Sustainability of the Loita Maasai Childrens’ Ethnomedicinal Knowledge

1
School of Biological Sciences, University of Nairobi, Nairobi P.O. Box 30197-00100, Kenya
2
School of Natural Resources and Animal Sciences, Maasai Mara University, Narok P.O. Box 861-20500, Kenya
3
Department of Bioscience—Ecoinformatics and Biodiversity, Aarhus University, Build. 1540, Ny Munkegade 116, DK-8000 Aarhus C, Denmark
*
Author to whom correspondence should be addressed.
Sustainability 2019, 11(19), 5530; https://0-doi-org.brum.beds.ac.uk/10.3390/su11195530
Submission received: 20 August 2019
/
Revised: 30 September 2019
/
Accepted: 4 October 2019
/
Published: 7 October 2019
(This article belongs to the Collection Cultural Crossovers and Social Sustainability)
Abstract
:Knowledge and practice of medicinal plant use is embedded in the Maasai culture. However, it is not known how that knowledge and practices are acquired by children and transferred across generations. We assessed children’s knowledge of medicinal plants and their uses, methods of knowledge acquisition and transfer, and how that process is influenced by demographic attributes such as gender, level of education, and age. We interviewed 80 children who were 6–17 years old. Mann–Whitney U, Kruskal–Wallis tests and Spearman Rank order correlation were performed to determine the influence of gender, level of education, and age when they are in the process of acquiring ethnomedicinal plant knowledge. The Maasai children acquired knowledge of medicinal plants progressively with their age. Ethnomedicinal knowledge was not influenced by gender or level of education. The children were introduced to the knowledge of local medicinal plants and their use at an average age of seven years and the knowledge was transferred indiscriminately to both girls and boys. This study aids in the protection and conservation of medicinal plant knowledge by encouraging the sustainability of the local cultural heritage.
1. Introduction
Medicinal plants have been used for generations as a source of inexpensive but effective remedies to treat various ailments [1]. Use of medicinal plants among the Maasai has surely been practiced for centuries and forms an important part of their culture, pride, and traditions, but the scientific documentation of Maasai medicinal plant use can only be traced back to the beginning of the last century [2,3]. The local knowledge related to their medicinal plants may not be sustainable and faces serious threats from acculturation and western world views [4]. This makes it vitally important to understand how traditional knowledge of medicinal plant use is transmitted to the younger generations in order to safeguard this wisdom against erosion and possible loss.
Children are the foundation for societies and they possess knowledge of their local environment, often acquired before they are 12 years old [5,6]. Local environmental knowledge has been passed on from one generation to the next since recorded time. Traditional knowledge is transmitted between generations through three major pathways; vertical transmission from parents to children, horizontal transmission between two individuals of the same generation, and oblique transmission from non-parental individuals [7,8,9,10].
Although traditional knowledge is a much broader concept, we here focus on ethnomedicinal knowledge about identification and uses of medicinal plants used in the treatment of human-related disorders, plant parts used, and preparation methods.
Local environmental knowledge, in general, is influenced by several factors including education, age, and gender [11,12]. Understanding the influence of education on ethnomedicinal plant knowledge is important, not least because the Maasai community has begun to embrace formal education by enrolling children in schools close to, or in some cases away from, their villages. It stands to reason that there is less knowledge passed through cultural lines when the children increasingly learn away from home. Age and gender are important parameters among the Maasai children because they engage in household activities early in life and because tasks are divided along gender lines. Boys are taught skills related to herding of cattle, while girls are taught various tasks related to domestic activities, including cooking, collecting firewood, and fetching water. As a result, children acquire environmental knowledge of their surroundings from interactions with nature. Traditional local knowledge is taught orally through experiential participation, observation, and storytelling, mostly by older members of the community [13].
Traditional knowledge may be declining due to factors such as introduction of western medicine, formal education, urbanization, and land degradation, among others [14,15,16,17]. The loss of medicinal plants and the associated knowledge will have negative impacts on communities such as the Maasai, who depend on traditional medicine for their well-being. In order to conserve and preserve this knowledge for posterity, research that targets children is needed.
The majority of ethnobotanical studies have concentrated on documenting ethnomedicinal knowledge from the adult’s perspective [18,19,20]. There is a general lack of knowledge concerning medicinal plants known to children and how children acquire this knowledge and along which channels the knowledge is transmitted [18,21,22,23]. The same is true for the Maasai community, where no research has been conducted to document children’s ethnomedicinal knowledge, and the factors that influence it.
In the Maasai community, children are an important component of the family and they participate in daily activities in their homes as directed by their parents [24]. The Maasai’s traditional pastoral way of life gives children the chance to learn basic activities early in life, which gives them an opportunity to familiarize themselves with their surrounding environment. Children as young as five years are assigned duties such as looking after newborn livestock around the homestead under the watch of older children or adults [24]. By the age of ten years, children have acquired enough skills to be entrusted with herding sheep, goats, or cattle further away from the homesteads [25].
Although there are a number of studies on the Maasai pastoral ways of knowing and managing natural resources [26,27,28,29], local knowledge of plants, and conservation strategies [30,31,32], there has, to our knowledge, not been any research conducted to document children’s ethnomedicinal knowledge, and how that knowledge is acquired and transmitted among the Maasai children. There is an incomplete picture of how this important knowledge, entrenched in the Maasai culture, flows from one generation to another. Documentation of this important cultural resource can contribute to our understanding of children’s ethnomedicinal knowledge in pastoral societies and the dynamics that affects that knowledge.
The objectives of this study were to identify and document medicinal plants commonly known by Maasai children, the mode of knowledge transmission, and how ethnomedicinal knowledge varies according to gender, level of education, and age. In this context, we specifically ask the following questions:
- Which medicinal plants are commonly known by children and to which use categories do the plants belong?
- At what age is the medicinal plant knowledge introduced to children?
- From whom do the children learn and through what mechanism?
- Do gender, level of education, and age influence the local knowledge of the medicinal system?
We hypothesized that:
- Gender will influence the Maasai children’s knowledge of medicinal plants.
- The informant’s level of education will have an influence on knowledge of the medicinal system.
- Age will have a significant influence on ethnomedicinal knowledge.
2. Materials and Methods
2.1. Study Area
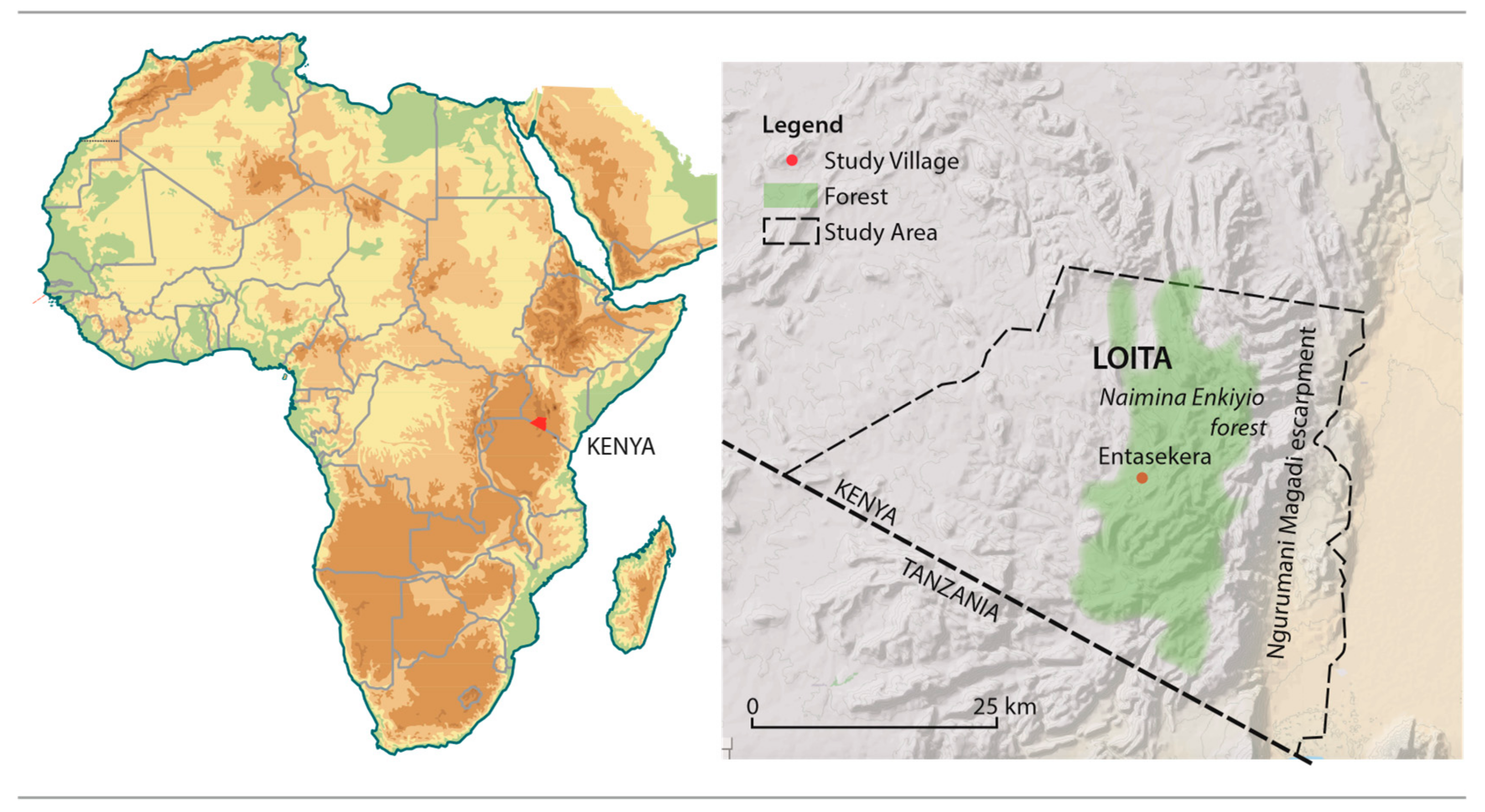
The study was done in Entasekera village in Loita, southern Kenya (Figure 1). The subcounty covers 1676 km2 and is home to 25,000 people known as the Loita Maasai or the Iloitai. Loita borders the Ngurumani-Magadi escarpment to the East and the United Republic of Tanzania to the South. The natural vegetation in the area includes grassland, wooded grassland, thickets, bush land, dry upland forest, and disturbed forest edges [31]. The climate is predominantly semiarid with a mean annual rainfall of 600–2000 mm and temperature that ranges from 17 to 20 °C in the wooded and forested areas and 20 to 22 °C in the open rangelands. The Naimina Enkiyio forest covers some 300 km2 and provides important ecosystem services to the local community as it meets many of their health, spiritual, cultural, and material needs [31], especially wood, foliage, and wild honey. In the context of this study, the forest is an important source of medicinal plants used in the treatment of human ailments and livestock diseases, not only in Loita but also beyond. The Loita Maasai are agro-pastoralist who rear cattle and practice small-scale agriculture, growing maize and beans. The local community has in the recent past adopted semipermanent settlement. This implies that their dependence on the existing woodlands and forests for medicinal plants, wood fuel, and livestock grazing has increased considerably. Most adult men and women lack formal education, though their children have increasingly enrolled for primary and secondary education, and a few have proceeded to undertake college and university education.
2.2. Research Permits
Permission to carry out this study was obtained from Kenya’s National Commission for Science, Technology and Innovation (NACOSTI) Permit Number NACOSTI/18/54615/26671. The permit was issued through the Maasai Mara Science Development Initiative. We also received permission to collect data from the local administrators. The parents or guardians of the children in the households selected to participate in the study were made aware of the purpose of the study, and consent for their children’s participation was granted.
2.3. Data Collection
Field work was conducted from July to October 2018. A total of 80 children, comprising 31 girls and 49 boys drawn from 45 households, were interviewed. The children were 6–17 years old. The choice of age bracket was guided by the Kenyan constitution, which describes a child as a person below the age of 18 years. Purposive sampling based on age was used while maintaining gender balance as much as possible. Conversations and explanations about the project and its activities at the site were made in local Maa language (mother tongue of first author) where necessary.
Initial data collection involved the compilation of a medicinal plant inventory (Table 1), which was subsequently used to document children’s ethnomedicinal plant knowledge. The compilation of the inventory involved walks within and around the village with three local medicinal plant experts drawn from the village. Local names and vouchers of all medicinal plants around the village were collected in duplicate. One batch was shown to the children—one specimen at a time—and in the same order to document children’s knowledge of the common medicinal plant found within and around the village. The other duplicate of the voucher specimens was identified to its scientific name by a taxonomist, and deposited for curation at the University of Nairobi Herbarium.
The interview questions used for assessing the 80 children’s knowledge of medicinal plants in the 45 households were divided into two sections. Section A collected information on social demographic traits of the children, including name, age, gender, and level of education. This was followed by questions about transmission channels of medicinal plant knowledge, that is, who taught them about the plants they knew, and at what age were they taught.
Section B gathered information on the knowledge of the medicinal plants found within and around the village, based on the plant inventory. Each child was shown a fresh sample of a medicinal plant one at a time, and asked if they knew the plant. If they said yes, they were asked for its vernacular name, the human health conditions that the plant was used to treat, as well as the plant parts used and the preparation methods.
From the plant inventory of the 20 medicinal species collected from within and around the village, the three local medicinal plant experts identified seven medicinal species (marked with double asterisk), which were not only found within and around the village, but also were the most commonly used for medication in the village (Table 1). The seven species were used to measure children’s knowledge of the commonly used medicinal species based on their age, gender, and level of education.
For each of the seven species the informant could earn a total score of two: one for correct identification of the plant specimen presented and another one for correct use mentioned. The responses given were validated by the three local medicinal plant experts. If an informant gave the correct identification of the species but a wrong response for use, a score of one was awarded for correct identification and a zero for wrong use. The informants who could not correctly identify and give correct use of the plant specimen were awarded zero score (i.e., 0/0). The maximum score for each child whose knowledge was evaluated was 14 points (7/7). Individual total scores for all the plant species were calculated and the data used for analysis to test whether or not gender, level of education, and age had an influence on the local knowledge of the medicinal system.
2.4. Data Analysis
Data were entered into a Microsoft Excel spreadsheet. Each plant was identified by its local and scientific name according to The Plant List website (www.theplantlist.org). Each use report was assigned to a use category following WHO’s International Classification of Primary Care (ICPC) [33]. To determine the species that are known to children, we calculated the percentage Relative Frequency of Citation (RFC) for each of the twenty species shown [34,35]. Where FC is the frequency of citation of a species and N is the total number of informants participating in the study.
Statistical Analysis
Statistical analysis of knowledge scores was performed in the Statistical Package for Social Sciences (SPSS) to test for the influence of gender, level of education, and age on ethnomedicinal knowledge. The Mann–Whitney U test was used to determine gender-related differences in knowledge of medicinal plants. The Kruskal–Wallis test was performed to determine whether or not there were differences in knowledge scores across children in various levels of education. Spearman Rank order correlation was used to test the relationship between informant’s age and ethnomedicinal knowledge.
3. Results
3.1. Children’s Knowledge of Medicinal Plants
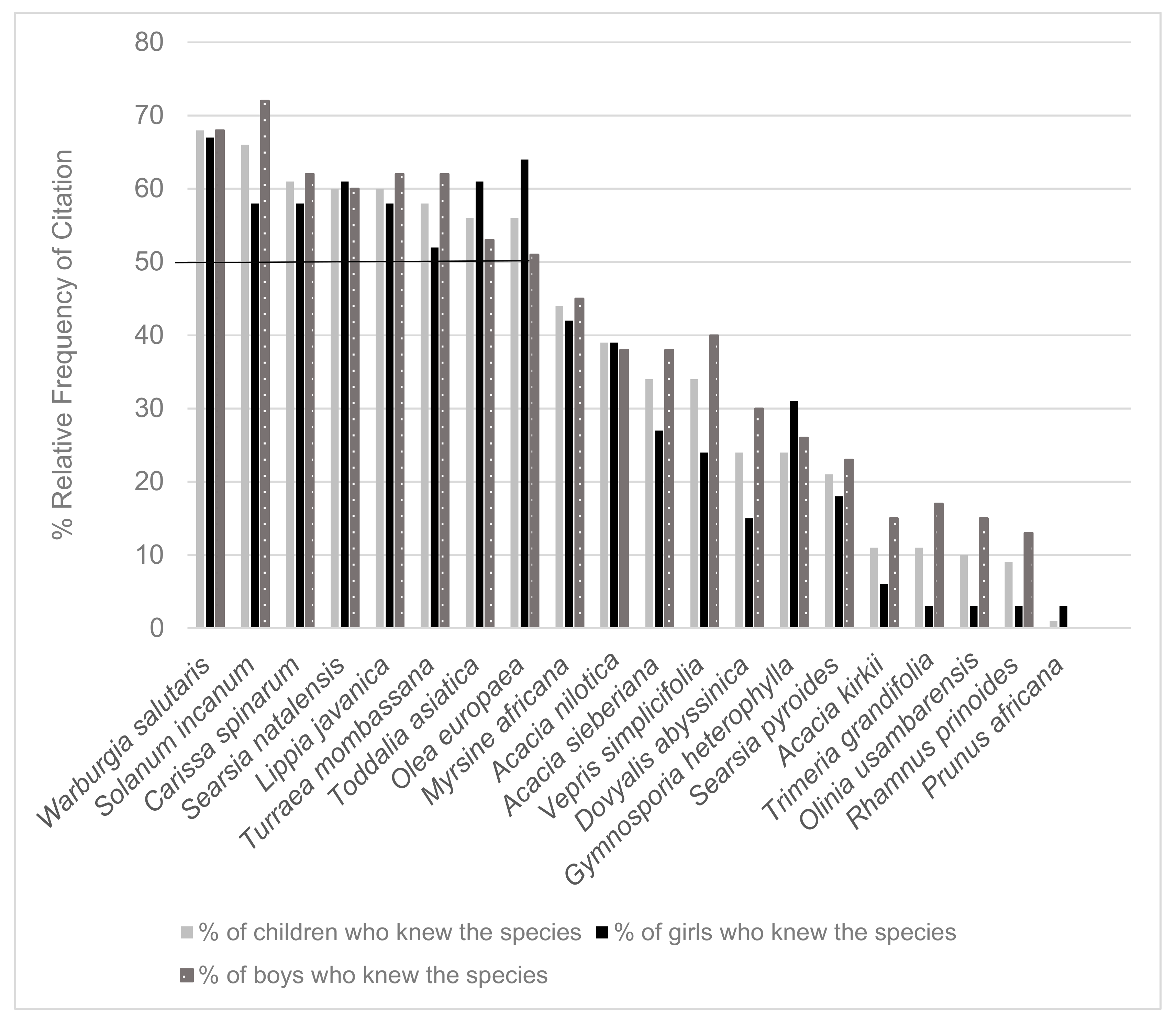
Among the 80 children aged 6–17 years, eight medicinal plant species were known by half of the children interviewed (Figure 2). Together, the 31 girls were able to identify all the 20 plant species presented to them, while the 49 boys were able to identify 19 of the 20 species (Figure 2).
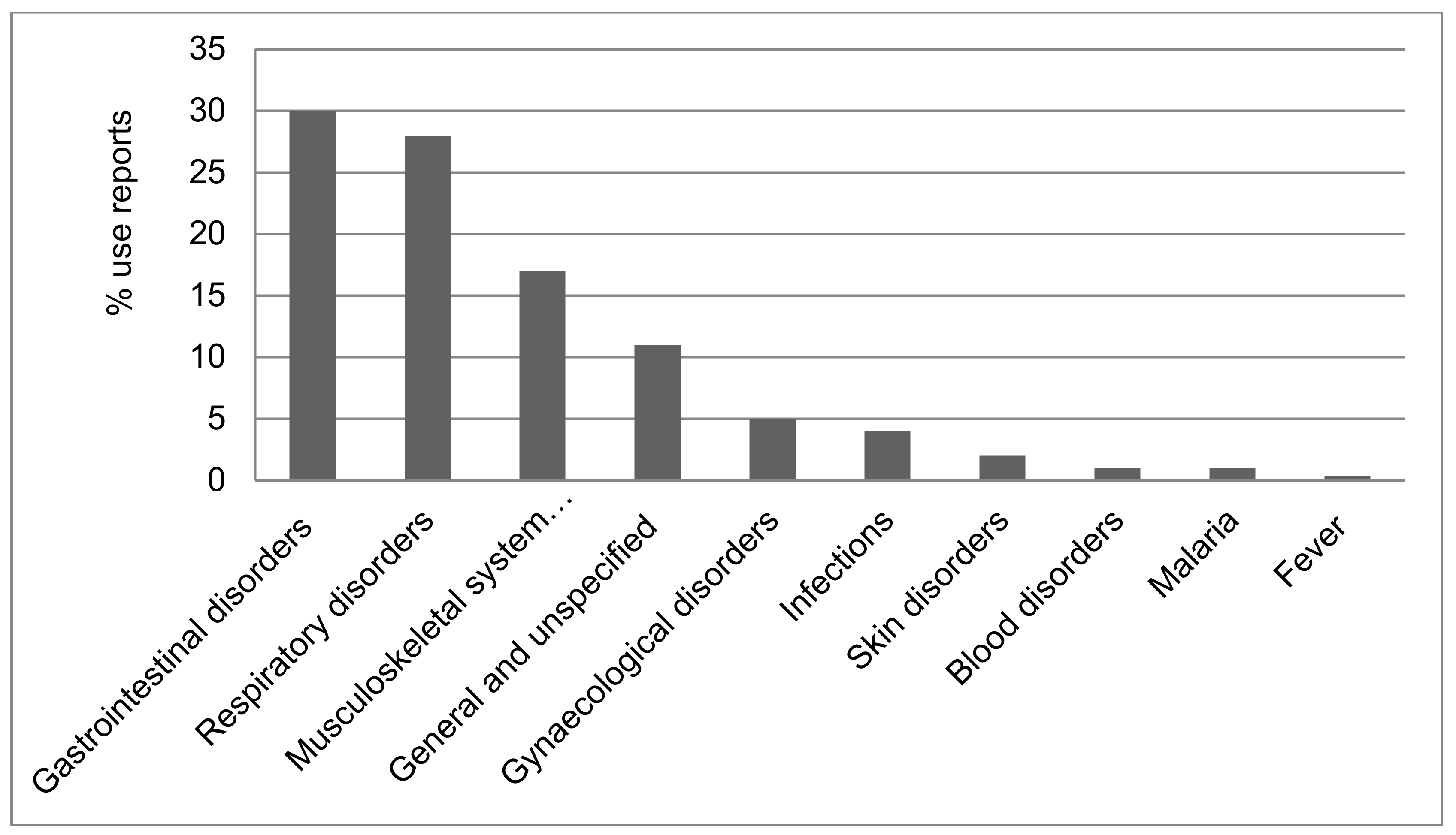
The total of 387 use reports obtained from the children in the study area belonged to ten use categories (Figure 3) as defined in the International Classification of Primary Care (ICPC) system [33]. The uses known by the children were mostly in the categories of gastrointestinal disorders, and respiratory- and musculoskeletal-system-related conditions. The use of medicinal plants to treat diseases, such as malaria, blood disorders, and fever, had the fewest use reports.
3.2. Plant Parts and Preparations
Besides the identification of medicinal plants and their uses, children also knew the plant parts used to extract the active ingredients needed for treatment of body conditions and diseases. The most common plant parts known to be used to extract the medicine were the bark with 168 use reports (43%), closely followed by roots (166 use reports; 43%), leaves (26 use reports; 7%), and fruits (17 use reports; 4%). Most of the children were not familiar with the use of multiple plant parts to extract the medicine and this category had only 11 use reports (3%). Similarly, the use of stems of woody plants to extract medicine had the fewest use reports (7; 2%) mentioned by the children.
The children knew a variety of methods for preparing the desired medicines. The common methods mentioned were decoction (309 use reports; 80%), maceration (40 use reports; 10%), and eating of the raw plant part without any preparation (23 use reports; 6%). The children had limited knowledge of mixing different parts (7 use reports; 2%) from the same medicinal plant species to extract a desired medicine. Similarly, crushing (4 use reports; 1%) of plant parts to prepare them for drug extraction was not widely known by the children in the study area.
3.3. Sources of Medicinal Knowledge, Teaching Age, and Methods
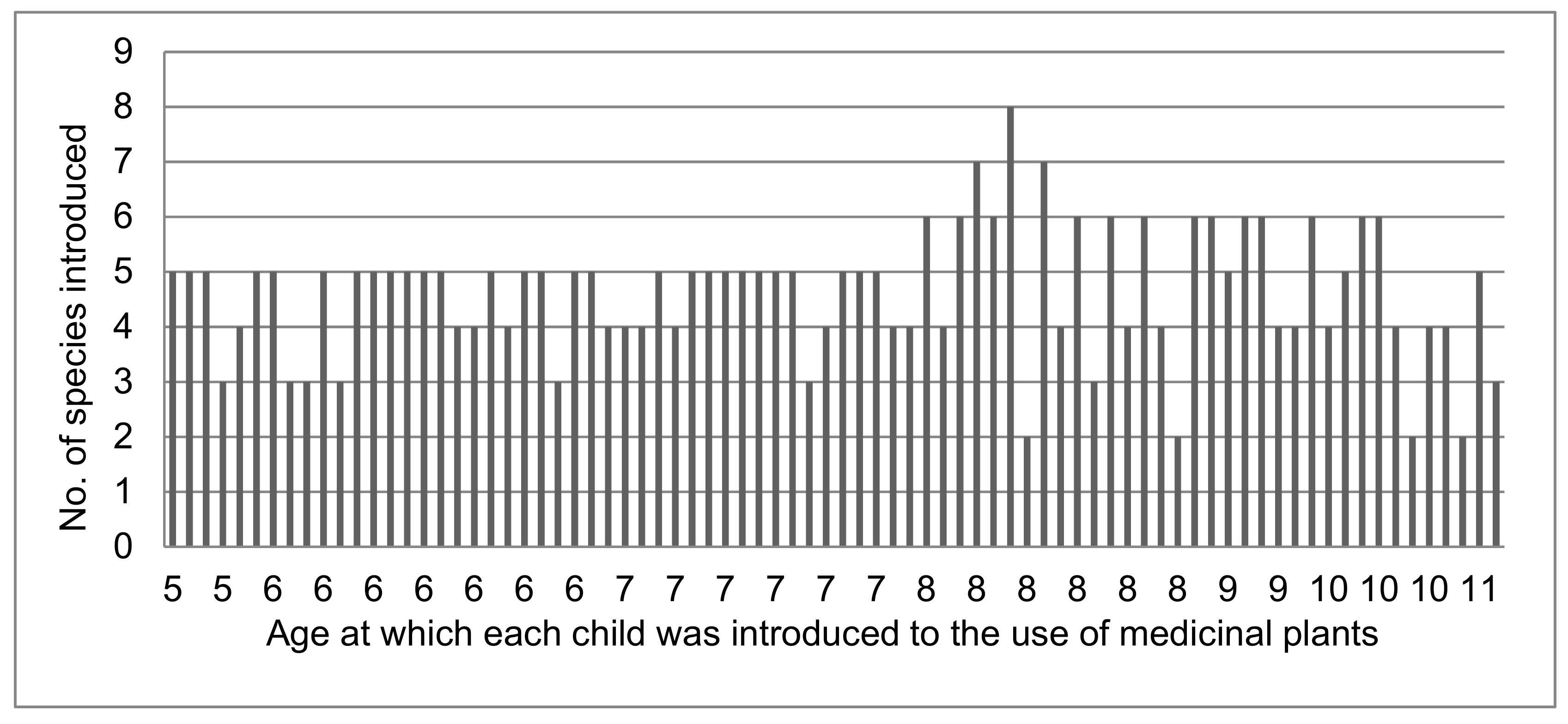
Adult men and women among the Loita Maasai made deliberate efforts to teach their children about medicinal plants and their significance. On average, children were introduced to medicinal plants and their uses when they attain an average age of seven years. By the time children attained an average age of seven years, they had acquired the knowledge of five medicinal species on average (Figure 4).
The children interviewed in Loita drew their knowledge of medicinal plants from a variety of sources. Parents were the primary source of ethnomedicinal knowledge, with 88% of the informants reporting to have acquired their knowledge largely from vertical transmission. The other sources of medicinal plant knowledge were close relatives (6%), the children’s friends from around the village and in the neighboring villages (5%), and neighbors (1%), which all represent oblique transfer.
The main mode of teaching was through experiential participation (53% of all informants), where children accompanied their parents during the collection and preparation of the required medicine. Children were also taught orally (35%) about medicinal plants by adults, and made their own observations or investigations (12%). The children also learned about medicinal plants from storytelling, as mentioned by 0.7% of the children interviewed.
3.4. Gender, Education Level, and Age
The children of the Loita Maasai had a wide range of opportunities to learn about medicinal plants while performing their different chores in the households. There was no significant difference between boys and girls in their ethnomedicinal plant knowledge (Mann–Whitney U, Z value = −1.53, P = 0.13). Knowledge of medicinal plants and their uses did not differ significantly across the education levels of the children in the study area (Kruskal–Wallis X2 = 1.23, p = 0.54). However, knowledge of medicinal plants increased significantly with the age of the children (Spearman Rank Correlation Coefficient, rho = 0.490, p < 0.000).
4. Discussion
4.1. Commonly Known Medicinal Plants and Use Categories
Medicinal plants are used all over the world to alleviate human suffering and they contribute to the global health and well-being of millions of people.
Ethnomedicinal knowledge is still effectively transmitted to the younger Maasai generation. The Loita children knew many medicinal plants in and around their village. Of the 20 medicinal species shown to children, eight were known by more than half of the children even if no child was able to correctly identify all the 20 plants they were shown. The parents knew all the 20 species and their uses, further confirming that the parents are the main transmitters of ethnomedicinal knowledge.
The Maasai of Sekenani, Maasai Mara in Narok County, and Kuku group ranch in Kajiado County were reported to use 39 and 41 medicinal species, respectively [15,27], to treat various human health conditions, confirming the reliance of medicinal plants for health care needs in the Maasai community of Kenya.
The Maasai people use medicinal plants to treat human and livestock diseases [36]. Some medicinal plants are used in the treatment of both human and livestock diseases. For example, the Ilkisonko Maasai use 18 medicinal species for treatment of livestock diseases [36]. Out of the 18 ethnoveterinary medicinal plants, Salvadora persica L., Acacia drepanolobium Sjostedt, Acacia gerrardii Benth., Rhamnus staddo A. Rich., and Albizia anthelmintica Brongn. were used to treat human health disorders [15,27,30,31,32]. Rhamnus staddo A. Rich., used for treatment of both human and livestock disease, was known by a total of 9 children.
In a rural village in northeast Thailand, children’s knowledge of wild resources was influenced by the abundance of species and by their taste; those with a sweet taste were better known [37]. It is possible that the species which were not recognized by a majority of the Loita children interviewed in our study were such ones with low abundances, or such ones that were not easy to gather.
The medicinal plants commonly known to children were mostly in the WHO categories [33] of plants used to treat gastrointestinal disorders, respiratory disorders, and musculoskeletal system disorders. Based on the use reports given by parents, digestive system disorders, musculoskeletal system disorders, and respiratory disorders had the highest numbers of use reports. Previous studies conducted in the Loita area reported that digestive system disorders [30] (which is a part of the category of gastrointestinal disorders) and respiratory disorders [31] were the most common health problem among the Loita Maasai. These findings agree with those of a recent study conducted in the town of Krummhübel in the Sudety Mountains (now SW Poland) that reported respiratory system disorders and gastrointestinal disorders to be the common disorders treated with medicinal plants mixed in with other ingredients [38].
Digestive system disorders are common in children during the early stages of development due to their limited body immunity. Children are highly susceptible to illnesses such as diarrhea, constipation, dysentery [39], cough, the common cold, among others. The fact that the children commonly experience such illnesses could be the reason why the plants in these two categories were so well known to them. Plants used to treat malaria, blood disorders, and fever had few use reports, possibly because of the complexity of diagnosing health conditions in these categories.
4.2. Sources of Medicinal Knowledge, Learning Age, and Methods
Learning of medicinal plants started as early as at an average age of seven years when they had been introduced to knowledge of five medicinal species on average. In Mexico, learning started early during childhood and the children obtained most of their environmental knowledge before the age of 12 years [5,6]. At the age of nine, Mayan children were able to identify half of the plants known by adults [18], while in Bolivia, children were able to identify 80% of the palm species at the age of six years [40]. The Loita Maasai children fall within these brackets from around the world.
It is important to know the transmitters of traditional knowledge as they help in the protection and conservation of local cultural and natural resources [41]. In Loita parents, both fathers and mothers were the main source of knowledge, which means that the transmission was mostly vertical. During the early stages of development, the Maasai children spend most of their time with their parents and play around their homesteads. They are able to learn and observe from parents and, in the process, the children acquire local ethnomedicinal plant knowledge. Our observations agree with those found in widely scattered locations such as subarctic Canada, the Orinoco delta in South America, and various localities in Africa [21,42,43,44]. All show that parents are the main transmitters of knowledge. In contrast to our observations, relatives were reported to provide horizontal transmission of food knowledge among Tyrolean migrants in Australia, Brazil, and Peru [45]. Other studies have reported that grandmothers and peers are important oblique transmitters of local environmental knowledge [6,44].
Medicinal plant knowledge among the Maasai was taught through use, which allowed children to gain empirical experience. Children were sent to collect medicinal plants, and sometimes they were given the task of preparing the medicine under the watchful eyes of their parents. Similar teaching methods were reported in a rural village in northeastern Thailand, where children joined their parents in the field to collect wild food resources [37].
4.3. Gender, Level of Education, and Age
We found no statistically significant difference in ethnomedicinal knowledge between girls and boys. Unlike other forms of knowledge, such as herding, hunting, and domestic chores, which are transmitted along gender lines in the Maasai community, medicinal plants knowledge appeared to be taught to both boys and girls equally. Similar to our findings, a study of childrens’ knowledge in a rural village in northeastern Thailand found that there was no significant difference in knowledge of wild food resources between girls and boys [37].
The level of education did not influence the ethnomedicinal plant knowledge of the Maasai children, maybe because most children were day scholars and attended local primary and secondary schools in the villages. Schooling in day schools allows for time after school or during weekends to learn about medicinal plants. As they join universities and colleges outside of the village, they have mastered most of the local ethnomedicinal knowledge, suggesting a longer persistence of that knowledge. As a result, external influences may not negatively affect the sustainability of ethnomedicinal knowledge, but other studies of Amerindian children found that the level of education indeed did influence local knowledge [7]. It was argued that people spend a lot of time in formal education and miss the opportunity to learn from their parents.
Children in the village acquired more ethnomedicinal knowledge as they became older. Older children had higher scores compared to the younger ones. The findings could be due to the increased responsibilities given to Maasai children as they grow up. This process may help them acquire more knowledge. In southern China, the number of known wild edible plants also increased with informants’ age [41], and in a study from northern South America, such growth was attributed to natural acquisition of knowledge over time [46].
5. Conclusions
Children possess local traditional knowledge of medicinal plants which they acquire early on in life. We found that the Loita children possessed ethnomedicinal knowledge that was introduced to them from when they attained an average age of seven years and parents are the main drivers in knowledge transmission. Based on our findings, the main mode of transmission of ethnomedicinal knowledge was largely through the vertical pathway and, to some extent, through oblique mechanisms, with very few children reporting to have acquired the knowledge through horizontal transmission. The children’s ethnomedicinal knowledge of the local plants could have been influenced to some extent by the availability of the species around the village.
Medicinal plant knowledge among the Loita Maasai children was not transmitted along gender lines. Boys and girls were given the same knowledge about medicinal plants. Non-gender related knowledge is different from gender skills such as herding, which is mainly taught by fathers to sons, and household chores, which are taught by mothers to daughters. We can therefore reject our hypotheses that gender influences the Maasai children’s knowledge of medicinal plants. However, the hypothesis that age influences the knowledge could not be rejected. Age was found to have a significant influence on ethnomedicinal knowledge. Despite the high enrolment of Maasai children into formal education, as compared to a few decades ago, the level of education did not affect ethnomedicinal knowledge.
We suggest that more research should be conducted to test medicinal knowledge of the children who are educated far away from the villages to determine whether being away from their natural environment has an impact on their knowledge.
We noted that no single species was known by all the children interviewed. We therefore suggest that further research should be conducted to understand the reason for this knowledge gap. Additional research should be conducted to document ethnoveterinary medicinal plants knowledge of the Maasai children and to establish which of the two domains of knowledge (ethnoveterinary plants or plants used for human remedies) is taught first.
This study identifies and documents medicinal plants known by the Loita Maasai children. It provides a deeper understanding of the acquisition of ethnomedicinal knowledge by the Maasai children and the factors that influence the knowledge. It also shows that the process of transmitting knowledge to the children is mostly vertical and appears sustainable.
Diseases such as pneumonia and diarrhea affect children worldwide. Traditional medicine has contributed to the discovery of life-saving drugs. The knowledge of local plants with medicinal values can contribute to global therapies, which can be used in the treatment of child-related illnesses, hence, reduction of child mortality, especially for the under-five years of age.
The potential of new drug discoveries may be beneficial in managing some of the common diseases affecting populations around the world, hence aid in the achievement of UN sustainable development goal number 3, that seeks to achieve good health and well-being.
This study may contribute to the protection, conservation, and sustainability of knowledge handed down culturally through familial lines.
Author Contributions
J.N., N.G., C.L., and H.B. conceived the study. J.N. prepared the manuscript; N.G., C.L., and H.B. reviewed and edited the manuscript and approved the final version.
Funding
This research was self-funded.
Acknowledgments
We thank all the informants for sharing their knowledge with us.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lamxay, V.; de Boer, H.J.; Björk, L. Traditions and plant use during pregnancy, childbirth and postpartum recovery by the Kry ethnic group in Lao PDR. J. Ethnobiol. Ethnomed. 2011, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Hollis, A.C. The Masai: Their language and folklore; Clarendon Press: Oxford, UK, 1905. [Google Scholar]
- Merker, M. Die Masai; Dietrich Reimer: Berlin, Germany, 1910. [Google Scholar]
- Voeks, R.A.; Leony, A. Forgetting the forest: Assessing medicinal plant erosion in eastern Brazil. Econ. Bot. 2004, 58, 294–306. [Google Scholar] [CrossRef]
- Stross, B. Acquisition of botanical terminology by Tzeltal children. In Meaning in Mayan languages: Ethnolinguistic Studies; Edmonson, M.S., Ed.; Mouton & Co. N.V.: Hague, The Netherlands, 1973; pp. 107–141. [Google Scholar]
- Zarger, R.K. Children’s ethnoecological knowledge: Situated learning and the cultural transmission of subsistence knowledge and skills among Q’eqchi’ Maya. Ph.D. Thesis, Department of Anthropology, University of Georgia, Athens, GA, USA, 2002. [Google Scholar]
- Reyes-García, V.; Broesch, J.; Calvet-Mir, L.; Fuentes-Pelaez, N.; McDade, T.W.; Parsa, S.; Tanner, S.; Huanca, T.; Leonard, W.; Martínez-Rodríguez, M. Cultural transmission of ethnobotanical knowledge and skills: An empirical analysis from an Amerindian society. Evol. Hum. Beh. 2009, 30, 274–285. [Google Scholar] [CrossRef]
- Cavalli-Sforza, L.L.; Feldman, M.W.; Chen, K.H.; Dornbusch, S.M. Theory and Observation in Cultural Transmission. Am. Assoc. Adv. Sci. Stable 1986, 218, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Eyssartier, C.; Ladio, A.H.; Lozada, M. Cultural transmission of traditional knowledge in two populations of North-western Patagonia. J. Ethnob. Ethnomed. 2008, 4, 1–8. [Google Scholar] [CrossRef]
- Ruiz-Mallén, I.; Morsello, C.; Reyes-garcía, V.; Barros, M.; De Faria, R. Children’s use of time and traditional ecological learning. A case study in two Amazonian indigenous societies. Learn. Individ. Differ. 2013, 27, 213–222. [Google Scholar] [CrossRef]
- Byg, A.; Balslev, H. Factors affecting local knowledge of palms in Nangaritza valley, southeastern Ecuador. J. Ethnobiol. 2004, 24, 255–278. [Google Scholar]
- Yates, S.; Ramırez-Sosa, C. Ethnobotanical knowledge of Brosimum alicastrum (Moraceae) among urban and rural El Salvadorian adolescents. Econ. Bot. 2004, 58, 72–77. [Google Scholar] [CrossRef]
- Hunn, E.S. Evidence for the precocious acquisitions of plant knowledge by Zapotec children. In Ethnobiology and Biocultural Diversity; Stepp, J.R., Wyndham, F.S., Zarger, R.K., Eds.; University of Georgia Press: Athens, GA, USA, 2002; pp. 604–613. [Google Scholar]
- Kala, C.P. Status and conservation of rare and endangered medicinal plants in the Indian trans-Himalaya. Biol. Conserv. 2000, 93, 371–379. [Google Scholar] [CrossRef]
- Kiringe, J.W. A survey on the use of ethno-medicinal health remedies among the Maasai of Southern Kajiado District, Kenya. Ethnobot. Res. Appl. 2006, 73, 61–73. [Google Scholar] [CrossRef]
- Anyinam, C. Ecology and ethnomedicine: Exploring links between current environmental crisis and indigenous medical practices. Soc. Sci. Med. 1995, 40, 321–329. [Google Scholar] [CrossRef]
- Romulo, A.; Rosa, M. Biodiversity, traditional medicine and public health: Where do they meet? J. Ethnobiol. Ethnomed. 2010, 3, 160–169. [Google Scholar]
- Zarger, R.; Stepp, J.R. Persistence of botanical knowledge among Tzeltal Maya Children. Curr. Anthropol. 2004, 45, 413–418. [Google Scholar] [CrossRef]
- Medin, D.L.; Atran, S. Introduction in Folkbiology; MIT Press: Cambridge, MA, USA, 1999. [Google Scholar]
- Waxman, S.R. The Dubbing Ceremony Revisited: Object Naming and Categorization in Infancy and Early Childhood. In Folkbiology; Medin, D., Atran, S., Eds.; MIT Press: Cambridge, MA, USA, 1999; pp. 233–284. [Google Scholar]
- Ohmagari, K.; Berkes, F. Transmission of indigenous knowledge and bush skills among the Western James Bay Cree woman of subarctic Canada. Hum. Ecol. 1997, 25, 197–222. [Google Scholar] [CrossRef]
- Young, K. Minding the children: Knowledge transfer and the future of sustainable agriculture. Conserv. Biol. 2002, 16, 855–856. [Google Scholar] [CrossRef]
- Souto, T.; Ticktin, T. Understanding interrelationships among predictors (age, gender, and origin) of local ecological knowledge. Econ. Bot. 2012, 66, 149–164. [Google Scholar] [CrossRef]
- Tian, X. Ethnobiological knowledge generation during “herding games” in pastoralist maasai society (southern kenya). Anthropochildren 2017, 7. [Google Scholar] [CrossRef]
- Grandin, B.E. The Maasai: Socio-historical context and group ranches. In Maasai Herding. An Analysis of the Livestock Production System of Maasai Pastoralists in Eastern Kajiado District, Kenya; Bekure, S., de Leeuw, P.N., Grandin, B.E., Neate, P.J.H., Eds.; International Livestock Center for Africa: Addis Ababa, Ethiopia, 1999; pp. 21–39. [Google Scholar]
- Bekure, S.; de Leeuw, P.N.; Grandin, B.E.; Neate, P.J.H. (Eds.) Maasai herding: An analysis of the livestock production system of Maasai pastoralists in Eastern Kajiado District, Kenya; International Livestock Centre for Africa: Addis Ababa, Ethiopia, 1991. [Google Scholar]
- Bussmann, R.W.; Gilbreath, G.G.; Solio, J.; Lutura, M.; Lutuluo, R.; Kunguru, K.; Wood, N.; Mathenge, S.G. Plant use of the Maasai of Sekenani Valley, Maasai Mara, Kenya. J. Ethnobiol. Ethnomed. 2006, 2, 22–27. [Google Scholar] [CrossRef]
- Galaty, J. Cattle and cognition: Aspects of Maasai practical reasoning. In The Walking Larder: Patterns of Domestication, Pastoralism, and Predation; Clutton -Brock, J., Ed.; Unwin Hyman Ltd.: London, UK, 1989; pp. 215–230. [Google Scholar]
- Konaka, S. Metaphorical projection and integrated cognitive systems: The Samburu in North Central Kenya. In Good to Eat, Good to Live with: Nomads and Animals in Northern Eurasia and Africa; Stammler, F., Takakura, H., Eds.; Center for Northeast Asian Studies: Sendai, Japan, 2010; pp. 63–73. [Google Scholar]
- Nankaya, J.; Nampushi, J.; Petenya, S.; Balslev, H. Ethnomedicinal plants of the Loita Maasai of Kenya. J. Env. Dev. Sustain. 2019. [Google Scholar] [CrossRef]
- Maundu, P.; Berger, D.; Ole Saitabau, C.; Nasieku, J.; Kipelian, M.; Mathenge, S.; Morimoto, Y.; Höft, R. Ethnobotany of the Loita Maasai: Towards Community Management of the Forest of the Lost Child Experiences from the Loita Ethnobotany Project, 8. People and plants working paper; UNESCO: Paris, France, 2001. [Google Scholar]
- Kiringe, J.W. Ecological and anthropological threats to ethno-medicinal plant resources and their utilization in Maasai communal ranches in the Amboseli region of Kenya. Ethnobot. Res. Appl. 2005, 3, 231–242. [Google Scholar] [CrossRef]
- International Classification of Diseases (ICD). Available online: http://www.who.int/classifications/icd/en/ (accessed on 10 April 2019).
- Tardío, J.; Pardo-de-Santayana, M. Cultural importance indices: A comparative analysis based on the useful wild plants of southern Cantabria (northern Spain). Econ. Bot. 2008, 62, 24–39. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, H.; Chen, H.; Wang, F.; Huai, H. Diversity of wetland plants used traditionally in China: A literature review. J. Ethnobiol. Ethnomed. 2014, 10, 72. [Google Scholar] [CrossRef] [PubMed]
- Miaron, J.O. The Maasai ethnodiagnostic skill of livestock diseases: A lead to traditional bioprospecting. J. Ethnopharmacol. 2003, 84, 79–83. [Google Scholar] [CrossRef]
- Setalaphruk, C.; Price, L. Children’s traditional ecological knowledge of wild food resources: A case study in a rural village in northeast Thailand. J. Ethnobiol. Ethnomed. 2007, 3, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Spałek, K.; Spielvogel, l.; Proćków, M.; Proćków, J. Historical ethnopharmacology of the herbalists from Krummhübel in the Sudety Mountains (seventeenth to nineteenth century), Silesia. J. Ethnobiol. Ethnomed. 2019, 15, 24. [Google Scholar] [CrossRef]
- Shaheen, S.; Abbas, S.; Hussain, J.; Mabood, F.; Umair, M.; Ali, M.; Ahmad, M.; Zafar, M.; Farooq, U.; Khan, A. Knowledge of medicinal plants for children diseases in the environs of District Bannu, Khyber Pakhtoonkhwa (KPK). Front. Pharmacol. 2017, 8, 430. [Google Scholar] [CrossRef] [PubMed]
- Blacutt-Rivero, E.; Moraes, M.R.; Gruca, M.; Balslev, H. Local knowledge about palms (Arecaceae) among children in Bolivia. Bot. J. Linn. Soc. 2016, 182, 505–516. [Google Scholar] [CrossRef] [Green Version]
- Geng, Y.; Zhang, Y.; Ranjitkar, S.; Huai, H.; Wang, Y. Traditional knowledge and its transmission of wild edibles used by the Naxi in Baidi Village, Northwest Yunnan province. J. Ethnobiol. Ethnomed. 2016, 12, 10. [Google Scholar] [CrossRef]
- Ruddle, K.; Chesterfield, R. Education for traditional food procurement in the Orinoco delta; University of California Press: Berkeley, CA, USA, 1977. [Google Scholar]
- Hewlett, B.; De Silvestri, A.; Guglielmino, C. Semes and genes in Africa. Curr. Anthropol. 2002, 43, 313–321. [Google Scholar] [CrossRef]
- Lancy, D.F. Playing on the Mother-Ground: Cultural Routine for Children’s Development: Culture and Human Development; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Haselmair, R.; Pirker, H.; Kuhn, E.; Vogl, C.R. Personal networks: A tool for gaining insight into the transmission of knowledge about food and medicinal plants among Tyrolean (Austrian) migrants in Australia, Brazil and Peru. J. Ethnobiol. Ethnomed. 2014, 10, 1. [Google Scholar] [CrossRef]
- Zent, S. Acculturation and ethnobotanical knowledge loss among the Piaroa of Venezuela: Demonstration of a quantitative method for the empirical study of traditional ecological knowledge change. In On Biocultural Diversity: Linking Language, Knowledge, and the Environment; Maffi, L., Ed.; Smithsonian Institute Press: Washington, DC, USA, 2001; pp. 190–211. [Google Scholar]
Figure 1.
Map of Loita showing the study area.

Figure 2.
The Relative Frequency of Citation (RFC) for each of the 20 medicinal species shown during the interviews of the 31 girls and 49 boys of Loita Maasai children 6–17 years old. The 50% line separates the eight medicinal species known by more than half of the 80 children interviewed.
Figure 2.
The Relative Frequency of Citation (RFC) for each of the 20 medicinal species shown during the interviews of the 31 girls and 49 boys of Loita Maasai children 6–17 years old. The 50% line separates the eight medicinal species known by more than half of the 80 children interviewed.

Figure 3.
Proportions of 387 use reports by 80 Maasai children in the Loita area, Kenya, in each of the categories defined by the WHO’s International Classification of Primary Care (ICPC) (33).
Figure 3.
Proportions of 387 use reports by 80 Maasai children in the Loita area, Kenya, in each of the categories defined by the WHO’s International Classification of Primary Care (ICPC) (33).

Figure 4.
Age at which each of the 80 interviewed children was introduced to the use of medicinal plants and the number of species introduced to them at that point.
Figure 4.
Age at which each of the 80 interviewed children was introduced to the use of medicinal plants and the number of species introduced to them at that point.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
List of the 20 medicinal species collected within and around the Entasekera village that were used to document children’s ethnomedicinal knowledge in Loita, Kenya. The species marked with asterisk (**) were identified by three local medicinal plant experts as the most commonly used for medication in the village and were used to test whether or not children’s knowledge of medicinal plants varied with their age, gender, and level of education.
Table 1.
List of the 20 medicinal species collected within and around the Entasekera village that were used to document children’s ethnomedicinal knowledge in Loita, Kenya. The species marked with asterisk (**) were identified by three local medicinal plant experts as the most commonly used for medication in the village and were used to test whether or not children’s knowledge of medicinal plants varied with their age, gender, and level of education.
| Scientific Name, Family and Voucher Number | Local Name | Ethnomedicinal Uses |
|---|---|---|
| ** Warburgia salutaris (G. Bertol.) Chiov. (Canellaceae) JN2018/008 | Osokonoi | Cleaning of the uterus, common cold, stomach pains |
| Solanum incanum L. (Solanaceae) JN2018/020 | Entulelei | Backache, body pain, colds, cough, heartburn, joints, sore throat |
| ** Carissa spinarum L. (Apocynaceae) JN2018/001 | Olamuriaki | Digestion during pregnancy, pelvic pain, backache, sexually transmitted diseases |
| ** Searsia natalensis (Bernh. ex C. Krauss) F.A. Barkley (Anacardiaceae) JN2018/012 | Olmisigiyioi | Cleaning of teeth for bad breath, stomach upset |
| Lippia javanica (Burm.f.) Spreng. (Verbenaceae) JN2018/006 | Osinoni | Chest pains, cleaning wounds, colds, constipation, general body health, heartburn, induce vomiting, joints, skin rashes, stomachache |
| Turraea mombassana C. DC. (Meliaceae) JN2018/003 | Olchani narok | Backache, wounds, common cold, cough, diarrhea, general good health, induce vomiting, joints, stomach pain |
| ** Toddalia asiatica (L.) Lam. (Rutaceae) JN2018/015 | Oleparmunyio | Fever, respiratory diseases, common cold |
| **Olea europaea L. (Oleaceae) JN2018/017 | Oloirien | Stomach pain, malaria, deworming |
| Myrsine africana L. (Primulaceae) JN2018/004 | Oseketeki | Backache, chest pains, cold, deworming, diarrhea, general body health, heartburn, high blood pressure, stomachache |
| ** Acacia nilotica (L.) Delile (Leguminosae) JN2018/010 | Olkiloriti | Chronic chest pains, joints, stomach upsets, cold, backache |
| Acacia sieberiana DC. (Leguminosae) JN2018/005 | Oltarara | Backache, chest pains, cleaning of the uterus after birth, coughs, general body health, stomachache |
| Vepris simplicifolia (Engl.) Mziray (Rutaceae) JN2018/013 | Orgilai | Backache, general good health, joints, malaria, stomach pain |
| Dovyalis abyssinica (A. Rich.) Warb. (Salicaceae) JN2018/007 | Olmorogi | Chest pain, cold, joints, mouth wash, stomachache |
| Gymnosporia heterophylla (Eckl. and Zeyh.) Loes. (Celastraceae) JN2018/009 | Olaimurunyai | Backache, cleaning wounds, cold general body health, heartburn joints, stomach pain |
| Searsia pyroides (Burch.) Moffett (Anacardiaceae) JN2018/018 | Olmunkushi | Backache, chest pain, general body health, joints, mouth sores Stomach pains |
| ** Acacia kirkii Oliv. (Leguminosae) JN2018/016 | Olngonguenyi | Expulsion of the afterbirth, Stomachache, chest pains general body health |
| Trimeria grandifolia (Hochst.) Warb. (Salicaceae) JN2018/014 | Oledat | Backache, general body health, pneumonia, stomachache |
| Olinia usambarensis Gilg ex Engl. (Penaeaceae) JN2018/011 | Olkirenyi | Cleaning wounds, colds, fever, malaria |
| Rhamnus prinoides L’Hér. (Rhamnaceae) JN2018/002 | Olkonyil | Backache, general body health, malaria, stomachache |
| Prunus africana (Hook.f.) Kalkman (Rosaceae) JN2018/019 | Olkujuk | Infections, urinary tract infection, wounds |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Nankaya, J.; Gichuki, N.; Lukhoba, C.; Balslev, H. Sustainability of the Loita Maasai Childrens’ Ethnomedicinal Knowledge. Sustainability 2019, 11, 5530. https://0-doi-org.brum.beds.ac.uk/10.3390/su11195530
AMA Style
Nankaya J, Gichuki N, Lukhoba C, Balslev H. Sustainability of the Loita Maasai Childrens’ Ethnomedicinal Knowledge. Sustainability. 2019; 11(19):5530. https://0-doi-org.brum.beds.ac.uk/10.3390/su11195530
Chicago/Turabian StyleNankaya, Jedidah, Nathan Gichuki, Catherine Lukhoba, and Henrik Balslev. 2019. "Sustainability of the Loita Maasai Childrens’ Ethnomedicinal Knowledge" Sustainability 11, no. 19: 5530. https://0-doi-org.brum.beds.ac.uk/10.3390/su11195530
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.