | 0.8786 |
| 2 | SVM Model | 0.9618 | 0.8946 | 0.8821 | 0.9048 |
| 3 | SVM Model | 0.8878 | 0.8786 | 0.9393 | 0.8376 |
| 4 | SVM Model | 0.9521 | 0.8964 | 0.9714 | 0.8447 |
| 5 | SVM Model | 0.9508 | 0.7946 | 0.9536 | 0.8536 |
| Average | SVM Model | 0.9410 ± 0.0301 | 0.8686 ± 0.0422 | 0.9250 ± 0.0423 | 0.8639 ± 0.0276 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, Y.-H.; Wang, Z.-C.; Zhang, F.-G.; Abbod, M.F.; Shih, C.-H.; Shieh, J.-S. Machine Learning Methods Applied to Predict Ventilator-Associated Pneumonia with Pseudomonas aeruginosa Infection via Sensor Array of Electronic Nose in Intensive Care Unit. Sensors 2019, 19, 1866. https://0-doi-org.brum.beds.ac.uk/10.3390/s19081866
Liao Y-H, Wang Z-C, Zhang F-G, Abbod MF, Shih C-H, Shieh J-S. Machine Learning Methods Applied to Predict Ventilator-Associated Pneumonia with Pseudomonas aeruginosa Infection via Sensor Array of Electronic Nose in Intensive Care Unit. Sensors. 2019; 19(8):1866. https://0-doi-org.brum.beds.ac.uk/10.3390/s19081866
Chicago/Turabian StyleLiao, Yu-Hsuan, Zhong-Chuang Wang, Fu-Gui Zhang, Maysam F. Abbod, Chung-Hung Shih, and Jiann-Shing Shieh. 2019. "Machine Learning Methods Applied to Predict Ventilator-Associated Pneumonia with Pseudomonas aeruginosa Infection via Sensor Array of Electronic Nose in Intensive Care Unit" Sensors 19, no. 8: 1866. https://0-doi-org.brum.beds.ac.uk/10.3390/s19081866