Knowledge, Attitudes, and Barriers towards Dietary Pulse Consumption in Women with Polycystic Ovary Syndrome Participating in a Multi-Disciplinary Lifestyle Intervention to Improve Women’s Health

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Ethical Approval
2.3. Participants
2.4. PCOS Diagnosis
2.5. Inclusion and Exclusion Criteria
2.6. Randomisation Procedures
2.7. Blinding Procedures
2.8. Intervention
2.9. Pulse Consumption Questionnaire
2.10. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Effect of Lifestyle Modification on Pulse Consumption Questionnaire Scores
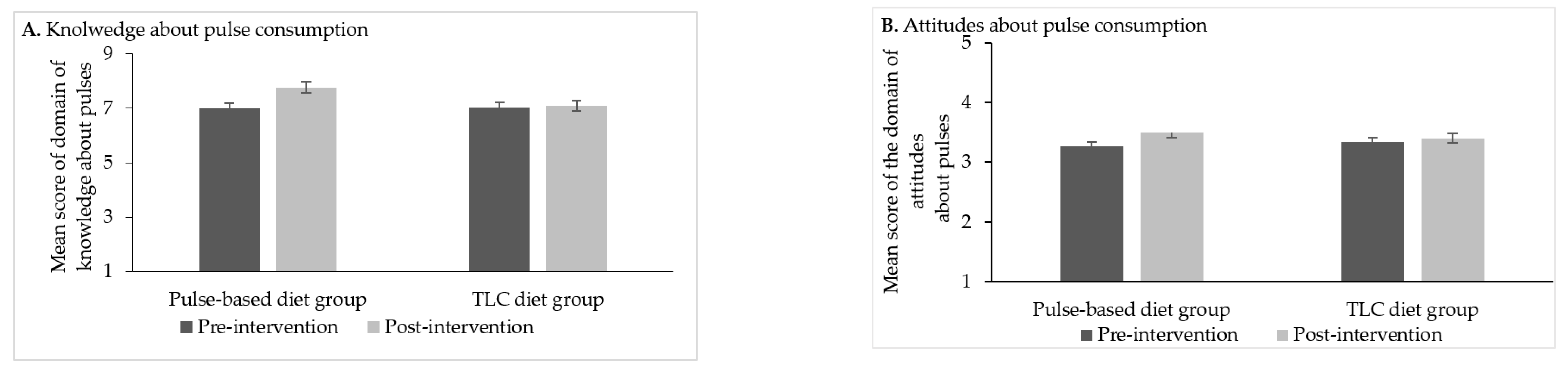
3.2.1. Knowledge
3.2.2. Attitudes
3.2.3. Perceived Barriers and Frequency
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kazemi, M.; Buddemeyer, S.; Fassett, C.M.; Gans, W.M.; Johnston, K.M.; Lungu, E.; Savelle, R.L.; Tolani, P.N.; Dahl, W.J. Chapter 5: Pulses and Prevention and Management of Chronic Disease. In Health Benefits of Pulses, 1st ed.; Dahl, W., Ed.; Springer Nature Switzerland AG: Cham, Switzerland, 2019; pp. 55–72. [Google Scholar] [CrossRef]
- Bekkering, E. Canadian Agriculture at a Glance. Pulses in Canada. Available online: https://www150.statcan.gc.ca/n1/en/pub/96-325-x/2014001/article/14041-eng.pdf?st=uNw1MxTH (accessed on 10 May 2020).
- Mudryj, A.N. Chapter 2. Pulse consumption: A global perspective. In Health Benefits of Pulses, 1st ed.; Dahl, W., Ed.; Springer: Cham, Switzerland, 2019; pp. 19–33. [Google Scholar] [CrossRef]
- Mudryj, A.N.; Aukema, H.M.; Fieldhouse, P.; Yu, B.N. Nutrient and food group intakes of Manitoba children and youth: A population-based analysis by pulse and soy consumption status. Can. J. Diet. Pract. Res. 2016, 77, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Ipsos, R. Factors Influencing Pulse Consumption in Canada. Summary Report. Alberta Agriculture and Rural Development. Government of Alberta. Available online: https://www1.agric.gov.ab.ca/$department/deptdocs.nsf/ba3468a2a8681f69872569d60073fde1/da8c7aee8f2470c38725771c0078f0bb/$FILE/v3_factors_influencing_pulse_consumption_final_report_feb24_2010.pdf (accessed on 20 April 2020).
- Mitchell, D.C.; Lawrence, F.R.; Hartman, T.J.; Curran, J.M. Consumption of dry beans, peas, and lentils could improve diet quality in the US population. J. Acad. Nutr. Diet. 2009, 109, 909–913. [Google Scholar] [CrossRef] [PubMed]
- Guenther, P.M.; Dodd, K.W.; Reedy, J.; Krebs-Smith, S.M. Most Americans eat much less than recommended amounts of fruits and vegetables. J. Am. Diet. Assoc. 2006, 106, 1371–1379. [Google Scholar] [CrossRef] [PubMed]
- Ha, V.; Sievenpiper, J.L.; de Souza, R.J.; Jayalath, V.H.; Mirrahimi, A.; Agarwal, A.; Chiavaroli, L.; Mejia, S.B.; Sacks, F.M.; di Buono, M. Effect of dietary pulse intake on established therapeutic lipid targets for cardiovascular risk reduction: A systematic review and meta-analysis of randomized controlled trials. CMAJ 2014, 186, E252–E262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, A.V. Overview of the market and consumption of pulses in Europe. Br. J. Nutr. 2002, 88 (Suppl. 3), S243–S250. [Google Scholar] [CrossRef] [Green Version]
- March, W.A.; Moore, V.M.; Willson, K.J.; Phillips, D.I.W.; Norman, R.J.; Davies, M.J. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Hum. Reprod. 2010, 25, 544–551. [Google Scholar] [CrossRef] [Green Version]
- Carmina, E.; Lobo, R.A. Polycystic ovary syndrome (PCOS): Arguably the most common endocrinopathy is associated with significant morbidity in women. J. Clin. Endocrinol. Metab. 1999, 84, 1897–1899. [Google Scholar] [CrossRef]
- Kazemi, M.; Pierson, R.A.; Lujan, M.E.; Chilibeck, P.D.; McBreairty, L.E.; Gordon, J.J.; Serrao, S.B.; Zello, G.A.; Chizen, D.R. Comprehensive evaluation of type 2 diabetes and cardiovascular disease risk profiles in reproductive-age women with polycystic ovary syndrome: A large Canadian cohort. J. Obstet. Gynaecol. Can. 2019, 41, 1453–1460. [Google Scholar] [CrossRef]
- Kazemi, M.; Kim, J.; Parry, S.; Azziz, R.; Lujan, M. Disparities in cardio-metabolic risk profile between Black and White women with polycystic ovary syndrome: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2020, 31395–31398. [Google Scholar] [CrossRef]
- Kazemi, M.; Jarrett, B.Y.; Parry, S.A.; Thalacker-Mercer, A.; Hoeger, K.M.; Spandorfer, S.D.; Lujan, M.E. Osteosarcopenia in reproductive-aged women with polycystic ovary syndrome: A multicenter case-control study. J. Clin. Endocrinol. Metab. 2020, 105, e3400–e3414. [Google Scholar] [CrossRef]
- McBreairty, L.E.; Kazemi, M.; Chilibeck, P.D.; Gordon, J.J.; Chizen, D.R.; Zello, G.A. Effect of a pulse-based diet and aerobic exercise on bone measures and body composition in women with polycystic ovary syndrome: A randomized controlled trial. Bone Rep. 2020, 12, 100248. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J.; International PCOS Network. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. 2018, 33, 1602–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazemi, M.; Hadi, A.; Pierson, R.A.; Lujan, M.E.; Zello, G.A.; Chilibeck, P.D. Effects of dietary glycemic index and glycemic load on cardio-metabolic and reproductive profiles in women with polycystic ovary syndrome: A systematic review and meta-analysis of randomized controlled trials. Adv. Nutr. 2020, nmaa092. [Google Scholar] [CrossRef]
- Kazemi, M.; McBreairty, L.E.; Chizen, D.R.; Pierson, R.A.; Chilibeck, P.D.; Zello, G.A. A comparison of a pulse-based diet and the Therapeutic Lifestyle Changes diet in combination with exercise and health counselling on the cardio-metabolic risk profile in women with polycystic ovary syndrome: A randomized controlled trial. Nutrients 2018, 10, 1387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazemi, M.; Pierson, R.A.; McBreairty, L.E.; Chilibeck, P.D.; Zello, G.A.; Chizen, D.R. A randomized controlled trial of a lifestyle intervention with longitudinal follow up on ovarian dysmorphology in women with polycystic ovary syndrome. Clin. Endocrinol. 2020, 92, 525–535. [Google Scholar] [CrossRef]
- National Cholesterol Education Program (NCEP). Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- McCrory, M.A.; Hamaker, B.R.; Lovejoy, J.C.; Eichelsdoerfer, P.E. Pulse consumption, satiety, and weight management. Adv. Nutr. 2010, 1, 17–30. [Google Scholar] [CrossRef] [Green Version]
- Sievenpiper, J.L.; Kendall, C.W.C.; Esfahani, A.; Wong, J.M.W.; Carleton, A.J.; Jiang, H.Y.; Bazinet, R.P.; Vidgen, E.; Jenkins, D.J.A. Effect of non-oil-seed pulses on glycaemic control: A systematic review and meta-analysis of randomised controlled experimental trials in people with and without diabetes. Diabetologia 2009, 52, 1479–1495. [Google Scholar] [CrossRef] [Green Version]
- Jayalath, V.H.; de Souza, R.J.; Sievenpiper, J.L.; Ha, V.; Chiavaroli, L.; Mirrahimi, A.; di Buono, M.; Bernstein, A.M.; Leiter, L.A.; Kris-Etherton, P.M.; et al. Effect of dietary pulses on blood pressure: A systematic review and meta-analysis of controlled feeding trials. Am. J. Hypertens. 2014, 27, 56–64. [Google Scholar] [CrossRef]
- Li, S.S.; Kendall, C.W.; Souza, R.J.; Jayalath, V.H.; Cozma, A.I.; Ha, V.; Mirrahimi, A.; Chiavaroli, L.; Augustin, L.S.; Mejia, S.B. Dietary pulses, satiety and food intake: A systematic review and meta—Analysis of acute feeding trials. Obesity 2014, 22, 1773–1780. [Google Scholar] [CrossRef]
- Abeysekara, S.; Chilibeck, P.D.; Vatanparast, H.; Zello, G.A. A pulse-based diet is effective for reducing total and LDL-cholesterol in older adults. Br. J. Nutr. 2012, 108, S103–S110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, T.; Zello, G.A.; Chilibeck, P.D.; Vandenberg, A. Perceived benefits and barriers surrounding lentil consumption in families with young children. Can. J. Diet. Pract. Res. 2015, 76, 3–8. [Google Scholar] [CrossRef] [PubMed]
- McBreairty, L.E.; Chilibeck, P.D.; Chizen, D.R.; Pierson, R.A.; Tumback, L.; Sherar, L.B.; Zello, G.A. The role of a pulse-based diet on infertility measures and metabolic syndrome risk: Protocol of a randomized clinical trial in women with polycystic ovary syndrome. BMC Nutr. 2017, 3, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. Ann. Int. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Schulz, K.F.; Altman, D.G. The CONSORT statement: Revised recommendations for improving the quality of reports of parallel-group randomised trials. Lancet 2001, 357, 1191–1194. [Google Scholar] [CrossRef] [Green Version]
- Azziz, R.; Carmina, E.; Dewailly, D.; Diamanti-Kandarakis, E.; Escobar-Morreale, H.F.; Futterweit, W.; Janssen, O.E.; Legro, R.S.; Norman, R.J.; Taylor, A.E.; et al. Criteria for defining polycystic ovary syndrome as a predominantly hyperandrogenic syndrome: An Androgen Excess Society guideline. J. Clin. Endocrinol. Metab. 2006, 91, 4237–4245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewailly, D.; Lujan, M.E.; Carmina, E.; Cedars, M.I.; Laven, J.; Norman, R.J.; Escobar-Morreale, H.F. Definition and significance of polycystic ovarian morphology: A task force report from the Androgen Excess and Polycystic Ovary Syndrome Society. Hum. Reprod. Update 2014, 20, 334–352. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, M.; McBreairty, L.E.; Zello, G.A.; Pierson, R.A.; Gordon, J.J.; Serrao, S.B.; Chilibeck, P.D.; Chizen, D.R. A pulse-based diet and the Therapeutic Lifestyle Changes diet in combination with health counseling and exercise improve health-related quality of life in women with polycystic ovary syndrome: Secondary analysis of a randomized controlled trial. J. Psychosom. Obstet. Gynaecol. 2019, 41, 144–153. [Google Scholar] [CrossRef]
- Schäfer, G.; Schenk, U.; Ritzel, U.; Ramadori, G.; Leonhardt, U. Comparison of the effects of dried peas with those of potatoes in mixed meals on postprandial glucose and insulin concentrations in patients with type 2 diabetes. Am. J. Clin. Nutr. 2003, 78, 99–103. [Google Scholar] [CrossRef] [Green Version]
- Shutler, S.M.; Bircher, G.M.; Tredger, J.A.; Morgan, L.M.; Walker, A.F.; Low, A.G. The effect of daily baked bean (Phaseolus vulgaris) consumption on the plasma lipid levels of young, normo-cholesterolaemic men. Br. J. Nutr. 1989, 61, 257–265. [Google Scholar] [CrossRef]
- Health Canada, Eating Well with Canada’s Food Guide. Available online: http://www.hc-sc.gc.ca/fn-an/alt_formats/hpfb-dgpsa/pdf/food-guide-aliment/print_eatwell_bienmang-eng.pdf (accessed on 20 May 2016).
- Hernandez-Rodas, M.C.; Valenzuela, R.; Videla, L.A. Relevant aspects of nutritional and dietary interventions in non-alcoholic fatty liver disease. Int. J. Mol. Sci. 2015, 16, 25168–25198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutler, D.A.; Pride, S.M.; Cheung, A.P. Low intakes of dietary fiber and magnesium are associated with insulin resistance and hyperandrogenism in polycystic ovary syndrome: A cohort study. Food Sci. Nutr. 2019, 7, 1426–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babapour, M.; Mohammadi, H.; Kazemi, M.; Hadi, A.; Rezazadegan, M.; Askari, G. Associations between serum magnesium concentrations and polycystic ovary syndrome status: A systematic review and meta-analysis. Biol. Trace Elem. Res. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, M.; Jarrett, B.; Brink, H.V.; Lin, A.; Hoeger, K.; Spandorfer, S.; Lujan, M. Associations between diet quality and ovarian dysmorphology in premenopausal women are mediated by obesity and metabolic aberrations. In Proceedings of the American Society for Nutrition, Baltimore, MD, USA, 8–11 June 2019. [Google Scholar] [CrossRef] [Green Version]
- Kazemi, M.; Jarrett, B.Y.; Brink, H.V.; Lin, A.W.; Hoeger, K.M.; Spandorfer, S.D.; Lujan, M.E. Obesity, insulin resistance, and hyperandrogenism mediate the link between poor diet quality and ovarian dysmorphology in reproductive-aged women. Nutrients 2020, 12, 1953. [Google Scholar] [CrossRef] [PubMed]
- Mudryj, A.N.; Yu, N.; Aukema, H.M. Nutritional and health benefits of pulses. Appl. Physiol. Nutr. Metab. 2014, 39, 1197–1204. [Google Scholar] [CrossRef]
- Kwik, J. Traditional food knowledge: A case study of an immigrant Canadian “Foodscape”. Environments 2008, 36, 59–74. [Google Scholar]
- Winham, D.M.; Davitt, E.D.; Heer, M.M.; Shelley, M.C. Pulse knowledge, attitudes, practices, and cooking experience of Midwestern US university students. Nutrients 2020, 12, 3499. [Google Scholar] [CrossRef]
- Mudryj, A.N.; Yu, N.; Hartman, T.J.; Mitchell, D.C.; Lawrence, F.R.; Aukema, H.M. Pulse consumption in Canadian adults influences nutrient intakes. Br. J. Nutr. 2012, 108, S27–S36. [Google Scholar] [CrossRef] [Green Version]
- Health Canada. Canada’s Food Guide; Health Canada: Ottawa, ON, Canada, 2019; Available online: https://food-guide.canada.ca/en/ (accessed on 28 December 2020).
- Dargie, F.; Henry, C.J.; Hailemariam, H.; Regassa, N. A peer-led pulse-based nutrition education intervention improved school-aged children ‘s knowledge, attitude, practice (KAP) and nutritional status in southern Ethiopia. J. Food. Res. 2018, 7. [Google Scholar] [CrossRef] [Green Version]
- Yetnayet, M.; Henry, C.; Berhanu, G.; Whiting, S.; Regassa, N. Nutrition education promoted consumption of pulse based foods among rural women of reproductive age in Sidama Zone, Southern Ethiopia. Afr. J. Food Agric. Nutr. Dev. 2017, 17, 12377–12395. [Google Scholar]
- Ersino, G.; Henry, C.J.; Zello, G.A. A nutrition education intervention affects the diet-health related practices and nutritional status of mothers and children in a pulse-growing community in Halaba, south Ethiopia. FASEB J. 2017, 31, 786.39. [Google Scholar] [CrossRef]
- Teshome, G.B.; Whiting, S.; Green, T.; Mulualem, D.; Henry, C. Scaled-up nutrition education on pulse-cereal complementary food in Ethiopia: A cluster-randomized trial. BMC Public Health 2020, 20, 1437. [Google Scholar] [CrossRef] [PubMed]
- Marsh, K.A.; Steinbeck, K.S.; Atkinson, F.S.; Petocz, P.; Brand-Miller, J.C. Effect of a low glycemic index compared with a conventional healthy diet on polycystic ovary syndrome. Am. J. Clin. Nutr. 2010, 92, 83–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chilibeck, P.D.; Kazemi, M.; McBreairty, L.E.; Zello, G.A. Chapter 67: Lifestyle Interventions for Sarcopenic Obesity in Polycystic Ovary Syndrome. In Obesity and Diabetes: Scientific Advances and Best Practice, 2nd ed.; Springer Nature Switzerland AG: Cham, Switzerland, 2020; pp. 907–920. [Google Scholar] [CrossRef]
- Quinlivan, J.A.; McGowan, L. Why nutrition should be the first prescription. J. Psychosom. Obstet. Gynaecol. 2018, 39, 247. [Google Scholar] [CrossRef] [Green Version]
- Royall, D. Modifying the food environment. Can. J. Diet. Pract. Res. 2020, 81. [Google Scholar] [CrossRef]
- Thompson, F.E.; Kirkpatrick, S.I.; Subar, A.F.; Reedy, J.; Schap, T.E.; Wilson, M.M.; Krebs-Smith, S.M. The national cancer institute’s dietary assessment primer: A resource for diet research. J. Acad. Nutr. Diet. 2015, 115, 1986–1995. [Google Scholar] [CrossRef] [Green Version]
- McCarney, R.; Warner, J.; Iliffe, S.; van Haselen, R.; Griffin, M.; Fisher, P. The Hawthorne Effect: A randomised, controlled trial. BMC Med. Res. Methodol. 2007, 7, 30. [Google Scholar] [CrossRef] [Green Version]
- Hoeger, K.M.; Kochman, L.; Wixom, N.; Craig, K.; Miller, R.K.; Guzick, D.S. A randomized, 48-week, placebo-controlled trial of intensive lifestyle modification and/or metformin therapy in overweight women with polycystic ovary syndrome: A pilot study. Fertil. Steril. 2004, 82, 421–429. [Google Scholar] [CrossRef]
- Turner-McGrievy, G.; Davidson, C.R.; Billings, D.L. Dietary intake, eating behaviors, and quality of life in women with polycystic ovary syndrome who are trying to conceive. Hum. Fertil. 2015, 18, 16–21. [Google Scholar] [CrossRef]
- Rao, M.; Broughton, K.S.; LeMieux, M.J. Cross-sectional Study on the Knowledge and Prevalence of PCOS at a Multiethnic University. Prog. Prev. Med. 2020, 5, e0028. [Google Scholar] [CrossRef]
- Inglis, V.; Ball, K.; Crawford, D. Why do women of low socioeconomic status have poorer dietary behaviours than women of higher socioeconomic status? A qualitative exploration. Appetite 2005, 45, 334–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekonnen, T.; Havdal, H.H.; Lien, N.; O’Halloran, S.A.; Arah, O.A.; Papadopoulou, E.; Gebremariam, M.K. Mediators of socioeconomic inequalities in dietary behaviours among youth: A systematic review. Obes. Rev. 2020, 21, e13016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soucie, K.; Samardzic, T.; Schramer, K.; Ly, C.; Katzman, R. The diagnostic experiences of women with polycystic ovary syndrome (PCOS) in Ontario, Canada. Qual. Health Res. 2020. [Google Scholar] [CrossRef]


{kind=link}
| Measure (Measurement Unit) | Pulse-Based Diet Group | TLC Diet Group |
|---|---|---|
| Age (year) | 26.9 ± 4.5 | 26.6 ± 5.0 |
| Metformin Tx (n (yes%)) | 11 (36.7) | 13 (41.9) |
| BMI (kg/m2) | 32.5 ± 8.4 | 34.0 ± 9.0 |
| PCOS diagnostic measures | ||
| TT (nmol/L) | 1.8 ± 0.7 | 1.7 ± 0.9 |
| FNPO (2–9 mm) | 46 ± 18 | 48 ± 16 |
| OV (mL) | 10.9 ± 5.5 | 12.2 ± 5.6 |
| Menstrual cycle length (day) | 98 ± 58 | 113 ± 70 |
| Presence of hirsutism (n (yes%)) | 22 (73.3) | 20 (64.5) |
| Question | Pulse-Based Diet Group n (%) | TLC Diet Group n (%) | p-Value a | ||||
|---|---|---|---|---|---|---|---|
| Baseline | Post-Intervention | Baseline | Post-Intervention | Time | Group | Group × Time | |
| According to Canada’s Food Guide, pulses are an example of a food in the | |||||||
| Vegetable and Fruit Group | 2 (6.5) | 0 | 5 (16.1) | 1 (3.2) | <0.05 | <0.05 | 0.05 |
| Grain Products Group | 7 (22.6) | 1 (3.2) | 6 (19.4) | 8 (25.8) | |||
| Milk and Alternatives Group | 1 (3.2) | 0 | 0 | 1 (3.2) | |||
| Meat and Alternatives Group b | 21 (67.7) | 30 (96.8) | 20 (64.5) | 21 (67.7) | |||
| Eating a proper diet will help to reduce your risk of certain types of diseases. | |||||||
| True b | 30 (100) | 30 (100) | 31 (100) | 31 (100) | - | - | - |
| False | 0 | 0 | 0 | 0 | |||
| One serving of cooked pulses, according to Canada’s Food Guide, equals | |||||||
| ¼ cup (60 mL) | 1 (3.3) | 1 (3.2) | 6 (19.4) | 2 (6.5) | <0.05 | 0.22 | 0.61 |
| ½ cup (125 mL) | 21 (70.0) | 13 (43.3) | 19 (61.3) | 19 (61.3) | |||
| ¾ cup (175 mL) b | 4 (13.3) | 11 (36.7) | 3 (9.7) | 6 (19.3) | |||
| 1 cup (250 mL) | 0 | 5 (16.7) | 3 (9.7) | 4 (12.9) | |||
| Pulses are a good source of protein. | |||||||
| True b | 30 (100) | 30 (100) | 31 (100) | 28 (93.5) | 0.94 | 0.93 | 0.95 |
| False | 0 | 0 | 0 | 2 (6.5) | |||
| Pulses are a good source of fibre. | |||||||
| True b | 28 (93.3) | 30 (100) | 31 (100) | 28 (93.5) | 0.97 | 0.45 | <0.05 |
| False | 2 (6.7) | 0 | 0 | 2 (6.5) | |||
| Pulses are a poor source of iron. | |||||||
| True | 26 (86.7) | 23 (76.7) | 26 (83.9) | 24 (77.4) | 0.35 | 0.67 | 0.60 |
| False b | 4 (13.3) | 7 (23.3) | 5 (16.1) | 7 (22.6) | |||
| Pulses have too much saturated fat. | |||||||
| True | 1 (2.2) | 2 (6.5) | 0 | 0 | 0.31 | 0.17 | 0.31 |
| False b | 30 (97.8) | 29 (93.5) | 31 (100) | 31 (100) | |||
| Which of the following does not belong in the Meat and Alternatives group in Canada’s Food Guide? | |||||||
| Eggs | 1 (3.3) | 1 (3.3) | 1 (3.2) | 2 (6.5) | 0.93 | 0.27 | <0.05 |
| Kidney Beans | 5 (16.7) | 1 (3.3) | 2 (6.5) | 3 (9.7) | |||
| Tofu | 3 (3.3) | 0 | 3 (9.7) | 1 (3.2) | |||
| Peanut Butter | 3 (3.3) | 3 (10.0) | 5 (16.1) | 5 (16.1) | |||
| Cottage Cheese b | 18 (60.0) | 25 (83.3) | 20 (64.5) | 20 (64.5) | |||
| Pulses are grown in Saskatchewan. | |||||||
| True b | 25 (83.3) | 29 (96.7) | 25 (80.6) | 27 (87.1) | 0.05 | 0.38 | 0.50 |
| False | 5 (16.7) | 1 (3.3) | 6 (19.4) | 4 (12.9) | |||
| Where do you access information on healthy eating? (Select all that apply) | |||||||
| Internet | 28 (93.3) | 29 (96.7) | 28 (90.3) | 29 (93.5) | 0.94 | 0.92 | 0.94 |
| Magazines | 16 (53.3) | 16 (53.3) | 16 (51.6) | 17 (54.8) | 0.93 | 0.91 | 0.92 |
| Cookbooks | 11 (36.7) | 16 (53.3) | 16 (51.6) | 15 (48.4) | 0.34 | 0.45 | 0.06 |
| Chefs | 0 | 1 (3.3) | 1 (3.2) | 1 (3.2) | 0.69 | 0.73 | 0.77 |
| Library | 12 (40.0) | 12 (40.0) | 10 (32.3) | 11 (35.5) | 0.34 | 0.52 | 0.36 |
| Canada’s Food Guide | 20 (66.7) | 28 (93.3) | 20 (64.5) | 22 (71.0) | 0.06 | 0.33 | <0.05 |
| Newspaper | 5 (16.7) | 6 (20.0) | 6 (19.4) | 6 (19.4) | 0.46 | 0.45 | 0.44 |
| Food labels | 1 (3.3) | 8 (26.7) | 1 (3.2) | 4 (12.9) | <0.05 | 0.08 | 0.05 |
| Health professional | 6 (20.0) | 18 (60.0) | 3 (9.7) | 11 (35.5) | <0.05 | <0.05 | <0.05 |
| Social networking sites | 12 (40.0) | 24 (80.0) | 15 (48.4) | 23 (74.2) | <0.05 | <0.05 | <0.05 |
| Television | 3 (10.0) | 3 (10.0) | 4 (12.9) | 3 (9.7) | 0.56 | 0.87 | 0.58 |
| Friends, family, colleagues | 13 (43.3) | 12 (40.0) | 19 (61.3) | 16 (51.6) | 0.07 | 0.12 | 0.10 |
| Grocery store | 16 (53.3) | 17 (56.7) | 18 (58.1) | 19 (61.3) | 0.33 | 0.76 | 0.44 |
| Radio | 10 (33.3) | 9 (30.0) | 6 (19.4) | 6 (19.4) | 0.45 | 0.65 | 0.53 |
| Other | 1 (3.3) | 1 (3.3) | 3 (9.7) | 3 (9.7) | 0.97 | 0.99 | 0.99 |
| Perceived Barrier | Total Score (Frequency of Response × Value b) | Rank |
|---|---|---|
| No/low consumers in pulse-based diet group at baseline (n = 7) | ||
| I do not know how to cook pulses. | 12 | 1 |
| I do not know where to find pulses. | 7 | 2 |
| I believe pulses do not taste good. | 5 | 3 |
| No/low consumers in pulse-based diet group post-intervention (n = 3) | ||
| I do not know how to cook pulses. | 7 | 1 |
| I believe pulses take a long time to cook. | 4 | 2 |
| I believe my family would not like pulses. | 3 | 3 |
| No/low consumers in TLC diet group at baseline (n = 9) | ||
| I do not know how to cook pulses. | 22 | 1 |
| I believe pulses do not taste good. | 9 | 2 |
| I do not know where to find pulses. | 8 | 3 |
| No/low consumers in TLC diet group post intervention (n = 10) | ||
| I do not know how to cook pulses. | 27 | 1 |
| I do not know where to find pulses. | 8 | 2 |
| I believe my family would not like pulses. | 7 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kazemi, M.; McBreairty, L.E.; Chilibeck, P.D.; Pierson, R.A.; Chizen, D.R.; Zello, G.A. Knowledge, Attitudes, and Barriers towards Dietary Pulse Consumption in Women with Polycystic Ovary Syndrome Participating in a Multi-Disciplinary Lifestyle Intervention to Improve Women’s Health. Sexes 2021, 2, 88-103. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2010008
Kazemi M, McBreairty LE, Chilibeck PD, Pierson RA, Chizen DR, Zello GA. Knowledge, Attitudes, and Barriers towards Dietary Pulse Consumption in Women with Polycystic Ovary Syndrome Participating in a Multi-Disciplinary Lifestyle Intervention to Improve Women’s Health. Sexes. 2021; 2(1):88-103. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2010008
Chicago/Turabian StyleKazemi, Maryam, Laura E. McBreairty, Philip D. Chilibeck, Roger A. Pierson, Donna R. Chizen, and Gordon A. Zello. 2021. "Knowledge, Attitudes, and Barriers towards Dietary Pulse Consumption in Women with Polycystic Ovary Syndrome Participating in a Multi-Disciplinary Lifestyle Intervention to Improve Women’s Health" Sexes 2, no. 1: 88-103. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2010008