Risk Perception and Its Influencing Factors among Construction Workers in Malawi
by
Esther Nkhawazawo Chaswa
1, 
Ishmael Bobby Mphangwe Kosamu
2,*,
Save Kumwenda
2 and
Wells Utembe
3 1
Malawi College of Health Sciences, P.O. Box 30368, Lilongwe 3, Malawi
2
The Polytechnic, Faculty of Applied Sciences, University of Malawi, Private Bag 303, Blantyre 3, Malawi
3
Toxicology Department, National institute for Occupational Health, Johannesburg 2001, South Africa
*
Author to whom correspondence should be addressed.
Safety 2020, 6(2), 33; https://0-doi-org.brum.beds.ac.uk/10.3390/safety6020033
Submission received: 3 April 2020
/
Revised: 25 May 2020
/
Accepted: 15 June 2020
/
Published: 24 June 2020
Abstract
:This study employed a deductive research approach and a survey strategy to assess risk perception and its influencing factors among construction workers in Malawi. Three specific construction hazards and their associated risks were selected. The hazards were “working at height (WAH)” “manual handling of loads (MHL)” and “heavy workload or intense pressure to be more productive (HWP).” The study engaged multistage sampling of 376 subjects. Univariate analysis, factor analysis and multiple linear regressions were performed in order to determine the main influencing factors among the independent variables. The study established that workers were aware of risks posed by their work. The majority perceived the risk associated with WAH, MHL and HWP as very high (62.7%, =8.80 ± 1.95); (48.5%, =8.10 ± 2.38); (57.9%, =8.49 ± 2.22) respectively. The study identified six factors as variables that showed a significant effect on workers’ perception of risk (p < 0.05). These factors were: “dreaded factor,” “avoidability and controllability,” “expert knowledge,” “personal knowledge,” “education level,” and “age”. It is concluded that contractors in the Malawian construction industry should integrate analysis of behaviors and risk perception of the workers and other players to guide the identification of better health and safety interventions at their worksites.
Keywords:
risk perception; safety; construction; workers; working at height; manual handling; workload; Malawi1. Introduction
Risk perception is defined as “the ability to determine the amount of risk from a hazard” while risk is defined as “the calculation of how likely an incident is to occur, and given its occurrence, how dire the consequences would be” [1]. Sjöberg, Moen [2] define risk perception as “the subjective assessment of the probability of a specified type of accident happening and how concerned people are with the consequences.” Several authors [3,4,5] agree that there are multiple factors which influence risk perception both at and outside work. At an individual level, a collection of psychological, social, institutional and cultural factors influence risk perception. These factors include safety climate, peer/community pressure, demographic and occupational characteristics. Risk perception is one of the factors that guides an individual’s response to risky situations [5]. When risk is perceived lowly, workers are left exposed to harmful work conditions [6]. In addition, lack of common perception of occupational risks among stakeholders compromises health and safety management at work [4]. “Risk management is a four-stage process; it involves identification of hazards in the work environment, assessment of the risks posed by the hazards, the selection of appropriate risk control measures according to a risk control hierarchy and review of control measures to ensure their effectiveness” [7].
Construction workers are at risk of exposure to a wide range of occupational health hazards [8], including “working at height (WAH) (risk of falling from a height causing serious injury),” “manual handling of loads (MHL) (risk of chronic musculoskeletal disorders),” and “heavy workload or intense pressure to be more productive (HWP) (risk of stress causing ill health).” The construction industry operates in a fragmented nature which, to some extent, contributes to the health and safety (H&S) hazards which construction workers are exposed to [9]. Construction work brings together a collection of tradesmen with very different practices and levels of skill, often working simultaneously at one site [8,9,10]. In addition to hazards from their own trade (primary hazards), construction workers are also exposed to hazards arising from jobs done by fellow tradesmen (bystander hazards). The physical worksite environment has been reported to create unsafe conditions in the construction industry [11]. In a study of risk perception among workers in the construction industry in the Pacific Northwest Region of USA [12], it was established that the level of perceived risk was five times higher than the tolerable risk value. Although exposure to a particular hazard in the construction industry is often characteristically irregular and short lived, chances of reoccurrence are usually high [8]. Nevertheless, despite the existence of various types of hazards, the construction industry is widely recognized as a major contributor to the economy of many nations [13].
There is scarcity of data and reported case studies for the Africa region on work-related injuries in specific sectors including the construction industry. Nevertheless, empirical research carried out in the region gives evidence of shortfalls in Occupational Health and Safety (OHS) regulations, management and practice which expose construction workers to risky working environments [14,15,16,17].
In Malawi, the Occupation Health, Safety and Welfare Act (OSHWA, 1997) makes provision for the regulation of the conditions of employment in workplaces regarding safety, health and welfare. However, utilization of the OSHWA is challenged by lack of sector-specific OHS regulations resulting in OHS standards not being met in most Malawian workplace environments [18]. Specifically, the regulatory authority of the construction industry falls under the jurisdiction of the National Construction Industry Council (NCIC) which was established through the National Construction Industry Act (NCIA) No. 19 of 1996. NCIC’s code of ethics for contractors requires that all contractors should give utmost consideration to safety, health and welfare of their workmen and the general public [19]. In spite of this, the standard of OHS practice in most sites in Malawi is poor. At sites where the contractors are making some efforts to promote H&S, for example, provision of personal protective equipment (PPE), cooperation and commitment of workers is often lacking. Safety measures are rarely followed, and PPE is worn incorrectly, disused or sold out. One notable result from a study on health and safety in the Malawian construction industry, conducted among key construction stakeholders, was that poor OHS persists in the construction industry [15]. Chiocha, Smallwood [15] concluded that consultants like architects and engineers, clients, project managers, building and civil contractors rarely provide significant contribution towards OHS, resulting in poor OHS standards in the Malawian construction industry. Malawi is reported to be far from meeting universal minimum standards of occupational health and safety, such as the ILO Convention No. 161 on Occupational Health Services and No. 155 on Occupational Safety and Health [18]. In another study by ILO [20], it was established that between 2000 and 2011, a total of 2034 occupation accidents were reported in Malawi and 7.4% of these were in the construction industry.
Occupational risks and risky behavior continue to be rampant in construction sites; a situation which may result in occurrence of accidents causing serious injuries and incidences of preventable ill health and death among workers. There appears to be lack of documented empirical evidence regarding the occupational risk perception of the various stakeholders in the construction industry in Malawi [15]. It is in this regard that this study sought to investigate risk perception of workers and its influencing factors in the construction industry, especially among workers of contractors in the central region of Malawi. Understanding how risk is perceived by people involved in construction is necessary for effective risk communication and risk management. It is also a critical step towards creating effective programs and campaigns to raise awareness and make construction workplaces safer. The study aimed at investigating risk perception and its related factors among construction workers in Malawi. Specifically, the study aimed to assess construction workers’ perception of risk posed by their work; identify factors that influence risk perception among construction workers; and determine construction workers’ actions related to perceived risky situations.
2. Materials and Methods
2.1. Study Population
The study was reviewed for ethical considerations and obtained approval on 27 November 2015 from University of Malawi-Polytechnic’s Postgraduate and Research Committee. The target population was all construction workers who are directly involved in actual construction work and these included brick layers, painters, plumbers, electricians, carpenters, unskilled laborers, their supervisors and managers. This excluded clients, employers (those not directly involved in work) and consultants. However, due to constraints of time and money, the study was conducted among construction workers working with building contractors in the central region of Malawi and registered with the National Construction Industry Council. In order to capture sufficient number of construction workers of all trades involved in construction, only contractors who had an active construction project were included.
According to key findings of the Malawi Labour Force Survey 2013, 2.6% of the 5.5 million (154,000) employed persons were in the construction sector [18]. From these key findings, it was estimated that there are over 10,000 construction workers in the central region of Malawi. Sample size was calculated using the Survey System sample size calculator; an online survey software package designed to help designing and conducting surveys. It allows for the calculation of sample size for large or unknown populations. At 95% confidence level and 5% significance level, an a priori sample was 384 construction workers. The study sampled 376 eligible subjects from 30 building construction sites. After excluding three subjects with missing data, 373 subjects remained, representing a response rate of 97%.
2.2. Research Design
The study was a cross-sectional survey involving analysis of data collected from the study population at a single point in time using multistage random sampling. Firstly, simple random sampling was employed to select a convenient number of 30 contractors from the 538 building contractors from the 2015 NCIC register for Central Region of Malawi. These contractors were contacted to inquire if they had an active project or not. Those without active projects were excluded and replaced by repeating the sampling process until the 30 active contractors were identified. All construction workers and subcontracted tradesmen working at project site of the selected contractors were eligible respondents. At each project site, 13 workers were selected. In the event that there were more than 13 construction workers at a site, simple random sampling was employed to select 13 workers who were included in the study.
2.3. Study Variables
First of all, three specific construction hazards and their associated risks were selected and termed as risk factors. These hazards were “WAH,” “risk of falling from a height causing serious injury,” “MHL,” “risk of chronic musculoskeletal disorders,” “HWP,” as well as risk of stress causing ill health. WAH was selected due to the fact that it is rated as the riskiest situation, causing many fatalities and injuries [7,21,22,23,24]. The other two hazards were selected based on their commonality among all trades in construction [8,19]. Respondents were asked to judge the “overall perceived risk” associated with each of the three risk factors; these were the criterion variables. In order to identify factors influencing risk perception, respondents were asked to rate each of the three risk factors across nine qualitative risk characteristics based on those used in the initial study of Portell, Gil [4]. In addition, data were collected on individual characteristics of the workers and construction site safety climate. Finally, the respondents’ immediate action when they or a fellow worker is exposed to a risky situation was assessed. The study variables are presented in Table 1.
2.4. Data Collection
Data was collected through in-depth interviews that were conducted either in English or Chichewa languages depending on the preference of the respondent. A questionnaire containing closed-ended questions was used to generate quantitative data. The interviews lasted for approximately 20 to 30 min. In addition, an observation checklist was administered at each project site to collect additional data regarding the state of health and safety at each construction site. The state of health and safety was assessed by observing availability of safety information and warnings, as well as availability and use of PPE.
The questionnaire comprised four sections, namely individual characteristics, risk perception and risk characteristics, safety climate and response to risky situations. Section one comprised questions on six individual worker’s characteristics, namely age, gender, education level, professional category, length of employment, and past history on safety training. Section two comprised ten questions developed by Portell, Gil [4], with Likert Scales that allowed respondents to rate each risk factor across nine qualitative risk characteristics and judge the overall perceived risk. For “overall perceived risk,” Portell, Gil [4] used scale starting at 0 (very small) to 100 (very high), while this questionnaire used a 0 to 10-point numeric scale. Section three adopted six safety climate evaluation questions developed by NIOSH-USA, rated on a numeric scale of 1 (strongly disagree) to 4 (strongly agree). Finally, section four comprised six questions that required the respondents to answer either yes or no to indicate the possible actions he or she would take in the event that he/she or co-workers were exposed to a risky situation.
2.5. Data Analysis
Data analysis was done using Statistical Package for Social Sciences version 16 (SPSS 16). First, univariate analysis was conducted to come up with descriptive statistics such as mean, standard deviation (SD), and percentage of the independent and dependent variables. Secondly, factor analysis of the risk qualitative characteristics was done. The analysis used principal component analysis (PCA) because communalities were high enough to opt for the PCA. To account for the problem that might arise due to inadequate sample size, the Barlett’s test of sphericity and the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy were performed. Initially, factors with Eigenvalues of over 1 were extracted. Furthermore, one method was selected to carry out the rotation: the Varimax, on assumption that the factors were not correlated with each other. In this method extraction was done, first with factor extraction via Eigenvalues >1. Lastly, multiple regressions were done to determine significantly influencing factors for the criterion variables. Multivariate Linear Regression analysis was performed by first changing the measurement levels of the three criterion variables: “WAH_Overall perceived risk,” “MHL_Overall perceived risk” and “HWP_Overall perceived risk,” from ordinal to continuous scale. This was followed by the multivariate linear regression on assumption that the three criterion variables were normally distributed.
3. Results and Discussion
3.1. Demographic Characteristics of Respondents
Out of the 373 study subjects, 98.4% (n = 367) were males, while 1.6% (n = 6) were females. Approximately 70% of the subjects were aged between 20 to 39 years (n = 268), 16.4% were aged 40–49 (n = 61), 7.8% were aged 50–59 (n = 29), 2.4% (n = 9) were over 60 years, while 1.6% (n = 6) were below the age of 20 years. The study subjects had a mean age of 35 years (+/−9.97). Majority of the subjects went as far as primary level of education (42.1%, n = 157); followed by secondary level (41.3%, n = 154); while only a few subjects completed vocational or tertiary levels of education (12.1%, n = 45 and 0.54%, n = 2, respectively). Four percent (n = 15) had no formal education. In terms of professional level, most of the subjects were skilled workers (62.7%, n = 234), 28.2% (n = 105) were general workers, 9.1% (n = 34) were supervisors and none of them had a managerial position. The skilled workers included trades such as brick layers (47%, n = 110), carpenters (19.7%, n = 46), electricians (7.7%, n = 18), plumbers (7.3%, n = 17) and steel fixers (9.4%, n = 22). The majority of the subjects (37.8%, n = 141) had work experience of over 10 years, 22.3% (n = 83) had work experience of 6–10 years, 31.6% (n = 118) had work experience of 1–5 years, while 8.3% (n = 31) had work experience of less than one year.
3.2. Construction Workers’ Perception of Risk
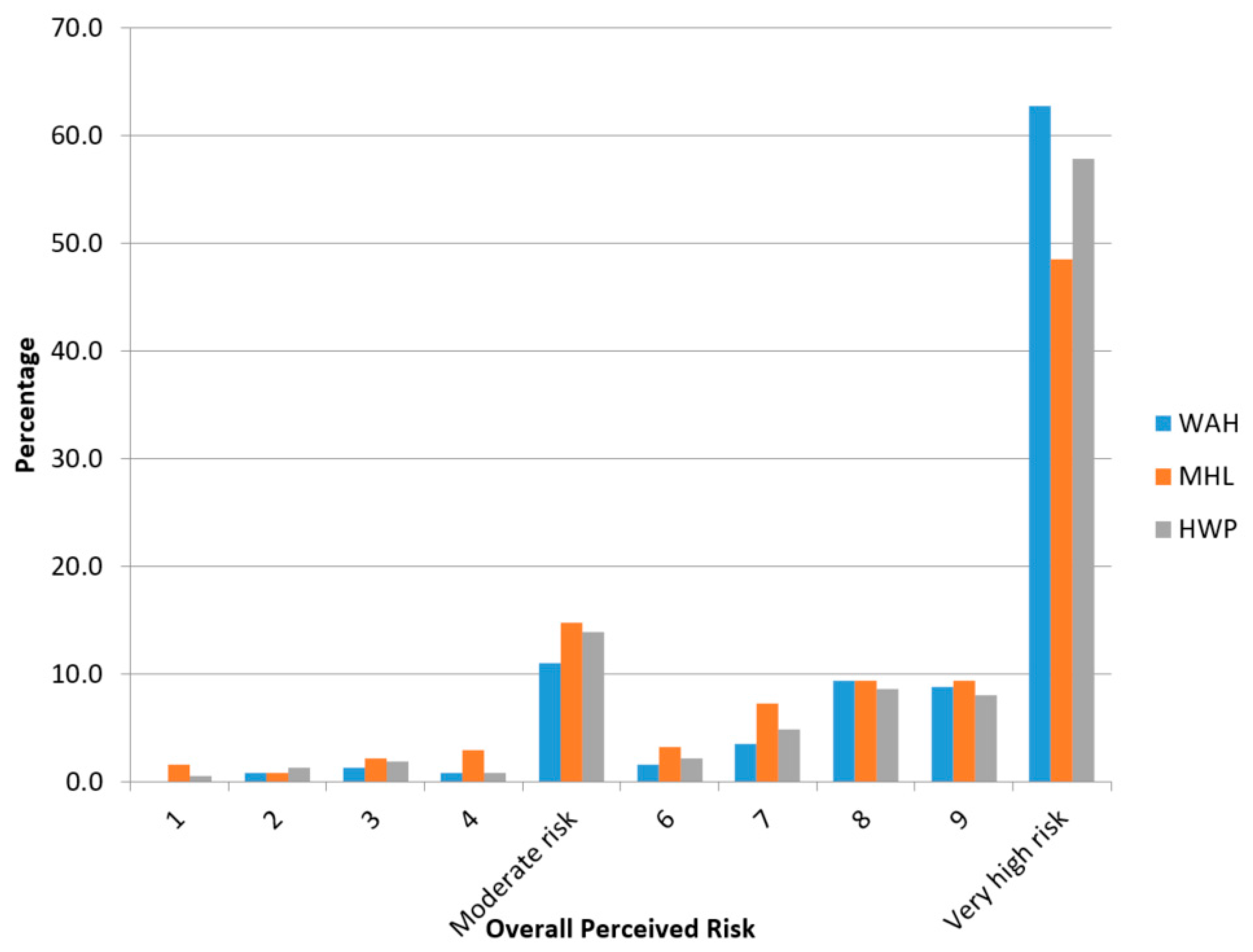
This study has shown that the majority of workers perceive the risks associated with WAH (63%, n = 234, = 8.8 ± 1.95), HWP (58%, n = 216, = 8.49 ± 2.22) and MHL (49%, n = 181, = 8.1 ± 2.38) as very high (Figure 1).
Similarly, the overall perceived risk (a combination of ratings for the three risk factors, WAH, MHL and HWP) showed that most workers (56%, n = 631) perceive risk posed by their construction work as being very high (Table 2). In Table 2, Risk Perception values of 1 to 4 are classified as Low Risk, 5 is Moderate Risk, 6 to 9 is High Risk, while 10 is very High Risk.
WAH_overall perceived risk score was highest ( = 8.8 ± 1.95) followed by HWP_overall perceived risk ( = 8.49 ± 2.22), while MHL_overall perceived risk had the lower score ( = 8.10 ± 2.38). This clearly reveals that construction workers in Malawi are aware of and understand the risks posed by their work. According to Portell, Gil [4], the evaluation of risk that workers make reveals their genuine concerns that may not be incorporated in expert risk assessments. These findings have shown that Malawian construction workers are in agreement with what other authors have said in that construction work is risky [8,10,22,24,25,26]. This is therefore a good premise for developing a proper safety culture [3] which can facilitate health and safety risk management in the Malawian construction industry. This is in consonant with what Charles [9] and Safe Work Australia [7] clearly stated in that an effective health and safety program in the workplace is underpinned by a good risk management system. Additionally, comparison of mean ratings of these three risk factors showed that workers are more concerned about the risk posed by WAH, then HWP, followed by MHL. This could be because working at a height is associated with high rates of fatal injuries worldwide [9,16,27], and such could also be the case in Malawi.
3.3. Factors Influencing Risk Perception
3.3.1. Qualitative Risk Characteristics
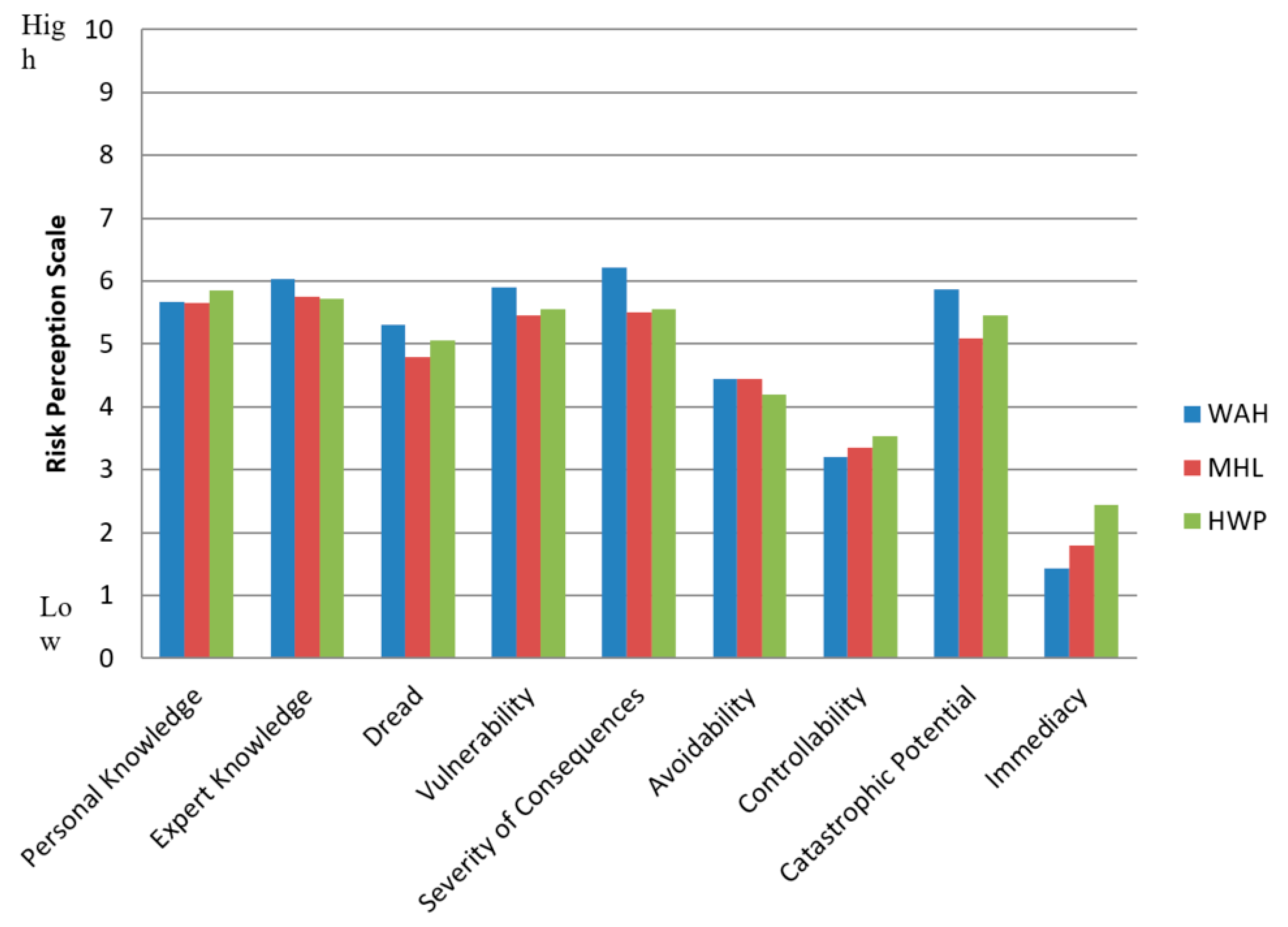
The study replicated the factor analysis of the psychometric paradigm to assess the influence of nine qualitative risk characteristics: expert knowledge, personal knowledge, dread, severity of consequences, catastrophic potential, avoidability, controllability and immediacy. Figure 2 shows the findings on the qualitative risk characteristics.
The study findings agree with several other studies that have used the psychometric paradigm [3,4,28] in that there is a correlation among many of them. There is a similarity in the way some of these qualitative risk characteristics are perceived. This study’s factor analysis (Table 3) identified four high-order factors that significantly accounted for risk perception among the workers. These are Factor 1 (dreaded factor) comprising “vulnerability, severity of consequences, dread and catastrophic potential” which accounted for 16.21% of total variance; Factor 2 (avoidability and controllability) which account for 12.17% of total variance; Factor 3 (expert knowledge) which accounted for 10.06% of the total variance; and finally Factor 4 (personal knowledge) which accounted for 5.89% of the total variance.
Findings from this study are consistent with previous psychometric studies and those that used other approaches in that Factor 1 (dreaded factor) has more influence on risk perception [4,28,29]. The findings revealed that “dreaded factor” accounted for a higher percentage (16.21%) of total variance as compared to the other factors. In fact, the dreaded factor proved to have significant influence on the perception of all the three risk factors, WAH, MHL and HWP. An increase in the perception of Factor 1 (dreaded factor) was associated with an increase in overall perceived risk for WAH, MHL and HWP. Factor 2 (avoidability and controllability) accounted for 12.17% and had a significant effect on WAH and HWP; the effect was rather inverse. An increase in the perception of “avoidability and controllability” decreased the overall perceived risk. Factor 3 (expert knowledge) accounted for 10.06% and had a positive effect on HWP. Lastly, Factor 4 (personal knowledge) accounted for 5.89% and also had a positive effect on WAH and HWP. It is apparent from these findings that risk control programmes should take into consideration the influence that these risk characteristics have on workers in order to create better measures that will make construction workplaces safer.
3.3.2. Individual Characteristics
Differing findings have been reported about the influence of individual characteristics [3,4,30]. This study, however, found that some characteristics like education level and age were significant predictors of risk perception while gender, professional category, duration of employment, attendance of safety induction or training course did not have any effect on construction workers’ risk perception. This is contrary to what Portell, Gil [4] observed in that individual characteristics “were not significant predictors of perceived risk.” A possible reason could be because the target populations of these studies were different (health care workers for Portell, Gil [4]). This study, however, concurs with Phoya, Eliufoo [30] in that education level attained influenced risk perception. Education was found to influence WAH and MHL, but the direction of influence differed as a function of the hazard. Perhaps workers’ understanding of the hazard characteristics improved, thereby influencing the way the workers perceived the risk posed by the hazards. Education influenced perception of WAH positively while it influenced MHL inversely. Attaining primary education decreased the score of WAH risk perception by factor of 3.337 (at 95% CI), as compared to attaining tertiary education. On the other hand, illiteracy significantly increased the score of MHL risk perception by a factor of 5.305 (at 95% CI).
This study also concurs with Phoya, Eliufoo, [30] in that the individual characteristic of age influenced risk perception. A significant decrease (by a factor of 1.933) in workers’ perception of risk associated with MHL was observed among young workers (aged 20 to 29) as compared to older workers. Interestingly, having an age <20 and 50 to 59 did not significantly predict risk perception, possibly due to the insufficient number of subjects that belonged to these groups (i.e., 6 = 1.6% and 29 = 7.8%, respectively).
According to findings by Portell, Gil [4] in their study about risk characterization among Spanish health care workers, professional category was a significant predictor for two risk variables, contrary to what has been revealed in this study. Professional category had no significant effect on any of the three risk variables of WAH, MHL and HWP. Alexopoulos, Kavadi [3] proved that risk perception was influenced by length of experience among Greek bakery workers. The “Greeks believed that risk management was a personal responsibility and was associated with length of work experience” (p. 7). Differing results were noted in this study in that length of experience had no effect on perception of risk for all the variables among the construction workers, possibly because the belief about who is responsible for safety is different.
3.3.3. Safety Climate
This study has revealed that majority (54.69%, n = 204) of the construction workers perceived their construction site safety climate as poor, followed by 42% (n = 158) who perceived their sites as fair. These findings echo what was reported by Chiocha, Smallwood [15] in that the OHS standards in Malawi construction sites are poor, and also agree with Zaid Alkilani, Jupp [13], Dias [31], Wong, Gray [6], and Pekka [32] in that construction sites in Malawi and Africa at large continue to be neglected with little or no effort to improve the health and safety conditions of the work sites. This situation is unpleasant considering that the construction industry employs a lot of people and is one of the major contributors to the country’s economy.
Findings similar to that reported by Zaid Alkilani, Jupp [13], Kheni, Gibb [16] and Musonda and Smallwood [17] were also observed at the construction sites. Contractor’s commitment to health and safety was pitiable as evidenced by failure to provide minimal OHS requirements like PPE, onsite safety signs and onsite safety training. This may be because the contractors have poor attitude towards health and safety; they lack health and safety awareness; or that they desire to maximize profits at the expense of workers’ lives. This also clearly indicates lack of monitoring and enforcement of existing OHS laws by regulatory authorities. Without deliberate effort from the regulatory bodies, contractors and other key players to improve the OHS state in Malawi, it is this research’s thesis that the construction industry will continue to negatively affect the health of workers through preventable occupational accidents and diseases.
According to Bohm and Harris [29], Inouye [1] and Hassan, Basha [33], a positive safety climate influences risk perception positively and reduces employees’ risk-taking behavior, thereby reducing workplace injury rates. Nevertheless, this study revealed contradicting findings in that workers’ perception of safety climate did not influence the worker’s risk perception. The regression analysis did not show a significant link between the safety climate and the worker’s risk perception. The possible reason is that most of the workers did not undergo safety inductions and that their sites lacked minimal safety requirements such that no idea or thought on safety (or risk) could be generated just by observing the safety climate at the sites.
3.4. Actions Related to Perceived Risky Situations
According to Rohrmann [5] as well as Schmidt [34], behaviors shown before, during and after an incident are greatly influenced by risk perception. Going by this statement, it would be expected that workers could stop working, report to supervisors, and request for PPE or safety information in the event that they or their colleagues are faced with a risky situation. Findings of this study are not consistent with findings by Rohrmann [5] and Schmidt [34] who said that behaviors are greatly influenced by risk perception. Another study in Romania [35] has also shown that men-dominated activities such as those in the construction industry (excluding mining) are generally perceived as riskier by workers. This study, however, is in agreement with Bohm and Harris [29] in that the relationship between risk perception and risk-taking behavior is rather complicated. Risky behaviors are not always as a result of misjudgment of risk. In some instances, willingness to engage in risky behavior prevails. This is what was observed in this study. Despite perceiving the risk posed by their work as risky, majority (58%, n = 218) of construction workers indicated that they would not stop working to report to their supervisor in times of risky situations; 80% (n = 299) would not ask for information regarding health and safety from their supervisor; and 67% (n = 234) would not request for PPE. The majority of workers (82%, n = 307) indicated that they would manage to warn co-workers about health and safety risks of the situation but continue working (63.27%, n = 236) even with full knowledge of risks associated. As highlighted by Sjöberg, Moen [2], construction workers in Malawi continue to work while tolerating considerably more risk at the expense of their health and safety. This could be because most of them are unskilled workers, do not have the required qualifications (even though they work as skilled workers) or they are desperate for the job. This is a sorry state because the construction sector in Malawi will continue to cause ill health and claim lives of workers unless safety measures are deliberately put it place to improve the safety climate and safety behaviors of the workers.
4. Conclusions
Risk perception by Malawian construction workers is influenced by a number of factors. These factors include qualitative risk characteristics like dreaded factor; avoidability and controllability; expert knowledge; personal knowledge; and individual characteristics of age and education level. Gender, professional category, length of employment, safety training history and safety climate did not show a significant link with the worker’s risk perception. These findings may be easily generalizable to the construction industry in Malawi and other countries with similar socioeconomic conditions. However, it has to be emphasized that human behaviour changes over time. As such, risk perceptions and indicators for behavioral safety compliance are subject to change. This study was done in 2015 and utilized a cross-sectional design which could only capture a snapshot of the situation in the construction industry in Malawi at that time. It is highly likely that the risk perspectives which have been highlighted in this study and the factors that influence them may have changed over time. Future studies should therefore consider the use of longitudinal studies that may capture more recent, real-time information consistently over a longer time period. Other factors not included in this study but need to be investigated include peer pressure and optimism bias.
The study has revealed that the status of health and safety management in many construction sites in Malawi remains poor. Nonetheless, the workers continue to work in hazardous environments despite being fully aware of the risks involved; with little effort by themselves, their employers (contractors) or other responsible authorities to promote health and safety. The quality of life of workers is a crucial prerequisite for productivity and is of utmost importance for overall socio-economic development. There is need, therefore, for the construction industry regulatory body (NCIC) in collaboration with OHS department to strengthen monitoring of contractors’ compliance with health and safety obligations as stipulated in OSHWA and the contractors’ code of ethics. This can be achieved by establishing a fully-fledged OHS monitoring section at NCIC and implementing strict corrective and disciplinary actions to non-complying contractors. NCIC should develop OHS awareness programs targeting key players in construction like contractor management and consultants such as engineers, architects and surveyors. The contractors should incorporate OHS management programs in the implementation of projects because it is their legal and moral obligation. Worker OHS inductions focusing on understanding work site risks and their management should form an integral part of a contractor’s OHS management program.
Author Contributions
E.N.C. was studying for a postgraduate Degree in Environmental Health at University of Malawi, The Polytechnic and she designed the research, collected data, analyzed and developed the manuscript. I.B.M.K., S.K. and W.U. from both the National Institute for Occupational Health in South Africa and the University of Malawi, The Polytechnic were involved significantly at each stage of the manuscript writing, field scoping, data analysis and reviewing the study tools. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
The authors acknowledge Malawi College of Health Sciences, Collins Kaunda of Image Designs in Malawi, and University of Malawi, The Polytechnic for making this study possible. Many thanks should also go to the construction workers for the lively participation during the data collection.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Inouye, J. Risk Perception: Theories, Strategies, and Next Steps; Campbell Institute National Safety Council: Itasca, IL, USA, 2014. [Google Scholar]
- Sjöberg, L.; Moen, B.E.; Rundmo, T. Explaining Risk Perception. An Evaluation of the Psychometric Paradigm in Risk Perception Research; Rotunde publikasjoner Rotunde: Trondheim, Norway, 2004. [Google Scholar]
- Alexopoulos, E.C.; Kavadi, Z.; Bakoyannis, G.; Papantonopoulos, S. Subjective risk assessment and perception in the Greek and English bakery industries. J. Environ. Pub. Health 2009, 6, 891754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portell, M.; Gil, M.R.; Losilla, M.J.; Vives, J. Characterizing occupational risk perception: The case of biological, ergonomic and organizational hazards in Spanish healthcare workers. Span. J. Psychol. 2014, 17, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohrmann, B. Risk perception, risk attitude, risk communication, risk management: A conceptual appraisal. In Proceedings of the 15th International Emergency Management Society (TIEMS) Annual Conference, Prague, Czech Republic, 17–19 June 2008. [Google Scholar]
- Wong, J.Y.Y.; Gray, J.; Sadiqi, Z. Barriers to good occupational health and safety (OHS) practices by small construction firms. J. Constr. Manag. 2015, 30, 55–66. [Google Scholar]
- SWA. How to Manage Work Health and Safety Risks: Code of Practice; Safe Work Australia: Canberra, Australia, 2011.
- Weeks, J.L. Health and Safety Hazards in the Construction Industry. Encyclopedia of Occupation Health and Safety. 2011. Available online: http://www.ilocis.org (accessed on 15 August 2019).
- Charles, M.; Pillay, J.; Ryan, R. Guide to Best Practice for Safer Construction: Literature Review from Concept to Completion; Cooperative Research Centre for Construction Innovation: Melbourne, Australia, 2007. [Google Scholar]
- Hinksman, J. Major Sectors and Their Hazards. Encyclopedia of Occupational Health and Safety. Available online: http://www.iloencyclopedia.org (accessed on 15 August 2019).
- Lingard, H. Occupational health and safety in the construction industry. Constr. Manag. Econ. 2013, 31, 505–514. [Google Scholar] [CrossRef]
- Hallowell, M. Safety risk perception in construction companies in the Pacific Northwest of the USA. Constr. Manag. Econ. 2010, 28, 403–413. [Google Scholar] [CrossRef]
- Zaid Alkilani, S.; Jupp, J.; Sawhney, A. Issues of construction health and safety in developing countries: A case of Jordan. Australas. J. Constr. Econ. Build. 2013, 13, 141. [Google Scholar] [CrossRef] [Green Version]
- Agumba, J.; Pretorius, J.H.; Haupt, T. Health and safety management practices in small and medium enterprises in the South African construction industry. Acta Structilia 2013, 20, 66–88. [Google Scholar]
- Chiocha, C.; Smallwood, J.; Emuze, F. Health and safety in the Malawian construction industry. Acta Structilia 2011, 18, 68–80. [Google Scholar]
- Kheni, N.A.; Gibb, A.G.; Dainty, A.R. The management of construction site health and safety by small and medium-sized construction businesses in developing countries: A Ghana case study. In Proceedings of the 22nd Annual ARCOM Conference, Birmingham, UK, 4–6 September 2006. [Google Scholar]
- Musonda, I.; Smallwood, J. Health and safety (H&S) awareness and implementation in Botswana’s construction industry. J. Eng. Des. Technol. 2008, 6, 81–90. [Google Scholar]
- Morse, D.T.; Taulo, D.S.; Lungu, K. Gap Analysis of Research Needs in Environmental Health, Malawi; The National Commission of Science and Technology: Lilongwe, Malawi, 2010.
- NCIC. Code of Ethics for Contractors in the Construction Industry. Malawi; The National Construction Industry Council of Malawi: Lilongwe, Malawi, 2009.
- ILO. Recording and Notification of Occupational Accidents and Diseases in Malawi. Geneva, Switzerland. 2012. Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---safework/documents/publication/wcms_208201.pdf (accessed on 10 April 2020).
- NSO. Malawi Labour Force Survey; National Statistical Office of Malawi: Zomba, Malawi, 2014.
- Hughes, P.; Ferrett, E. Introduction to Health and Safety at Work: The Handbook for the NEBOSH; Elsevier Butterworth-Heinemann: Oxford, UK, 2004. [Google Scholar]
- Schwatka, N.V.; Butler, L.M.; Rosecrance, J.R. An aging workforce and injury in the construction industry. Epidemiol. Rev. 2011, 34, 156–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, N.; Hrymak, V. Safety Behaviour in the Construction Industry: Report to the Health and Safety Authority; The Health and Safety Executive: Dublin, UK, 2002.
- Hislop, R.D. Construction Site Safety: A Guide for Managing Contractors; CRC Press: Boca Raton, FL, USA, 1999. [Google Scholar]
- ILO. The Construction Industry in the Twenty First Century: It’s Image, Employment Prospects and Skill Requirements. 2001. Available online: https://www.ilo.org/global/publications/ilo-bookstore/order-online/books/WCMS_PUBL_9221126226_EN/lang--en/index.htm (accessed on 20 August 2019).
- Petrovic-Lazarevic, S.; Perry, M.; Ranjan, R. Improving the occupational health and safety measures in the Australian construction industry. Zagreb Int. Rev. 2007, 10, 17–34. [Google Scholar]
- Slovic, P. Perception of risk. Science 1987, 236, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Bohm, J.; Harris, D. Risk perception and risk-taking behavior of construction site dumper drivers. Int. J. Occup. Saf. Ergon. 2010, 16, 55–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phoya, S.; Eliufoo, H.; Pietrzyk, K.; Nyström, M. Assessment of Health and Safety Risk Perception of Site Managers, Supervisors and Workers in Tanzania Urban Construction Sites. In Proceedings of the Prevention: Means to end of safety and health incidents and illiness Conference, Washington, DC, USA, 24–26 August 2011. [Google Scholar]
- Dias, A.L. Inspecting Occupational Safety and Health in the Construction Industry; International Training Centre of the ILO: Turin, Italy, 2009. [Google Scholar]
- Pekka, R. Health, Prevention and Management. Encyclopedia of Occupational Health and Safety. 2011. Available online: Hhtp://www.iloencyclopedia.org (accessed on 18 August 2019).
- Hassan, C.C.; Basha, O.; Hanafi, W.W. Perception of building construction workers towards safety, health and environment. J. Eng. Sci. Technol. 2007, 3, 271–279. [Google Scholar]
- Schmidt, M. Investigating Risk Perception: A Short Introduction. Loss of Agro-Biodiversity in Vavilov Centers, with a Special Focus of Genetically Modified Organisms (GMOs). Ph.D. Thesis, University of Vienna, Vienna, Austria, 2004. [Google Scholar]
- Ivascu, L.; Cioca, L.I. Occupational accidents assessment by field of activity and investigation model for prevention and control. Safety 2019, 5, 12. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Percentage Distribution of Respondents by Overall Perceived Risk for working at height (WAH), manual handling of loads (MHL) and heavy workload or intense pressure to be more productive (HWP).
Figure 1.
Percentage Distribution of Respondents by Overall Perceived Risk for working at height (WAH), manual handling of loads (MHL) and heavy workload or intense pressure to be more productive (HWP).

Figure 2.
Profile of Mean Ratings for Qualitative Risk Characteristics.


{kind=link}
{kind=link}
Table 1.
An overview of the study variables.
| Criterion Variables | WAH-Overall Perceived Risk MHL-Overall Perceived Risk HWP-Overall Perceived Risk | |
|---|---|---|
| Independent Variables | Categories | Variables |
| Qualitative Risk Characteristics | Dread Factor- dread, vulnerability, severity and catastrophic potential | |
| Knowledge/understanding factor- personal knowledge, expert knowledge and immediacy | ||
| Controllable damage factor: “avoidability” and “controllability.” | ||
| Individual Characteristics | Age | |
| Gender | ||
| Education Level | ||
| Professional Category | ||
| Length of employment | ||
| Safety Training History | ||
| Safety Climate | Construction Site Safety Climate | |
| Response to risky situation | Immediate action when exposed to risky situation | |
Table 2.
Number and Percentage Distribution of Respondents by Overall Perceived Risk.
| Risk Perception Scale Values | Count (n) | Percent (%) |
|---|---|---|
| 1 | 8 | 0.7 |
| 2 | 11 | 1.0 |
| 3 | 20 | 1.8 |
| 4 | 17 | 1.5 |
| Moderate Risk | 148 | 13.2 |
| 6 | 26 | 2.3 |
| 7 | 58 | 5.2 |
| 8 | 102 | 9.1 |
| 9 | 98 | 8.8 |
| Very High Risk | 631 | 56.4 |
| Total | 1119 | 100 |
Table 3.
Risk Characteristics Factor Analysis Rotational Component Matrix.
| Risk Characteristics | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
|---|---|---|---|---|
| HWP_Dread | 0.737 | 0.064 | −0.056 | 0.045 |
| MHL_Dread | 0.625 | −0.070 | −0.189 | 0.158 |
| WAH_Dread | 0.488 | −0.082 | −0.022 | 0.015 |
| HWP_Vunerability | 0.724 | 0.043 | 0.093 | −0.134 |
| MHL_Vunerability | 0.664 | −0.085 | −0.081 | 0.223 |
| WAH_Vunerability | 0.447 | −0.323 | 0.094 | −0.090 |
| HWP_Catastrophic potential | 0.640 | 0.082 | 0.040 | −0.277 |
| MHL_Catastrophic potential | 0.541 | −0.042 | −0.023 | −0.089 |
| WAH_Catastrophic potential | 0.327 | −0.146 | 0.161 | −0.427 |
| HWP_Severity of consequences | 0.623 | 0.148 | 0.080 | −0.205 |
| MHL_Severity of consequences | 0.600 | −0.239 | −0.010 | 0.159 |
| WAH_Severity of consequences | 0.160 | −0.121 | 0.334 | −0.083 |
| HWP_Controllability | −0.103 | 0.580 | −0.031 | −0.142 |
| MHL_Controllability | −0.063 | 0.744 | 0.042 | 0.025 |
| WAH_Controllability | 0.039 | 0.727 | 0.134 | −0.011 |
| HWP_Avoidability | 0.219 | 0.665 | −0.117 | 0.039 |
| MHL_Avoidability | 0.083 | 0.733 | −0.052 | 0.015 |
| HWP_Expert Knowledge | −0.082 | −0.105 | 0.755 | −0.152 |
| MHL_Expert Knowledge | −0.142 | 0.009 | 0.798 | −0.021 |
| WAH_Expert Knowledge | −0.156 | 0.039 | 0.705 | −0.150 |
| HWP_Personal Knowledge | 0.402 | 0.149 | 0.363 | 0.294 |
| MHL_Personal Knowledge | 0.185 | 0.105 | 0.437 | 0.624 |
| WAH_Personal Knowledge | 0.093 | 0.062 | 0.384 | 0.570 |
| MHL_Immediacy | 0.046 | −0.033 | −0.238 | 0.396 |
| HWP_Immediacy | −0.292 | −0.240 | −0.240 | 0.347 |
| WAH_Immediacy | 0.147 | 0.051 | −0.414 | −0.030 |
| Eigenvalue | 4.376 | 3.287 | 2.715 | 1.592 |
| % Variance accounted for: | 16.206 | 12.174 | 10.057 | 5.898 |
| Cumulative Variance | 16.206 | 28.380 | 38.437 | 44.335 |
Note: Extraction method is Principal Component Analysis with Kaizer Normalization. Factor loadings ≥0.5 are reported in bold.
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chaswa, E.N.; Kosamu, I.B.M.; Kumwenda, S.; Utembe, W. Risk Perception and Its Influencing Factors among Construction Workers in Malawi. Safety 2020, 6, 33. https://0-doi-org.brum.beds.ac.uk/10.3390/safety6020033
AMA Style
Chaswa EN, Kosamu IBM, Kumwenda S, Utembe W. Risk Perception and Its Influencing Factors among Construction Workers in Malawi. Safety. 2020; 6(2):33. https://0-doi-org.brum.beds.ac.uk/10.3390/safety6020033
Chicago/Turabian StyleChaswa, Esther Nkhawazawo, Ishmael Bobby Mphangwe Kosamu, Save Kumwenda, and Wells Utembe. 2020. "Risk Perception and Its Influencing Factors among Construction Workers in Malawi" Safety 6, no. 2: 33. https://0-doi-org.brum.beds.ac.uk/10.3390/safety6020033
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.