Prevalence and Determinants of Sinus Problems in Farm and Non-Farm Populations of Rural Saskatchewan, Canada

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Baseline Survey
2.2. Variables
2.2.1. Primary Outcome
2.2.2. Contextual Factors
2.2.3. Individual Factors
2.2.4. Covariates
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Environmental Factors
4.2. Lifestyle
4.3. Early Life Exposure
4.4. Occupational History and Exposures
4.5. Health Conditions
4.6. Family History
4.7. Other Risk Factors (Female Sex and Educational Status)
4.8. Limitation and Strengths of This Study
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wang, D.Y. Risk factors of allergic rhinitis: Genetic or environmental? Ther. Clin. Risk Manag. 2005, 1, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Dykewicz, M.S.; Hamilos, D.L. Rhinitis and sinusitis. J. Allergy Clin. Immunol. 2010, 125, S103–S115. [Google Scholar] [CrossRef] [PubMed]
- Slager, R.E.; Simpson, S.L.; LeVan, T.D.; Poole, J.A.; Sandler, D.P.; Hoppin, J.A. Rhinitis associated with pesticide use among private pesticide applicators in the agricultural health study. J. Toxicol. Environ. Health A 2010, 73, 1382–1393. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J.; Ekerljung, L.; Lötvall, J.; Pullerits, T.; Wennergren, G.; Rönmark, E.; Torén, K. Growing up on a farm leads to lifelong protection against allergic rhinitis. Allergy 2010, 65, 1397–1403. [Google Scholar] [CrossRef] [PubMed]
- Matheson, M.C.; Dharmage, S.C.; Abramson, M.J.; Walters, E.H.; Sunyer, J.; de Marco, R.; Leynaert, B.; Heinrich, J.; Jarvis, D.; Norbäck, D.; et al. Early-life risk factors and incidence of rhinitis: Results from the European Community Respiratory Health Study—An international population-based cohort study. J. Allergy Clin. Immunol. 2011, 128, 816–823. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, K.I.; McNally, J.D.; Massoud, E. The health and resource utilization of Canadians with chronic rhinosinusitis. Laryngoscope 2009, 119, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Poole, J.A. Farming-associated environmental exposures and effect on atopic diseases. Ann. Allergy Asthma Immunol. 2012, 109, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Sundaresan, A.S.; Hirsch, A.G.; Storm, M.; Tan, B.K.; Kennedy, T.L.; Greene, J.S.; Kern, R.C.; Schwartz, B.S. Occupational and environmental risk factors for chronic rhinosinusitis: A systematic review. Int. Forum Allergy Rhinol. 2015, 5, 996–1003. [Google Scholar] [CrossRef] [PubMed]
- Demos, K.; Sazakli, E.; Jelastopulu, E.; Charokopos, N.; Ellul, J.; Leotsinidis, M. Does farming have an effect on health status? A comparison study in West Greece. Int. J. Environ. Res. Public Health 2013, 10, 776–792. [Google Scholar] [CrossRef] [PubMed]
- Riedler, J.; Braun-Fahrlander, C.; Eder, W.; Schreuer, M.; Waser, M.; Maisch, S.; Carr, D.; Schierl, R.; Nowak, D.; von Mutius, E.; et al. Exposure to farming in early life and development of asthma and allergy: A cross-sectional survey. Lancet 2001, 358, 1129–1133. [Google Scholar] [CrossRef]
- Leynaert, B.; Neukirch, C.; Jarvis, D.; Chinn, S.; Burney, P.; Neukirch, F.; European Community Respiratory Health Survey. Does living on a farm during childhood protect against asthma, allergic rhinitis, and atopy in adulthood? Am. J. Respir. Crit. Care Med. 2001, 164, 1829–1834. [Google Scholar] [CrossRef] [PubMed]
- Braun-Fahrlander, C.; Riedler, J.; Herz, U.; Eder, W.; Waser, M.; Grize, L.; Maisch, S.; Carr, D.; Gerlach, F.; Bufe, A.; et al. Environmental exposure to endotoxin and its relation to asthma in school-age children. N. Engl. J. Med. 2002, 347, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Waser, M.; Michels, K.B.; Bieli, C.; Flöistrup, H.; Pershagen, G.; von Mutius, E.; Ege, M.; Riedler, J.; Schram-Bijkerk, D.; Brunekreef, B.; et al. Inverse association of farm milk consumption with asthma and allergy in rural and suburban populations across Europe. Clin. Exp. Allergy 2007, 37, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Von Mutius, E.; Vercelli, D. Farm living: Effects on childhood asthma and allergy. Nat. Rev. Immunol. 2010, 10, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Smit, L.A.; Hooiveld, M.; van der Sman-de Beer, F.; Opstal-van Winden, A.W.; Beekhuizen, J.; Wouters, I.M.; Yzermans, C.J.; Heederik, D. Air pollution from livestock farms, and asthma, allergic rhinitis and COPD among neighbouring residents. Occup. Environ. Med. 2014, 71, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Brunekreef, B.; Von Mutius, E.; Wong, G.K.; Odhiambo, J.A.; Clayton, T.O.; ISAAC Phase Three Study Group. Early life exposure to farm animals and symptoms of asthma, rhinoconjunctivitis and eczema: An ISAAC Phase Three Study. Int. J. Epidemiol. 2012, 41, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.J.; Vaca, M.; Rodriguez, A.; Chico, M.E.; Santos, D.N.; Rodrigues, L.C.; Barreto, M.L. Hygiene, atopy and wheeze-eczema-rhinitis symptoms in schoolchildren from urban and rural Ecuador. Thorax 2014, 69, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Matheson, M.C.; Walters, E.H.; Simpson, J.A.; Wharton, C.L.; Ponsonby, A.L.; Johns, D.P.; Jenkins, M.A.; Giles, G.G.; Hopper, J.L.; Abramson, M.J.; et al. Relevance of the hygiene hypothesis to early vs. late onset allergic rhinitis. Clin. Exp. Allergy 2009, 39, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Pahwa, P.; Karunanayake, C.P.; Hagel, L.; Janzen, B.; Pickett, W.; Rennie, D.; Senthilselvan, A.; Lawson, J.; Kirychuk, S.; Dosman, J. The Saskatchewan rural health study: An application of a population health framework to understand respiratory health outcomes. BMC Res. Notes 2012, 5, 400. [Google Scholar] [CrossRef] [PubMed]
- Dillman, D.A. Mail and Internet Surveys: The Tailored Design Method; John Wiley: Hoboken, NJ, USA, 2007. [Google Scholar]
- Pickett, W.; Day, L.; Hagel, L.; Brison, R.J.; Marlenga, B.; Pahwa, P.; Koehncke, N.; Crowe, T.; Phyllis Snodgrass, P.; Dosman, J. The Saskatchewan Farm Injury Cohort: Rationale and methodology. Public Health Rep. 2008, 123, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Strategies for Population Health: Investing in the Health of Canadians; Health Canada: Ottawa, ON, Canada, 1994. Available online: http://publications.gc.ca/collections/Collection/H88-3-30-2001/pdfs/other/strat_e.pdf (accessed on 1 December 2017).
- Statistics Canada. Statistical Report on the Health of Canadians; Statistics Canada: Ottawa, ON, Canada, 1999. Available online: http://www.statcan.gc.ca/pub/82-570-x/4227734-eng.pdf (accessed on 1 December 2017).
- Health Canada. Toward a Healthy Future: Second Report on the Health of Canadians; Health Canada: Ottawa, ON, Canada, 1999. Available online: http://publications.gc.ca/collections/Collection/H39-468-1999E.pdf (accessed on 1 December 2017).
- Desrosiers, M.; Evans, G.A.; Keith, P.K.; Wright, E.D.; Kaplan, A.; Bouchard, J.; Ciavarella, A.; Doyle, P.W.; Javer, A.R.; Leith, E.S.; et al. Canadian clinical practice guidelines for acute and chronic rhinosinusitis. Allergy Asthma Clin. Immunol. 2011, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. National Population Health Survey Household Component: Documentation for the Derived Variables and the Constant Longitudinal Variables; Statistics Canada: Ottawa, ON, Canada. Available online: http://www23.statcan.gc.ca/imdb-bmdi/pub/document/3225_D10_T9_V3-eng.pdf (accessed on 1 December 2017).
- Human Resources and Skills Development Canada, the Public Health Agency of Canada and Indian and Northern Affairs Canada. The Well-Being of Canada’s Young Children: Government of Canada Report; Government of Canada: Ottawa, ON, Canada, 2011. Available online: http://www.dpe-agje-ecd-elcc.ca/eng/ecd/well-being/sp_1027_04_12_eng.pdf (accessed on 1 December 2017).
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.; Curtin, S.C.; Mathews, T.J. Births: Final Data for 2012; National Vital Statistics Reports; National Center for Health Statistics: Hyattsville, MD, USA, 2013; Volume 62. Available online: https://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_09.pdf (accessed on 1 December 2017).
- Pan, W. Akaike’s information criterion in generalized estimating equations. Biometrics 2001, 57, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Hardin, J.W.; Hilbe, J.M. Generalized Estimating Equations; Chapman & Hall/CRC: Boca Raton, FL, USA, 2003. [Google Scholar]
- Fisk, W.J.; Eliseeva, E.A.; Mendell, M.J. Association of residential dampness and mold with respiratory tract infections and bronchitis: A meta-analysis. Environ. Health 2010, 9, 72. [Google Scholar] [CrossRef] [PubMed]
- Thrasher, J.D.; Gray, M.R.; Kilburn, K.H.; Dennis, D.P.; Yu, A. A water-damaged home and health of occupants: A case study. J. Environ. Public Health 2012, 2012, 312836. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.; Sundquist, K.; Sundquist, J.; Winkleby, M.A. Gestational age at birth and risk of allergic rhinitis in young adulthood. J. Allergy Clin. Immunol. 2011, 127, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.Y.; Tang, A.Z. Bacteriology of postradiotherapy chronic rhinosinusitis in nasopharyngeal carcinoma patients and chronic rhinosinusitis. Eur. Arch. Otorhinolaryngol. 2009, 266, 1403–1407. [Google Scholar] [CrossRef] [PubMed]
- Miura, M.S.; Mascaro, M.; Rosenfeld, R.M. Association between otitis media and gastroesophageal reflux: A systematic review. Otolaryngol. Head Neck Surg. 2012, 146, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Sone, M.; Kato, T.; Nakashima, T. Current concepts of otitis media in adults as a reflux-related disease. Otol. Neurotol. 2013, 34, 1013–1017. [Google Scholar] [CrossRef] [PubMed]
- Katle, E.J.; Hatlebakk, J.G.; Steinsvag, S. Gastroesophageal reflux and rhinosinusitis. Curr. Allergy Asthma Rep. 2013, 13, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Bohnhorst, I.; Jawad, S.; Lange, B.; Kjeldsen, J.; Hansen, J.M.; Kjeldsen, A.D. Prevalence of chronic rhinosinusitis in a population of patients with gastroesophageal reflux disease. Am. J. Rhinol. Allergy 2015, 29, e70–e74. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.; Winkleby, M.A.; Sundquist, J.; Sundquist, K. Gestational age at birth and risk of gastric acid-related disorders in young adulthood. Ann. Epidemiol. 2012, 22, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Shpakou, A.; Brozek, G.; Stryzhak, A.; Neviartovich, T.; Zejda, J. Allergic diseases and respiratory symptoms in urban and rural children in Grodno Region (Belarus). Pediatr. Allergy Immunol. 2012, 23, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Govaere, E.; Van Gysel, D.; Massa, G.; Verhamme, K.M.; Doli, E.; De Baets, F. The influence of age and gender on sensitization to aero-allergens. Pediatr. Allergy Immunol. 2007, 18, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, T.; Ninomiya, T.; Osawa, Y.; Imoto, Y.; Ito, Y.; Takabayashi, T.; Narita, N.; Kijima, A.; Murota, H.; Katayama, I.; et al. Factors associated with the development and remission of allergic diseases in an epidemiological survey of high school students in Japan. Am. J. Rhinol. Allergy 2015, 29, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Kilty, S.J.; McDonald, J.T.; Johnson, S.; Al-Mutairi, D. Socioeconomic status: A disease modifier of chronic rhinosinusitis? Rhinology 2011, 49, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Hox, J.J.; De Leeuw, E.D. A comparison of nonresponse in mail, telephone, and face-to-face surveys. Qual. Quant. 1994, 28, 329–344. Available online: https://0-link-springer-com.brum.beds.ac.uk/article/10.1007/BF01097014 (accessed on 3 December 2017). [CrossRef]


{kind=link}
| Quadrant of Saskatchewan | Farm Residents | Non-Farm Residents | Total | |||
|---|---|---|---|---|---|---|
| Sinus Problems | Sinus Problems | Sinus Problems | ||||
| Yes/Total | (%) | Yes/Total | (%) | Yes/Total | (%) | |
| Southwest | 182/546 | 33.3 | 383/965 | 39.7 ** | 565/1511 | 37.4 |
| Southeast | 239/699 | 34.2 | 376/1057 | 35.6 | 615/1756 | 35.0 |
| Northeast | 379/1176 | 32.2 | 366/1174 | 31.2 | 745/2350 | 31.7 |
| Northwest | 301/987 | 30.5 | 527/1493 | 35.3 ** | 828/2480 | 33.4 |
| Not Identified | 0/0 | - | 2/4 | 50.0 | 2/4 | 50.0 |
| Total | 1101/3408 | 32.3 | 1654/4693 | 35.2 * | 2755/8101 | 34.0 |
| Sinus Problems | Unadjusted OR * (95% CI) | ||
|---|---|---|---|
| Yes/Total | (%) | ||
| Contextual Factors | |||
| Socioeconomic | |||
| Household Income Adequacy | |||
| Lowest income | 98/211 | 31.7 | 0.87 (0.67, 1.14) |
| Lower middle income | 370/1183 | 31.3 | 0.85 (0.74, 0.99) |
| Upper middle income | 815/2273 | 35.9 | 1.05 (0.93, 1.18) |
| Highest income | 1081/3106 | 34.8 | 1 |
| Unknown | 391/1230 | 31.8 | 0.87 (0.75, 1.01) |
| Environmental | |||
| Quadrant (Region) | |||
| Southwest | 565/1511 | 37.4 | 1.19 (1.04, 1.37) |
| Southeast | 615/1756 | 35.0 | 1.07 (0.94, 1.23) |
| Northeast | 745/2350 | 31.7 | 0.93 (0.81, 1.05) |
| Northwest | 828/2480 | 33.4 | 1 |
| Location of Home | |||
| Farm | 1101/2307 | 32.3 | 0.87 (0.79, 0.97) |
| Non-farm | 1654/4693 | 35.2 | 1 |
| Household Smoking | |||
| Yes | 392/1222 | 32.1 | 0.90 (0.78, 1.03) |
| No | 2355/6843 | 34.4 | 1 |
| Filter of Heating system | |||
| Yes | 2385/6916 | 34.5 | 1.13 (0.97, 1.32) |
| No | 283/890 | 31.8 | 1 |
| Dampness in Past Year | |||
| Yes | 603/1551 | 38.9 | 1.29 (1.14, 1.46) |
| No | 2135/6495 | 32.9 | 1 |
| Mildew Odor or Musty Smell | |||
| Yes | 519/1350 | 38.4 | 1.27 (1.11, 1.44) |
| No | 2158/6527 | 33.1 | 1 |
| Any Pets in Home in Past Year | |||
| Yes | 1350/3688 | 36.6 | 1.24 (1.13, 1.37) |
| No | 1405/4413 | 31.8 | 1 |
| Pesticides Applied Inside Residence in Past Year | |||
| Yes | 653/1694 | 38.5 | 1.28 (1.14, 1.43) |
| No | 2073/6315 | 32.8 | 1 |
| Livestock Operation Located near Home | |||
| Yes | 442/1325 | 33.4 | 0.98 (0.86, 1.11) |
| No | 2261/6649 | 34.0 | 1 |
| Feedlot or Corrals Located near Home | |||
| Yes | 917/2690 | 34.1 | 1.01 (0.91, 1.12) |
| No | 1793/5298 | 33.8 | 1 |
| Balestack or Bales Located near Home | |||
| Yes | 1034/3017 | 34.3 | 1.03 (0.93, 1.14) |
| No | 1678/4974 | 33.7 | 1 |
| Grain Bins Located near Home | |||
| Yes | 1389/4082 | 34.0 | 1.00 (0.91, 1.11) |
| No | 1328/3910 | 34.0 | 1 |
| Sewage Pond or Manure Lagoon Located near Home | |||
| Yes | 1134/3016 | 36.5 | 1.22 (1.11, 1.35) |
| No | 1527/4777 | 32.0 | 1 |
| Water Source | |||
| Lake | 4/15 | 26.7 | 0.94 (0.73, 1.21) |
| Dugout or reservoir | 125/419 | 29.8 | 0.78 (0.61, 0.98) |
| Spring, river, or creak | 117/306 | 38.2 | 1.11 (0.85, 1.46) |
| Shallow well water (less than 100ft) | 507/1577 | 32.1 | 0.86 (0.75, 0.99) |
| Deep well water (more than 100ft) | 654/1897 | 34.5 | 0.55 (0.84, 1.10) |
| Bottled water | 872/2456 | 35.5 | 1 |
| Another source | 101/297 | 34.0 | 0.94 (0.73, 1.21) |
| Unknown | 329/1006 | 32.7 | 0.89 (0.75, 1.04) |
| Sinus Problems | Unadjusted OR * (95% CI) | ||
|---|---|---|---|
| Yes/Total | (%) | ||
| Individual Factors | |||
| Lifestyle Factors | |||
| Smoking | |||
| Current smoker | 305/951 | 32.1 | 0.96 (0.82, 1.11) |
| Ex-smoker | 1049/2868 | 36.6 | 1.18 (1.07, 1.30) |
| Never smoker | 1394/4252 | 32.8 | 1 |
| Alcohol Consumption | |||
| More than 3 times a week | 260/850 | 30.6 | 0.83 (0.69, 0.99) |
| 1–3 times a week | 637/1923 | 33.1 | 0.93 (0.80, 1.08) |
| Less than once a week | 1355/3871 | 35.0 | 1.02 (0.89, 1.16) |
| Never | 495/1435 | 34.5 | 1 |
| Early Life Exposure | |||
| Ever Lived on a Farm | |||
| Yes | 2245/6690 | 33.6 | 0.88 (0.78, 1.00) |
| No | 508/1399 | 36.3 | 1 |
| Lived on a Farm during First Year of Life | |||
| Yes | 1791/5452 | 32.9 | 0.85 (0.77, 0.93) |
| No | 939/2574 | 36.5 | 1 |
| Mother Smoking in Pregnancy | |||
| Yes | 472/1200 | 39.3 | 1.31 (1.16, 1.50) |
| No | 1954/5972 | 32.7 | 1 |
| Unknown | 323/907 | 35.6 | 1.11 (0.96, 1.29) |
| Birth Weight | |||
| <2500 g | 197/433 | 45.5 | 1.39 (1.13, 1.70) |
| ≥2500, <4000 g | 1163/3113 | 37.4 | 1 |
| ≥4000 g | 179/527 | 34.0 | 0.85 (0.70, 1.04) |
| Unknown | 1150/3842 | 29.9 | 0.70 (0.63, 0.78) |
| Breastfed as a Child | |||
| Yes | 1257/3702 | 34.0 | 0.90 (0.80, 1.00) |
| No | 804/2228 | 36.1 | 1 |
| Unknown | 648/2038 | 31.8 | 0.80 (0.70, 0.91) |
| Breastfed for 6 Months or Longer | |||
| Yes | 485/1440 | 33.7 | 0.88 (0.77, 1.01) |
| No | 1101/3042 | 36.2 | 1 |
| Unknown | 1123/3486 | 32.2 | 0.82 (0.74, 0.91) |
| Occupational History | |||
| Any Occupational History in Farm | |||
| Yes | 1113/3506 | 31.7 | 0.81 (0.74, 0.89) |
| No | 1616/4498 | 35.9 | 1 |
| Adult Farming Exposure Years | |||
| 0 | 1651/4506 | 35.8 | 1 |
| >0, <30 | 444/1355 | 32.8 | 0.86 (0.76, 0.98) |
| ≥30, <50 | 500/1534 | 32.6 | 0.85 (0.75, 0.96) |
| ≥50 | 134/505 | 26.5 | 0.63 (0.51, 0.77) |
| Occupational Exposures | |||
| Grain Dust | |||
| Yes | 1805/5431 | 33.2 | 0.86 (0.78, 0.96) |
| No | 916/2535 | 36.1 | 1 |
| Mine Dust | |||
| Yes | 151/438 | 34.5 | 0.98 (0.80, 1.20) |
| No | 2570/7528 | 34.1 | 1 |
| Asbestos Dust | |||
| Yes | 218/538 | 40.5 | 1.29 (1.08, 1.54) |
| No | 2503/7428 | 33.7 | 1 |
| Wood Dust | |||
| Yes | 1079/3073 | 35.1 | 1.04 (0.94, 1.14) |
| No | 1642/4893 | 33.6 | 1 |
| Livestock | |||
| Yes | 1393/4096 | 34.0 | 0.97 (0.88, 1.06) |
| No | 1328/3870 | 34.3 | 1 |
| Stubble Smoke | |||
| Yes | 1137/3204 | 35.5 | 1.09 (0.99, 1.20) |
| No | 1584/4762 | 33.3 | 1 |
| Diesel Fumes | |||
| Yes | 1598/4682 | 34.1 | 0.96 (0.87, 1.05) |
| No | 1123/3284 | 34.2 | 1 |
| Welding Fumes | |||
| Yes | 1048/3272 | 32.0 | 0.82 (0.75, 0.90) |
| No | 1673/4694 | 35.6 | 1 |
| Solvents | |||
| Yes | 1079/2828 | 38.2 | 1.27 (1.15, 1.40) |
| No | 1642/5138 | 32.0 | 1 |
| Oil or Gas Fumes | |||
| Yes | 636/1912 | 33.3 | 0.92 (0.83, 1.03) |
| No | 2085/6054 | 34.4 | 1 |
| Herbicides | |||
| Yes | 1408/4038 | 34.9 | 1.04 (0.95, 1.14) |
| No | 1313/3928 | 33.4 | 1 |
| Fungicides | |||
| Yes | 893/2615 | 34.1 | 0.97 (0.88, 1.07) |
| No | 1828/5351 | 34.2 | 1 |
| Insecticides | |||
| Yes | 1294/3593 | 36.0 | 1.14 (1.04, 1.25) |
| No | 1427/4373 | 32.6 | 1 |
| Mold | |||
| Yes | 1155/2761 | 41.8 | 1.64 (1.49, 1.81) |
| No | 1566/5205 | 30.1 | 1 |
| Radiation | |||
| Yes | 290/678 | 42.8 | 1.48 (1.26, 1.74) |
| No | 2431/7288 | 33.4 | 1 |
| Health Conditions | |||
| House Dust Allergy | |||
| Yes | 645/1016 | 63.5 | 4.09 (3.56, 4.69) |
| No | 2032/6848 | 29.7 | 1 |
| Cat Allergy | |||
| Yes | 519/906 | 57.3 | 2.99 (2.59, 3.45) |
| No | 2158/6958 | 31.0 | 1 |
| Dog Allergy | |||
| Yes | 289/468 | 61.8 | 3.39 (2.80, 4.12) |
| No | 2388/7396 | 32.3 | 1 |
| Grass Allergy | |||
| Yes | 730/1243 | 58.7 | 3.37 (2.97, 3.82) |
| No | 1947/6621 | 29.4 | 1 |
| Pollen Allergy | |||
| Yes | 986/1663 | 59.3 | 3.85 (3.43, 4.31) |
| No | 1691/6201 | 27.3 | 1 |
| Mold Allergy | |||
| Yes | 856/1380 | 62.0 | 4.16 (3.68, 4.69) |
| No | 1821/6484 | 28.1 | 1 |
| Ear Infection in Past Year | |||
| Yes | 248/423 | 58.6 | 2.85 (2.34, 3.46) |
| No | 2466/7520 | 32.8 | 1 |
| Stomach Acidity or Reflux in Past Year | |||
| Yes | 566/1139 | 49.7 | 2.08 (1.83, 2.36) |
| No | 2143/6788 | 31.6 | 1 |
| Usual Cough | |||
| Yes | 540/1207 | 44.7 | 1.66 (1.47, 1.88) |
| No | 2189/6822 | 32.1 | 1 |
| Usual Phlegm | |||
| Yes | 529/1222 | 43.3 | 1.55 (1.37, 1.75) |
| No | 2172/6721 | 32.3 | 1 |
| Ever Wheeze | |||
| Yes | 1494/3304 | 45.2 | 2.29 (2.08, 2.51) |
| No | 1261/4797 | 26.3 | 1 |
| Ever Asthma | |||
| Yes | 459/787 | 58.3 | 2.99 (2.57, 3.47) |
| No | 2296/7314 | 31.4 | 1 |
| Ever Hay Fever | |||
| Yes | 659/967 | 68.1 | 5.10 (4.39, 5.91) |
| No | 2095/7133 | 29.4 | 1 |
| Number of Chronic Diseases | |||
| 0 | 1486/4575 | 32.5 | 1 |
| 1 | 806/2247 | 35.9 | 1.15 (1.04, 1.28) |
| ≥2 | 463/1279 | 36.2 | 1.17 (1.03, 1.33) |
| Family History | |||
| Father Lung Disease | |||
| Yes | 541/1236 | 43.8 | 1.65 (1.46, 1.86) |
| No | 1884/5989 | 31.5 | 1 |
| Unknown | 328/870 | 37.7 | 1.31 (1.13, 1.52) |
| Mother Lung Disease | |||
| Yes | 404/872 | 46.3 | 1.74 (1.51, 2.01) |
| No | 2145/6623 | 32.4 | 1 |
| Unknown | 206/605 | 34.0 | 1.07 (0.89, 1.27) |
| Brother/Sister Lung Disease | |||
| Yes | 411/858 | 47.9 | 1.90 (1.65, 2.20) |
| No | 2057/6414 | 32.1 | 1 |
| Unknown | 286/825 | 34.7 | 1.10 (0.94, 1.28) |
| Sinus Problems | Unadjusted OR * (95% CI) | ||
|---|---|---|---|
| Yes/Total | (%) | ||
| Covariates | |||
| Sex | |||
| Male | 1115/3984 | 28.0 | 1 |
| Female | 1640/4113 | 39.9 | 1.69 (1.55, 1.85) |
| Age (Years) | |||
| 18–45 | 665/1264 | 34.5 | 1 |
| 46–55 | 710/2025 | 35.1 | 1.03 (0.90, 1.17) |
| 56–65 | 712/1915 | 37.2 | 1.11 (0.97, 1.27) |
| >65 | 668/2227 | 30.0 | 0.80 (0.70, 0.92) |
| Body Mass Index (kg/m2) | |||
| Normal (<25) | 743/2301 | 32.3 | 1 |
| Overweight (≥25, <30) | 1010/3143 | 32.1 | 0.98 (0.88, 1.10) |
| Obese (≥30) | 854/2258 | 37.8 | 1.25 (1.11, 1.42) |
| Education | |||
| ≤Grade 12 | 1482/4825 | 30.7 | 0.69 (0.63, 0.76) |
| >Grade 12 | 1237/3186 | 38.8 | 1 |
| Adjusted OR * (95% CI) | |
|---|---|
| Contextual Factors | |
| Environmental | |
| Quadrant (Region) | |
| Southwest | 1.10 (0.93, 1.31) |
| Southeast | 0.96 (0.81, 1.14) |
| Northeast | 0.95 (0.81, 1.11) |
| Northwest | 1 |
| Location of Home | |
| Farm | 0.83 (0.73, 0.94) |
| Non-farm | 1 |
| Sewage Pond or Manure Lagoon Located near Home | |
| Yes | 1.19 (1.05, 1.34) |
| No | 1 |
| Individual Factors | |
| Lifestyle Factors | |
| Smoking | |
| Current smoker | 0.92 (0.76, 1.10) |
| Ex-smoker | 1.22 (1.08, 1.38) |
| Never smoker | 1 |
| Early Life Exposure | |
| Birth Weight | |
| <2500 g | 1.66 (1.29, 2.13) |
| ≥2500, <4000 g | 1 |
| ≥4000 g | 1.08 (0.85, 1.38) |
| Unknown | 0.90 (0.79, 1.03) |
| Occupational Exposures | |
| Solvents | |
| Yes | 1.35 (1.18, 1.53) |
| No | 1 |
| Mold | |
| Yes | 1.32 (1.16, 1.50) |
| No | 1 |
| Radiation | |
| Yes | 0.95 (0.67, 1.35) |
| No | 1 |
| Health Conditions | |
| House Dust Allergy | |
| Yes | 1.98 (1.50, 2.61) |
| No | 1 |
| Pollen Allergy | |
| Yes | 1.38 (1.16, 1.65) |
| No | 1 |
| Mold Allergy | |
| Yes | 1.93 (1.55, 2.39) |
| No | 1 |
| Ear Infection in Past Year | |
| Yes | 2.99 (2.28, 3.93) |
| No | 1 |
| Stomach Acidity or Reflux in Past Year | |
| Yes | 2.37 (1.85, 3.02) |
| No | 1 |
| Ever Wheeze | |
| Yes | 1.69 (1.51, 1.90) |
| No | 1 |
| Ever Hay Fever | |
| Yes | 2.85 (2.36, 3.45) |
| No | 1 |
| Family History | |
| Father Lung Disease | |
| Yes | 1.28 (1.10, 1.48) |
| No | 1 |
| Unknown | 1.35 (1.09, 1.67) |
| Mother Lung Disease | |
| Yes | 1.30 (1.10, 1.54) |
| No | 1 |
| Unknown | 0.99 (0.76, 1.29) |
| Brother/Sister Lung Disease | |
| Yes | 1.34 (1.12, 1.61) |
| No | 1 |
| Unknown | 1.08 (0.88, 1.32) |
| Covariates | |
| Sex | |
| Male | 1 |
| Female | 1.81 (1.61, 2.03) |
| Age (Years) | |
| 18–45 | 1 |
| 46–55 | 1.08 (0.92, 1.26) |
| 56–65 | 1.18 (1.00, 1.39) |
| >65 | 0.99 (0.83, 1.17) |
| Education | |
| ≤Grade 12 | 0.76 (0.68, 0.86) |
| >Grade 12 | 1 |
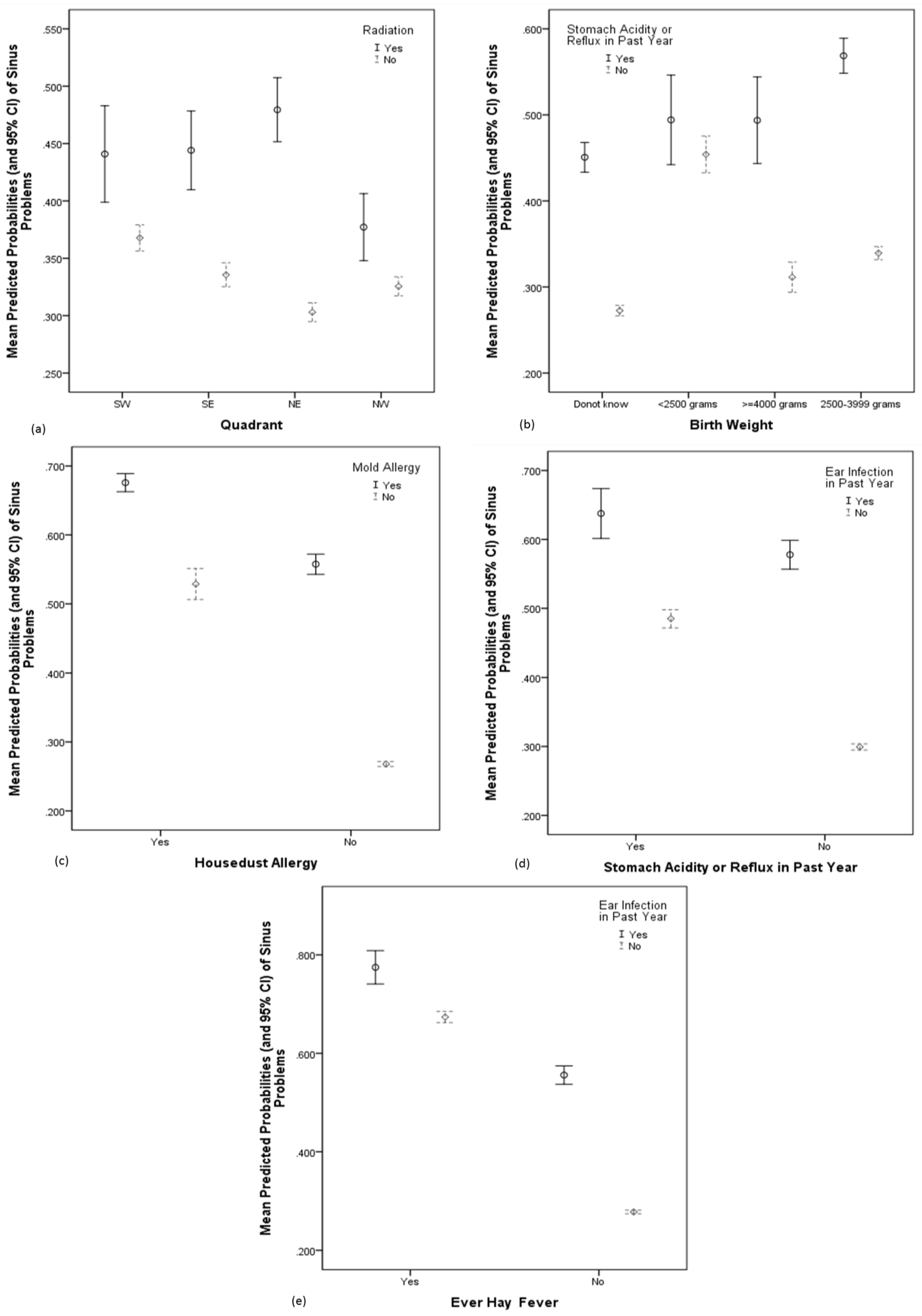
| Significant Interactions (Please see Figure 1) | p-Value |
| Quadrant and Radiation | 0.010 |
| Birth Weight and Stomach Acidity or Reflux | 0.003 |
| House Dust Allergy and Mold Allergy | 0.003 |
| Stomach Acidity or Reflux and Ear Infection | 0.025 |
| Ever Hay Fever and Ear Infection | 0.041 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kajiwara-Morita, A.; Karunanayake, C.P.; Dosman, J.A.; Lawson, J.A.; Kirychuk, S.; Rennie, D.C.; Dyck, R.F.; Koehncke, N.; Senthilselvan, A.; Pahwa, P.; et al. Prevalence and Determinants of Sinus Problems in Farm and Non-Farm Populations of Rural Saskatchewan, Canada. Sinusitis 2018, 3, 2. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis3010002
Kajiwara-Morita A, Karunanayake CP, Dosman JA, Lawson JA, Kirychuk S, Rennie DC, Dyck RF, Koehncke N, Senthilselvan A, Pahwa P, et al. Prevalence and Determinants of Sinus Problems in Farm and Non-Farm Populations of Rural Saskatchewan, Canada. Sinusitis. 2018; 3(1):2. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis3010002
Chicago/Turabian StyleKajiwara-Morita, Ayami, Chandima P. Karunanayake, James A. Dosman, Joshua A. Lawson, Shelley Kirychuk, Donna C. Rennie, Roland F. Dyck, Niels Koehncke, Ambikaipakan Senthilselvan, Punam Pahwa, and et al. 2018. "Prevalence and Determinants of Sinus Problems in Farm and Non-Farm Populations of Rural Saskatchewan, Canada" Sinusitis 3, no. 1: 2. https://0-doi-org.brum.beds.ac.uk/10.3390/sinusitis3010002