
The Perinatal Journey of a Refugee Woman in Greece: A Qualitative Study in the Context of the ORAMMA Project to Elucidate Current Challenges and Future Perspectives



Abstract
:1. Introduction
2. Materials and Methods
2.1. Review of the Literature
2.2. Qualitative Research with Representatives of Key Stakeholder Groups
2.3. Procedures
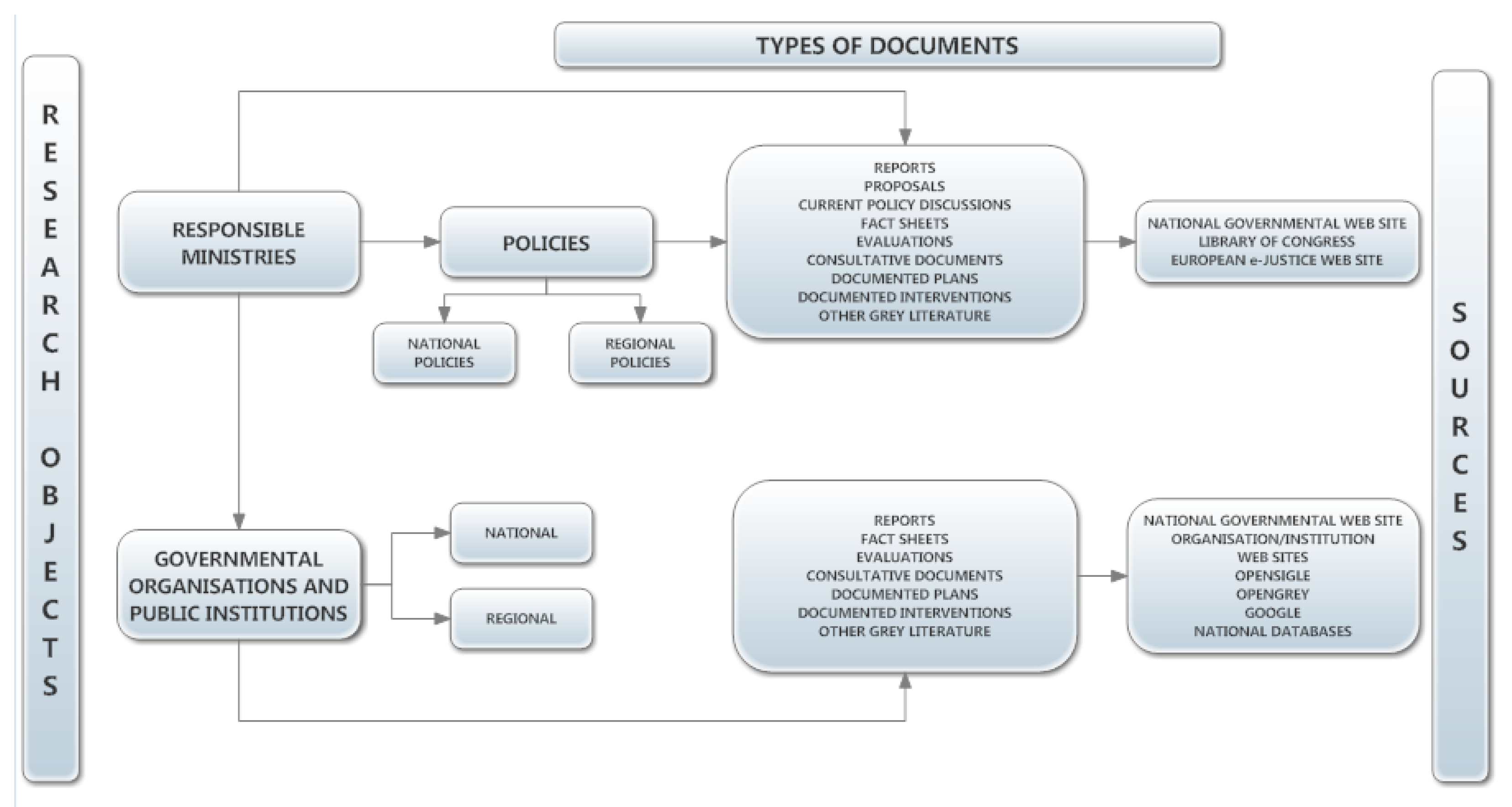
2.3.1. Desk Research
2.3.2. Qualitative Research
2.4. Data Analysis
3. Results
3.1. Description of Literature
3.2. Focus Group Participant Profile
3.3. Main Findings
3.3.1. Barriers Related to Service Users
- (a)
- Language as a barrier in access to perinatal care: Many women experience difficult family situations such as domestic violence and controlling relationships which are not easy to share with cultural mediators and/or interpreters. This crucial factor excludes women from seeking and/or accessing the necessary care, thus, affecting both their own and the fetus’s health, and maternal/newborn outcomes. Furthermore, health service providers rely excessively on “informal” interpretation coming from family environment and friends, which compromises both the quality of interpretation and confidentiality. Indeed, informal interpreters’ lack of knowledge of medical terminology may result in women being subjected to medical interventions they did not consent to, without any of the procedures being explained or understood. Medical interpreters and trained maternity peer supporters need to be available for women who are at the perinatal phase. It is also recommended that culturally appropriate educational materials should be distributed to pregnant and childbearing refugees, including information on key symptoms and health complications. Furthermore, women may be less likely to be willing to disclose information that may not be treated confidentially, either because of a relationship of a personal nature with the informal interpreter and/or because of the lack of training in terms of Code of Conduct for interpreters to informal interpreters from the wider ethnic and cultural community these women belong in.
- (b)
- Cultural barriers in woman-healthcare professional (e.g., patient-doctor) communication: Communication restrictions worsen due to limitations of understanding different traditions related to pregnancy and childbirth. The provider’s gender can be a barrier in help-seeking behaviors for those women whose tradition or religion does not allow interaction with men. Culturally appropriate service, with high cultural understanding and informed consent practices, can encourage women to utilize the available maternity care.
- (c)
- Financial incapacity, irregularity, and low sense of safety preventing safe perinatal practices: The illegal employment status that many refugee women have, results on relying on employers’ intention to afford them maternity leave to be able to access the care they need. Newly arrived refugees are commonly unemployed or in best cases are low-paid or have occasional employment. Insecurity, as well as ignorance of labor and residency rights, is a major barrier for women, who frequently ignore symptoms of illness or other health care needs or postpone seeking care. Women are unable to attend appointments or meet their needs due to the legal status and the associated restrictions in their rights and entitlements to welfare, low-paid work, and controlling behaviors within the family culture. Refugee women, regardless of their migrant status or regularity, should be informed about their rights in the country of destination prior to pregnancy, including their right to a safe perinatal journey.
- (d)
- General disappointment with the health care system: Refugee women frequently arrive in the country of destination with unrealistic expectations of its people and services, either because they were intentionally misinformed by those who arranged their transfer or because of excessive optimism combined with lack of understanding of the policies and capacity of the country of destination. The difficulty of obtaining legal status confirming they are entitled to receive care and challenges in accessing services turns enthusiasm into disappointment, which frequently results in emotional reactions such as withdrawal from trying to negotiate their rights. To prevent emotional burnout and the psychological consequences of distress and withdrawal, refugee women should be given culturally appropriate assistance in navigating to local services from the moment they arrive in their host country. Trying to ensure that refugee women understand how to navigate the healthcare system can help to reduce delays in seeking health care and receiving adequate treatment.
- (e)
- Racism victimization creates a generalized resistance and suspicion of system requirements: Refugee women are frequently subjected to racism and are sometimes humiliated by the local population. This frequently makes them feel unwelcome, preventing them from investing in the health care system and developing trusting relationships with health care providers. Mutual trust is essential for ensuring quality of care between refugee women and healthcare providers. To ensure that refugees trust the local setting, its people, and services, action to combat racism and xenophobia in local society must be enhanced.
- (f)
- High psychological distress because of migration conditions, preventing effective self-care, self-hygiene, and help-seeking: Refugee women are frequently faced with numerous challenges, which lead to high levels of psychological distress. A history of torture which entailed their urgent transfer, sex and gender-based violence due to cultural proneness, female genital mutilation (FGM), unemployment and racism, and the stress of obtaining legal status in the country of destination are among the most common factors affecting refugee mental health. Perinatal stages are also related to emotional stress and fragility, highlighting the need for specialized care. Lengthy social and psychological support should be provided to them beginning with their arrival in the country in order to prevent mental health problems.
3.3.2. Barriers Related to Service Providers
- (a)
- Low capacity to meet the health care needs of migrants in a culturally appropriate manner: Cross-cultural training and resources for health care providers appear to be missing to aid migrant women in a culturally appropriate way. In the busy primary health care environment, the lack of cultural mediators and interpreters appears to be a serious shortcoming that requires additional attention, particularly when paired with staff and resource shortages. The absence of a social and family network to aid women in adhering to therapy and care pathways is a significant shortcoming that creates many difficulties for health care providers who must work collaboratively with important others to treat serious medical issues in migrant women. Appropriate cross-cultural communication is hard to accomplish in a system that lacks resources to support the development of a culturally competent workforce. Furthermore, a lack of cross-cultural training allows for stereotyped thinking and does not promote trusting and caring relationships among health care providers and migrant women.
- (b)
- Doctor-centered and patriarchal systems of care with minimal investment in the interdisciplinary and interprofessional training of the care team: The healthcare system appears to be overly reliant on the medical doctor rather than the healthcare team, which makes it less flexible, particularly during a crisis. The healthcare team must be reinforced, and patient care must be re-distributed with tasks allocated to all team members in a balanced manner. Specific medical procedures may need to be delegated to other healthcare professionals to save time and improve quality (e.g., prescription by a midwife or nurse). Social workers and mental health professionals must be part of the team to address the various psychosocial problems that co-exist or arise as a result of the medical problem and other circumstances.
- (c)
- Lack of service integration and continuity of care: Despite migrant women’s multimorbidity, medical and psychosocial services in the community are not horizontally linked, making it more difficult for them to seek help. Bio-psychosocial assessment and treatment proves difficult, despite the fact that it is required to meet the health care needs of women holistically. In order to enhance continuity of care, particularly in this difficult-to-reach population, the lack of horizontal integration of services must be resolved through organizational changes in the PHC setting.
- (d)
- Low engagement during crisis—healthcare professional’s burnout: Many changes have occurred as a result of the financial crisis, including service mergers or closures, salary cuts, staff and equipment shortages, and this has increased the burden on health care providers. There appear to be deficient mechanisms in place to address this enormous psychological and physical burden and prevent exhaustion and even burnout, which has a significant impact on care quality. Furthermore, training and information to allow the healthcare professional to identify signs of exhaustion early and manage stress, workload and to seek care too, is urgently needed.
4. Discussion
4.1. Implications for Research and Practice
4.2. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| UNHCR | United Nations High Commissioner for Refugees |
| SDGs | Sustainable Development Goals |
| UHC | Universal Health Coverage |
| MIPEX | Migrant Integration Policy Index |
| ANC | Antenatal Care |
| PNC | Postnatal Care |
| NGOs | Non-governmental organizations |
| MdM | Médecins du Monde |
| FGM | Female genital mutilation |
| GPs | General practitioners |
| WHO | World Health Organization |
Appendix A

{kind=link}
| No | Name of Organization | Name and Position of Contact Person | Contact Info | Website | Mission |
|---|---|---|---|---|---|
| 1 | |||||
| 2 | |||||
| 3 | |||||
| 4 | |||||
| 5 | |||||
| 6 | |||||
| 7 | |||||
| 8 |
| (1) | (2) | (3) | (4) | (5) | (6) | (7) |
|---|---|---|---|---|---|---|
| 1 | ||||||
| 2 | ||||||
| 3 | ||||||
| 4 | ||||||
| 5 | ||||||
| 6 | ||||||
| 7 | ||||||
| 8 |
References
- WHO. How Health Systems Can Address Health Inequities Linked to Migration and Ethnicity; WHO Regional Office for Europe: Copenhagen, Denmark, 2010; Available online: http://www.euro.who.int/__data/assets/pdf_file/0005/127526/e94497.pdf (accessed on 20 January 2017).
- Baum, F.E.; Bégin, M.; Houweling, T.A.; Taylor, S. Changes not for the fainthearted: Reorienting health care systems toward health equity through action on the social determinants of health. Am. J. Public Health 2009, 99, 1967–1974. [Google Scholar] [CrossRef]
- Baum, F.; Legge, D.G.; Freeman, T.; Lawless, A.; LaBonte, R.; Jolley, G.M. The potential for multi-disciplinary primary health care services to take action on the social determinants of health: Actions and constraints. BMC Public Health 2013, 13, 460. [Google Scholar] [CrossRef] [Green Version]
- United Nations Refugee Agency; United Nations Population Fund; Women’s Refugee Commission. Initial Assessment Report: Protection Risks for Women and Girls in the European Refugee and Migrant Crisis—Greece and the Former Yugoslav Republic of Macedonia; UNHCR: Geneva, Switzerland; UNFPA: New York, NY, USA; Women’s Refugee Commission: Geneva, Switzerland, 2015; p. 6. Available online: http://eeca.unfpa.org/sites/default/files/pub-pdf/GBV-Assessment-Greece-Macedonia.pdf (accessed on 29 April 2017).
- European Parliament. Female Refugees and Asylum Seekers: The Issue of Integration; DG For Internal Policies; European Parliament: Strasbourg, France, 2016; Available online: http://www.europarl.europa.eu/supporting-analyses (accessed on 5 October 2018).
- Florian, L.; Young, K.; Rouse, M. Preparing teachers for inclusive and diverse educational environments: Studying curricular reform in an initial teacher education course. Int. J. Incl. Educ. 2010, 14, 709–722. [Google Scholar] [CrossRef]
- UNHCR. Operational Portal, Refugee Situations, Mediterranean Situations, Greece. 2020. Available online: https://data2.unhcr.org/en/situations/mediterranean/location/5179 (accessed on 10 March 2020).
- UNHCR. Nationality of Arrivals to Greece, Italy, and Spain. January–December 2015. 2016. Available online: https://data2.unhcr.org/en/documents/download/46811 (accessed on 3 June 2018).
- Malakasis, C.H. Migrant Maternity Care in Athens, Greece, 2016–2017; A Policy Report; Cadmus, European University Institute Research Repository: Fiesole, Italy, 2020. [Google Scholar]
- Shortall, C.K.; Glazik, R.; Sornum, A.; Pritchard, C. On the ferries: The unmet health care needs of transiting refugees in Greece. Int. Health 2017, 9, 272–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, H.M.; Wallis, N. Maternity care for refugees living in Greek refugee camps: What are the challenges to provision? Birth 2020, 48, 114–121. [Google Scholar] [CrossRef]
- Gibson-Helm, M.; Teede, H.; Block, A.; Knight, M.; East, C.; Wallace, E.M.; Boyle, J. Maternal health and pregnancy outcomes among women of refugee background from African countries: A retrospective, observational study in Australia. BMC Pregnancy Childbirth 2014, 14, 392. [Google Scholar] [CrossRef] [PubMed]
- WHO. Improving the Health Care of Pregnant Refugee and Migrant Women and Newborn Children; Technical Guidance; WHO Regional Office for Europe: Copenhagen, Denmark, 2018; Volume 52. [Google Scholar]
- Kentikelenis, A.; Papanicolas, A. Economic crisis, austerity and the Greek public health system. Euro J. Public Health 2012, 22, 4–5. [Google Scholar] [CrossRef] [Green Version]
- Lionis, C.; Symvoulakis, E.K.; Markaki, A.; Vardavas, C.; Papadakaki, M.; Daniilidou, N.; Souliotis, K.; Kyriopoulos, I. Integrated primary health care in Greece, a missing issue in the current health policy agenda: A systematic review. Int. J. Integr. Care 2009, 9, e88. [Google Scholar] [CrossRef]
- Niakas, D. Greek economic crisis and health care reforms: Correcting the wrong prescription. Int. J. Health Serv. 2013, 43, 597–602. [Google Scholar] [CrossRef]
- Papadakaki, M.; Ratsika, N.; Pelekidou, L.; Halbmayr, B.; Kouta, C.; Lainpelto, K.; Solinc, M.; Apostolidou, Z.; Christodoulou, J.; Kohont, A.; et al. Migrant domestic workers’ experiences of sexual harassment: A qualitative study in four EU countries. Sexes 2021, 2, 272–292. [Google Scholar] [CrossRef]
- Kouta, C.; Pithara, C.; Apostolidou, Z.; Zobnina, A.; Christodoulou, J.; Papadakaki, M.; Chliaoutakis, J. A qualitative study of female migrant domestic workers’ experiences of and responses to work-based sexual violence in Cyprus. Sexes 2021, 2, 315–330. [Google Scholar] [CrossRef]
- Papadakaki, Μ.; Chliaoutakis, J. Sexual Harassment Against Female Migrant Domestic Workers; WHO Public Health Aspects of Migration in Europe (PHAME Newsletter); WHO Regional Office for Europe: Copenhagen, Denmark, 2016; pp. 10–11. Available online: http://www.euro.who.int/__data/assets/pdf_file/0020/321806/PHAME-Newsletter-issue-10-en.pdf (accessed on 30 September 2021).
- Mechili, E.-A.; Angelaki, A.; Petelos, E.; Sifaki-Pistolla, D.; Chatzea, V.-E.; Dowrick, C.; Hoffmann, K.; Jirovsky, E.; Pavlic, D.R.; Dückers, M.; et al. Compassionate care provision: An immense need during the refugee crisis: Lessons learned from a European capacity-building project. J. Compassionate Health Care 2018, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- Fair, F.; Soltani, H.; Raben, L.; van Streun, Y.; Sioti, E.; Papadakaki, M.; Burke, C.; Watson, H.; Jokinen, M.; Shaw, E.; et al. Midwives’ experiences of cultural competency training and providing perinatal care for migrant women a mixed methods study: Operational Refugee and Migrant Maternal Approach (ORAMMA) project. BMC Pregnancy Childbirth 2021, 21, 340. [Google Scholar] [CrossRef] [PubMed]
- Lionis, C.; Papadakaki, M.; Saridaki, A.; Dowrick, C.; O’Donnell, C.; Mair, F.S.; Muijsenbergh, M.V.D.; Burns, N.; de Brún, T.; de Brún, M.O.; et al. Engaging migrants and other stakeholders to improve communication in cross-cultural consultation in primary care: A theoretically informed participatory study. BMJ Open 2016, 6, e010822. [Google Scholar] [CrossRef] [Green Version]
- Vazquez, M.L.; Vargas, I.; Jaramillo, D.L.; Porthe, V.; Lopez-Fernandez, L.A.; Vargas, H.; Bosch, L.; Hernandez, S.S.; Azarola, A.R. Was access to health care easy for immigrants in Spain? The perspectives of health personnel in Catalonia and Andalusia. Health Policy 2016, 120, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Lyberg, A.; Viken, B.; Haruna, M.; Severinsson, E. Diversity and challenges in the management of maternity care for migrant women. J. Nurs. Manag. 2011, 20, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Otero-Garcia, L.; Goicolea, I.; Sánchez, M.G.; Barbero, B.S. Access to and use of sexual and reproductive health services provided by midwives among rural immigrant women in Spain: Midwives’ perspectives. Glob. Health Action 2013, 6, 22645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadakaki, M.; Petridou, E.; Petelos, E.; Germeni, E.; Kogevinas, M.; Lionis, C. Management of victimized patients in greek primary care settings: A pilot study. J. Fam. Violence 2014, 29, 371–379. [Google Scholar] [CrossRef]
- Iliadou, M.; Papadakaki, M.; Sioti, E.; Giaxi, P.; Leontitsi, E.; Petelos, E.; Van der Muijsenbergh, M.; Tziaferi, S.; Mastroyannakis, A.; Vivilaki, V.G. Addressing mental health issues among migrant and refugee pregnant women: A call for action. Eur. J. Midwifery 2019, 3, 9. [Google Scholar] [CrossRef]
- Degni, F.; Suominen, S.B.; Essén, B.; El Ansari, W.; Vehviläinen-Julkunen, K. Communication and cultural issues in providing reproductive health care to immigrant women: Health care providers’ experiences in meeting somali women living in Finland. J. Immigr. Minor. Health 2011, 14, 330–343. [Google Scholar] [CrossRef]
- Puthussery, S.; Twamley, K.; Harding, S.; Mirsky, J.; Baron, M.; Macfarlane, A. ‘They’re more like ordinary stroppy British women’: Attitudes and expectations of maternity care professionals to UK-born ethnic minority women. J. Health Serv. Res. Policy 2008, 13, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Lyons, S.M.; O’Keeffe, F.M.; Clarke, A.T.; Staines, A. Cultural diversity in the Dublin maternity services: The experience of maternity service providers when caring for ethnic minority women. Ethn. Health 2008, 13, 261–276. [Google Scholar] [CrossRef]
- Binder, P.; Borné, Y.; Johnsdotter, S.; Essén, B. Shared language is essential: Communication in a multiethnic obstetric care setting. J. Health Commun. 2012, 17, 1171–1186. [Google Scholar] [CrossRef]
- Tobin, C.L.; Murphy-Lawless, J. Irish midwives’ experiences of providing maternity care to non-Irish women seeking asylum. Int. J. Women’s Health 2014, 6, 159–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadakaki, M.; Lionis, C.; Saridaki, A.; Dowrick, C.; De Brún, T.; Brún, M.O.-D.; O’Donnell, C.; Burns, N.; Van Weel-Baumgarten, E.; Muijsenbergh, M.V.D.; et al. Exploring barriers to primary care for migrants in Greece in times of austerity: Perspectives of service providers. Eur. J. Gen. Pract. 2017, 23, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Kolak, M.; Jensen, C.; Johansson, M. Midwives’ experiences of providing contraception counselling to immigrant women. Sex. Reprod. Health 2017, 12, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Falla, A.M.; Veldhuijzen, I.K.; Ahmad, A.A.; Levi, M.; Richardus, J.H. Limited access to hepatitis B/C treatment among vulnerable risk populations: An expert survey in six European countries. Eur. J. Public Health 2016, 27, 302–306. [Google Scholar] [CrossRef] [Green Version]
- Robson, C. Real World Research; Blackwell: Oxford, UK, 2002. [Google Scholar]
- Bloor, M.; Frankland, J.; Thomas, M.; Robson, K. Focus Groups in Social Research; Sage: London, UK, 2001. [Google Scholar]

| Type of Documents | N of Docs |
|---|---|
| Scientific papers | 15 |
| Scientific review papers | 4 |
| Institution/special committee reports | 10 |
| Book chapters | 1 |
| Legislative documents | 3 |
| Newsletters/material | 2 |
| Master/PhD Theses | 2 |
| Previous EU-project reports | 3 |
| Organizations | N |
|---|---|
| Regional health care authorities | 1 |
| Local health care authorities (primary/secondary/tertiary health care) | 3 |
| Regional social care authorities | 1 |
| Local social care authorities/committees | 4 |
| Academic institutions (primary care professions) | 3 |
| Professional associations/societies of primary care professions | 4 |
| Local branches of international/national NGOs for health/social care of vulnerable groups | 3 |
| Local branches of international/national NGOs on migrant issues | 1 |
| Local branches of international/national human rights NGOs | 1 |
| Local interpreting and cultural mediation services | 3 |
| Local migrant communities | 2 |
| Barriers Related to Service Users | Selected Quotes |
|---|---|
| Language as a barrier in access to perinatal care | “I believe that emphasis should be placed on the interpretation process and the certification of interpreters. The process remains problematic as the selection of interpreters does not include medical knowledge and standards” (PHC society, FG2) “There were times when interpreters were adding their personal belief and experience instead of interpreting word-by-word what I was saying (i.e., “that is what the midwife said, but... when I was pregnant, I did this differently and I didn’t have any problems” (Midwife, FG1) “Very frequently you have to work with women who have very low educational level and this can cause communication issues” (NGO, FG2) |
| Cultural barriers in patient-doctor communication | “Women are afraid of male doctors so they do not go to the hospital even when they have serious problems” (PHC provider, FG2) “... These women are not comfortable to discuss female issues in front of men, which can result in missing important information” (Midwife, FG1) “Once, when I accompanied a pregnant woman to the hospital to assist in interpretation, she didn’t feel comfortable with me being present, because I was a man. I tried to facilitate her privacy… as I deeply understood her. You see…I was the only interpreter available” (Interpretation services, FG2). |
| Financial incapacity, irregularity and low sense of safety preventing safe perinatal practices | “Many times refugees are confronted with financial obstacles to obtain medical supplies or follow a dietary recommendation, which is required for prevention or treatment of their problems. This is usually because of financial hardship as well as because of cultural peculiarities in eating habits” (Midwife, FG1) “The subsidy we get from the refugee support program is very low and can’t cover the needs of a family. We need support to find jobs, have vocational training and gain normal lives in this country” (Migrant community, FG2) “You can’t advice women to follow a certain diet during maternity when they don’t have a regular income in the family. It’s all in theory and we need to have in mind the practical barriers.” (NGO, FG2) |
| General disappointment with the health care system | “The system is problematic. We got in huge trouble when we needed to apply for a Social Security Registration Number. Our municipal services had its own regulation and could not accept our application. I had to travel to a different municipality to complete this task” (Migrant community, FG2) “I am afraid that the awareness of professionals is still low. There are new laws that apply without prior training of front-line professionals and this makes things difficult for users. They are often disappointed when they attempt to seek for help and they reach a dead end” (NGO, FG2) |
| Racism victimization creates a generalized resistance and suspicion of system requirements | “They are severely traumatized and need time to trust people. Nevertheless, people are not always friendly towards them and this is sometimes evident among health care professionals as well” (Health authority, FG2) “When they realize that I speak their mother language, they feel safe and start asking me things… Sometimes they try to validate things they have been told earlier… sometimes testing me too” (Interpretation services, FG2) “There is great support for us… but still the full picture is not perfect. I am still a foreigner to them” (Migrant community, FG2) |
| High psychological distress preventing effective self-care, self-hygiene and help-seeking | “Refugee women function as post traumatic people and they might seem aggressive sometimes. We have to find female leaders in the community in order for them to help each other” (PHC society, FG2) “There are women raped by strangers or husbands. So many adverse events in a woman’s life!! What should I expect from this woman? To do what all the pregnant women do?” (Midwife, FG1) |
| Barriers Related to Service Providers | Selected Quotes |
| Low capacity to meet the health care needs of migrants in a culturally appropriate manner | “... There are specific conditions that are not yet easy to deal with even with an interpreter. For example, psychiatric conditions are not easy to discuss even with an interpreter.” (Health authority, FG2) “…the clinical setting doesn’t offer privacy and that makes women feel uncomfortable” (Midwife, FG1) “... No one is allowed to be with the woman in the room during labor. Women are very fragile at that moment and they need their own people. They don’t even understand the doctors’ language…” (Interpretation Service, FG2) |
| Doctor-centered system with minimal investment in the health care team | “There are still cases when clinicians deny offering help to refugees because they lack the appropriate interpretation services and language support” (Interpretation service, FG2) “Midwives are very emotional and the main problem is that we cannot help these women with the social determinants. It would be very helpful to have social services for helping them find a job, for helping their families and especially their children” (Midwife, FG1) “… sexual violence victims need attention and care from specialists which is not offered in the health care system” (NGO, FG2) |
| Lack of service integration and continuity of care | “The link between primary care facilities and hospitals is still lacking... we face difficulties in formal procedures” (PHC society, FG2) “We know that there are a number of socioeconomic and family matters to consider when helping a refugee woman during maternity, but it is often the case to need to refer women to different services to meet her needs…and then you can’t be sure whether she has visited these services because there is no connection between the different sectors to follow up on this case… in most cases the woman has been discouraged...” (Academic Institution, FG2) |
| Low engagement during crisis—service providers’ burn out | “Sometimes midwives feel like they are not doing a good job, because refugee women do not follow the advice given to them, but we need to understand that these people need time to adapt to our culture.” (Midwife, FG1) “It is worthy to offer assistance to a woman who suffered so much, but we are very few and unsupported. We need more support from the system. All those providers working with vulnerable populations like refugees or other traumatized individuals, spent a huge amount of effort to care for these people, help them feel safe and meet their needs. We sometimes disregard our own needs and get exhausted.” (NGO, FG2) “It is disappointing to know that the woman who just left will probably not return and will not seek further help, despite your enthusiasm to help her…” (PHC society, FG2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadakaki, M.; Iliadou, M.; Sioti, E.; Petelos, E.; Vivilaki, V. The Perinatal Journey of a Refugee Woman in Greece: A Qualitative Study in the Context of the ORAMMA Project to Elucidate Current Challenges and Future Perspectives. Sexes 2021, 2, 452-467. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2040036
Papadakaki M, Iliadou M, Sioti E, Petelos E, Vivilaki V. The Perinatal Journey of a Refugee Woman in Greece: A Qualitative Study in the Context of the ORAMMA Project to Elucidate Current Challenges and Future Perspectives. Sexes. 2021; 2(4):452-467. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2040036
Chicago/Turabian StylePapadakaki, Maria, Maria Iliadou, Eirini Sioti, Elena Petelos, and Victoria Vivilaki. 2021. "The Perinatal Journey of a Refugee Woman in Greece: A Qualitative Study in the Context of the ORAMMA Project to Elucidate Current Challenges and Future Perspectives" Sexes 2, no. 4: 452-467. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2040036