
Migrants’ Health Policies and Access to Health Care in Portugal within the European Framework


Centro Lusíada de Investigação em Serviço Social e Intervenção Social (CLISSIS), Lusíada University of Lisbon, 1349-001 Lisboa, Portugal
*
Author to whom correspondence should be addressed.
Societies 2022, 12(2), 55; https://0-doi-org.brum.beds.ac.uk/10.3390/soc12020055
Submission received: 28 January 2022
/
Revised: 19 February 2022
/
Accepted: 25 March 2022
/
Published: 28 March 2022
(This article belongs to the Special Issue Racial Capitalism and Public Health: Decolonizing Diversity and Inclusion)
Abstract
:Migratory flows have a specific influence in the European and Portuguese demographic context. Societies’ commitment to ensure fundamental rights of all citizens and migrants includes the promotion of health. This study aims to describe migrants’ health policies and access to the health system in Portugal within the European framework. We carried out a mixed methods approach, analyzing health policies in European Union countries and public health key indicators from statistical secondary data collected from Eurostat and Migrant Integration Policy Index. This data was complemented with a survey applied to immigrants living in Portugal. Portugal is a European country known for its favorable immigrant integration policies and has developed access to the health care system. However, our study has shown that greater investment is needed to overcome limitations or social inequalities which inhibit migrants’ access. Additionally, we sought to present a comparative analysis between Portugal and European Union countries, which can contribute to improve health systems within the current crisis.
1. Introduction
Migration flows have a profound impact on European societies, its economy and its culture [1]. Migrants move to and within Europe for various reasons, such as seeking work, better life opportunities, family reunification, as well as people seeking for asylum and international protection due to conflict, persecution and human rights violations [2,3,4,5]. Considering the increase of migration to European countries, effective integration of migrants and refugees is crucial for the well-being and cohesion of European societies and for regional development [6].
In Portugal, this is a relevant issue considering the influence of globalization in the accentuation of migratory trends, as shown in the Strategic Plan for Migration 2015–2020 (Resolution of the Council of Ministers no. 12-B/2015) which mentioned the concern to respond to the multiple impacts of the global crises, including in the field of health. Among the global crises, the 2008 financial crisis and resulting austerity measures negatively affected the universality of health coverage and health care, evidenced particularly in southern European countries [4,7,8].
Additionally, the National Implementation Plan of the Global Migration Pact (Council of Ministers Resolution no. 141/2019) highlighted the relevance of promoting the reception and integration of immigrants in different areas (e.g., family reunification, mastery of the Portuguese language, education and vocational training, access conditions to housing, health and social protection), stimulating their integration and civic participation. In the field of health, this plan reinforces the commitment to the Sustainable Development Goals [9] and to the Pillar of European Rights [10], reinforcing the European responsibility to affirm health as a right for all, as stated in the Charter of Fundamental Rights of the European Union [11].
Looking at the Portuguese historical context, the influence of migratory movements in Portugal corresponds to an evident and quite relevant transformation in contemporary societies with the integration of the immigrant population [4,12,13]. The relationship between migratory flows and immigrant integration in Portugal has accompanied the various historical events and changes, with different flows and levels of intensity, as well as in diverse origins of the immigrant population [14,15].
The large influx of the immigrant population coming from African Countries of Portuguese Official Language (PALOP) originates after the end of the dictatorship in Portugal in the 1970s. This event contributed to an increase in immigration movements from PALOP [4,13] and later from Brazil, boosted by the decolonization and independence of these peoples, as well as the need and demand for labor [4,16]. The migratory trends to Portugal followed a logic of recruitment and demand for low-skilled labor, with situations of precariousness, illegality and social vulnerability [17]. Post-colonial dependency, family reunification and high fertility among young immigrant groups were an important factor in the intensification of immigration in Portugal [14]. These migration flows, although occurring in different historical periods and contexts, portray transversally the need to search for better living conditions, regardless of the language barrier or the labor conditions that immigrants face in the host country [10]. Even for immigrants from Portuguese-speaking countries, the existence of different dialects and variations in Portuguese, which include large phonological and lexical differences, creates difficulties in communicating in the host country [18].
According to the Immigration, Borders and Asylum Report [19], in recent years, the effects of economic recovery have led to a new growth of immigration in Portugal. Between 2018 and 2019, a quite significant increase (22.9%) of the immigrant population in Portugal was recorded, increasing the number of citizens coming from European countries. However, the largest number of immigrants entering Portugal comes from Brazil and PALOP countries, especially from Cape Verde, Angola and Guinea-Bissau. These data correspond to the immigrant population in a situation of legal stay or residence in Portugal (i.e., it does not include immigrants in an irregular situation in the country) [19].
Access to health care has been the subject of several studies which follow a line of sociological research on migratory flows and the integration of immigrant people in Portugal [20,21,22]. However, we found that there were few studies on the Portuguese context of health care accessibility for the migrant population [23], thus leading us to develop this topic.
Health services and the promotion of the physical and social wellbeing of immigrant populations can create improved conditions and contribute to a better social integration in the host destinations [24]. Thus, the consequences of the lack of access to health care are not only limited to the individual but also extend to the family nucleus and to the community where he/she lives [25]. In this biopsychosocial intervention, the dimension of health needs to be analyzed in a context that also includes environmental, social and behavioral factors [26].
This study intends to summarize and describe an analysis of the health care access policies in European Union countries, as well as immigrant population health status and access in Portugal. We seek to provide readers with a reflected and informed scope, combining official and international statistical data, as well as a set of policies taken to promote access to health care and immigrants’ perception within the Portuguese context. This becomes particularly relevant with the COVID-19 pandemic, since there has been a worsening of the health conditions of the global population and an overload of health systems, which has had a strong impact on the lives of the population [27].
Therefore, we conducted a research project on the promotion of access to health care for the immigrant population in Portugal which aims to: (i) elaborate a systematization of integrating and effective practices of social rights and (ii) analyze the conditions of access to health care for immigrant populations. Regarding the first part of this project, we present an exploratory analysis of immigrants’ health status, health care and health policies to guide future researchers, but also health and social care professionals, providing a diversity of systemized data. The main finding regarding health policies, health key indicators and immigrants’ perception are triangulated in the Results section. Finally, we discuss our findings referring to the main aspects to improve in health status and access to health care in Portugal, followed by study limitations, future research, and conclusions.
2. Materials and Methods
This study’s goal started with the following research question: “How does Portugal ensure access to health care for migrants with its health policies within the European framework?”. To address this question, we followed a mixed methods study combining qualitative and quantitative data as an added value research approach, a methodology that has been recognized in health studies [28]. The first procedure was the analysis of systematization and review documents, which allowed a better understanding of the context and to complement other types of research data sources, thus enabling a comparative analysis between health policies [29]. In a second procedure, we examined secondary statistical data on health indicators in different European Union countries, which have already been proved useful in other comparative health studies [30]. Finally, we carried out a survey addressed to immigrants in Portugal, using the same questions applied by Eurostat on basic health indicators, in order to make a current descriptive analysis on the access to health care of the immigrant population in Portugal.
2.1. Document Analysis
Document analysis enables further policy research into health policy [31]. We selected a diversity of international and national documents, laws and reports that allowed us to obtain a characterization of the health policies and measures adopted in the different European Union countries and in Portugal.
For a country-by-country analysis, we selected the most recent Country Health Profile produced by the OECD/European Observatory on Health Systems and Policies [32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51] to identify observations regarding the accessibility of health care to migrants. Therefore, we analyzed the reports for 2019 for all 28 countries of the European Union, including the United Kingdom. We also consulted other reports from international bodies such as the Migrant Integration Policy Index (2020) [52] and the European Centre for Disease Prevention and Control (2021) [53]. Additionally, we collected and compiled the legal framework regarding access to health care and services for the migrant population in Portugal, including the exceptional and temporary measures during the COVID-19 pandemic.
2.2. Secondary Statistical Data
The first source of secondary statistical data collection was the Migrant Integration Policy Index (MIPEX) online database [54], which allowed for the analysis of the ranking of immigrant integration policies in all the countries of the European Union. Secondly, we considered it particularly important to analyze all the variables on health status, because they represent the Minimum European Health Module [55]. The data collected and examined relates to the foreign population aged over 16 years or over living in European Union countries. These indicators use health variables of the European Statistics of Income and Living Condition (EU-SILC) survey. In this sense, we scrutinized the 3 variables on health status and 1 variable on health care. This last variable, regarding self-reported unmet needs for medical examination, included seven main reasons for classification. Thus, we analyzed a set of indicators according to the following description criteria (Table 1).
Considering the data available, the values regarding European Union countries’ (EU28) mean are estimated and only until 2019. For a more complete analysis, we included the United Kingdom, referring to data from EU28 in 2019. Additionally, we collected Eurostat data from 2020, selecting the countries which had this data available for comparison, including Portugal. These data allow for a description of each of the indicators and their relationship contributes to a combined view between health policies and migrants’ perception of their health status, health care and the health policies.
2.3. Survey
The aim of our survey was to collect data to describe immigrants’ responses within the data collected by Eurostat, and also to allow participants to respond to open-ended questions based on their previous close-ended answers. Therefore, our questionnaire was based on a common framework defined by the European Statistics of Income and Living Condition (EU-SILC) survey, regarding the small module on health issues [55]. We used four sections referring to the variables used by Eurostat and added a question on access to health care during the pandemic period. For this reason, in all parts of the questionnaire, after the presentation of each closed response question, we presented an open response question. In total, the questionnaire was composed of 5 sections: (i) Health status (2 questions); (ii) Part 2—Chronic (long-standing) illness or condition (2 questions); (iii) Limitation in activities because of health problems (2 questions); (iv)—Unmet need for medical examination or treatment (1 or 2 questions—dependent on the answer to the 1st question); (v)—Access to health services during the pandemic (2 questions).
Before the questions that made up the main part of the questionnaire were presented, we dedicated the first part to the introduction of the study, indicating its objectives and purposes. It was also mentioned that the questionnaire was intended only for immigrant people aged 16 or older. To comply with the ethical procedures fundamental to any research, we informed participants that all questions would be anonymous and confidential, that no question would reveal their identity, and that they could contact the researchers via email if they had any questions. All participants had to validate that they agreed to participate in this study, expressing their informed consent. If they selected the “yes” option, the questionnaire was presented. If they selected the option “no”, they were automatically directed to a closing page. As for socio-demographic data, we only used those that could be convergent with the Eurostat indicators used in the secondary data analysis. Therefore, we only asked for gender and country of origin/birth.
Of the 102 participants in the study, the majority were women (59.8%), with one person refusing to indicate his or her gender. Most participants came from African Countries whose official language is Portuguese (37.3%), namely: Angola—8.8%; Guinea-Bissau—7.8%; Sao Tome and Principe —7.8%; Mozambique—6.9% and Cape Verde—5.9%; also of note is the participation of the Brazilian population (33.3%), which is the largest country with Portuguese as an official language. Of the total number of European participants (24.5%), most are from European Union countries, namely Belgium, France, Germany, Italy, Lithuania, Poland, Romania and Spain. There was also the participation of the Asian population (4.9%) namely India, Pakistan and Nepal.
The participants’ age was not asked, since according to the Eurostat script, respondents are not specifically asked to compare their health with that of other people of the same age. We also felt that fewer questions would be less intrusive, considering that health is a personal and, in some cases, very delicate/sensitive subject.
The questionnaire was designed using Microsoft Office Forms application with an institutional email account of the Research Centre/University where this study is integrated. For a better understanding of the questionnaire’s content, we prepared a version in Portuguese and another in English. For this article, we translated open responses to English. Its dissemination was carried out through associations and informal groups of immigrants via WhatsApp during December 2021. We chose this route so that the questionnaire would not be extended to non-immigrant people and to avoid invalid answers. The data were analyzed using SPSS v.28 to carry out a descriptive analysis of collected information, with a previous categorization of the open answers. The data analysis allowed a triangulation, combining the information obtained via the different sources and data collection techniques selected [56].
3. Results
In this section, we share the findings, organizing them into four dimensions: (1) Health policy; (2) Health status; (3) Health care and (4) Health care during COVID-19. For each sub-section, we provide our results through documents and/or statistical data analysis, which supports each dimension.
3.1. Health Policy
Analyzing the measures implemented in European countries, the data provided by the Migrant Integration Policy Index (MIPEX) allowed us to systematize the evaluation of immigrant integration policies, namely in the field of health. Based on the evaluation of the measures in the different countries, we compared the ranking of the different countries, namely the European Union (Table 2).
The countries that stand out with favorable health policies are Ireland (85), Sweden (83), Spain (81) and Austria (81). Data reported regarding Ireland highlighted the National Intercultural Health Strategy 2018–2023 and state that, in general, immigrant population are informed and supported by responsive health services and the National Office of Social Inclusion [52]. For Sweden, this value is consistent with other indicators, considering that it is the best EU28 ranked country in this index (86). Immigrants, including undocumented immigrants, have almost the same rights as nationals. It is highlighted that immigrants are regularly informed about their rights and receive additional forms of support [52]. In Spain, immigrants are informed of their health rights and benefit from adequate services, and since 2018, there are no obstacles to access health care for immigrant people [52]. Finally, in Austria, the equal conditions of the insurance-based health system for legal migrants and nationals are mentioned, and immigrant people are informed about health care in several languages through different means [52].
The case of Ireland, Spain and Austria shows that although these countries have only slightly favorable and halfway favorable immigrant integration policies (64, 60 and 45, respectively), they are more prepared to respond to the health issues of the immigrant population.
Portugal is in third place in the classification of this index with a favorable global score (82), being one of the European countries with the better integration policies. The Portuguese health system has slowly improved immigrants’ access to health care and health information [52]. However, we observed that this value decreases when the global total includes health as a variable, considering that the measures adopted in Portugal still need further reinforcement, according to the reports by MIPEX. Although Portugal stands out above the average of the European Union countries, it is in ninth place regarding health policies for the integration of immigrants with a classification in the index of Slightly favorable (65).
The right to health protection is universal through the National Health Service and tends to be free (Constitutional Law no. 1/2005—article 64) and should be guaranteed to all citizens regardless of their economic, social or legal status. According to the Ministry of Health (Order no. 25360/2001), foreign citizens legally residing in Portugal have equal access to health care and medication provided by the National Health Care System, and by the institutions and services that constitute it. In addition, it is stated that undocumented migrants need a certificate to prove they are living in the country for longer than 90 days to have free access to the health care system, on equal terms as nationals. In case of urgent and lifesaving care, health assistance is always granted.
With the financial crisis in Portugal, an exemption from charging migrants or nationals was introduced upon proof of financial need. To qualify, it was necessary to fill in an application form and to provide copies of personal documents such as identification card, health card, fiscal identification and social security number (Decree-Law No. 113/2011; Decree-Law No. 128/2012).
In 2016, a Joint Informative Document of the Central Administration of Health Systems and the Directorate-General for Health reinforced the free access to the National Health System for asylum seekers and beneficiaries of international protection and their family members (Circular Informativa Conjunta no. 13/2016/CD/ACSS).
The recent Portuguese Health Law No. 95/2019 strengthens the right to health protection for all people, defending free, equal and non-discriminatory access to quality health care. Protecting the guarantee of equity is stated with the adoption of measures of positive differentiation of people and groups in situations of greater vulnerability (Law No. 95/2019—Article 4) and people participation in health policies’ planning, design and evaluation (Law No. 95/2019—Article 5).
Regarding the historical and political context of immigration in the country, it is important to mention the international/bilateral protocols with some countries, mainly Portuguese-speaking countries, which allow access to free care for these foreign citizens under the established treatment agreements. There are also agreements with social security, allowing access to health services in cases of extended stay or residence.
3.2. Health Status
In this sub-section, we present three variables linked to health status according to European Statistics of Income and Living Condition (EU-SILC). The variables on health status indicate: “Self-perceived health” (how a person perceives his/her health in general); “Chronic morbidity” (if the person suffers from any longstanding illness or health problem—for a duration of at least six months) and “Activity limitation” (limitation in activities people usually do because of one or more health problems—lasting for at least the past six months) [57].
3.2.1. Self-Perceived Health
Eurostat data for the year 2019 indicates a less favorable self-perception of health among the foreign population in Portugal, in which only 12% said they were very healthy, compared to the average in the countries of the European Union (23.6 percentage points—pp). In Portugal, it is especially the national population that has the least positive perception of their state of health (9.3 pp).
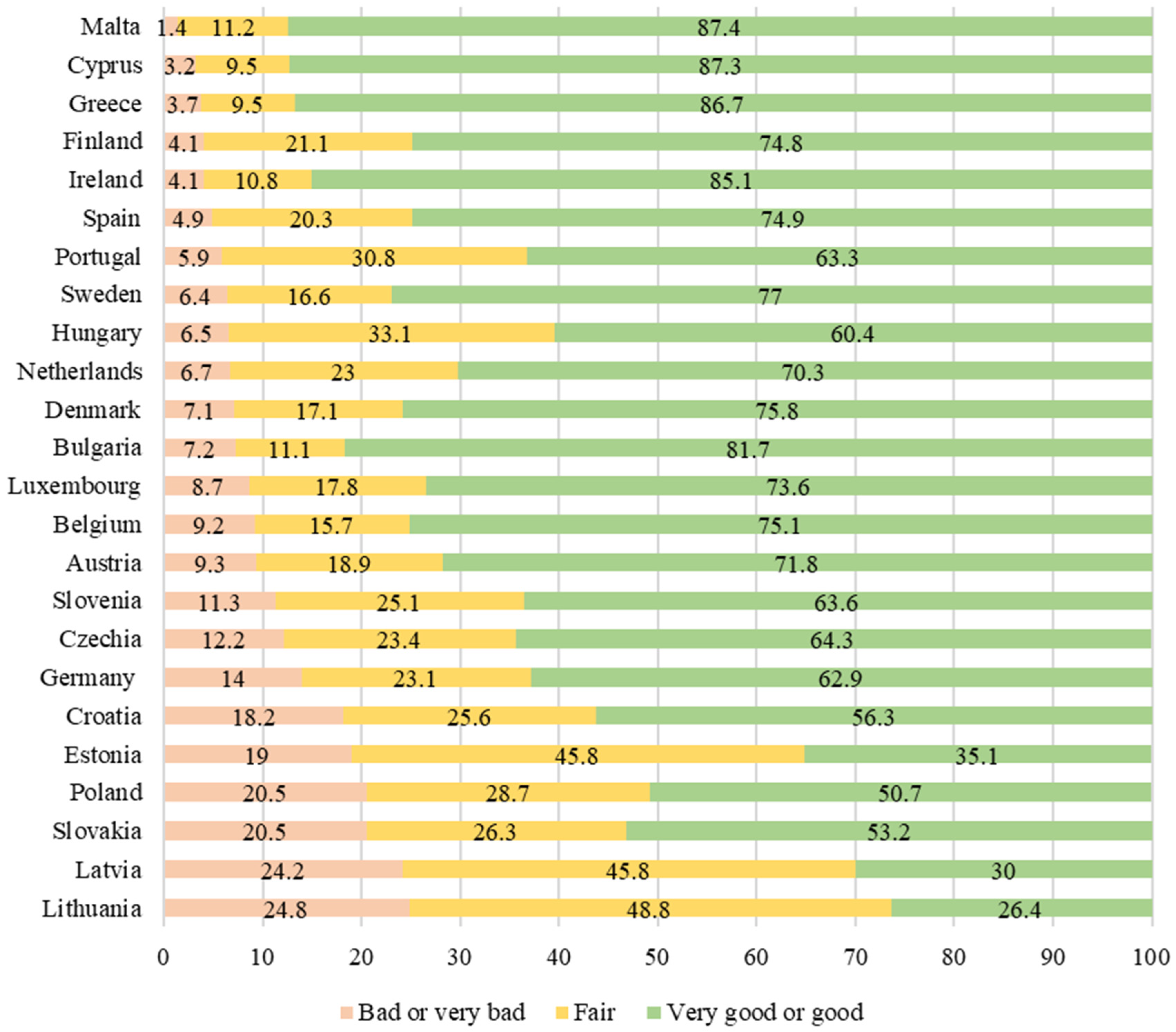
When comparing the perception of health of the foreign population in Portugal with other European Union countries in 2020, we can see that it is predominantly in Eastern Europe that the foreign population considers itself to be less healthy (Figure 1).
We highlight that in Lithuania, Estonia and Latvia, the positive assessment on the perception of the state of health by the foreign population is well below 50%, being Lithuania and Latvia where this result is more negative (24.8 pp and 24.2 pp, respectively). In this analysis, we excluded the data referring to the average of the European Union, France, Italy and Romania, as there are no figures for the year 2020. Although Portugal is the sixteenth country on the list with a “good or very good” satisfaction (63.3 pp), it appears in seventh place (5.9 pp) for “bad or very bad” satisfaction.
The data we collected for our questionnaire presents a better scenario. The majority of the foreign population participating in the study states that they are in good health (48%) or in very good health (25.5%). The most indicated reason for a positive perception of health status is a healthy lifestyle or genetic conditions.
“No physical issues because of genetics (Black race). It is a cultural thing, social and emotional dimension... It runs in the family! All healthy” (ID11, Male, Africa).
“I am a sports person, I have a long period throughout the year in which I eat correctly, I do activities that keep my mind active such as reading, etc.” (ID31, Male, Europe).
It is important to mention that some people who rated their health as good or very good, in the open response, indicate situations of illness.
“I don’t have any major health problems, just a few colds and flus, as usual” (ID 13, female, South America).
“I am healthy in general, but I have some issues like scoliosis and an ovarian cyst” (ID 58, female, Europe).
It is only women who claim to have bad (6.9%) or very bad (1%) health. The main reasons include both physical and mental health issues.
“I feel very tired of life, it’s very hard to take all the pressure of this virus” (ID 101, female, Europe).
Additionally, we categorized the answers into a double classification of healthy or unhealthy. Based on the open answers, we analyzed the participants who responded, “nor good nor bad” (18.6%) except for those who did not answer or provided an unclear answer. In a total of 98 valid answers, we identified that 77.6% of the participants feel healthy.
3.2.2. Chronic Morbidity
As for long-standing illness or health problems (Chronic morbidity), the 2019 data indicate that Portuguese (42 pp) feel worse than the foreign population living in Portugal (−10.8 pp) and worse than the average European Union citizen (−4.9 pp). The comparison between the national and foreign populations shows that foreign people have fewer long-standing illness or health problems than the Portuguese (43.8 pp), especially those that are from other European Union countries (33.1%). However, we must mention that during the year 2020, all groups indicated more health problems, with this increase being greater for foreign citizens.
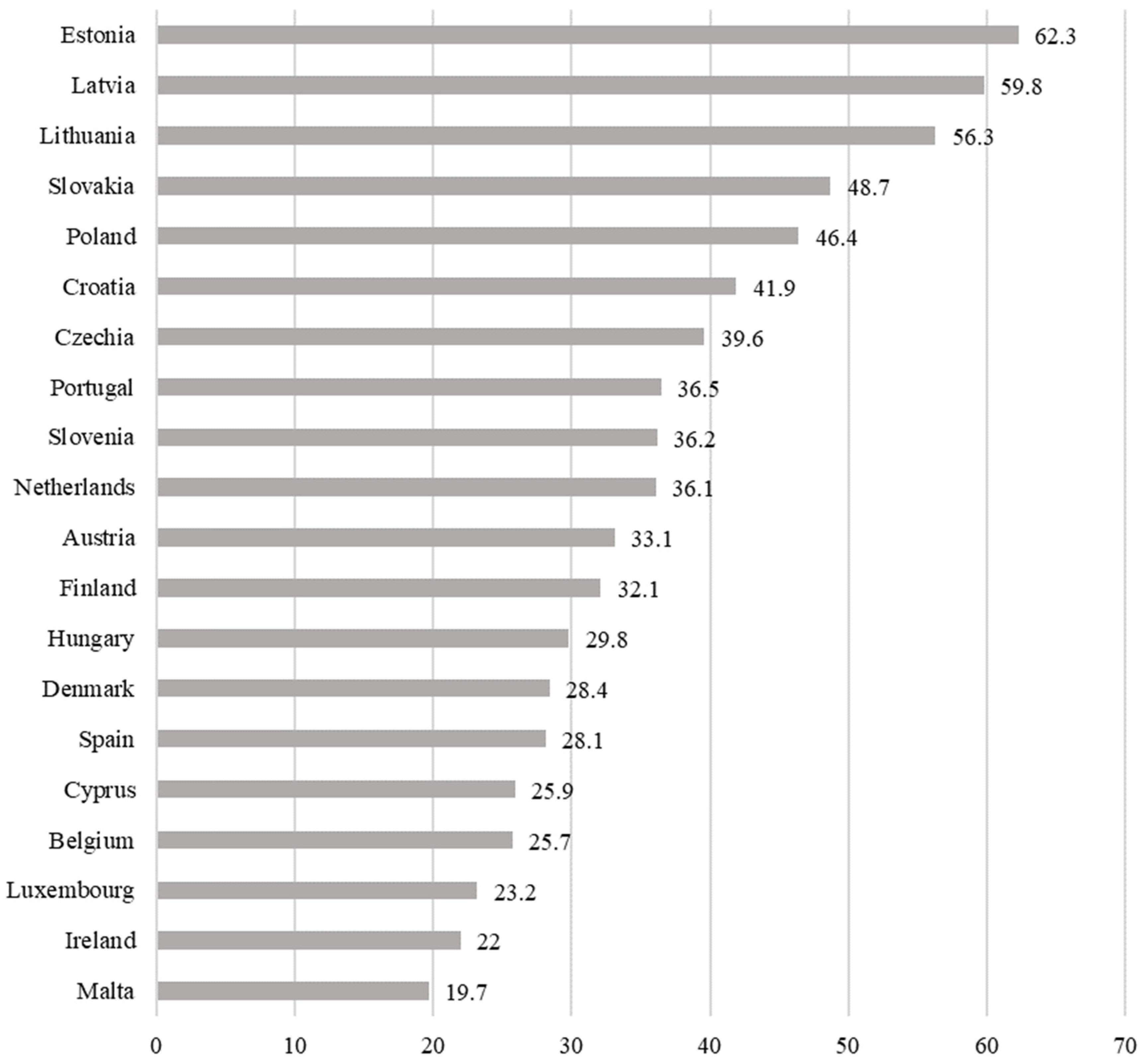
The data in Figure 2, referring to 2020, helps us to understand the position of Portugal compared to other European Union countries regarding long-standing illness or health problem in the foreign population. Portugal is the eighth country in which the immigrant population claims to have more chronic diseases.
The countries with worse results, when compared to Portugal, are Eastern European countries. In some of these countries, more than half of the foreign population claims to have a long-standing illness or health problem, such as Estonia (62.2 pp), Latvia (59.8 pp) and Lithuania (56.3 pp). We excluded Bulgaria, France, Germany, Italy and Romania from this analysis as in Eurostat, there is no data available for the year 2020.
Regarding the answers to our questionnaire, 35.3% of the respondents stated that they had a long-standing illness or health problem. This result is in line with the latest Eurostat data. Among the main complaints are the following: allergies and respiratory diseases, depression and anxiety, gynecological problems, headaches, hypertension, muscle aches/pains, among others. Some people indicate suffering from comorbidity.
“I don’t sleep more than 5 h, suffer with pain in my ovaries, back and legs” (ID92, female, Europe).
It is noteworthy that several participants indicated having access to regular check-ups and medical follow-ups.
“Lupus, which has been under investigation for 4 months, but I have had symptoms for at least 2 years” (ID 89, female, South America).
Of all the men participating in the study, 23.1% indicated suffering from chronic diseases, this value being higher among women (44.3%). In terms of nationalities, people from Africa (38.9%) indicated more chronic diseases, followed by Europeans (33.3%) and South Americans (27.8%). None of the Asian immigrants surveyed reported cases, although one person responded that did not know.
3.2.3. Activity Limitation
Eurostat data for 2019 indicated that the foreign population in Portugal and in the European Union feel less limited in their usual activities due to health problems (23.8 pp and 21.2 pp, respectively). In contrast, the Portuguese population has the worst perception regarding limitations on their usual activities (33.2 pp), being 9.5% higher than the foreign population of the country and 8.1% higher than citizens from European Union countries.
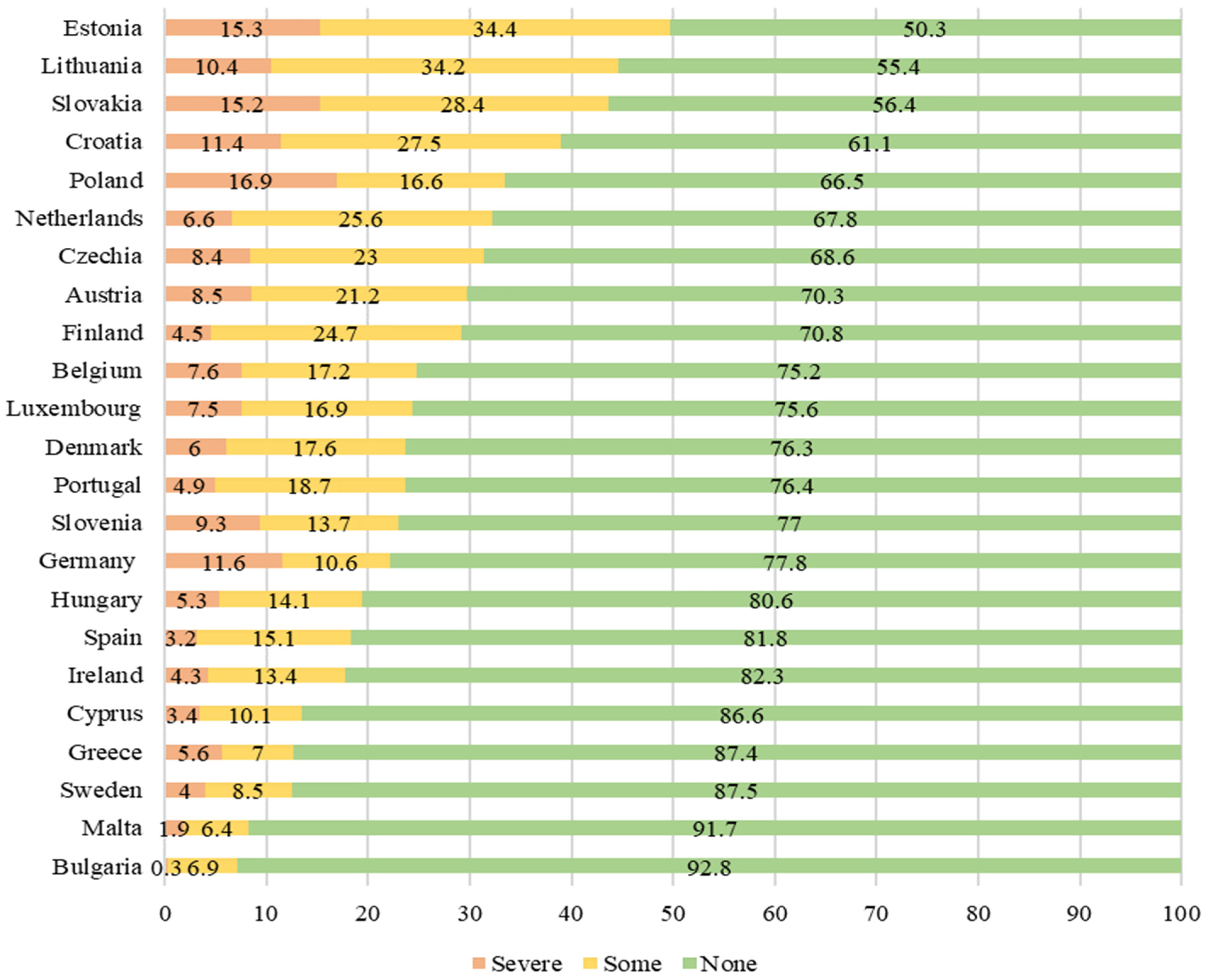
Analyzing the data in Figure 3 on self-perceived long-standing limitations in usual activities due to health problems, once again we find that it is in Eastern European countries that the foreign population have the most severe health problems that limit their activities, namely Poland (16.9 pp), Estonia (15.3 pp) and Slovakia (15.2 pp).
In most countries, more than three-quarters of immigrant citizens do not have any health problems that prevent them from carrying out their usual activities. According to the data collected, the average number of immigrant persons who respond positively to this indicator is 73.3%. In Portugal, we can see that only around 5 in every 100 foreigners consider that they are severely limited in their daily activities due to some illness and that around 18.7% have felt some limitation, but not severe.
While Eurostat data points to indicators of autonomy in the usual activities of the foreign population in Portugal (76.4%), our questionnaire registered only 59.9% of people who stated that they did not feel any limitation. In the case of severe limitations, we obtained the same percentage as the Eurostat data (4.9%), but there are more people indicating some limitations (25.5%). It was also registered that 8.8% answered that they did not know. Although we cannot make a comparative analysis of the data, we understand that there may be health factors (e.g., COVID-19) that may contribute to these results, given that some answers indicated that the limitations felt are associated with post-COVID recovery.
Of the participants who reported feeling severe limitations (4.9%), all were women and revealed that they felt limitations in several essential daily tasks.
“Inability to drive, take care of house and everyday things, inability to work” (ID36, female, Brazil).
There are several reasons described for the limitations experienced. We found answers that are in line with the aforementioned chronic diseases. Interestingly, people who feel limited due to headaches indicated that they felt their health status was good, but manifested limitations in their activities.
“Well, when I have migraines, I can’t do activities, I have to sleep” (ID28, female, Europe).
“I’ve had to stop work with such a headache, I couldn’t concentrate on the things I was doing” (ID64, female, Africa).
The analysis of the answers allowed understanding that certain symptoms or discomforts experienced by participants did not negatively influence their perception of their health status but reflect limitations in their daily activities. Finally, it is also indicated that mental health issues exist as barriers to daily activities, although they are difficult to explain by the participants.
3.3. Health Care Services
This sub-section provides data on the health care services variable regarding “self-reported unmet needs to medical care” (i.e., self-assessment of individual health care services—medical examination or treatment excluding dental care—provided by health professionals according to national health care systems”) [57]. We also analyze and systematize the 28 OECD Country Health Profiles regarding health care accessibility.
3.3.1. Self-Reported Unmet Needs for Medical Examination
In the next table, we provide data by group of citizenship in European Union-28, Euro Area-19 and Portugal (Table 3). Data for 2019 show that most of the immigrant population in Portugal (97.4 pp) did not declare reasons for unmet needs for medical examination or treatment. These values remain practically the same in 2020, with only a decrease of 0.1%. Among the foreign population, citizens from European Union countries show an increase in this indicator from 2019 to 2020 (96.4 pp to 98.1 pp, respectively). The values for Portugal are very similar to the average of the European Union and the Euro Zone.
As for the reasons associated with the need for medical examination or treatment, the 2019 data show that most categories have values below 0.5%, except for about 1.4% of the national population and 1.3% of the foreign population who mentioned “too expensive”. Still, regarding this reason, it is mainly the immigrant population from the European Union that stated it the most in 2019 (2.6 pp), although this figure drops to less than half in 2020 (0.7 pp).
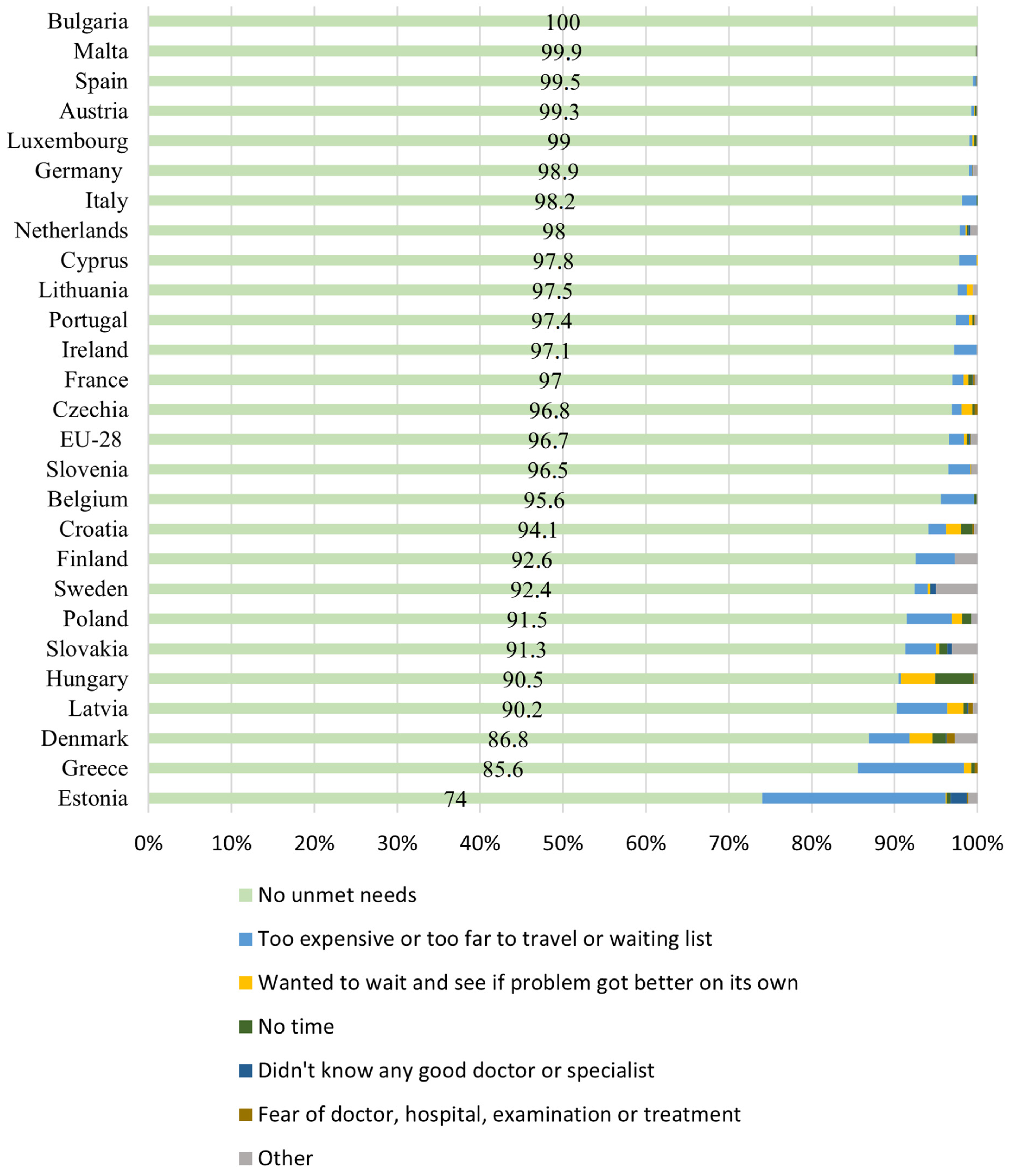
In 2019, we observed that more than 9 out of 10 foreign people in the European Union (96.7 pp) declared not having unmet needs for medical examination or treatment. This is a reality in most countries of the European Union (Figure 4).
The countries scoring less well on this indicator are Estonia (74 pp) and Greece (85.6 pp), the main reasons being “too expensive or too far to travel or waiting list” (22.1 pp and 12.8 pp, respectively). This is the main reason identified as a barrier to accessing health care, although the EU-28 average is only 1.8 pp. We have not included information for Romania in this figure, as the most recent data available from Eurostat is for 2011.
Other reasons noted in this indicator, but less significantly, relate to foreign people who “wanted to wait and see if problem got better on its own” (EU-28 mean = 0.3 pp). Countries such as Hungary (4.1 pp) and Denmark (2.8 pp) are where this reason was most frequently mentioned by foreigners.
As for the data we collected from our survey, we observed that there is a big difference compared to the Eurostat data. Contrary to the European portrait presented, 42.2% of the participants responded that they did not use medical services even when they needed them. It is important to note that on this question, these responses were mainly from women (61.9%) and immigrants from South America (37.2%) and Africa (34.9%).
Among the participants who indicated reasons, the main reasons for unmet medical needs were 13.8% “could not afford to” (too expensive or not covered by the SNS) or “waiting list” (13.8%); 13.7% “have no time” (e.g., because of work, care for children or for others), 8.8% “other reasons not specified”; 4.9% “wanted to wait and see if the problem got better on its own” and 1% “did not know any good doctor or specialist”.
Although there were health situations in which participants did not seek medical care, 69.6% stated having resorted to it, with 62.7% of them mentioning medical examination or treatment. In the total number of participants that used health services in the last year, 41.2% used the National Health System, 17.6% used the private sector and 10.8% used both (public and private).
The participants who utilized the private sector were mostly immigrants from South America (50%) and Europe (44.4%). Although not directly asked, in the open-ended response regarding the reasons for accessing health services, one third of these participants who used the private sector shared their dissatisfaction or lack of trust in public services.
“Due to leg injuries [reason for going to the health services]. I would add that it is extremely difficult to get health care through the NHS. I haven’t had a family doctor for 8 years and in my health center (Cacém), it is almost impossible to make an appointment, as the appointments only open once a month and quickly run out” (ID 57, female, Europe).
“Due to pain in the knees, neck and that prevented me from having a day with normal activity. Lupus under investigation in the private sector, because in the public sector I haven’t been able to get an appointment for years” (ID 89, female, South America).
There were also examples of those who resorted to the National Health Service, but mentioned a lack of conditions for timely and quality medical care.
“Performing exams, but I did it in the private one because of the waiting time, which was very long in the national service since there was broken equipment...” (ID 88, female, South America).
“To get vaccinated. Otherwise, only the rich have access to doctors. Those who don’t have money die waiting at the public” (ID 100, male, Europe).
We also point out that the lack of access to mental health care was mentioned by a participant who indicated that she was not followed up after an anxiety crisis, because she did not have a family doctor (ID 66, female, South America). However, most immigrants reported having used health care through the National Health Service for different reasons (e.g., hospital medical care, primary health care, long-term care, etc.) and did not mention any additional accessibility barriers.
3.3.2. Migrant Health Care Access in European Union
In order to complete the statistical information, we systematized the available data from the Country Health Profiles by the OECD/European Observatory on Health Systems and Policies for the 28 countries of the European Union (Table 4). Not all the reports contain the accessibility information for the different categories of foreign population (e.g., irregular migrants, refugees, asylum seekers). From this analysis, no explicit results were obtained for the foreign population in the reports on 8 countries: Croatia, Denmark, Hungary, Ireland, Latvia, Lithuania, The Netherlands and Poland.
Thus, we understand that although there are countries where there is good health system coverage and access to health care, foreign citizens still encounter some exclusion factors. Irregular immigrants are one group with the least guaranteed right to health care.
In Portugal, protection is extended to all citizens without discriminating on the basis of socio-economic situation or legal status. However, it was found that although irregular immigrant citizens have access to the public health system, there are factors that limit the full guarantee to medical care.
The Portugal Country Health Profile 2019, State of Health in the EU [45] indicates that despite the reduction of barriers in accessibility to health care and the decrease in unmet medical care needs declared by people, citizens still have to undertake relatively high expenses. However, the Portuguese National Health System is universal for all residents without discriminating against their socioeconomic status, professional situation or legal status. The system is financed by the State Budget and does not charge citizens, allowing tendentially free access. Thus, this report states that “All immigrants who are in Portugal for over 90 days have access to GP services, irrespective of their legal status. There are no restrictions for pregnant women, children, people with infectious diseases or those needing urgent care. While the NHS covers all residents in Portugal, there are barriers that, indeed, prevent immigrants from accessing NHS services, including language and cultural differences” [45] (p. 16).
3.4. Health Care during COVID-19
According to the European Centre for Disease Prevention and Control, there are risk factors for increased exposure to COVID-19 in migrant populations, which are disproportionately represented in COVID-19 cases, as well as evident low COVID-19 vaccination rates in some migrant and ethnic minority groups in the EU [53]. This technical report identified risk factors of the migrant population in Europe with higher COVID-19 morbidity and mortality, namely occupational risk factors, overcrowded accommodation and barriers to public health messaging. Additional factors are also mentioned, such as comorbidities and barriers or exclusion from health systems, in line with the data that was presented in the previous sections.
In this section, we describe the exceptional and temporary measures that were implemented in order to promote access to health care for the immigrant population in Portugal during the current pandemic. One of these measures was the extension of the validity period of identification documents, namely visas or residence permits, thus safeguarding citizens’ rights; even if these documents have expired, they remain valid for the citizen’s regular stay in Portugal (Decree-Law no. 10-A/2020). New guidelines were established in the legislation in force to mitigate the side effects of the pandemic, mainly with the immigrant population residing in Portugal, which simplified the existing bureaucratic processes and procedures and allowed for an alternative to the suspension of appointments at any embassy, registry office, consulate or other immigration services.
Moreover, with the publication of Decree-Law no. 12-A/2020 of 6 April 2020, and given the situation of public health emergency, procedures within the scope of health care were altered. These include the exemption from fees and changes in health services related to the diagnosis and treatment of COVID-19, such as free laboratory tests to detect the disease, as well as follow-ups after doctor appointments or urgent medical care.
One measure implemented was also the temporary regularization of immigrant citizens with processes pending at SEF (Order no. 3863-B/2020), i.e., all those who have started the regularization request by registering or requesting an expression of interest and are thus awaiting the attribution of a residence permit—this being the document that guarantees the regularization of legal stay in Portugal. This measure allowed a simplification of administrative processes and easier access to goods and services, such as obtaining a National Health System user number, assistance with health and hospital care, and the possibility of integration in eligibility lists for vaccination, especially against COVID-19.
Order no. 5793-A/2020 of 26 May has simplified the procedures for the granting of a residence permit, and it is now possible to apply for a renewal automatically via the SEF portal www.sapa.sef.pt (accessed on 18 February 2022), therefore eliminating the need to go in person and avoiding large crowds in these services. Another relevant change is that it is no longer needed to present the previous documents for residence permit renewal, as they are already available in each citizen’s database.
The High Commission for Migrations announced that all migrants in Portugal were eligible for vaccination in the open house modality (i.e., without prior appointment), even without a National Health Service user number. For this, it would only be necessary to present the documentation they possess attesting to their identity. This information was disclosed digitally in different languages (Arabic, Spanish, French, Hindi, English, Mandarin, Nepali, Portuguese, Romanian, Russian, Thai and Ukrainian).
However, only 14.7% of the participants in our study reported using health services for issues related to COVID-19 or the vaccination process. All those who reported medical care related to COVID-19 were only seen in the national health care system. There were participants who indicated unawareness of these measures, as they refer that they did not access the health services due to lack of documentation, namely for not having a user number. As regards to the lack of confidence mentioned in the previous section, this issue is also pointed out by the European Centre for Disease Prevention and Control as one reason that may contribute to lower uptake of the COVID-19 vaccine [53].
4. Discussion
Within the European framework, Portugal presents an intermediate position in terms of health status indicators. We have identified that these results are in line with the latest MIPEX assessments in which Portuguese policies on immigrant integration are quite positive, except in some areas such as the health indicator, where there is still room for improvement. The OECD data points to an extended protection in access to the National Health Service, which includes irregular immigrants. One of the contradictory aspects is that although policies protect these citizens, in reality, there are barriers preventing access to medical care. These include linguistic and cultural barriers, but also administrative barriers and reasons associated with low living conditions. Therefore, we can see that the country’s assessments according to MIPEX could be more favorable if there were greater investment in policies to promote better health care for the immigrant population.
The evolution of health policies has been an important factor in the integration of immigrants in Portugal and in Europe. Nevertheless, in the legal framework, we observed that most policies are for the general population, and attention to the health of migrants or ethnic minorities is not always prioritized. In Portugal, these issues should be subject to analysis, considering the Portuguese Constitutional Law that grants universal and non-discrimination access to health rights and the new Health Law that affirms the role of the National Health Service in guaranteeing this right.
Using Eurostat data, we can reach some conclusions on the conditions and access to health care of the immigrant population in Portugal and in Europe. In terms of health status, we can see that the foreign population in Portugal shows more favorable results than the native population in terms of a better self-perception of their health condition, as well as fewer diseases and health problems in this group. Compared to the data on the average of foreign citizens in the European Union, we understand that the immigrant population in Portugal presents better health indicators, except for the self-perception of their health condition.
When comparing the data from each 2020 indicator regarding the specific origin of the foreign population in Portugal, we understand that foreign people from European Union countries are those who indicate a more favorable perception of their health status, as well as fewer limitations to their usual activities due to illness. On the other hand, foreigners from countries outside the European Union have a less positive perception of health and are those who feel more limitations in their usual activities.
The Portuguese scenario indicates that in 2020, there was a slightly more favorable increase in the perception of native and foreign citizens, with foreign citizens from European Union countries being those who have a more favorable perception of their state of health. However, it should be noted that in Portugal, over one third of the foreign population reports suffering from chronic diseases, which shows that they need special attention regarding their health condition.
The data collected from our survey seems to point in another direction. The participants of this study presented a more positive perception of their health condition. However, they revealed a greater limitation in their daily activities and in seeking health services. It was also possible to register some complaints that should make us reflect on the public health system in Portugal. Since the pandemic started, its impacts have affected the national health system and could continue to worsen the waiting time and accessibility to health services.
One issue that stood out in our analysis was the amount of people who did not seek health services and care for different reasons. This question was the only one that was not followed by an open question because it had different response options according to the Eurostat survey, but for which we will conduct in-depth interviews in the next phase of the study. This question becomes relevant, as there were people who chose another reason for not seeking health services. These may be associated with linguistic, cultural and administrative difficulties that immigrants face, as well as the lack of health literacy and low educational level that hinder access to health services [2]. Although we have not collected data to confirm these statements, we believe that fighting the social inequalities that affect the immigrant population, namely in education [15], will allow greater access to health care. This becomes a necessary dimension of study, as the integration of immigrants through access to health care, mental health and health education are an added value for better policies, information and care among the population, and should be a strategic priority [58]. The indications of the European Centre for Disease Prevention and Control in the current pandemic context reinforce the need for strategies that include adapted public health messages co-designed and targeted at different cultures and in the main languages of the migrant communities.
The questionnaire data shows that there are immigrants who express a lack of trust and dissatisfaction with the responses from the public sector, although it is the national health system that ensures fair access to all citizens with these rights safeguarded in the constitution. The cultural dimension is relevant so that we can demystify taboos, mistrust and prejudices, as well as the lack of trust in the health system which are also considered important factors influencing the behavior of immigrants living in Europe [2].
Even during the pandemic, the results show it was possible to guarantee the provision of public health care to citizens, regardless of their economic condition and legal situation in the country. Portugal’s political efforts were recognized by the United Nations World Organization for its intervention and level of control of national contagions, as well as for implementing social and economic policy measures, internal planning and management, regarding the regularization of migrant’s temporary measurers [59]. We cannot ignore that the pandemic has enhanced inequalities in contemporary societies, being the migration status one of the main axes of inequality [60]. There are barriers to understanding in the use and evaluation of health information or services, which are essential if access is to be obtainable [2]. This issue is also related to the immigrants’ own living conditions, namely economic and housing precariousness [53,60]. Thus, there are aspects that, although not directly manifested in the health indicators, lead us to understand that it is necessary to invest in improving the living conditions of citizens. Due to the difficulty in accessing the right to health, there may also be constraints such as the existence of cultural differences, whether in terms of language, cultural habits or irregular situation in the country.
This study had an exploratory and descriptive nature, so there are limitations to be mentioned. One limitation is the fact that we used a small sample and it is not possible to generalize results or perform a more robust data analysis. Participants were selected by convenience, which also limited access to more vulnerable groups such as irregular immigrants. The number of questions presented was also restricted in order to seek coherence with the instrument used by Eurostat and to simplify completion by foreigners. Although we are aware of the aspects mentioned above, we seek to provide a view focused on a dimension of analysis of migrants’ health policies, health status and access to health in Portugal in the current context. This research highlights the importance of health policies to guarantee the rights of immigrant population. Furthermore, we consider it important that there is room for the analysis of open questions, which allowed for the construction of data collection instruments more directed towards this population. These will allow the elaboration of a wider questionnaire and interviews in a future phase of this research project. This information may also be useful to other researchers or health or social sector professionals. It should be noted that new research should focus on the voice of immigrants, seeking to collect in-depth information on the barriers, potential and challenges in accessing health care.
5. Conclusions
The improvement of access to health for the most vulnerable, including combating stereotypes and discrimination, is a commitment of European countries [10]. The New Pact on Migration and Asylum recognizes that foreign-born persons often face integration challenges, and that actions and measures are needed to accompany migrants and their families for a successful social inclusion and integration process, including on issues related to health and medical care access [1]. Moreover, as stated in the European Action plan on Integration and Inclusion 2021–2027, “the challenge of integration and inclusion is particularly relevant for migrants, not only newcomers but some-times also for third-country nationals who might have naturalised and are EU citizen” [61] (p. 1), where host societies should play a key role for economic, social, cultural, and political integration and participation. We recognize the importance of the power and representativeness of a country’s decision-making bodies, as well as their impact on the guarantee of certain fundamental rights, such as the right to health care. The provision of and access to health services for migrants becomes a key issue in academic and political debate.
These topics are particularly relevant in the Portuguese framework, as the right to health is considered a fundamental right (Constitutional Law, no. 1/2015), and therefore should cover all citizens residing in the national territory. In this sense, the existence and functioning of the National Health Service, particularly in Portugal, represents an important advance in the achievement of social rights, allowing and facilitating the conditions of access to health care. It is essential to understand the right to health as universal and without discrimination. Future research must reflect on the impacts that may arise from barriers imposed on accessibility to health care, guaranteeing the promotion of human dignity, and the non-discrimination or categorization of people.
Author Contributions
Conceptualization, I.C.-M. and S.F.; methodology, I.C.-M. and S.F.; software, IC-M.; validation, I.C.-M. and S.F.; formal analysis, I.C.-M.; writing—original draft preparation, I.C.-M..; writing—review and editing, I.C.-M. and S.F.; supervision, I.C.-M.; project administration, I.C.-M.; funding acquisition, I.C.-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by national funds FCT—Fundação para a Ciência e a Tecnologia, I.P., grant number UIDB/04624/2020.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Centro Lusíada de Investigação em Serviço Social e Intervenção Social Coordination Board (14 December 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon request. The data are not publicly available due to privacy restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- European Commission. Comunicação da Comissão ao Parlamento Europeu, ao Conselho, ao Comité Económico e Social e ao Comité das Regiões sobre um novo Pacto em Matéria de Migração e Asilo. Bruxelas, 23.9.2020. COM(2020) 609 Final. 2020. Available online: https://eur-lex.europa.eu/resource.html?uri=cellar:85ff8b4f-ff13-11ea-b44f-01aa75ed71a1.0013.02/DOC_1&format=PDF (accessed on 18 February 2022).
- Ahmadinia, H.; Eriksson-Backa, K.; Nikou, S. Health-seeking behaviours of immigrants, asylum seekers and refugees in Europe: A systematic review of peer-reviewed articles. J. Doc. 2021, 78, 18–41. [Google Scholar] [CrossRef]
- Oliveira, C.R.; Peixoto, J.; Góis, P. A nova crise dos refugiados na Europa: O modelo de repulsão-atração revisitado e os desafios para as políticas migratórias. Rev. Bras. Estud. Popul. 2017, 34, 73–98. [Google Scholar] [CrossRef] [Green Version]
- Padilla, B.; Ortiz, A. Fluxos Migratórios em Portugal: Do BOOM migratório à desaceleração no contexto de crise—balanços e desafios. Rev. Interdiscip. Mobilidade Hum. 2012, 39, 159–184. [Google Scholar] [CrossRef]
- Sousa, C.U. A Europa no contexto global das migrações. In Janus—Anuário de Relações Exteriores 2018–2019; Observatório de Relações Exteriores da Universidade Autónoma de Lisboa: Lisboa, Portugal, 2019; pp. 10–11. [Google Scholar]
- OECD. Working Together for Local Integration of Migrants and Refugees, OECD Regional Development Studies; OECD Publishing: Paris, France, 2018. [Google Scholar] [CrossRef]
- Legido-Quigley, H.; Karanikolos, M.; Hernandez-Plaza, S.; de Freitas, C.; Bernardo, L.; Padilla, B.; Sá Machado, R.; Diaz-Ordaz, K.; Stuckler, D.; McKee, M. Effects of the financial crisis and Troika austerity measures on health and health care access in Portugal. Health Policy 2016, 120, 833–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padilla, B. Saúde e migrações: Metodologias participativas como ferramentas de promoção da cidadania. Interface-Comun. Saúde Educ. 2017, 21, 273–284. [Google Scholar] [CrossRef] [Green Version]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; UN: New York, NY, USA, 2015; Available online: https://sdgs.un.org/publications/transforming-our-world-2030-agenda-sustainable-development-17981 (accessed on 18 February 2022).
- European Commission. European Pillar of Social Rights Action Plan; Publications Office of the European Union: Luxembourg, 2021. [Google Scholar]
- European Union. Charter of Fundamental Rights of the European Union, 26 October 2012, 2012/C 326/02. Available online: https://www.refworld.org/docid/3ae6b3b70.html (accessed on 18 February 2022).
- Peixoto, J. Dinâmicas e regimes migratórios: O caso das migrações internacionais em Portugal. Análise Soc. 2007, 42, 445–469. [Google Scholar]
- Casquilho-Martins, I.; Belchior-Rocha, H.; Ferreira, J.M.L. Community Strategies for Intercultural Participation. Trab. Soc. Glob. 2020, 10, 157–179. [Google Scholar] [CrossRef]
- Góis, P.; Marques, J. Retrato de um Portugal migrante: A evolução da emigração, da imigração e do seu estudo nos últimos 40 anos. E-Cadernos CES 2018, 29, 125–152. [Google Scholar] [CrossRef] [Green Version]
- Casquilho-Martins, I.; Matela, T. Inequalities in access to education: A socio-educational intervention with migrant children and youth. In ICERI2021 Proceedings; IATED Academy: Valencia, Spain, 2021; pp. 6888–6895. [Google Scholar] [CrossRef]
- Martins, I.C.D. Políticas de Imigração e Integração: Intervenção do Serviço Social. Interv. Soc. 2015, 46, 57–75. [Google Scholar]
- Peixoto, J.; Iorio, J. Crise, Imigração e Mercado de Trabalho em Portugal: Retorno, regulação ou resistência? Princípia: Cascais, Portugal, 2011. [Google Scholar]
- Matias, A.R.; Pinto, P.F. Overcoming linguistic barriers in Portuguese higher education: The case of international African students. Port. J. Soc. Sci. 2020, 19, 189–214. [Google Scholar] [CrossRef]
- SEF/GEPF. Relatório de Imigração, Fronteiras e Asilo 2020; Serviço de Estrangeiros e Fronteiras: Oeiras, Portugal, 2021. [Google Scholar]
- Estrela, P. A saúde dos imigrantes em Portugal. Rev. Port. De Clínica Geral 2009, 25, 45–55. [Google Scholar] [CrossRef]
- Padilla, B. Saúde dos Imigrantes: Multidimensionalidade, desigualdades e acessibilidades em Portugal. Rev. Interdiscip. Mobilidade Hum. 2013, 21, 49–68. [Google Scholar] [CrossRef]
- Padilla, B.; Rodrigues, V.; Lopes, J.; Ortiz, A. Saúde dos imigrantes: Desigualdades e crise no SNS. In Desigualdades Sociais: Portugal e a Europa; Carmo, R., Sebastião, J., Azevedo, J., Martins, S.C., Costa, A.F., Eds.; Mundos Sociais: Lisboa, Portugal, 2018; pp. 315–334. [Google Scholar]
- Jordão, N.; Freitas, C.; Ramírez, M. Efeitos da crise económica e das políticas de austeridade na saúde e no acesso aos cuidados de saúde da população migrante em países do sul da Europa: Revisão scoping. Rev. Interdiscip. Mobilidade Hum. 2018, 26, 213–230. [Google Scholar] [CrossRef] [Green Version]
- Dias, S.; Gama, A.; Silva, A.; Cargaleiro, H.; Martins, M. Barreiras no acesso e utilização dos serviços de saúde pelos imigrantes: A perspetiva dos profissionais de saúde. Acta Med. Port. 2011, 24, 511–516. [Google Scholar] [PubMed]
- Heyman, J.; Congress, E. Health and Social Work: Practice, Policy and Research; Springer Publishing Company: New York, NY, USA, 2018. [Google Scholar]
- Gehlert, S.; Brownie, T. Handbook of Health Social Work; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2019. [Google Scholar]
- World Health Organization. Health Inequity and the Effects of COVID-19: Assessing, Responding to and Mitigating the Socioeconomic Impact on Health to Build a Better Future; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Tariq, S.; Woodman, J. Using mixed methods in health research. JRSM Short Rep. 2013, 4, 2042533313479197. [Google Scholar] [CrossRef] [PubMed]
- Bowen, G.A. Document Analysis as a Qualitative Research Method. Qual. Res. J. 2009, 9, 27–40. [Google Scholar] [CrossRef] [Green Version]
- Papanicolas, I.; Mossialos, E.; Gundersen, A.; Woskie, L.; Jha, A.K. Performance of UK National Health Service compared with other high income countries: Observational study. BMJ 2019, 367, l6326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalglish, S.; Khalid, H.; McMahon, S. Document analysis in health policy research: The READ approach. Health Policy Plan. 2020, 35, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- OECD/European Observatory on Health Systems and Policies. Austria: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Belgium: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Bulgaria: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Cyprus: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Czechia: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Estonia: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Finland: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. France: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Germany: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Greece: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Italy: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Luxembourg: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Malta: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Portugal: Country Health Profile 2019, State of Health in the EU European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Romania: Country Health Profile 2019, State of Health in the EU European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Slovakia: Country Health Profile 2019, State of Health in the EU European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Slovenia: Country Health Profile 2019, State of Health in the EU European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Spain: Country Health Profile 2019, State of Health in the EU, European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Sweden: Country Health Profile 2019, State of Health in the EU, European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. United Kingdom: Country Health Profile 2019, State of Health in the EU, European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- Solano, G.; Huddleston, T. Migrant Integration Policy Index 2020; CIDOB: Barcelona, Spain; MPG: Brussels, Belgium, 2020. [Google Scholar]
- European Centre for Disease Prevention and Control. Reducing COVID-19 Transmission and Strengthening Vaccine Uptake among Migrant Populations in the EU/EEA—3 June 2021; ECDC: Stockholm, Sweden, 2021. [Google Scholar]
- Migrant Integration Policy Index (MIPEX). Available online: https://www.mipex.eu/play/ (accessed on 5 December 2021).
- Eurostat. Glossary: Minimum European Health Module (MEHM). Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:Minimum_European_Health_Module_(MEHM) (accessed on 5 December 2021).
- Vilelas, J. Investigação: O Processo de Construção do Conhecimento, 3rd ed.; Edições Sílabo: Lisboa, Portugal, 2020. [Google Scholar]
- Eurostat. Health variables of EU-SILC Reference Metadata in Euro SDMX Metadata Structure (ESMS). Available online: https://ec.europa.eu/eurostat/cache/metadata/en/hlth_silc_01_esms.htm (accessed on 3 December 2021).
- International Organization for Migration. Summary Report on the MIPEX Health Strand and Country Reports; International Organization for Migration: Geneva, Switzerland, 2016. [Google Scholar]
- Food and Agriculture Organization of the United Nations. Migrant Workers and the COVID-19 Pandemic. 2020. Available online: http://www.fao.org/3/ca8559en/CA8559EN.pdf (accessed on 12 December 2021).
- Peixoto, J. O que nos ensina a pandemia sobre migrações internacionais? O caso português e o contexto mundial. In Migrações Internacionais e a Pandemia de COVID-19; Baeninger, R., Vedovato, L.R., Nandy, S., Eds.; NEPO/UNICAMP: Campinas, SP, Brasil, 2020; pp. 132–137. [Google Scholar]
- European Commission. Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of Region Action plan on Integration and Inclusion 2021–2027. Brussels, 24.11.2020. COM(2020) 758 Final. Available online: https://ec.europa.eu/migrant-integration/news/ec-reveals-its-new-eu-action-plan-integration-and-inclusion-2021-2027_en (accessed on 18 February 2022).
Figure 1.
Self-perceived health, foreign population in European Union countries (EU28), 2020 (%). Source: Eurostat—last data extracted on 5 December 2021 (online data code: HLTH_SILC_23).
Figure 1.
Self-perceived health, foreign population in European Union countries (EU28), 2020 (%). Source: Eurostat—last data extracted on 5 December 2021 (online data code: HLTH_SILC_23).

Figure 2.
People having a long-standing illness or health problem, foreign population, European Union countries (EU28), 2020 (%). Source: Eurostat—last data extracted on 5 December 2021 (online data code: HLTH_SILC_25).
Figure 2.
People having a long-standing illness or health problem, foreign population, European Union countries (EU28), 2020 (%). Source: Eurostat—last data extracted on 5 December 2021 (online data code: HLTH_SILC_25).

Figure 3.
Self-perceived long-standing limitations in usual activities due to health problem, foreign population, European Union countries (EU28), 2020 (%). Source: Eurostat—last data extracted on 5 December 2021 (online data code: HLTH_SILC_27).
Figure 3.
Self-perceived long-standing limitations in usual activities due to health problem, foreign population, European Union countries (EU28), 2020 (%). Source: Eurostat—last data extracted on 5 December 2021 (online data code: HLTH_SILC_27).

Figure 4.
Self-reported unmet needs for medical examination by main reason declared, foreign population in European countries, 2019 (%). Source: Eurostat—last data extracted on 5 December 2021 (online data code: HLTH_SILC_29).
Figure 4.
Self-reported unmet needs for medical examination by main reason declared, foreign population in European countries, 2019 (%). Source: Eurostat—last data extracted on 5 December 2021 (online data code: HLTH_SILC_29).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Statistical indicators, time, geopolitical territory and source of data.
| Indicators—Variables | Time | Geopolitical Territory | Source |
|---|---|---|---|
| Health status—Self-perceived health (%) | 2019–2020 | European Union—28 countries | Eurostat |
| Health status—People having a long-standing illness or health problem (%) | 2019–2020 | European Union—28 countries | Eurostat |
| Health status—Self-perceived long-standing limitations in usual activities due to health problem (%) | 2019–2020 | European Union—28 countries | Eurostat |
| Health care—Self-reported unmet needs for medical examination by main reasons declared (%) | 2019–2020 | European Union—28 countries | Eurostat |
| Migrant Integration Policy—Overall score (index) | 2019 | European Union—28 countries | Mipex |
| Migrant Integration Policy—Overall score with health (index) | 2019 | European Union—28 countries | Mipex |
| Migrant Integration Policy—Health (index) | 2019 | European Union—28 countries | Mipex |
Table 2.
Migrant Integration Policy, European Union Countries (EU28), 2019 (index 0–100).
| Integration Policy Indicators | |||
|---|---|---|---|
| Geopolitical Territory | Overall Score (with Health) | Overall Score | Health |
| Sweden | 86 | 87 | 83 |
| Finland | 85 | 87 | 67 |
| Portugal | 81 | 84 | 65 |
| Belgium | 69 | 69 | 73 |
| Ireland | 64 | 61 | 85 |
| Luxembourg | 64 | 66 | 46 |
| Spain | 60 | 57 | 81 |
| Germany | 58 | 58 | 63 |
| Italy | 58 | 55 | 79 |
| Netherlands | 57 | 56 | 65 |
| France | 56 | 55 | 65 |
| United Kingdom | 56 | 54 | 75 |
| Czechia | 50 | 48 | 61 |
| Estonia | 50 | 53 | 29 |
| Denmark | 49 | 48 | 56 |
| Romania | 49 | 50 | 46 |
| EU28 | 49 | 50 | 53 |
| Malta | 48 | 47 | 56 |
| Slovenia | 48 | 50 | 33 |
| Austria | 46 | 41 | 81 |
| Greece | 46 | 46 | 48 |
| Hungary | 43 | 45 | 29 |
| Cyprus | 41 | 41 | 36 |
| Bulgaria | 40 | 41 | 29 |
| Poland | 40 | 42 | 27 |
| Croatia | 39 | 41 | 27 |
| Slovakia | 39 | 37 | 50 |
| Latvia | 37 | 38 | 31 |
| Lithuania | 37 | 38 | 31 |
Meaning of scores: 80–100—Favorable; 60–79—Slightly favorable; 41–59—Halfway favorable; 21–40—Slightly unfavorable; 1–20—Unfavorable; 0—Critically unfavourable. Source: Migrant Integration Policy Index (MIPEX) online tool available at: https://www.mipex.eu/play/ (accessed on 5 December 2021).
Table 3.
Self-reported unmet needs for medical examination (main reasons declared) by group of citizenship, European Union, Euro Area and Portugal, 2019–2020 (%).
Table 3.
Self-reported unmet needs for medical examination (main reasons declared) by group of citizenship, European Union, Euro Area and Portugal, 2019–2020 (%).
| 2019 | 2020 | ||||
|---|---|---|---|---|---|
| EU28 | EA19 | PT | PT | ||
| Too expensive | Foreign population (total) | 1 | 1 | 1.3 | 1.1 |
| Foreign population (Non-EU28 countries) | 1.1 | 1.2 | 1 | 1.2 | |
| Foreign population (EU28 countries) | 0.8 | 0.8 | 2.6 | 0.7 | |
| National population | 0.9 | 0.8 | 1.4 | 1.1 | |
| Too far to travel | Foreign population (total) | 0.1 | 0 | 0 | 0.1 |
| Foreign population (Non-EU28 countries) | 0.1 | 0 | 0 | 0 | |
| Foreign population (EU28 countries) | 0 | 0 | 0.1 | 0.3 | |
| National population | 0.1 | 0 | 0 | 0.1 | |
| No time | Foreign population (total) | 0.3 | 0.2 | 0.2 | 0.3 |
| Foreign population (Non-EU28 countries) | 0.3 | 0.2 | 0.1 | 0.4 | |
| Foreign population (EU28 countries) | 0.2 | 0.1 | 0.3 | 0 | |
| National population | 0.3 | 0.2 | 0.2 | 0.2 | |
| Didn’t know any doctor or specialist | Foreign population (total) | 0.1 | 0 | 0 | 0 |
| Foreign population (Non-EU28 countries) | 0.1 | 0.1 | 0 | 0 | |
| Foreign population (EU28 countries) | 0.1 | 0 | 0 | 0 | |
| National population | 0.1 | 0 | 0 | 0 | |
| Waiting list | Foreign population (total) | 0.8 | 0.3 | 0.2 | 0.2 |
| Foreign population (Non-EU28 countries) | 0.9 | 0.4 | 0.3 | 0.2 | |
| Foreign population (EU28 countries) | 0.7 | 0.3 | 0 | 0 | |
| National population | 1 | 0.5 | 0.3 | 0.5 | |
| Fear of doctor, hospital, examination or treatment | Foreign population (total) | 0.1 | 0.1 | 0.1 | 0 |
| Foreign population (Non-EU28 countries) | 0.1 | 0.1 | 0.1 | 0 | |
| Foreign population (EU28 countries) | 0.1 | 0.1 | 0.1 | 0 | |
| National population | 0.1 | 0.1 | 0.3 | 0.3 | |
| Wanted to wait and see if the problem got better on its own | Foreign population (total) | 0.3 | 0,2 | 0,4 | 0.2 |
| Foreign population (Non-EU28 countries) | 0.3 | 0,2 | 0,5 | 0.1 | |
| Foreign population (EU28 countries) | 0.2 | 0,1 | 0,1 | 0.5 | |
| National population | 0.6 | 0,3 | 0,4 | 0.3 | |
| No unmet needs to declare | Foreign population (total) | 96.7 | 97.8 | 97.4 | 97.3 |
| Foreign population (Non-EU28 countries) | 96.4 | 97.6 | 97.7 | 97 | |
| Foreign population (EU28 countries) | 97 | 98.2 | 96.4 | 98.1 | |
| National population | 96.5 | 97.9 | 97.3 | 96 | |
Source: Eurostat—last data extracted on 5 December 2021 (online data code: HLTH_SILC_29).
Table 4.
Migrant health care access in European Union countries (EU28).
| Country | Health Profiles 2019 |
|---|---|
| Austria | Population coverage by health system is near-universal, including registered asylum seekers. Asylum seekers have good accessibility to outpatient clinics in public hospitals. A small number of people remain uninsured, including irregular migrants [32]. |
| Belgium | Large population covered for health services. Asylum seekers are entitled to medical care as the responsibility of reception centers that pays for any needed medical services. Irregular migrants are not covered and are excluded from the population covered because of the lack of legal resident authorization or regular address [33]. |
| Bulgaria | Lack of health system coverage as barrier to access to medical care for a considerable proportion of the population. Irregular migrants and population without a valid ID card (are not covered) [34]. |
| Cyprus | Only three quarters of residents are being covered free of charge to access the public health service (under the old system). The new General Health Care System aims to provide health coverage for third country nationals with legal residence and documented asylum seekers [35]. |
| Czechia | Most of the population benefited from the health system which is linked to permanent residence. Asylum seekers are also covered, but non-EU population, who are not employed or self-employed in Czechia, must purchase private health insurance to be allowed to stay in the country and have access to health care [36]. |
| Estonia | Many populations have not been granted access for their health needs. The non-Estonian-speaking population, near a quarter of the population, is more likely to be uninsured for health access [37]. |
| Finland | Public health services are provided to all permanent residents if they are registered as residents in one of the municipalities. Irregular immigrants and asylum seekers who have not been granted asylum are the only people not covered by health services [38]. |
| France | The public health system covers most of the population, including costs for medical services provided in and outside hospitals. Irregular immigrants have access to a standard health benefit package [39]. |
| Germany | Health system coverage is mostly universal with a broad social benefit to population. Refugees, asylum seekers and irregular migrants have limited coverage and access to health care services, depending on their individual status [40]. |
| Greece | Universal coverage for health care for all population. Irregular migrants and asylum seekers (until they receive refugee status) and Roma population face further barriers in access to health services [41]. |
| Italy | Nearly all resident populations have automatic coverage of health services, including legal foreign residents, and have access to universal health care and medical services. Irregular immigrants’ access to health coverage in urgent and essential services [42]. |
| Luxembourg | Good coverage for health services to resident population with limitations for some vulnerable population groups, such as third-country nationals, for who inequalities to health access are higher [43]. |
| Malta | All resident population are covered by health system, as well as refugees and asylum seekers with a good population coverage. Free health care includes migrants, but with exclusions for those who are not entitled to work in the formal sector [44]. |
| Portugal | Residents are covered by health system, including all immigrants (who are in Portugal for more than 90 days) regardless of their legal status. Irregular migrants have granted access to public health services but face some barriers such as language and cultural differences [45]. |
| Romania | Health system aims to provide universal coverage. Those who are not covered by health system have access to a restricted minimum benefit package. The number of population without coverage is difficult to quantify (data are reported for the general population only and statistics by ethnic group is prohibited), but people without an identification document are excluded from statutory coverage [46]. |
| Slovakia | Health system provides a comprehensive benefit package to nearly the entire population and is generally good, though hospital-centric. The Roma have guaranteed access to health care on equal terms, but with a low use of health services marked by limitations such as language, cultural and information barriers, and discrimination [47]. |
| Slovenia | Mostly all population residents are covered by health system if having permanent residency. Undocumented migrants, ethnic minorities and people with difficulty to meet formal residency requirements are excluded from health care access [48]. |
| Spain | Nearly all populations have access to health services provided and covered by the health system, but irregular migrants and asylum seekers face greater barriers in accessing health care [49]. |
| Sweden | All residents are automatically entitled to public health services, including new immigrants, and access to health care is generally good [50]. |
| United Kingdom | Health services are granted to people who are normal residents. Access to services is based on need rather than ability to pay. Irregular migrants have a limited benefit package that covers some health care. Non-European Economic Area migrants (until they have been awarded ‘indefinite leave to remain’) are required to pay for health services, but refugees and asylum seekers have free access to it [51]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Casquilho-Martins, I.; Ferreira, S. Migrants’ Health Policies and Access to Health Care in Portugal within the European Framework. Societies 2022, 12, 55. https://0-doi-org.brum.beds.ac.uk/10.3390/soc12020055
AMA Style
Casquilho-Martins I, Ferreira S. Migrants’ Health Policies and Access to Health Care in Portugal within the European Framework. Societies. 2022; 12(2):55. https://0-doi-org.brum.beds.ac.uk/10.3390/soc12020055
Chicago/Turabian StyleCasquilho-Martins, Inês, and Soraia Ferreira. 2022. "Migrants’ Health Policies and Access to Health Care in Portugal within the European Framework" Societies 12, no. 2: 55. https://0-doi-org.brum.beds.ac.uk/10.3390/soc12020055
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.