
Effects of Respiratory Muscle Warm-up on High-Intensity Exercise Performance


Abstract
:1. Introduction
2. Materials and Method
2.1. Study Design
2.2. Study Controls
2.3. Participants

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean ± SD |
|---|---|
| Age (y) | 24.9 ± 4.2 |
| Height (cm) | 178.8 ± 9.0 |
| Mass (kg) | 78.5 ± 10.4 |
| Body Fat (%) | 13.4 ± 4.2 |
| VO2max (mL·kg−1·min−1) | 54.8 ± 6.9 |
| Cycling Intensity (W) | 274.5 ± 45.8 |
2.4. Preliminary Testing
2.5. Experimental Trials

2.6. Statistical Analyses
3.Results
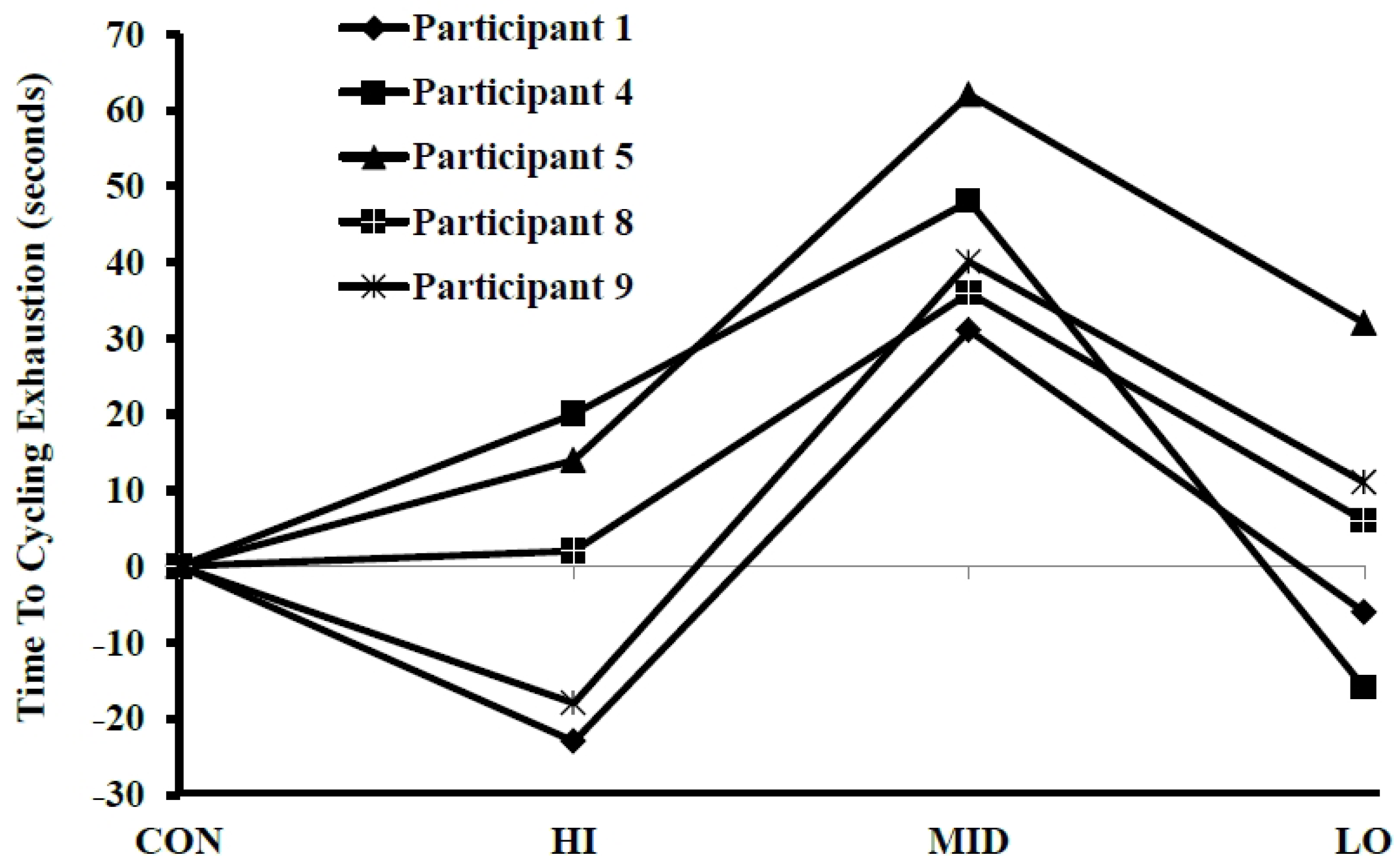
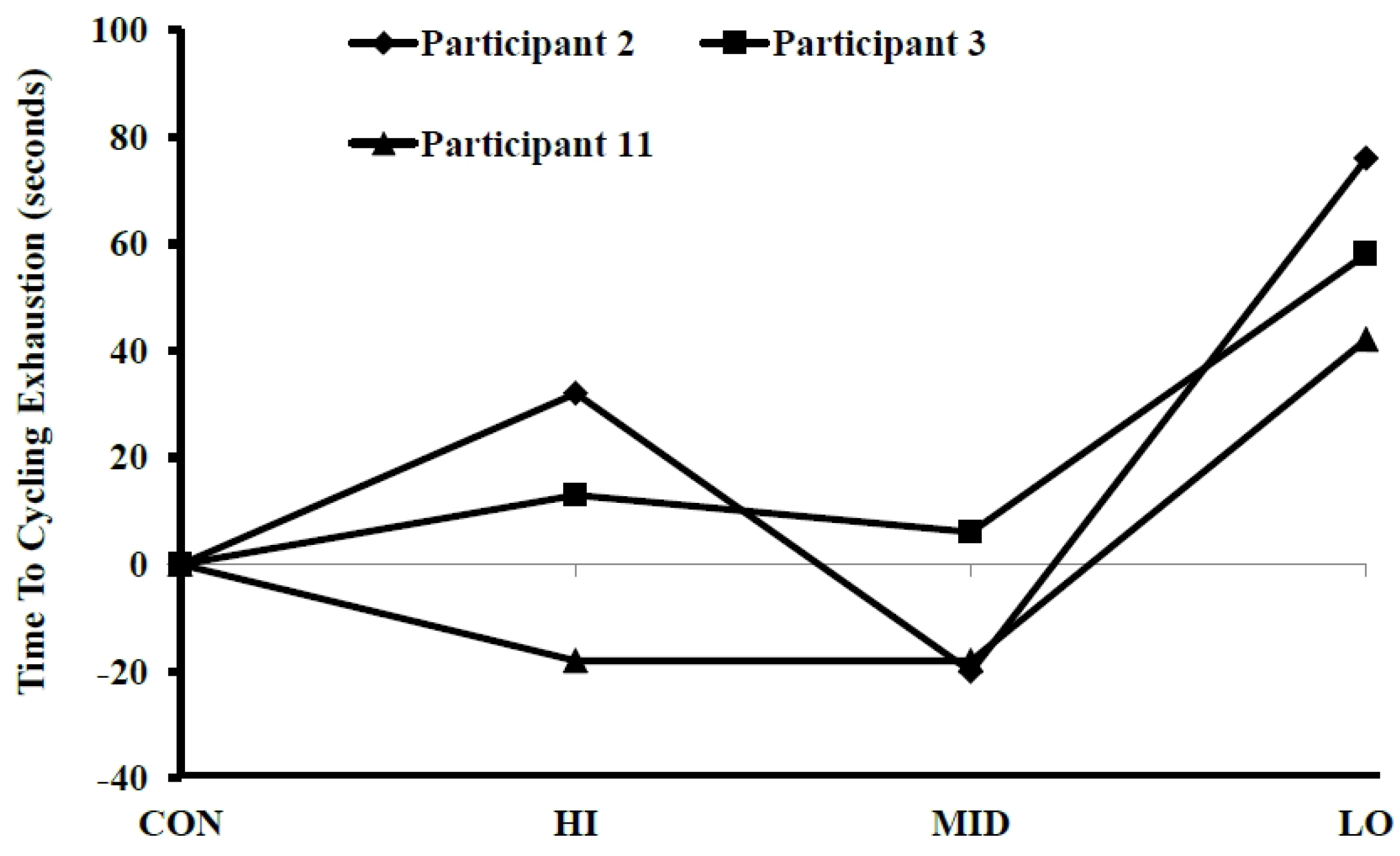
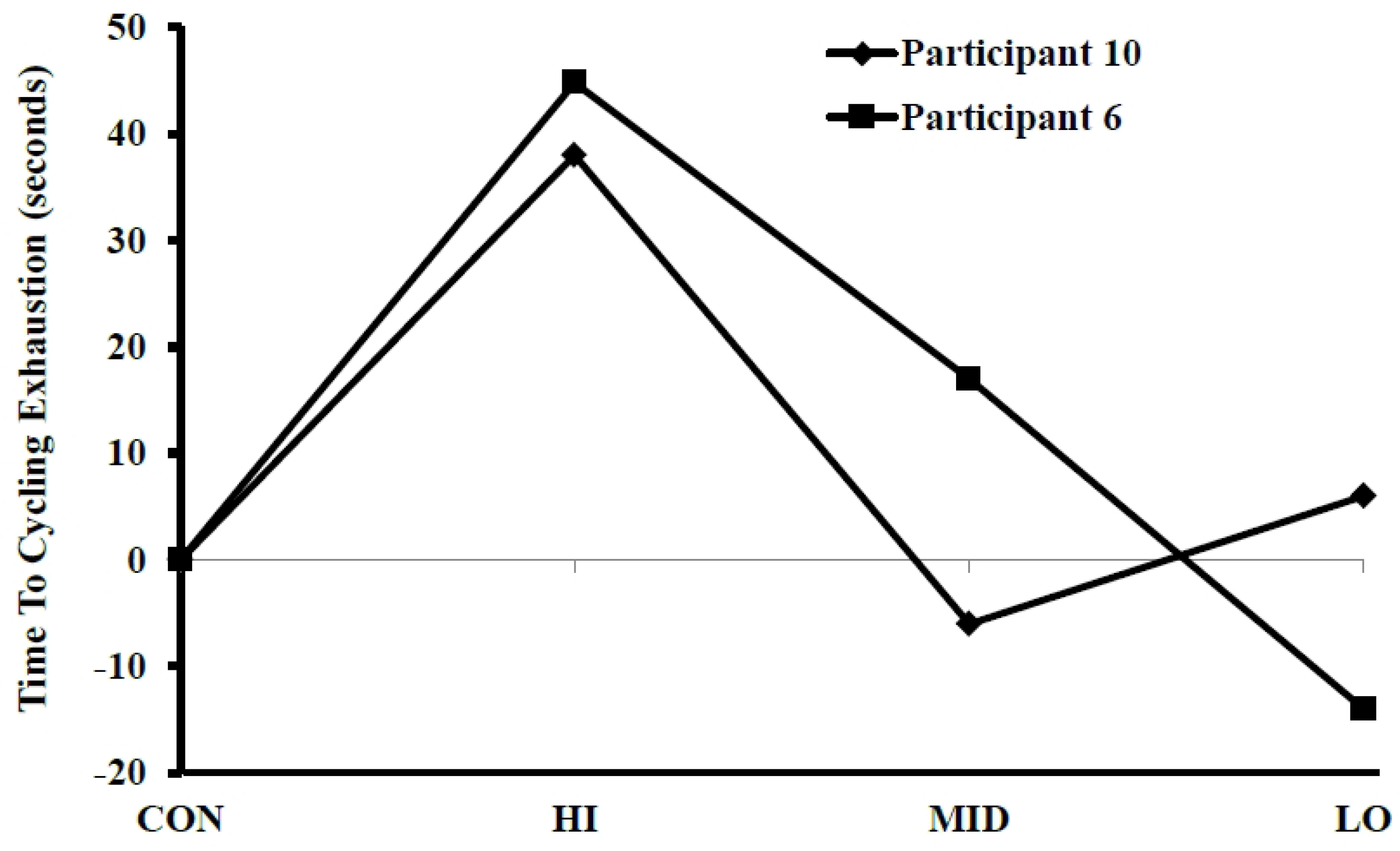
3.1. Time to Exhaustion



3.2. Rating of Perceived Exertion and Lactate
| Condition | Pre | Post |
|---|---|---|
| HI | 1.95 ± 0.56 | 15.38 ± 4.49 |
| MID | 1.91 ± 0.40 | 15.80 ± 4.03 |
| LOW | 2.17 ± 0.82 | 13.74 ± 4.14 |
| CON | 1.88 ± 0.47 | 14.20 ± 3.70 |
3.3. Pulmonary Function
3.4. Gas Exchange
4. Discussion
4.1. Performance
4.2. Metabolic Function
4.3. Blood Lactate and Pulmonary Function
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mador, M.J.; Acevedo, F.A. Effect of respiratory muscle fatigue on subsequent exercise performance. J. Appl. Physiol. 1991, 70, 2059–2065. [Google Scholar] [PubMed]
- Verges, S.; Sager, Y.; Erni, C.; Spengler, C.M. Expiratory muscle fatigue impairs exercise performance. Eur. J. Appl. Physiol. 2007, 101, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Romer, L.M.; Polkey, M.I. Exercise-induced respiratory muscle fatigue: Implications for performance. J. Appl. Physiol. 2008, 104, 879–888. [Google Scholar] [CrossRef] [PubMed]
- Volianitis, S.; McConnell, A.K.; Jones, D.A. Assessment of maximum inspiratory pressure. Prior submaximal respiratory muscle activity (“warm-up”) enhances maximum inspiratory activity and attenuates the learning effect of repeated measurement. Respir. Int. Rev. Thorac. Dis. 2001, 68, 22–27. [Google Scholar]
- Dempsey, J.A.; Romer, L.; Rodman, J.; Miller, J.; Smith, C. Consequences of exercise-induced respiratory muscle work. Respir. Physiol. Neurobiol. 2006, 151, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.M. Discharge of group iv phrenic afferent fibers increases during diaphragmatic fatigue. Brain Res. 2000, 856, 240–244. [Google Scholar] [CrossRef]
- Jammes, Y.; Balzamo, E. Changes in afferent and efferent phrenic activities with electrically induced diaphragmatic fatigue. J. Appl. Physiol. 1992, 73, 894–902. [Google Scholar] [PubMed]
- Harms, C.A.; Babcock, M.A.; McClaran, S.R.; Pegelow, D.F.; Nickele, G.A.; Nelson, W.B.; Dempsey, J.A. Respiratory muscle work compromises leg blood flow during maximal exercise. J. Appl. Physiol. 1997, 82, 1573–1583. [Google Scholar] [PubMed]
- Sheel, A.W.; Derchak, P.A.; Morgan, B.J.; Pegelow, D.F.; Jacques, A.J.; Dempsey, J.A. Fatiguing inspiratory muscle work causes reflex reduction in resting leg blood flow in humans. J. Physiol. 2001, 537, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Verges, S.; Lenherr, O.; Haner, A.C.; Schulz, C.; Spengler, C.M. Increased fatigue resistance of respiratory muscles during exercise after respiratory muscle endurance training. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2007, 292, R1246–R1253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verges, S.; Renggli, A.S.; Notter, D.A.; Spengler, C.M. Effects of different respiratory muscle training regimes on fatigue-related variables during volitional hyperpnoea. Respir. Physiol. Neurobiol. 2009, 169, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Romer, L.M.; McConnell, A.K.; Jones, D.A. Inspiratory muscle fatigue in trained cyclists: Effects of inspiratory muscle training. Med. Sci. Sports Exerc. 2002, 34, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Volianitis, S.; McConnell, A.K.; Koutedakis, Y.; Jones, D.A. Specific respiratory warm-up improves rowing performance and exertional dyspnea. Med. Sci. Sports Exerc. 2001, 33, 1189–1193. [Google Scholar] [CrossRef] [PubMed]
- Wilson, E.E.; McKeever, T.M.; Lobb, C.; Sherriff, T.; Gupta, L.; Hearson, G.; Martin, N.; Lindley, M.R.; Shaw, D.E. Respiratory muscle specific warm-up and elite swimming performance. Br. J. Sports Med. 2013, 48, 789–791. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Tong, T.K.; Huang, C.; Nie, J.; Lu, K.; Quach, B. Specific inspiratory muscle warm-up enhances badminton footwork performance. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2007, 32, 1082–1088. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.F.; Tong, T.K.; Kuo, Y.C.; Chen, P.H.; Huang, H.W.; Lee, C.L. Inspiratory muscle warm-up attenuates muscle deoxygenation during cycling exercise in women athletes. Respir. Physiol. Neurobiol. 2013, 186, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Tong, T.K.; Fu, F.H. Effect of specific inspiratory muscle warm-up on intense intermittent run to exhaustion. Eur. J. Appl. Physiol. 2006, 97, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Lomax, M.; Grant, I.; Corbett, J. Inspiratory muscle warm-up and inspiratory muscle training: Separate and combined effects on intermittent running to exhaustion. J. Sports Sci. 2011, 29, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Roussos, C.S.; Macklem, P.T. Diaphragmatic fatigue in man. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1977, 43, 189–197. [Google Scholar] [PubMed]
- Armstrong, L.E.; Maresh, C.M.; Castellani, J.W.; Bergeron, M.F.; Kenefick, R.W.; LaGasse, K.E.; Riebe, D. Urinary indices of hydration status. Int. J. Sport Nutr. 1994, 4, 265–279. [Google Scholar] [PubMed]
- Jackson, A.S.; Pollock, M.L. Practical assessment of body composition. Phys. Sports Med. 1985, 13, 76–90. [Google Scholar]
- American College of Sports Medicine. Acsm’s Guidelines for Exercise Testing and Prescription, 7th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; p. 366. [Google Scholar]
- Ghosh, A.K.; Rahaman, A.A.; Singh, R. Combination of sago and soy-protein supplementation during endurance cycling exercise and subsequent high-intensity endurance capacity. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 216–223. [Google Scholar] [PubMed]
- Ferguson-Stegall, L.; McCleave, E.L.; Ding, Z.; Kammer, L.M.; Wang, B.; Doerner, P.G.; Liu, Y.; Ivy, J.L. The effect of a low carbohydrate beverage with added protein on cycling endurance performance in trained athletes. J. Strength Cond. Res. 2010, 24, 2577–2586. [Google Scholar] [CrossRef] [PubMed]
- Volianitis, S.; McConnell, A.K.; Koutedakis, Y.; Jones, D.A. The influence of prior activity upon inspiratory muscle strength in rowers and non-rowers. Int. J. Sports Med. 1999, 20, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.A.; Gregson, I.R.; Mills, D.E.; Gonzalez, J.T.; Sharpe, G.R. Inspiratory muscle warm-up does not improve cycling time-trial performance. Eur. J. Appl. Physiol. 2014, 114, 1821–1830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, L.M.; Heigenhauser, G.J.; Paterson, D.H.; Kowalchuk, J.M. Effect of voluntary hyperventilation with supplemental CO2 on pulmonary O2 uptake and leg blood flow kinetics during moderate-intensity exercise. Exp. Physiol. 2013, 98, 1668–1682. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.L.; Bourdillon, N.; Kayser, B. Effect of end-tidal CO2 clamping on cerebrovascular function, oxygenation, and performance during 15-km time trial cycling in severe normobaric hypoxia: The role of cerebral O2 delivery. Physiol. Rep. 2013, 1. [Google Scholar] [CrossRef] [PubMed]
- Enright, S.J.; Unnithan, V.B.; Heward, C.; Withnall, L.; Davies, D.H. Effect of high-intensity inspiratory muscle training on lung volumes, diaphragm thickness, and exercise capacity in subjects who are healthy. Phys. Ther. 2006, 86, 345–354. [Google Scholar] [PubMed]
- Kilding, A.E.; Brown, S.; McConnell, A.K. Inspiratory muscle training improves 100 and 200 m swimming performance. Eur. J. Appl. Physiol. 2010, 108, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Romer, L.M.; McConnell, A.K. Specificity and reversibility of inspiratory muscle training. Med. Sci. Sports Exerc. 2003, 35, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.; Kavuru, M.S. A practical guide for peak expiratory flow monitoring in asthma patients. Clevel. Clin. J. Med. 1997, 64, 195–202. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thurston, T.S.; Coburn, J.W.; Brown, L.E.; Bartolini, A.; Beaudette, T.L.; Karg, P.; McLeland, K.A.; Arevalo, J.A.; Judelson, D.A.; Galpin, A.J. Effects of Respiratory Muscle Warm-up on High-Intensity Exercise Performance. Sports 2015, 3, 312-324. https://0-doi-org.brum.beds.ac.uk/10.3390/sports3040312
Thurston TS, Coburn JW, Brown LE, Bartolini A, Beaudette TL, Karg P, McLeland KA, Arevalo JA, Judelson DA, Galpin AJ. Effects of Respiratory Muscle Warm-up on High-Intensity Exercise Performance. Sports. 2015; 3(4):312-324. https://0-doi-org.brum.beds.ac.uk/10.3390/sports3040312
Chicago/Turabian StyleThurston, Taylor S., Jared W. Coburn, Lee E. Brown, Albert Bartolini, Tori L. Beaudette, Patrick Karg, Kathryn A. McLeland, Jose A. Arevalo, Daniel A. Judelson, and Andrew J. Galpin. 2015. "Effects of Respiratory Muscle Warm-up on High-Intensity Exercise Performance" Sports 3, no. 4: 312-324. https://0-doi-org.brum.beds.ac.uk/10.3390/sports3040312