Author Contributions
Conceptualization, R.B.M., J.G.M., L.L.S., D.W., and A.V.H.; data curation, R.B.M. and B.P.T.; formal analysis, R.B.M., B.P.T., C.D., D.W. and A.V.H.; funding acquisition, L.L.S., D.W. and A.V.H.; investigation, R.B.M., B.P.T., C.D., J.G.M., L.L.S., D.W. and A.V.H.; methodology, R.B.M., B.P.T., C.D., L.L.S., D.W., and A.V.H.; project administration, L.L.S., D.W. and A.V.H.; resources, L.L.S., D.W. and A.V.H.; software, R.B.M. and B.P.T.; supervision, C.D., J.G.M., L.L.S., D.W. and A.V.H.; validation, R.B.M. and A.V.H.; visualization, R.B.M., B.P.T. and A.V.H.; writing—original draft, R.B.M.; writing—review and editing, R.B.M., C.D., J.G.M., L.L.S., D.W. and A.V.H. All authors have read and agreed to the published version of the manuscript.
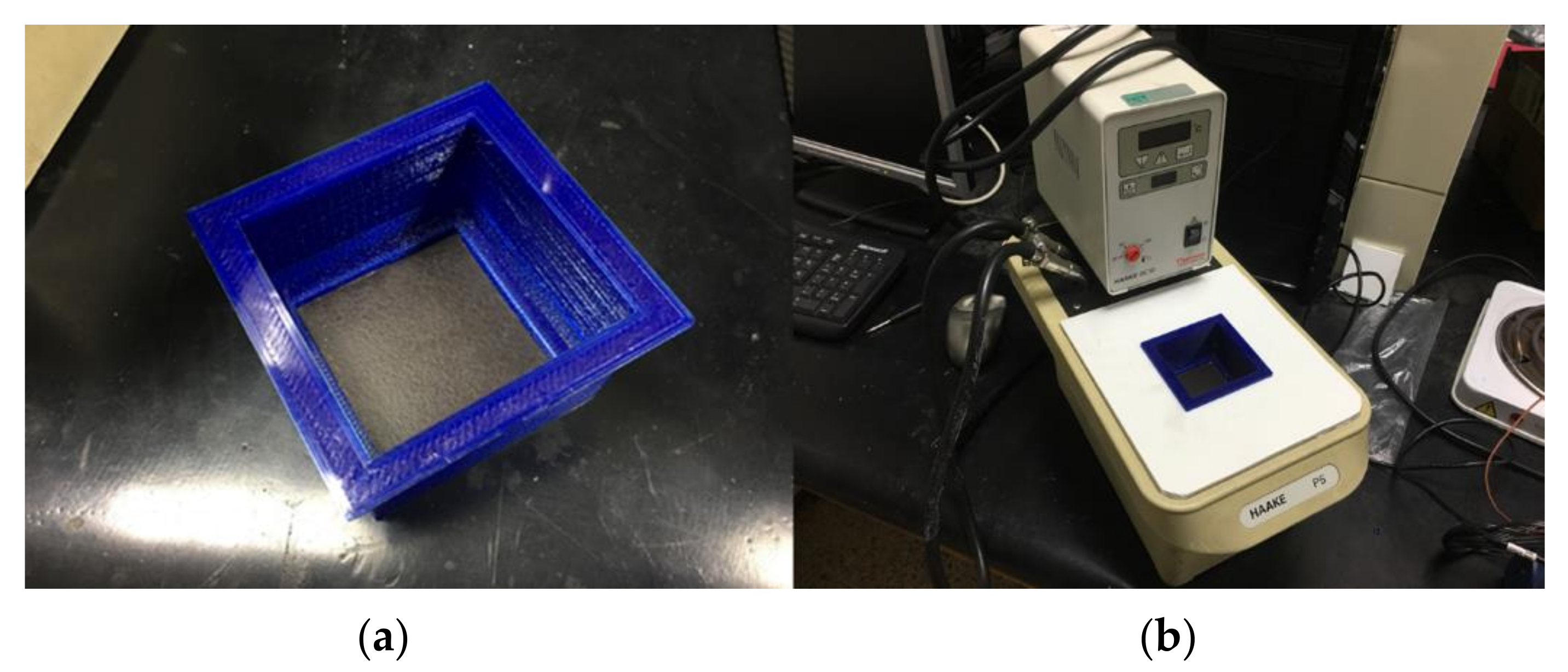
Figure 1.
Temperature calibration material. (a) Blackbody placed inside a sealed container to isolate the upper surface from the water. (b) Thermally controlled water bath with the blackbody placed inside the closed bath container.
Figure 1.
Temperature calibration material. (a) Blackbody placed inside a sealed container to isolate the upper surface from the water. (b) Thermally controlled water bath with the blackbody placed inside the closed bath container.
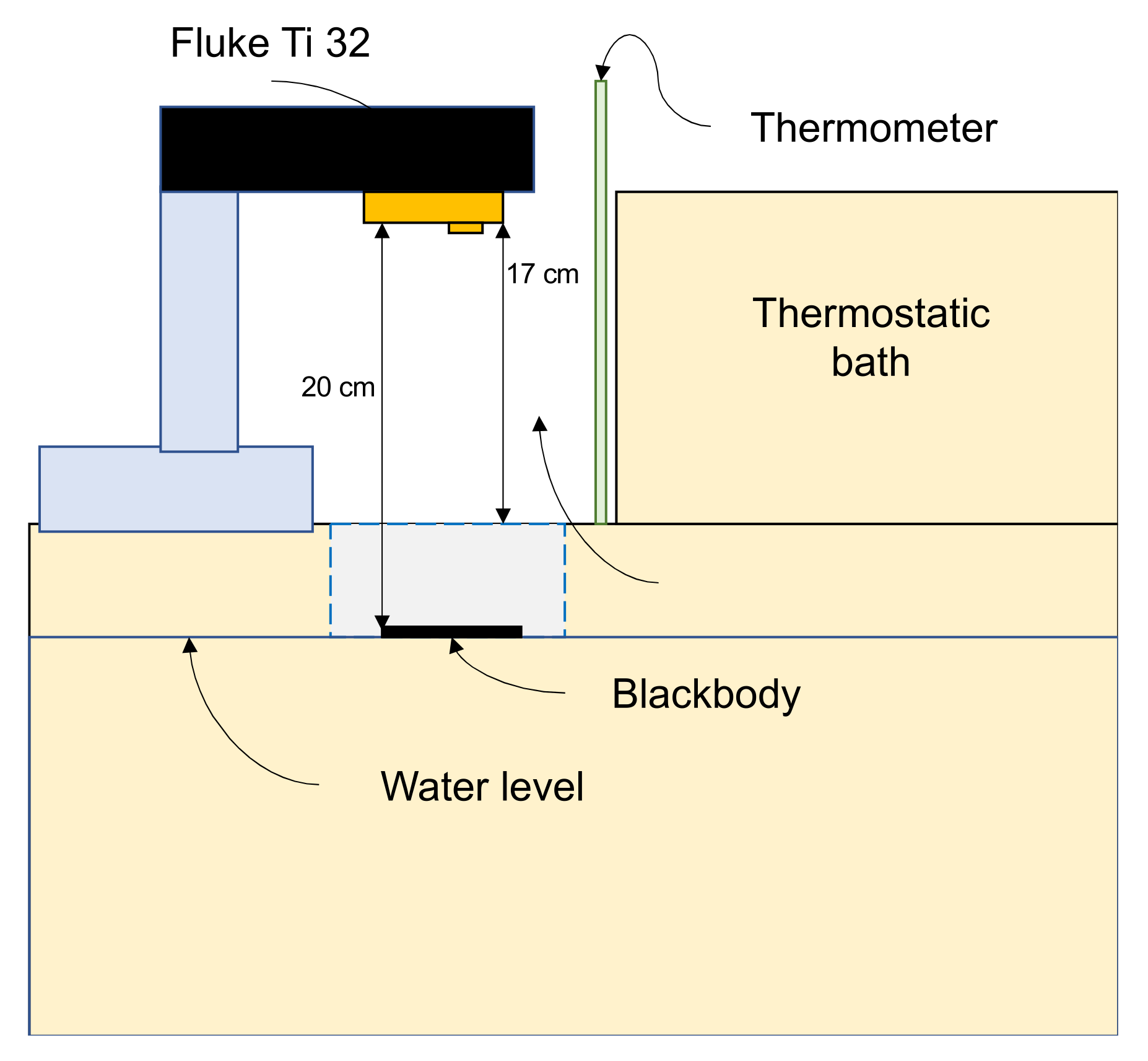
Figure 2.
Thermal calibration system.
Figure 2.
Thermal calibration system.
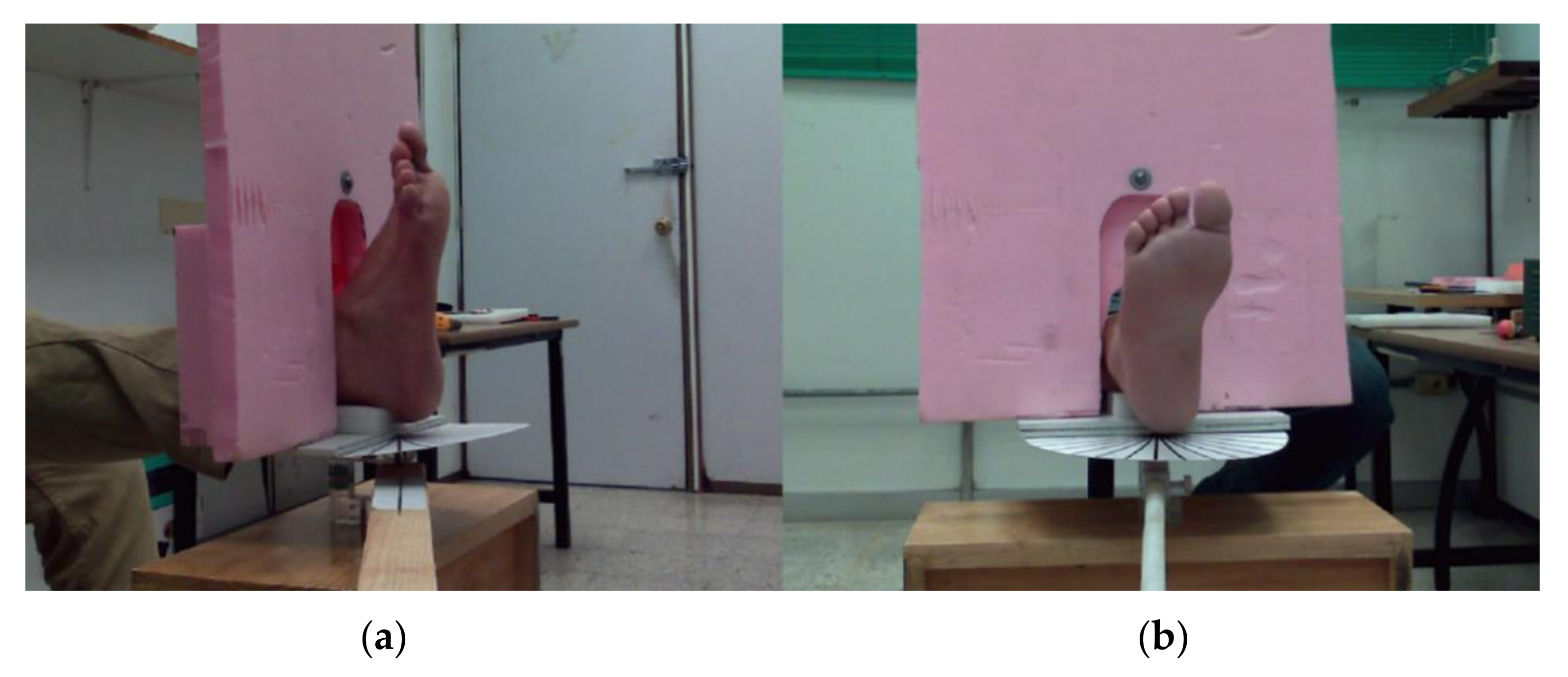
Figure 3.
Foot posture during the image acquisition. (a) Lateral view of the foot on the resting base with angle and the thermal insulating foam background. (b) Frontal view. It is noteworthy that the pink background foam is large enough to isolate the foot from the remaining body of the volunteer so that the IR radiation does not interfere with the captured frame.
Figure 3.
Foot posture during the image acquisition. (a) Lateral view of the foot on the resting base with angle and the thermal insulating foam background. (b) Frontal view. It is noteworthy that the pink background foam is large enough to isolate the foot from the remaining body of the volunteer so that the IR radiation does not interfere with the captured frame.
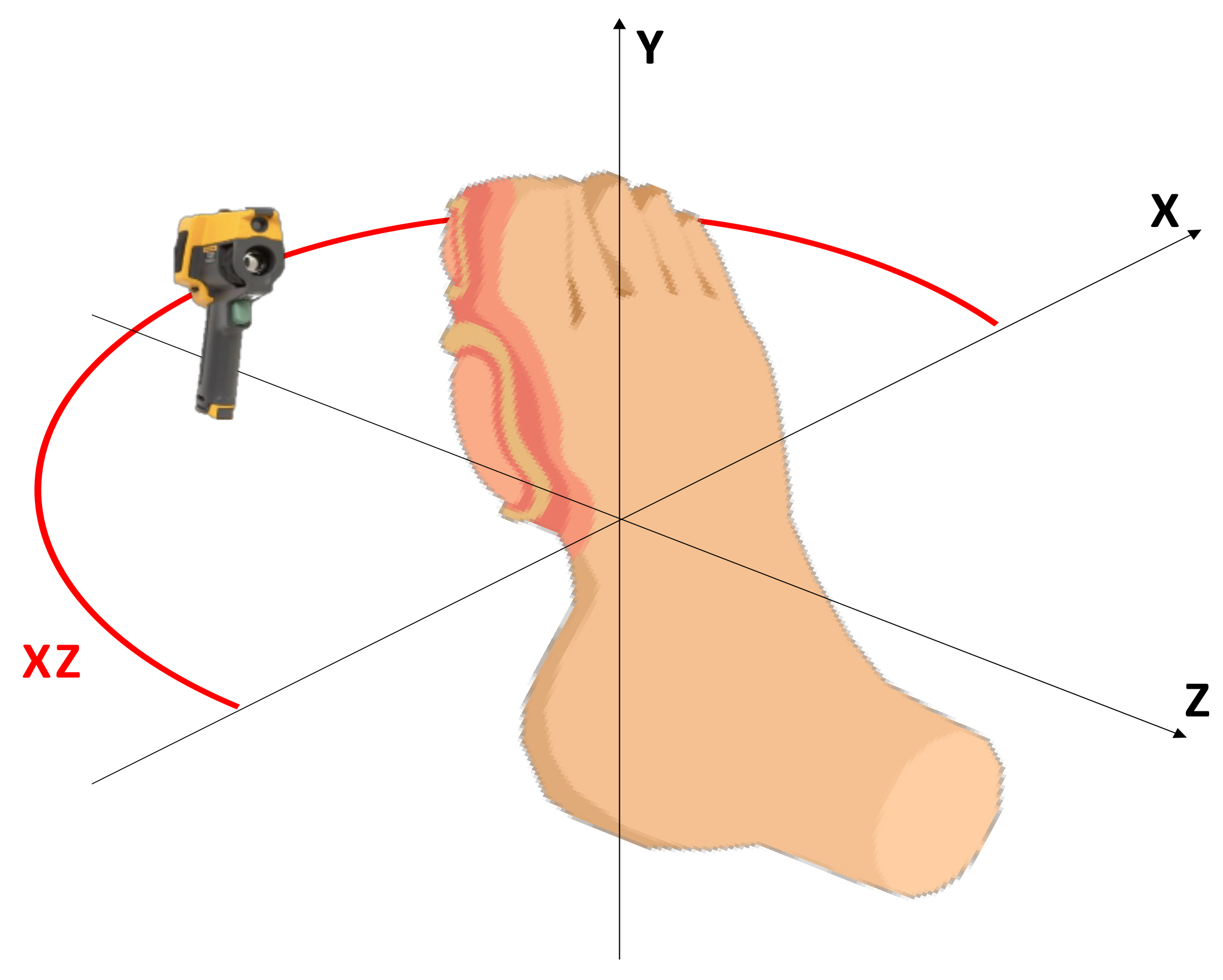
Figure 4.
The sequence trajectory in the XZ plane is represented by the red arc. The camera was placed in a vertical position regarding the foot.
Figure 4.
The sequence trajectory in the XZ plane is represented by the red arc. The camera was placed in a vertical position regarding the foot.
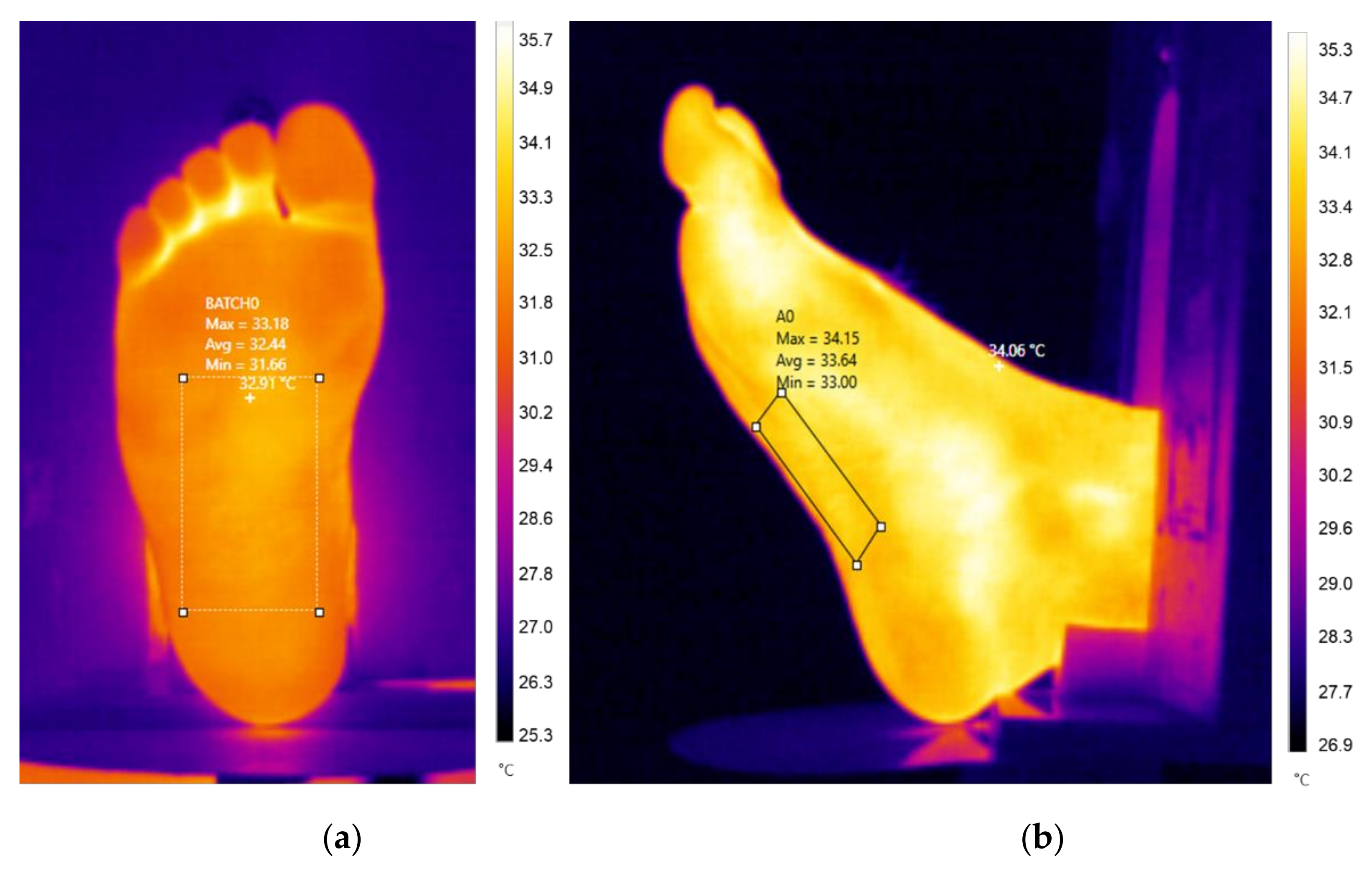
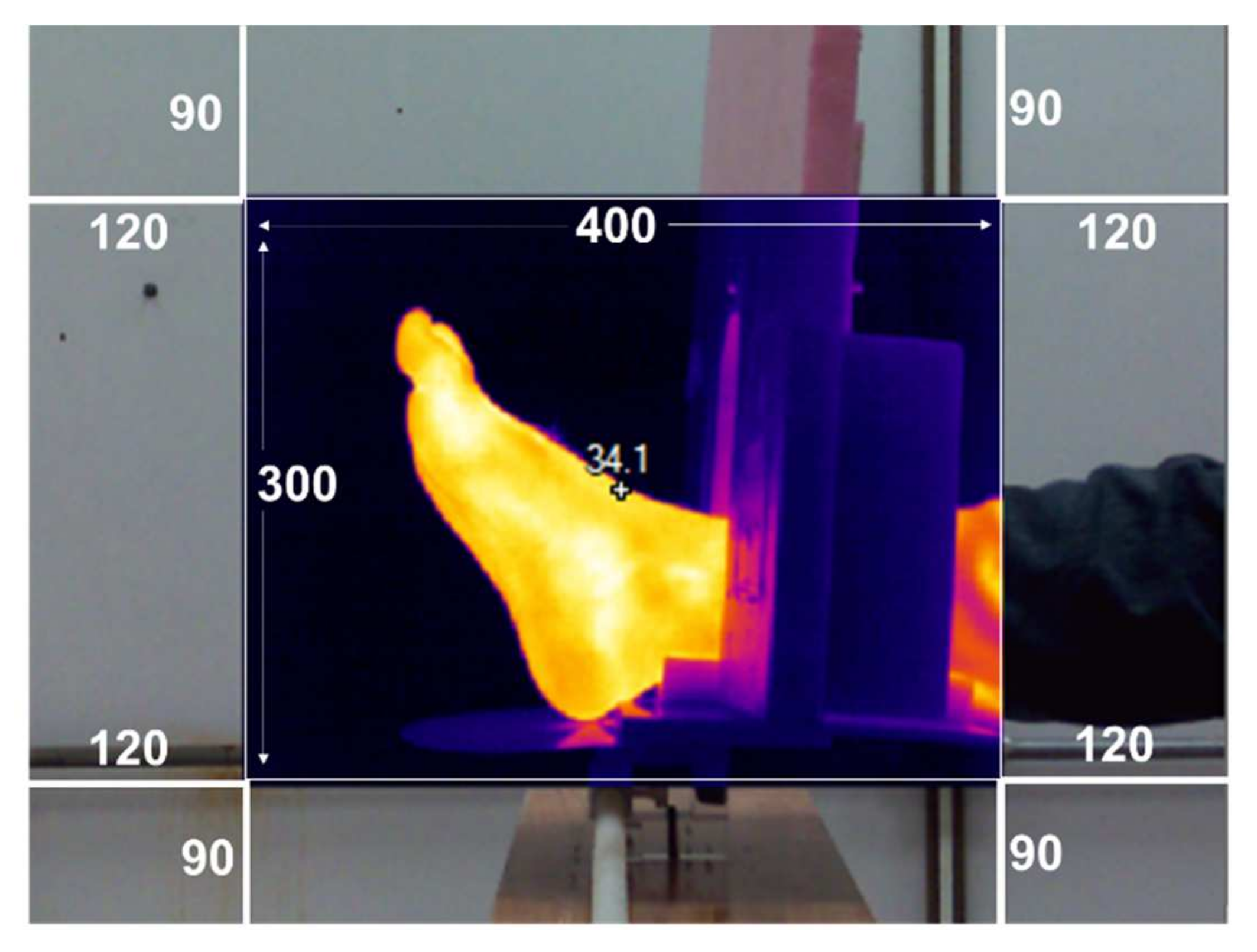
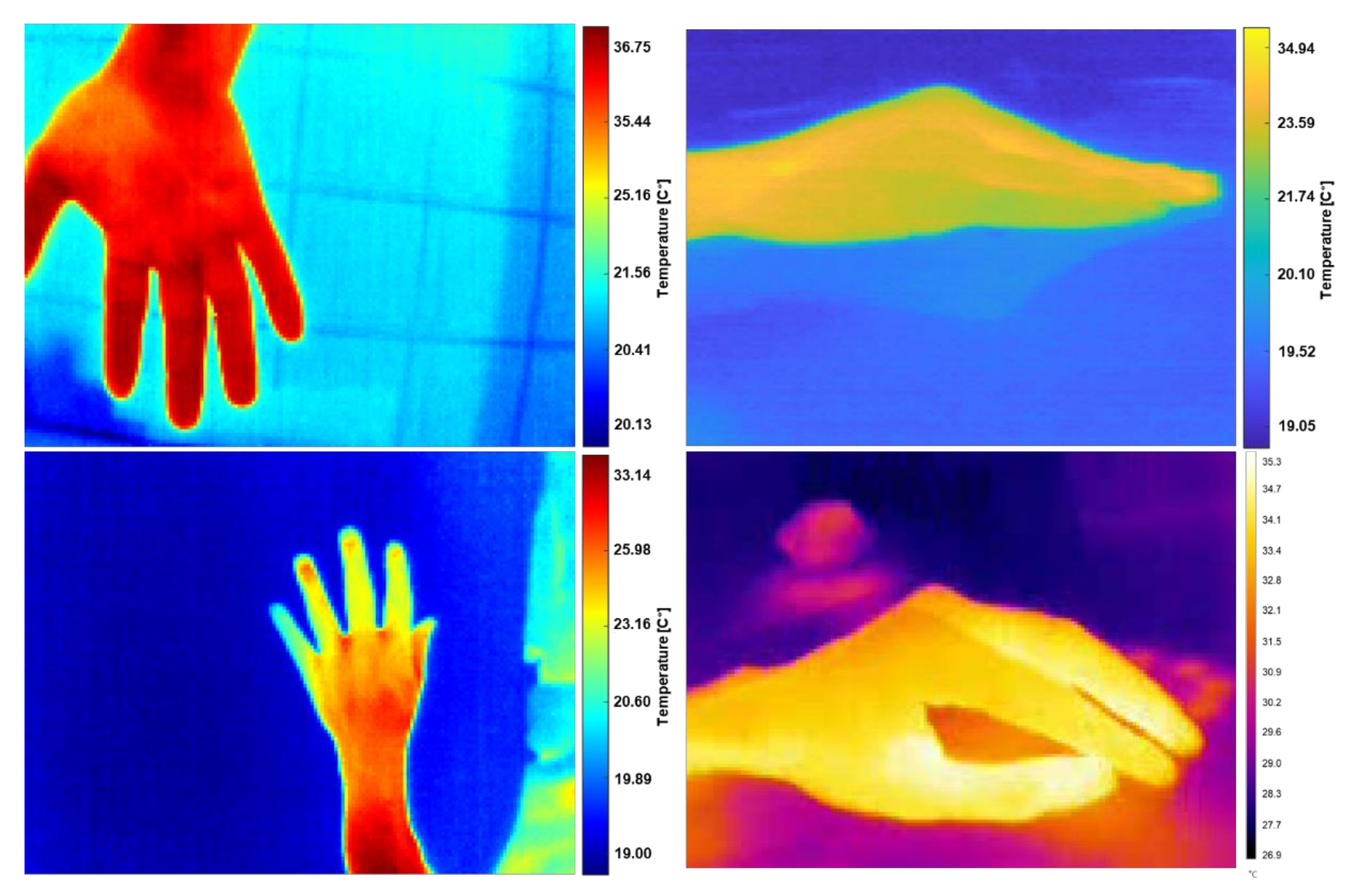
Figure 5.
Thermal images taken from different viewpoints. (a) Reference sample at a normal angle. (b) The last sample at a 90° angle change position. For each sample, the average temperature was retrieved within a marker box.
Figure 5.
Thermal images taken from different viewpoints. (a) Reference sample at a normal angle. (b) The last sample at a 90° angle change position. For each sample, the average temperature was retrieved within a marker box.
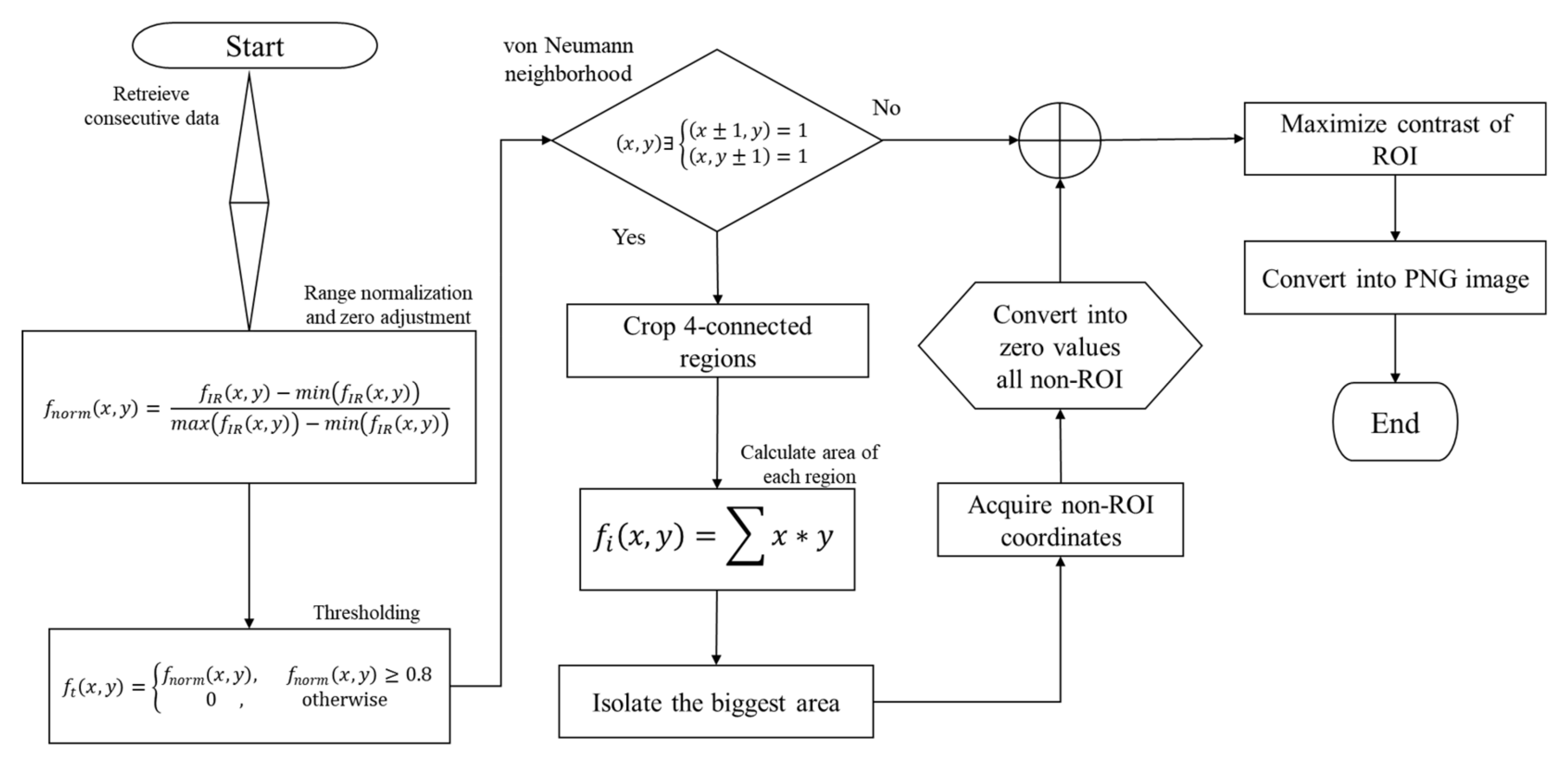
Figure 6.
Flowchart of the radiometric data processing to obtain a segmented IR image, without interferences or non-desirable artifacts.
Figure 6.
Flowchart of the radiometric data processing to obtain a segmented IR image, without interferences or non-desirable artifacts.
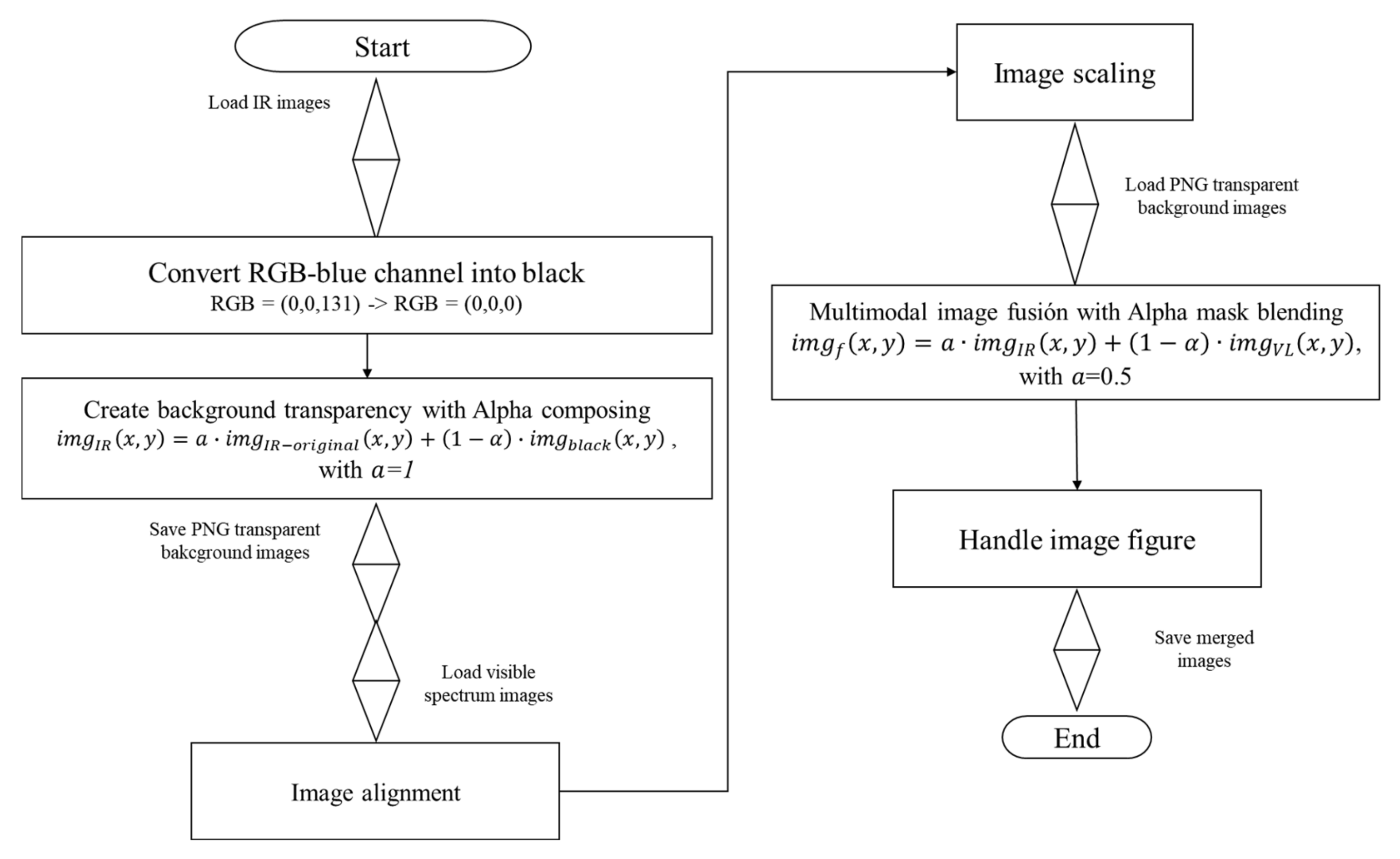
Figure 7.
Flowchart of the multimodal co-registration. For each IR image, the blue background was transformed into black to apply the alpha mask transformation. The visible-light images were co-registered with the IR images by alignment, scaling, and merging.
Figure 7.
Flowchart of the multimodal co-registration. For each IR image, the blue background was transformed into black to apply the alpha mask transformation. The visible-light images were co-registered with the IR images by alignment, scaling, and merging.
Figure 8.
Multimodal superimposed images without RoI segmentation.
Figure 8.
Multimodal superimposed images without RoI segmentation.
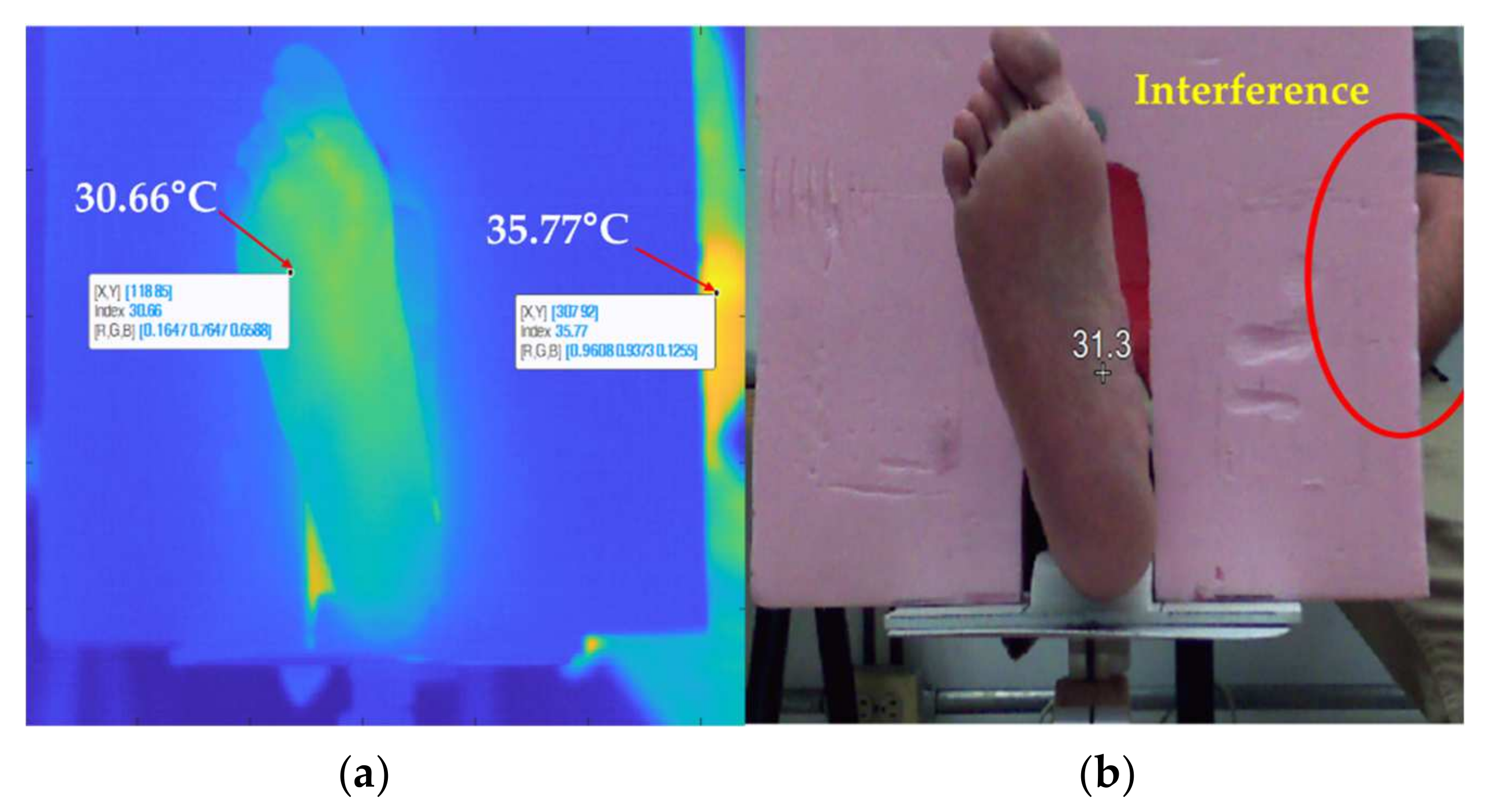
Figure 9.
Color contrast mapping according to the warmest spot. (a) The hottest spot of the picture frame is located on the upper limb, which decreases the color contrast of the foot image. (b) The image was acquired by a wrongly aligned camera since the foam background should completely cover the volunteer’s body.
Figure 9.
Color contrast mapping according to the warmest spot. (a) The hottest spot of the picture frame is located on the upper limb, which decreases the color contrast of the foot image. (b) The image was acquired by a wrongly aligned camera since the foam background should completely cover the volunteer’s body.
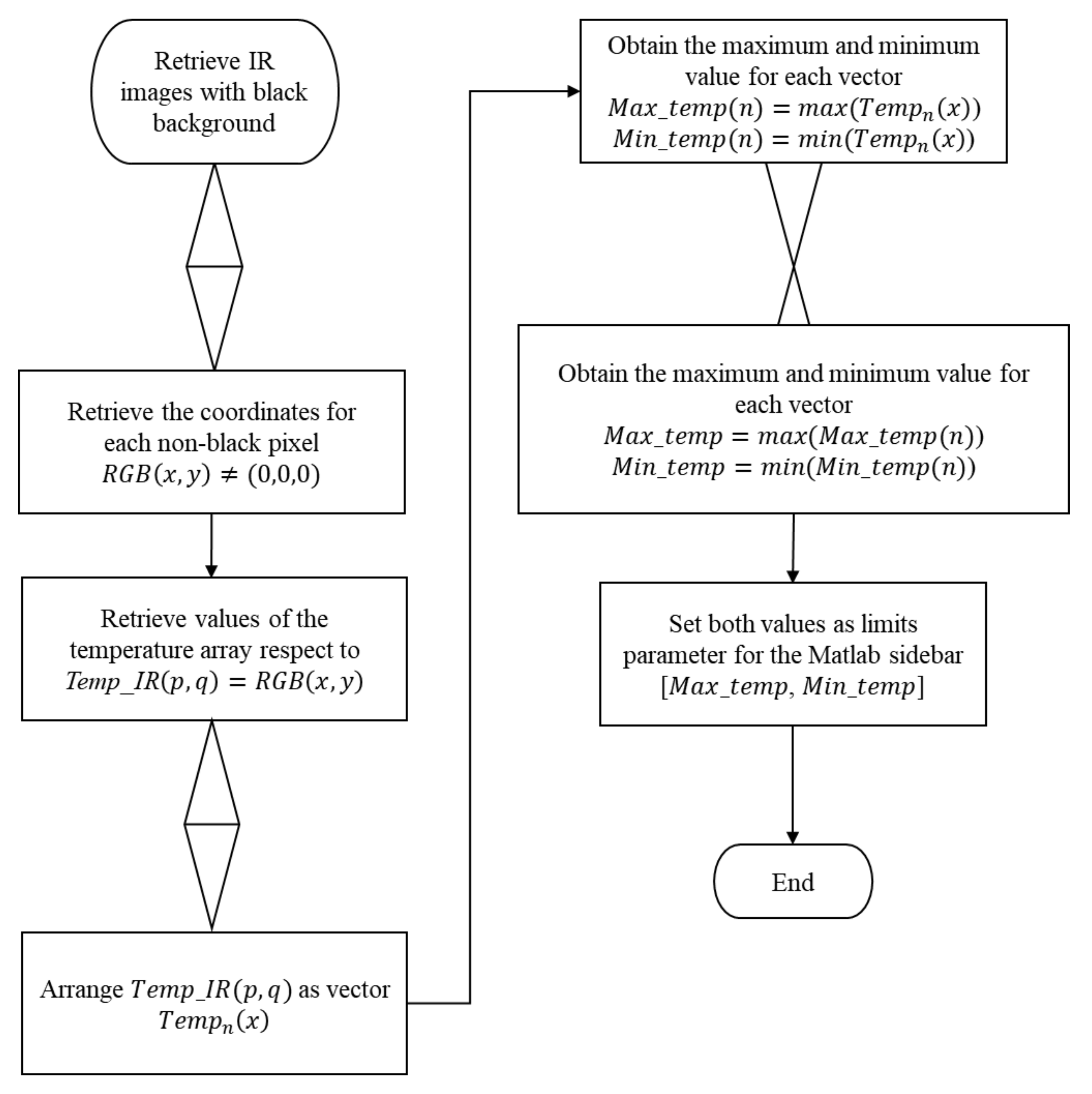
Figure 10.
Flowchart for obtaining the limits of the color bar function for the temperature matrix set.
Figure 10.
Flowchart for obtaining the limits of the color bar function for the temperature matrix set.
Figure 11.
Samples of radiometric information in an uncontrolled environment are represented in false-color images. These samples were used to test the robustness of the automatic segmentation method.
Figure 11.
Samples of radiometric information in an uncontrolled environment are represented in false-color images. These samples were used to test the robustness of the automatic segmentation method.
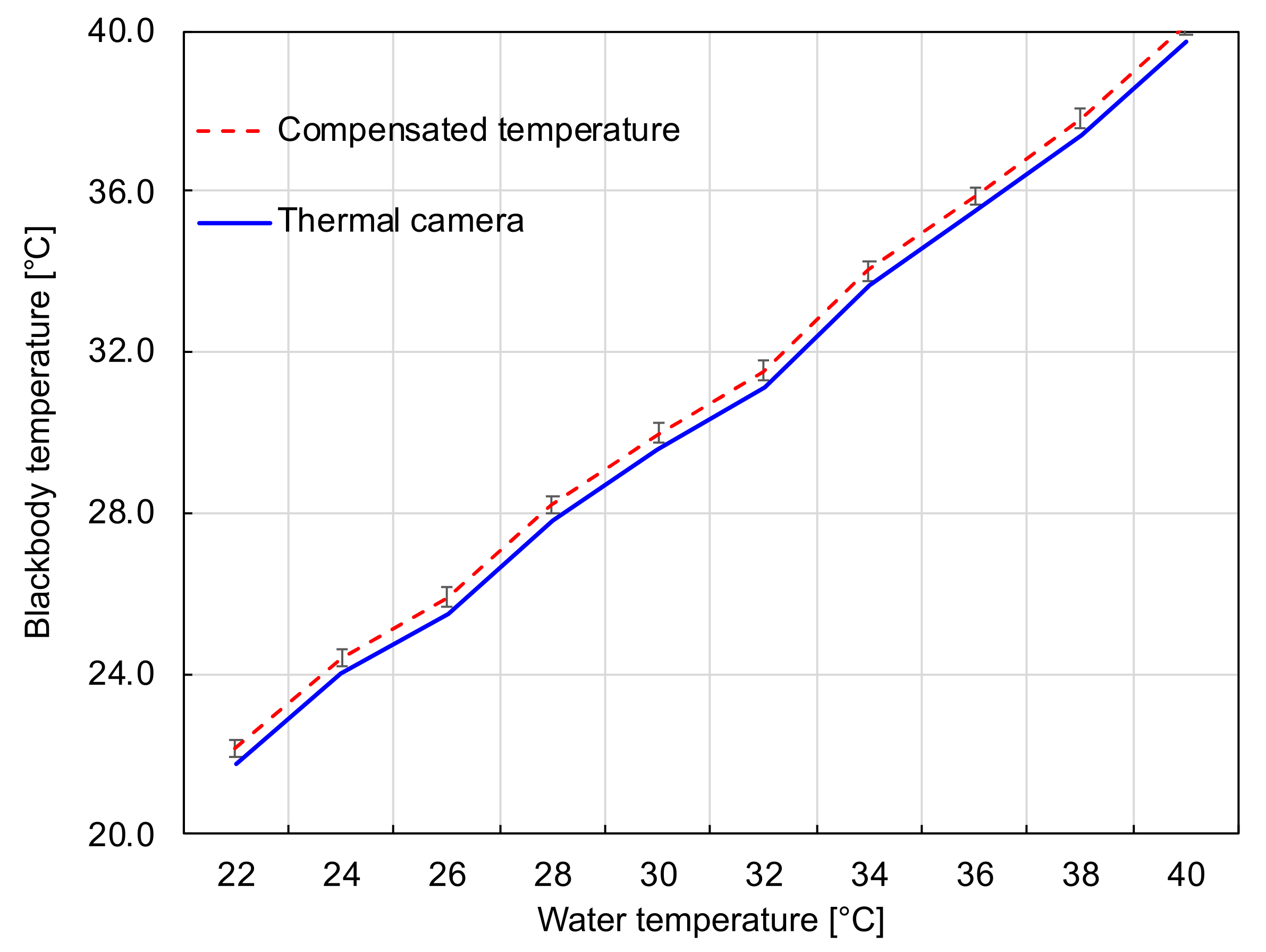
Figure 12.
Temperature differences between the measurements of the thermal camera and the standard thermometer. The red dashed line represents the ground truth values and the blue solid curve corresponds to the values measured by the calibrated camera.
Figure 12.
Temperature differences between the measurements of the thermal camera and the standard thermometer. The red dashed line represents the ground truth values and the blue solid curve corresponds to the values measured by the calibrated camera.
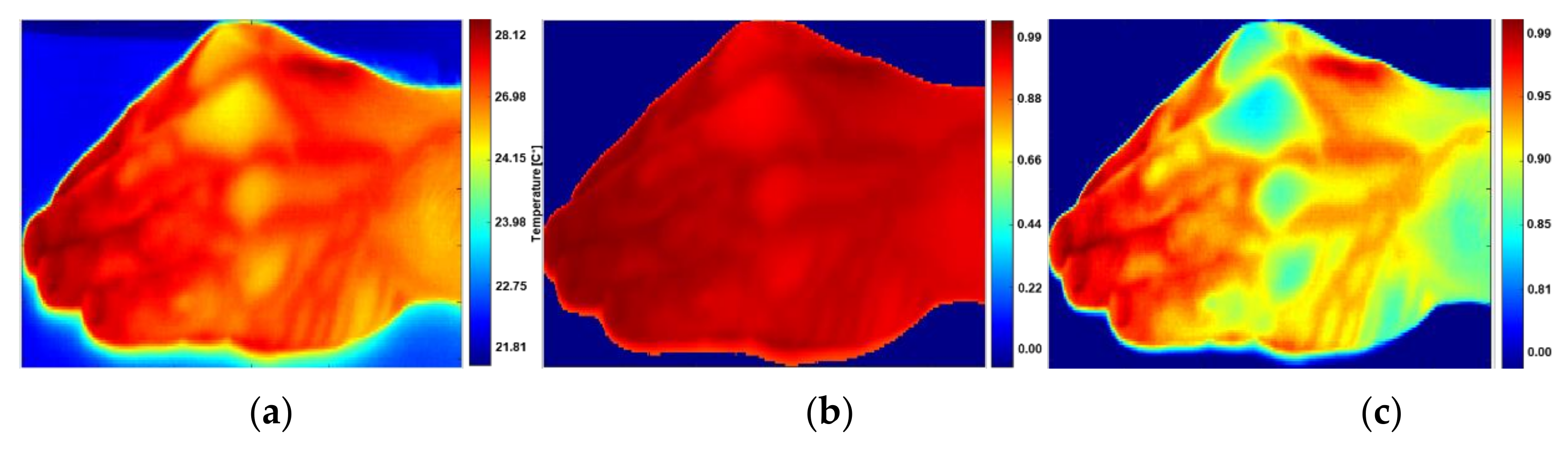
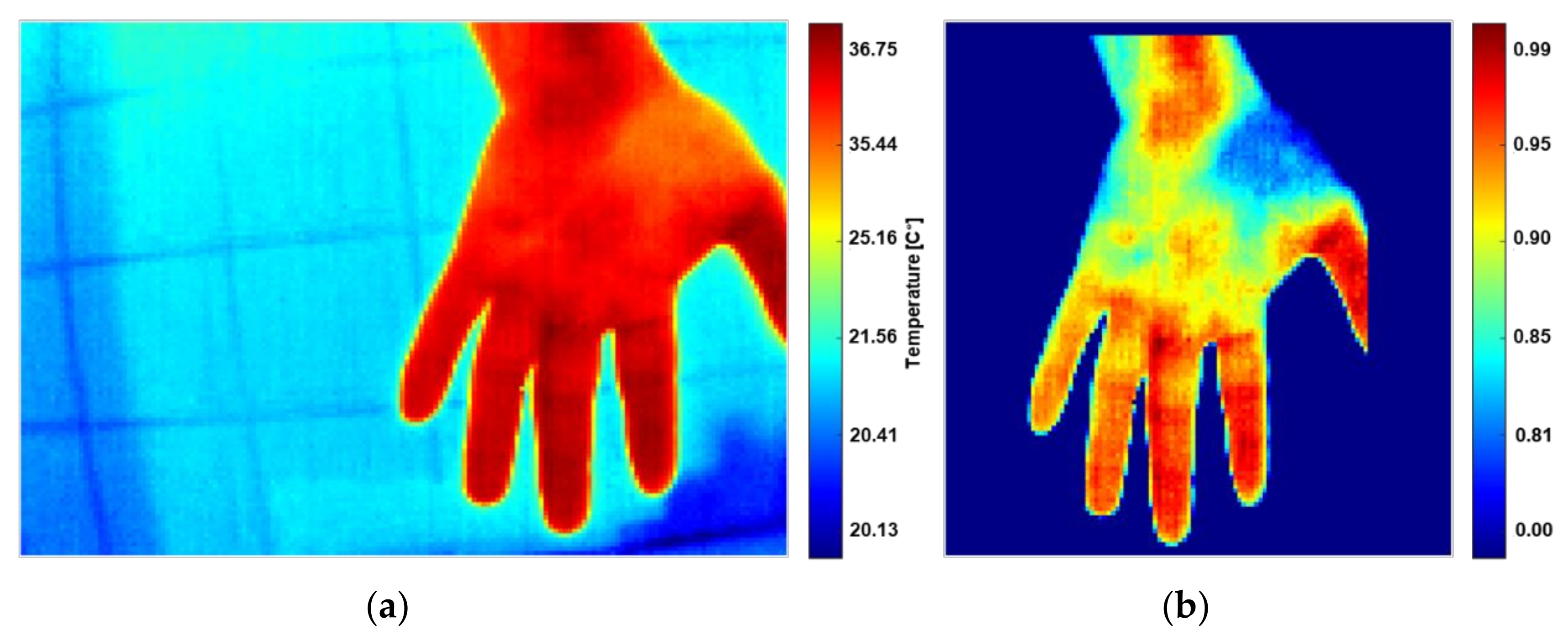
Figure 13.
Normalization and segmentation obtained in
Section 2.4. (
a) False-color image with thermal interferences, (
b) IR image after thresholding step at 0.8. The thresholding leads to a homogeneous image background. (
c) Segmentation results with color contrast on the RoI, in which the false colors represent the temperature intensities.
Figure 13.
Normalization and segmentation obtained in
Section 2.4. (
a) False-color image with thermal interferences, (
b) IR image after thresholding step at 0.8. The thresholding leads to a homogeneous image background. (
c) Segmentation results with color contrast on the RoI, in which the false colors represent the temperature intensities.
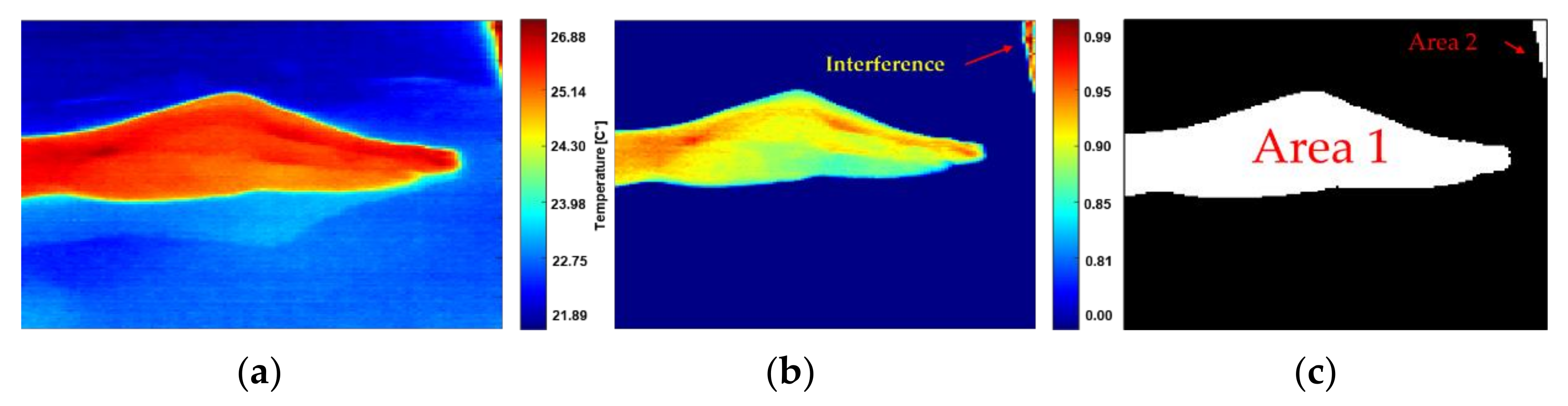
Figure 14.
Illustration of the inference treatment. (a) Raw IR image with thermal interferences and reflection, (b) normalized radiometric data with interference on the corner, (c) area 1 and 2, correspond to warm and large areas with ∆T < 2.6%, but only the area 1 should be labeled as RoI.
Figure 14.
Illustration of the inference treatment. (a) Raw IR image with thermal interferences and reflection, (b) normalized radiometric data with interference on the corner, (c) area 1 and 2, correspond to warm and large areas with ∆T < 2.6%, but only the area 1 should be labeled as RoI.
Figure 15.
(a) Raw IR image, (b) segmentation of the RoI, and removal of artifacts.
Figure 15.
(a) Raw IR image, (b) segmentation of the RoI, and removal of artifacts.
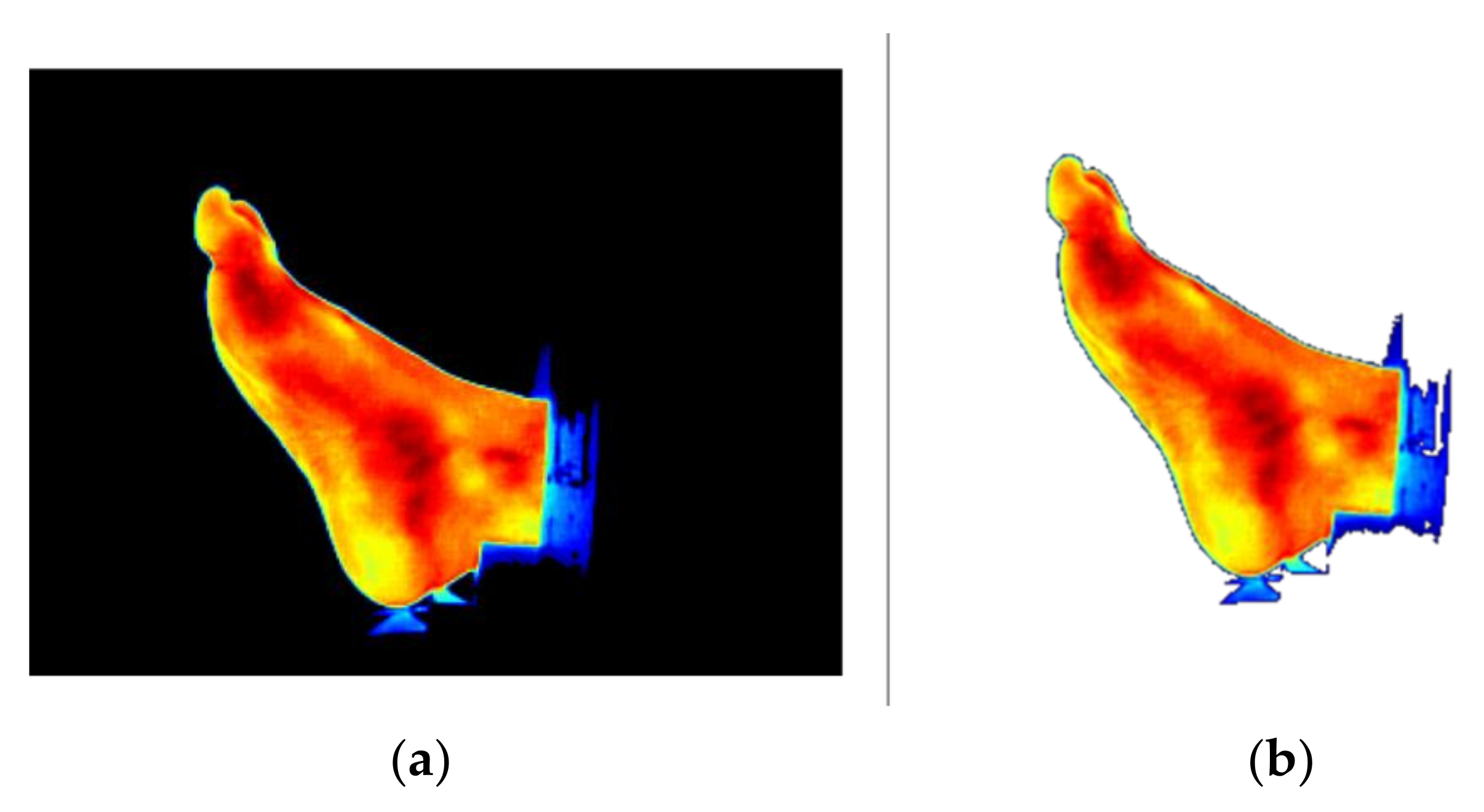
Figure 16.
Illustration of the transparency process. (a) IR image with a black background and (b) IR image with a transparent background.
Figure 16.
Illustration of the transparency process. (a) IR image with a black background and (b) IR image with a transparent background.
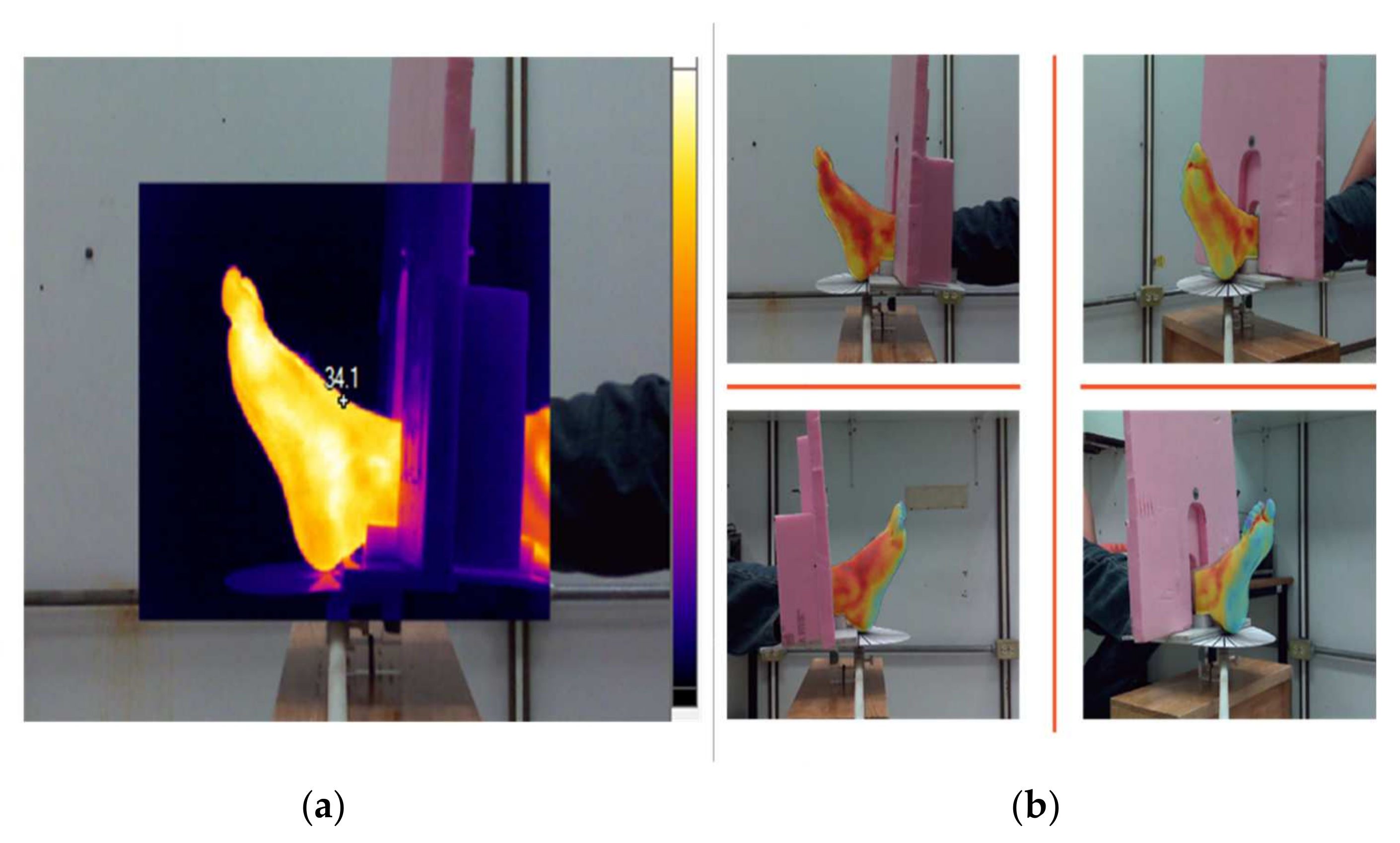
Figure 17.
Multimodal image representation: (a) SmartView Picture-In-Picture image in which the IR is superimposed on the center of the visible-light image. (b) Results of the merged stage, provided by an IR image with a transparent background and the visible-light image as the scene.
Figure 17.
Multimodal image representation: (a) SmartView Picture-In-Picture image in which the IR is superimposed on the center of the visible-light image. (b) Results of the merged stage, provided by an IR image with a transparent background and the visible-light image as the scene.
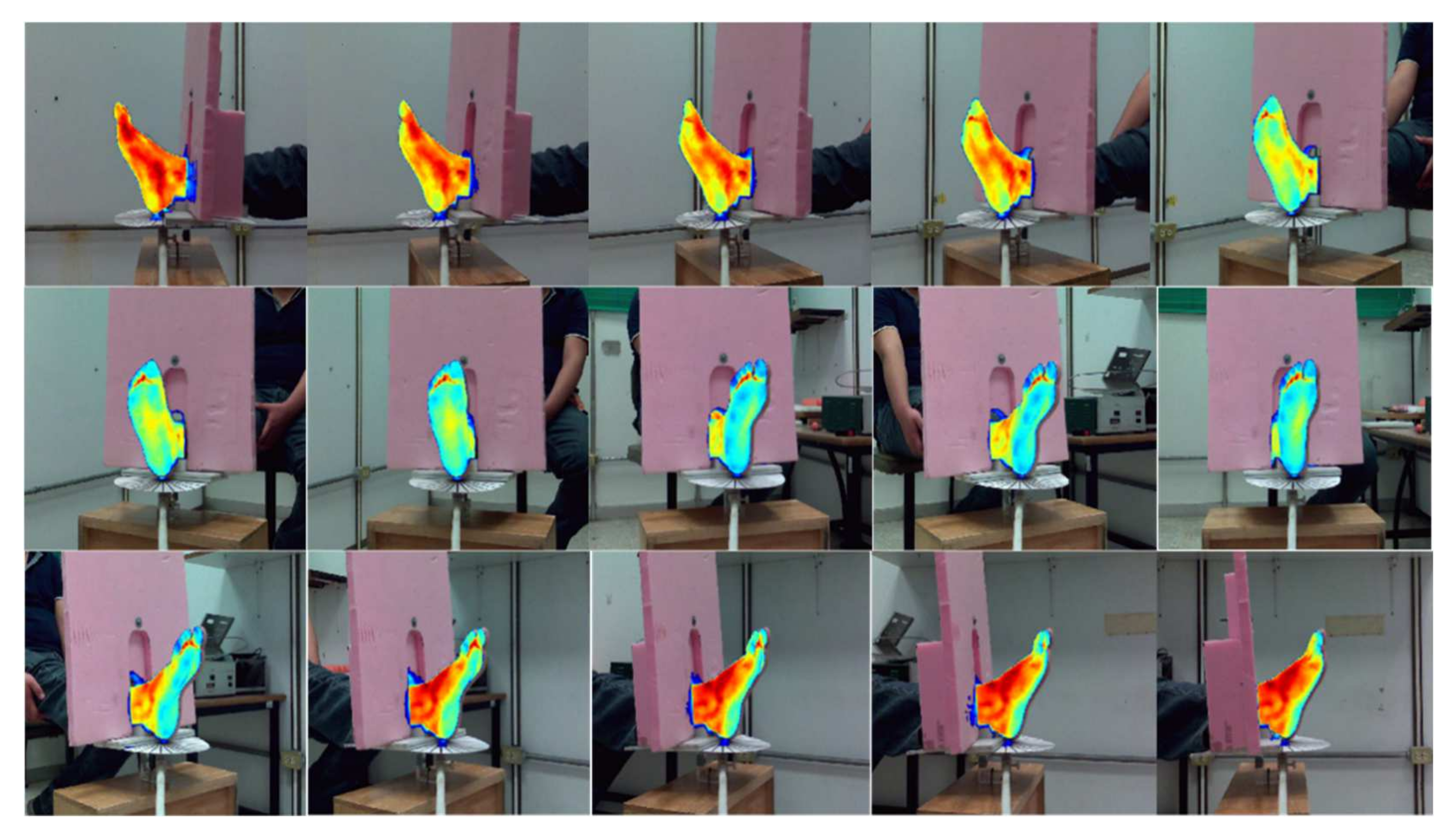
Figure 18.
Set of 15 merged image pairs used for determining the 3D point cloud.
Figure 18.
Set of 15 merged image pairs used for determining the 3D point cloud.
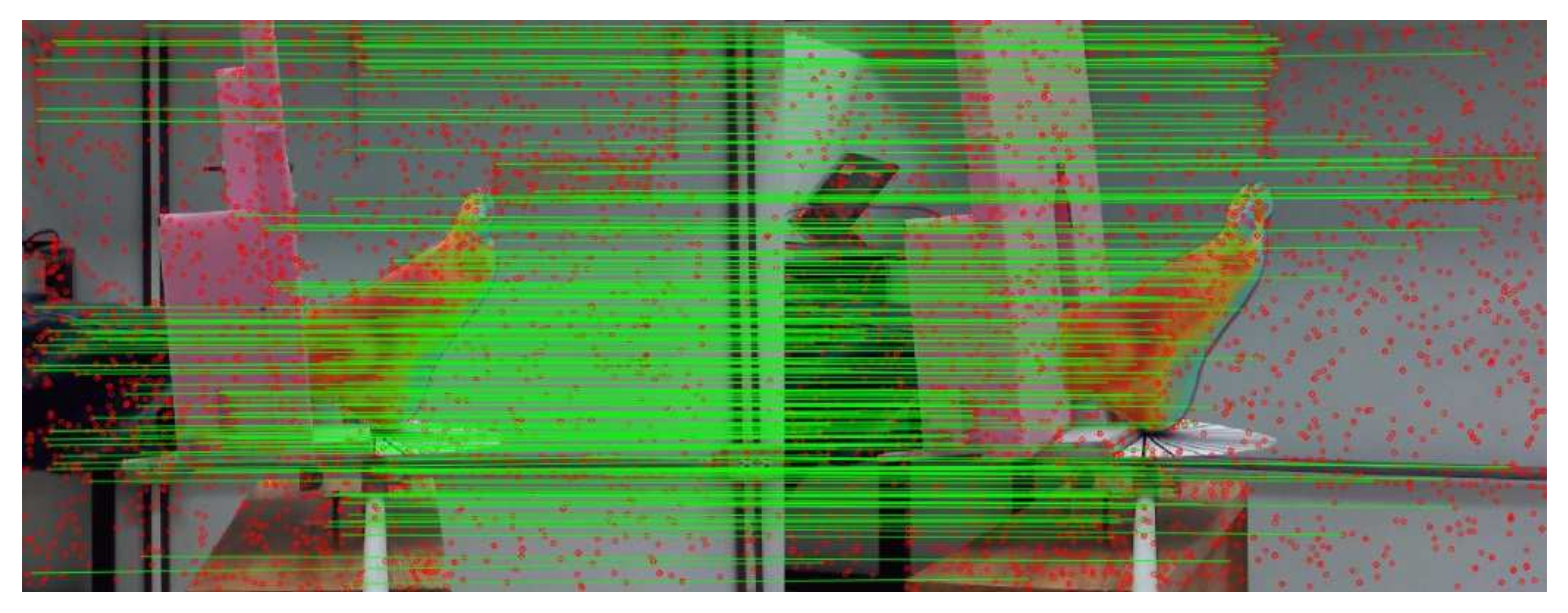
Figure 19.
Detected feature points (red dots) and visualization of their correspondence (the green lines represent the link between homologous points). This figure represents 202 matches between images 6 and 7 from set S1, in which most of the key points were dismissed, proving that the quality of the model depends on the accuracy of the matching points’ process.
Figure 19.
Detected feature points (red dots) and visualization of their correspondence (the green lines represent the link between homologous points). This figure represents 202 matches between images 6 and 7 from set S1, in which most of the key points were dismissed, proving that the quality of the model depends on the accuracy of the matching points’ process.
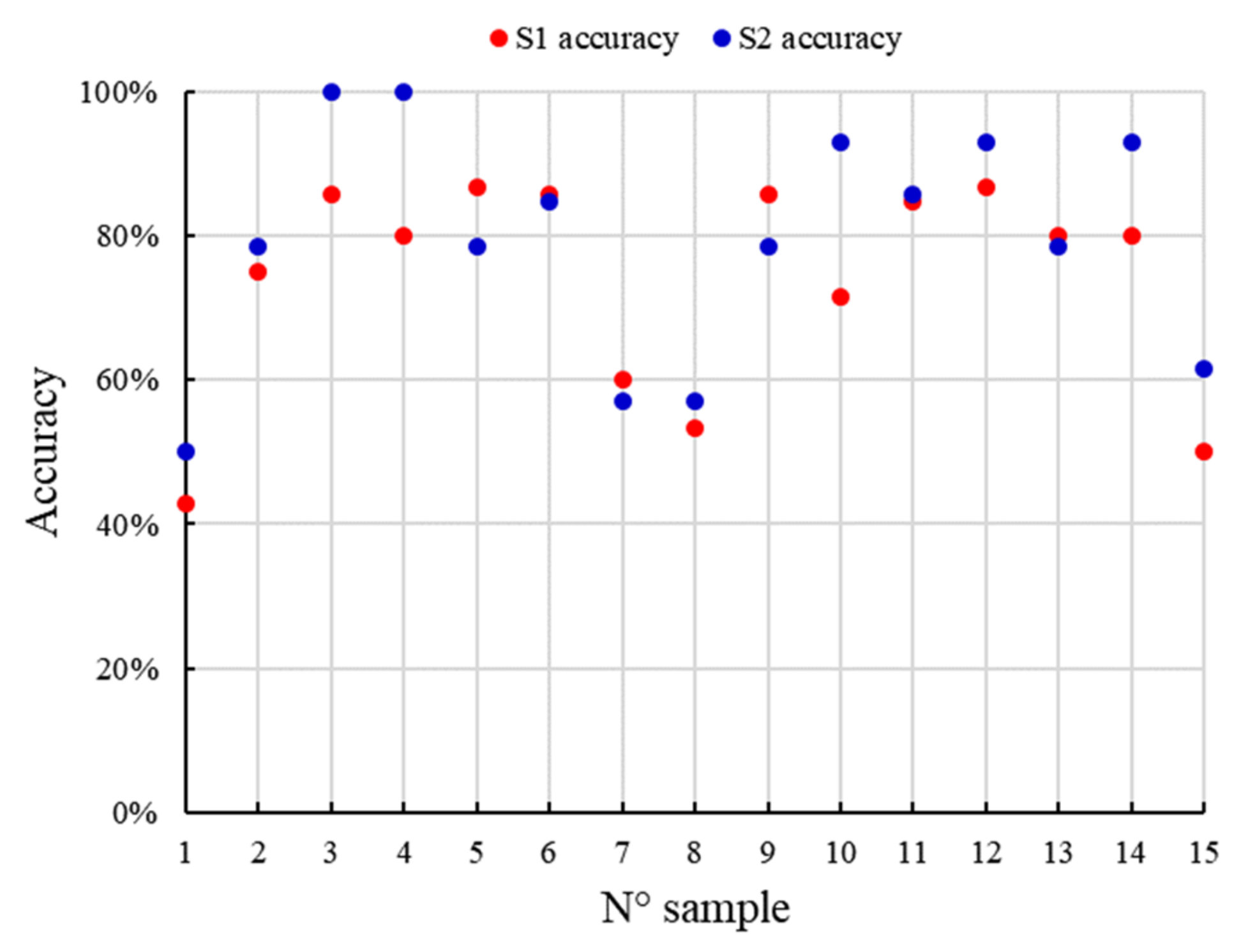
Figure 20.
Geometric verification accuracy for each S1 and S2 image set of the foot.
Figure 20.
Geometric verification accuracy for each S1 and S2 image set of the foot.
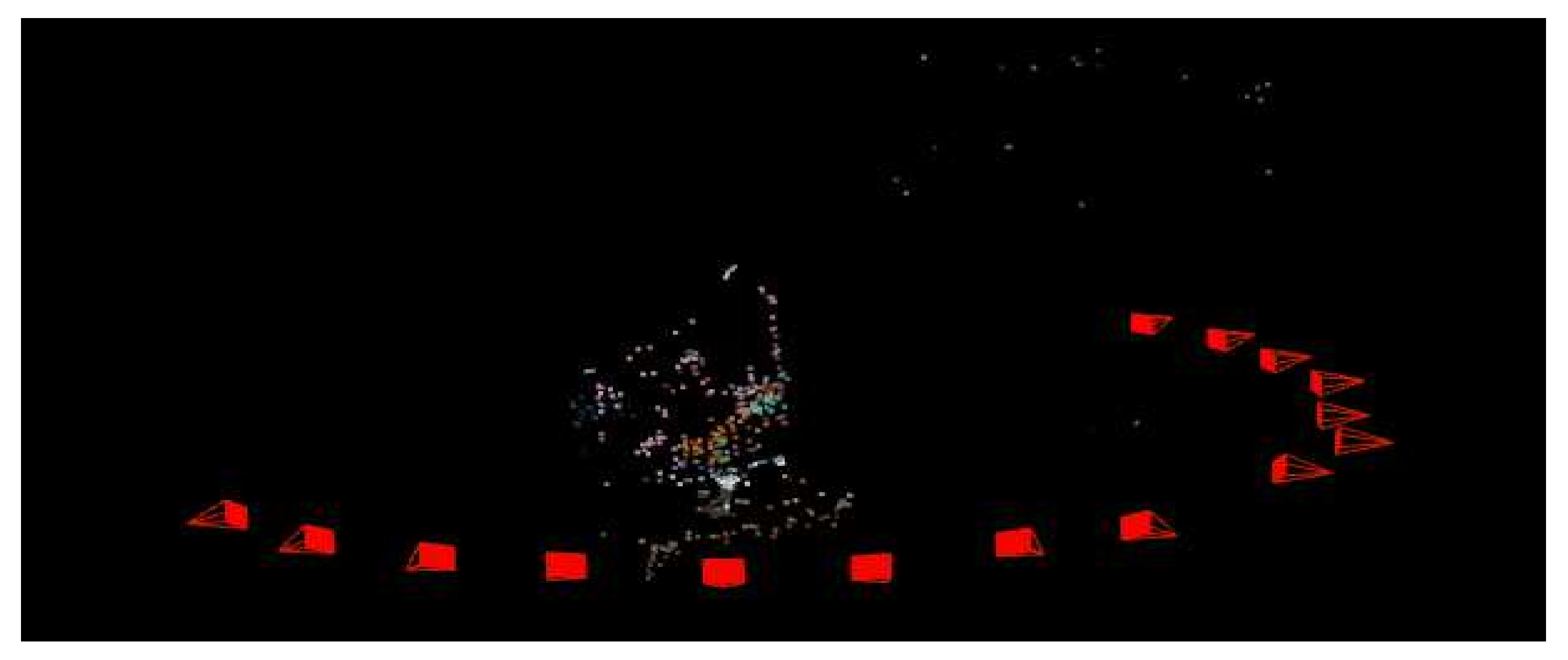
Figure 21.
Successive camera poses (the vertex of the red tetrahedron indicates the camera optical center position while the complete tetrahedron represents the camera orientation). This figure also shows the sparse 3D point cloud determined by COLMAP.
Figure 21.
Successive camera poses (the vertex of the red tetrahedron indicates the camera optical center position while the complete tetrahedron represents the camera orientation). This figure also shows the sparse 3D point cloud determined by COLMAP.
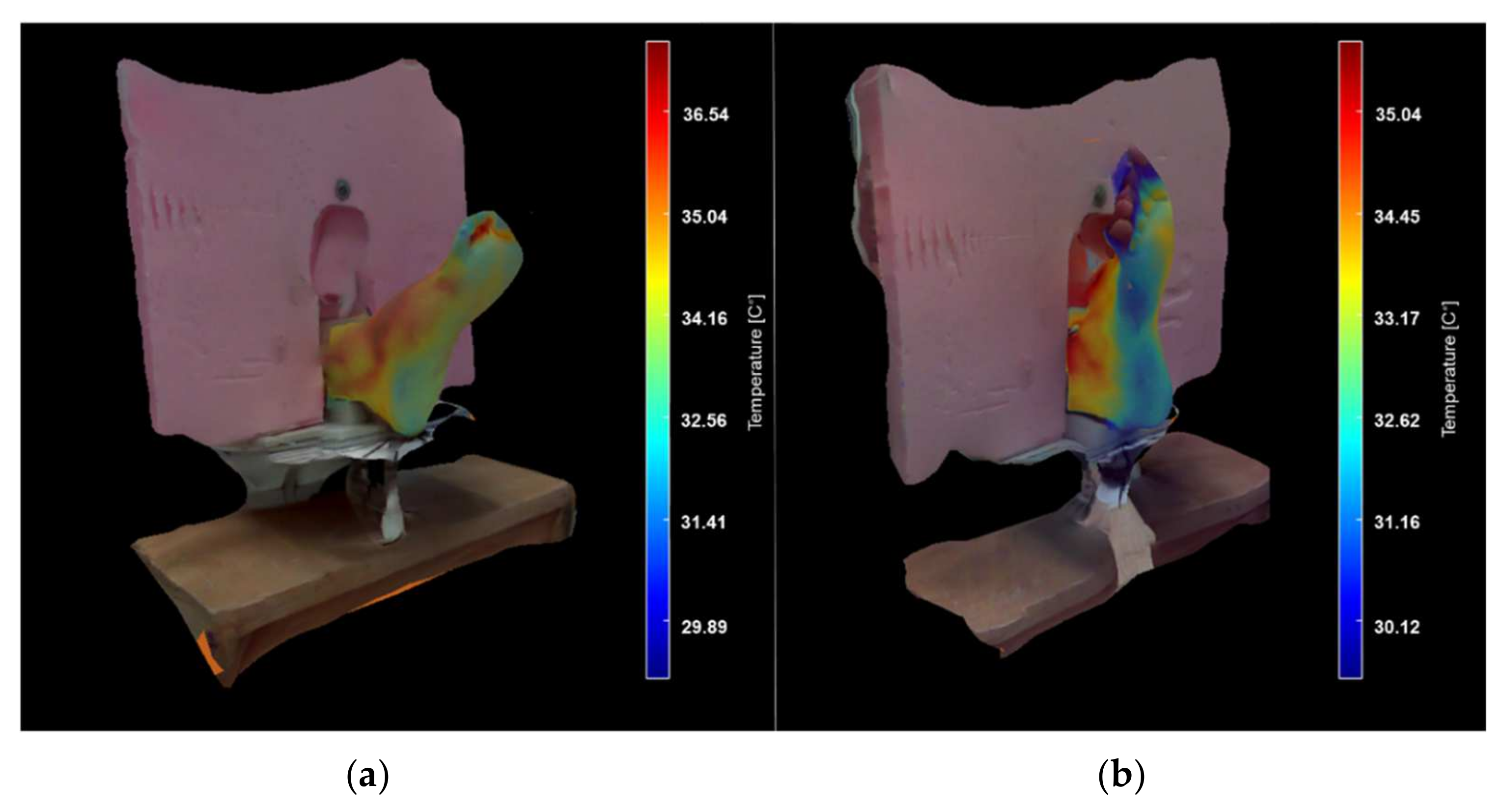
Figure 22.
3D models of the foot in a thermal surface and a visible-light environment. (a) Volunteer 1 and (b) Volunteer 2.
Figure 22.
3D models of the foot in a thermal surface and a visible-light environment. (a) Volunteer 1 and (b) Volunteer 2.
Table 1.
State-of-the-art of medical imaging for DM complication studies on lower limb and foot.
Table 1.
State-of-the-art of medical imaging for DM complication studies on lower limb and foot.
| Author | Year | Medical Imaging Technique | Application |
|---|
| Short and Zgonis [7] | 2017 | Tomography and MRI | Diabetic Charcot neuroarthropathy |
| Ramanujam et al. [8] | 2018 | Radiography and MRI | Diabetic Foot Osteomyelitis and Partial Foot Amputations |
| Toledo Peral et al. [9] | 2018 | Digital image processing | Skin Macules Characterization |
| Goyal et al. [10] | 2020 | Image-based machine learning algorithms | Recognition of ischemia and infection |
| Maldonado et al. [11] | 2020 | Image-based machine learning algorithms and thermography | Diabetic foot necrosis detection |
| Bayareh Mancilla et al. [12] | 2021 | Radiometry data and digital image processing | Detection of regions with non-homogeneous temperatures |
Table 2.
Overview of recent studies regarding the registration between visible and thermal images.
Table 2.
Overview of recent studies regarding the registration between visible and thermal images.
| Author | Year | Method | Application |
|---|
| Liu [24] | 2017 | Convolutional neural networks | Multi-modal medical image fusion aims |
| El-Hoseny et al. [25] | 2019 | Non-sub-Sampled Shearlet Transform and Modified Central Force Optimization | Object detection and medical diagnosis |
| González-Pérez et al. [20] | 2021 | Geometric Optical Translation, Homography, Iterative Closest Point, and Affine transform with Gradient Descent | Diabetic foot monitoring |
Table 3.
Overview of the 3D reconstruction techniques based on visible-light images and/or IR images. Although the acquisition techniques are different, the objective is common for all the reported papers for a 3D structure estimation.
Table 3.
Overview of the 3D reconstruction techniques based on visible-light images and/or IR images. Although the acquisition techniques are different, the objective is common for all the reported papers for a 3D structure estimation.
| Author | Year | Method | Optical Technique | Data/Image Processing | 3D Structure Estimation | Acquisition | Application |
|---|
| Souza et al. [27] | 2015 | Structured light | Active | Particle Swarm Optimization | Structure from motion | Sequential frames | General purposes |
| Chernov et al. [28] | 2017 | Stereoscopy | Active | Correlation between depth and IR images | Structure from motion | Non-sequential multi-frame | Breast reconstruction |
| van Doremalen et al. [29] | 2019 | Stereoscopy | Passive | Projective transformation | Not reported | Non-sequential multi-frame | Diabetic Foot study |
| de Queiroz Júnior and de Lima [30] | 2020 | Stereoscopy | Passive | Manual tracing of the profile curve | Not reported | Sequential frames | Breast pathologies study |
Table 4.
Fluke Ti32 Commercial Thermal Imager characteristics.
Table 4.
Fluke Ti32 Commercial Thermal Imager characteristics.
| Characteristics | Range | Units |
|---|
| Visible-light sensor resolution | 480 × 640 | Pixel |
| Infrared sensor resolution | 240 × 320 | Pixel |
| Temperature Range | −20 to +600 | °C |
| Thermal Sensitivity | ≤50 | mK |
| Infrared Spectral Band | 8–14 | µm |
| Minimal focus distance | 46 | cm |
| Refresh rate | 60 | Hz |
Table 5.
COLMAP parameters for feature detection, matching, and point cloud estimation.
Table 5.
COLMAP parameters for feature detection, matching, and point cloud estimation.
| Parameter | Value/Option |
|---|
| Camera model | Simple Radial |
| Guided Matching | Activated |
| Edge threshold | 50 |
| Peak threshold | 0.00067 |
Table 6.
RoI elements of the images collection S1 and S2. It is noticed that not all regions of interest have a constant number of elements.
Table 6.
RoI elements of the images collection S1 and S2. It is noticed that not all regions of interest have a constant number of elements.
| Image N° | Image Set S1 (Volunteer 1 Foot) | Image Set S2 (Volunteer 2 Foot) |
|---|
| RoI Elements | RoI % | RoI Elements | RoI % |
|---|
| 1 | 14,361 | 18.7 | 18,084 | 23.55 |
| 2 | 16,020 | 20.86 | 17,175 | 22.36 |
| 3 | 15,681 | 20.42 | 15,952 | 20.77 |
| 4 | 15,677 | 20.41 | 17,981 | 23.41 |
| 5 | 13,567 | 17.67 | 16,850 | 21.94 |
| 6 | 12,740 | 16.59 | 15,943 | 20.76 |
| 7 | 11,770 | 15.33 | 14,718 | 19.16 |
| 8 | 13,004 | 14.32 | 14,442 | 18.97 |
| 9 | 16,069 | 20.92 | 13,311 | 17.33 |
| 10 | 12,100 | 15.76 | 15,268 | 19.88 |
| 11 | 12,341 | 16.07 | 16,005 | 20.84 |
| 12 | 13,173 | 17.15 | 16,337 | 21.27 |
| 13 | 14,476 | 18.85 | 14,632 | 19.05 |
| 14 | 14,079 | 18.33 | 12,496 | 16.27 |
| 15 | 13,641 | 17.76 | 10,298 | 13.41 |
Table 7.
Detected and matched features in the two consecutive multimodal images.
Table 7.
Detected and matched features in the two consecutive multimodal images.
| Modality | Image Set S1 (Volunteer 1 Foot) | Image Set S2 (Volunteer 2 Foot) |
|---|
| Detected Features | Detected Features |
|---|
| IR | 307,404 | 99,887 |
| Visible light | 465,777 | 255,421 |
| IR + Visible light | 440,978 | 243,440 |
Table 8.
Statistics data retrieved by COLMAP.
Table 8.
Statistics data retrieved by COLMAP.
| Statistics | Image Set S1 (Volunteer 1 Foot) | Image Set S2 (Volunteer 2 Foot) |
|---|
| Cameras | 15 | 15 |
| Images | 15 | 15 |
| Registered images | 15 | 15 |
| Points | 907 | 1573 |
| Observations | 2731 | 4649 |
| Mean track length | 3.01103 | 2.9555 |
| Mean observations per image | 182.067 | 309.933 |
| Mean reprojection error | 0.916495 | 0.955175 |
Table 9.
∆T regarding the angle of measurement. The temperature was compensated in the original thermal arrays with the calculated delta.
Table 9.
∆T regarding the angle of measurement. The temperature was compensated in the original thermal arrays with the calculated delta.
| Angle of Acquisition (°) | Image Set S1 (Volunteer Foot 1) | Image Set S2 (Volunteer Foot 2) |
|---|
| Average Temperature (°C) | ∆T (%) | Average Temperature (°C) | ∆T (%) |
|---|
| 0 | 32.44 | 0.00 | 31.01 | 0.00 |
| 12 | 32.84 | 3.22 | 31.19 | 1.63 |
| 24 | 32.88 | 3.54 | 31.28 | 2.45 |
| 36 | 33.16 | 5.79 | 31.63 | 5.63 |
| 48 | 33.24 | 6.43 | 31.83 | 7.45 |
| 60 | 33.31 | 6.99 | 31.89 | 7.99 |
| 72 | 33.24 | 6.43 | 32.02 | 9.17 |
| 84 | 33.64 | 9.65 | 32.24 | 11.17 |
Table 10.
Average maximum and minimum temperatures for image sets S1 and S2. The temperature standard deviations were not higher than one degree, which can be acceptable to be considered as stable information concerning the passive thermography technique.
Table 10.
Average maximum and minimum temperatures for image sets S1 and S2. The temperature standard deviations were not higher than one degree, which can be acceptable to be considered as stable information concerning the passive thermography technique.
| Image Set | Average Maximum Temperature (°C) | Standard Deviation (°C) | Average Minimum Temperature (°C) | Standard Deviation (°C) |
|---|
| S1 | 36.54 | 0.24 | 29.89 | 0.67 |
| S2 | 35.04 | 0.56 | 30.12 | 0.78 |


 ,
, 























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}