The Success of Public Health Measures in Europe during the COVID-19 Pandemic


Institute for Economic Research, Kardeljeva ploscad 17, 1000 Ljubljana, Slovenia
*
Author to whom correspondence should be addressed.
Sustainability 2020, 12(10), 4321; https://0-doi-org.brum.beds.ac.uk/10.3390/su12104321
Submission received: 28 April 2020
/
Revised: 19 May 2020
/
Accepted: 21 May 2020
/
Published: 25 May 2020
(This article belongs to the Section Health, Well-Being and Sustainability)
Abstract
:SARS-CoV-2, a serious threat to sustainable development prospects, is spreading within countries at varying speeds, among other things depending on their population density, behavioural responses, cultural factors, personal hygiene practices and habits. This has led to significant variation in countries’ policy responses aimed at stemming the proliferation of the virus. Using crisp-set qualitative comparative analysis, we conducted a comparative study at the European level to study the performance of different combinations of COVID-19 containment measures along with the response speeds. A set of configurations for two different scenarios (above- and below-median death rates) helps to illustrate how specific containment measures in each examined European country are related to the number of deaths. The main observation arising from the analysis is that the speed of response along with the decision to suspend international flights might determine the epidemic outbreak’s impact on fatality. The results also imply that several different combinations of containment measures are associated with death rates across Europe. The outcome of this analysis can assist in identifying which set of containment measures in the event of an epidemic outbreak is beneficial/detrimental.
1. Introduction
Fighting the unique COVID-19 pandemic poses an immense challenge for countries around the globe. A new strain known as SARS-CoV-2, closely related to bat coronaviruses, not previously detected in humans has emerged. First identified in China, this highly contagious virus was rapidly imported into Europe [1], bringing with it serious socioeconomic disruption, including cancelled events, widespread supply chain interruption, and school closures.
The COVID-19 pandemic is an exogenous shock for almost the entire world, hitting countries unevenly in terms of citizens’ health. They have been exposed to the virus at various times and have different numbers of cases and case fatality rates. European countries have yet to experience such an epidemiological picture and have therefore responded to the COVID-19 outbreak at varying speeds and with policy measures of different severity. If the shock had been symmetrical, joint action at the EU level could probably have been seen. In general, such asymmetries may create a range of institutional, economic, and political challenges that undermine the EU’s stability and the effectiveness of the various containment measures. Consequently, differences in the steps taken by European countries may have exacerbated the losses caused by the health asymmetries of the crisis.
According to the WHO, member states are encouraged to develop flexible plans to manage the health risks from pandemic influenza based on a national risk assessment that considers the global risk assessment conducted by the WHO [2]. This includes social distancing strategies to reduce the spread of influenza disease such as class suspensions, travel restrictions, cancelling events, reducing public transport, restricting gatherings, and adjusting patterns of work. Accurate, timely information, and the development of pandemic risk management plans are necessary commodities during a health emergency [3]. To contribute to what is currently known about the COVID-19 pandemic, this paper discusses the link between fatality rates and the stringency of the most common containment measures being implemented in the EU and the United Kingdom. Although all countries in Europe, except for Sweden, have taken a wide variety of prevention measures, our study focuses on the most imposing decisions that bring social interaction to a complete halt as the most effective way of stemming the spread of COVID-19 [4,5]. We identified several factors—namely, speed of response, state of emergency, social and physical distancing measures affecting mass gatherings, international travel, and borders—as being critical to reducing the virus’ transmission. By determining any links between the stringency of the measures applied and the fatality rates, we aimed to explore ways in which the results could be of value in future health emergency responses at the national/international level. Generating information based on real data for and especially during pandemic outbreaks is crucial for supporting governments and international organisations in their public health decision-making.
2. Background
After the causative virus, SARS-CoV-2, was detected in Wuhan (China) at the end of 2019 and formally identified in early January 2020, the country undertook severe interventions to mitigate and limit the spread of the virus. Kraemer and his colleagues confirmed that the drastic, agile, and aggressive health and social measures that were imposed in China have greatly helped to contain the COVID-19 pandemic [6]. In addition, they found that laboratory testing in the early stages of the epidemic was vital to limiting the virus’ spread and that the primary driver of the pandemic was the movement of humans from Wuhan to other areas before putting the city into quarantine. By mid April 2020, a new outbreak in the east of the country was already being witnessed, starting with imported cases mostly from Russia [7]. It has emerged that the traditional public health measures similar to those adopted in 2003 to curb the outbreak of severe acute respiratory syndrome (SARS), such as syndromic surveillance, the prompt isolation of patients, and enforced quarantine, are less effective with SARS-CoV-2, and, above all, we have learned that containment measures must be strict and broad, and not loosened too early. At the moment, however, there is a belief that traditional public health measures may be insufficient for containing the entire outbreak but effective for reducing the peak incidence [8].
China had faced five pandemics in the last century, three of which originated in China, namely the “Asian flu” (1957), the “Hong Kong flu” (1968), and the “Russian flu” (1977) [9]. These experiences have made the country able to react relatively quickly and effectively. However, when the disease appeared en masse in Europe, both the health profession and governments were quite unprepared. This was especially evident in Italy, one of the first countries in Europe with a large number of infected. As the number of infected grew exponentially after 21 February, the capacity of the public health system was soon under pressure. Public health measures and their level of severity at the start of the outbreak were considerably different to those adopted in China, seeing cases skyrocket [10]. In Italy, approximately 40% of cases required hospitalisation, whereas in China, the reported numbers are considerably lower (15%–20%) [11,12].
The variability in acute and critical care bed numbers across Europe is considerable. The number of critical care beds per 100,000 population ranges from 4.2 in Portugal to 29.2 in Germany, with 6.6 in the United Kingdom, 9.7 in France, and 12.5 in Italy. The number of doctors per 1000 population ranges from 1.9 in Turkey to 5.2 in Austria, while the need for critical care capacity is continually rising [1]. The increase in demand is particularly problematic in times of quick and unexpected events, where healthcare and the supporting system have no time to accommodate. When the population is old, like in Italy—which has the oldest population in Europe and the second oldest in the world, with 23 percent of older adults (65+) and a life expectancy at birth that amounts to 81 years for men and 85.3 years for women [13,14]—a disaster is likely to occur [15]. The success of public health measures to curb the transmission of the virus is a critical step in reducing the surge-capacity needs. Therefore, to plan for changes in a timely manner, we need to better understand the current situation in each country and its policy responses in past pandemics and the current one. It is only with a combination of an effective set of policies that are suitably aligned that we will be able to successfully respond to outbreaks.
3. Materials and Methods
The data for the analysis were obtained from the Oxford COVID-19 Government Response Tracker [16], which collects publicly available information on a set of indicators of government responses; POLITICO, a policy news organisation [17]; and Worldometer for the number of deaths per 1,000,000 population on 15 April 2020 [18]. The cut-off date for the data on containment measures is 1 April 2020, a date when European countries reached peak values on the stringency index that records the number and strictness of government policies, published by Hale and his colleagues [19]. Our study explores the adoption of containment measures in 24 European Union member states and the UK (Table 1).
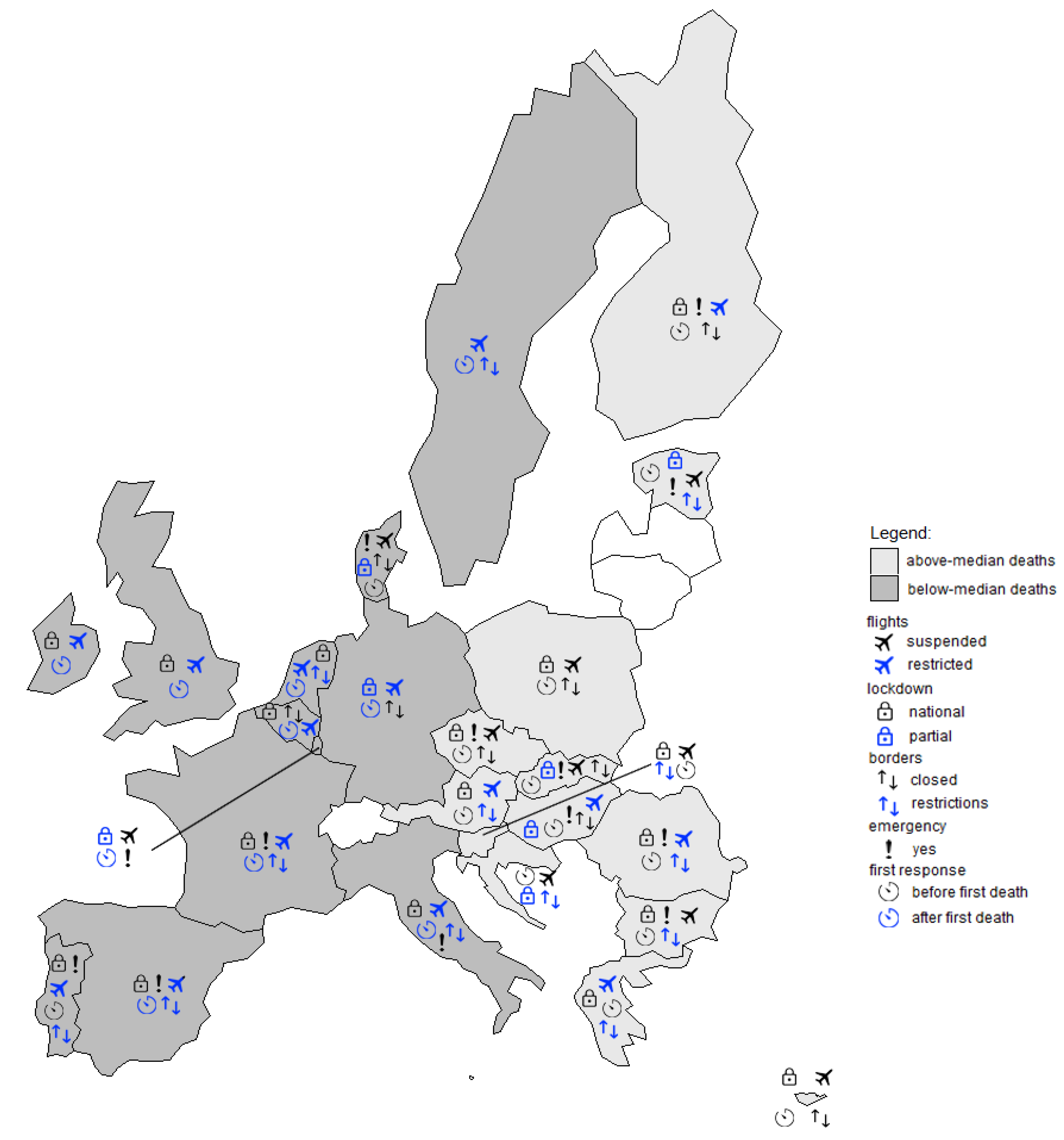
European countries for which data were missing from the sources used (Malta, Latvia, and Lithuania) were excluded from the analysis. School closures and public events were omitted from the analysis since all the examined countries, except Sweden, have taken these measures (Figure 1). For a detailed description of the measures by countries, see Appendix A.
This study adopts a crisp-set qualitative comparative analysis (csQCA) approach. csQCA is a common QCA technique used in the case of categorical variables to identify multiple causal pathways and derive logical conclusions supported by a data set. One key operation of the csQCA is Boolean minimisation to reduce complex expressions into more parsimonious expressions [20]. The obtained minimal formula allows an easier interpretation of the phenomenon of interest, which in our study is fatality in relation to the measures taken, and thus clearly shows what is common to all countries that share above-median or below-median death rates. The conditions (i.e., measures) and an outcome (i.e., fatality rate) are codified and described in Table 2.
All possible combinations of conditions (technically known as configurations) for which empirical evidence exists are presented in Table 3. The present study includes five conditions, leading to 25 configurations. To illustrate, Row 15 represents European countries that share the following set of conditions: national lockdown, emergency state declared, restrictions on borders, restricted international flights, and first measures taken after the first deaths. All countries (Spain, Italy, and France) in this set have above-median levels of death.
The following section presents the results of an analysis of necessity and sufficiency to help determine the conditions required for the outcome (analysis of necessity), and which combination of conditions produces which outcomes (analysis of sufficiency) [21]. To perform these analyses, we used the fsQCA 2.5 software [22]. To assess how well the cases in the data set fit a relation of necessity and sufficiency, we report the following parameters of fit: consistency and coverage. If consistency or coverage scores for the solution are low (below 0.75), this signals a badly specified model [23].
4. Results
The first part of the analysis is intended to examine the existence of necessary conditions. When the value for consistency exceeds 0.9 and the coverage is greater than 0.5, a condition is regarded as necessary [24]. A test of necessity reveals that the presence of TIMING is necessary for below-median deaths (Table 4).
Table 5 shows the results for the combination of conditions associated with above-median deaths. The csQCA generated three complex solutions. The analysis clearly shows that all three configurations include the condition of the late introduction of the first quarantine measures (TIMING). According to the first minimal part of the formula (AMD1), a late response, an undeclared state of emergency, and restricted—but not suspended—international flights led to above-median deaths (the presence or absence of the conditions LOCKDOWN and BORDERS are irrelevant for this configuration). These are Germany, Belgium, Sweden, the UK, the Netherlands, and Ireland. In the next solution, AMD2, one finds countries that share a late response, national lockdown, restricted international flights, and restrictions on borders (the condition EMERGENCY is redundant for this solution to emerge). Representatives of this configuration are France, Italy, and Spain. For three countries, namely Ireland, the UK, and the Netherlands, both paths are valid. This combination of conditions is seen in countries with the highest fatality rates. Similarly to AMD1, this implies that the countries opted for less stringent measures to combat COVID-19. The only stringent measure in these two reduced expressions is national lockdown. The third solution, AMD3, covers the case of Luxembourg with two stringent measures—a declared state of emergency and stopping international flights, but coupled with a late response, partial lockdowns, and restrictions on borders.
To examine which set of conditions leads to below-median deaths (Table 6), we performed a separate analysis of sufficiency. Four alternative paths lead to the outcome. The first two cover most cases. The cases in BMD1 all share an early response, stopped international flights, and restrictions on borders. This combination corresponds to Bulgaria, Croatia, Slovenia, and Estonia. The second configuration combines an early response, national lockdown, and stopped international flights (Bulgaria, Poland, Czech Republic, Slovenia, and Cyprus). The other two solutions are composed of an early response, national lockdowns put in place, an undeclared state of emergency, and restrictions on borders (BMD3); and an early response, a declared state of emergency, closed borders, and restricted international flights (BMD4). Solution BMD3 is specific to Greece, Austria, and Slovenia, while solution BMD4 corresponds to Hungary and Finland.
According to our expectations, an early response is common to all countries in the set of below-median deaths. Likewise, the suspension of international flights is seen in many countries in the set of BMD. The results also imply that these countries implemented more stringent measures compared to those facing above-median and severe deaths. In terms of redundant conditions, the state of emergency does not play a role in configurations BMD1 and BMD2; likewise, the LOCKDOWN condition has no role in BMD1 and BMD4.
5. Discussion and Conclusion
In this short study, we conducted an analysis to help understand how the responses of individual EU member states and UK are linked to the fatality rates caused by SARS-CoV-2. csQCA minimal formulas allow us to focus on the “ingredients” producing (or not) an outcome of interest, with an eye on within-case narratives and cross-case patterns [20]. Our results imply that no single combination of conditions leads to the outcome of non-high or high fatalities related to the disease. In other words, more than one combination of measures leads to either outcome. If a similar situation were to occur in the future (also including repeated waves of the virus), it would be beneficial to have all the information available from past experiences to respond as effectively as possible. This explains the important need to investigate this extreme health phenomenon from a policy perspective, promptly, spatially, broadly, and in depth, allowing for the specifics of countries and their different responses.
One month after learning of the outbreak of a new disease in Wuhan on 31 December 2019, the WHO declared a Public Health Emergency of International Concern. Depending on how they assessed the severity and magnitude of the coronavirus’ presence in the country, many governments decided to declare a state of emergency to unlock certain government powers to deal with the pandemic. However, this measure is present and absent in both outcomes; namely, in the sets of countries with above-median fatality rates and below-median ones. Therefore, our results imply that a state of emergency can bring about different outcomes based on how it is combined with other causal conditions. The same applies to the national lockdown measure since this condition is present in two of the four paths leading to the BMD outcome and in one path leading to AMD. On the other hand, the roles of closed borders and restrictions on borders in fighting the COVID-19 pandemic remain unclear.
A core condition for below-median fatality rates seems to be a quick response because this condition is present in all BMD paths. In Europe, the adoption of measures before the first deaths was a characteristic of Central and Eastern European countries and Finland. Their decisions were most likely based on the experiences of other European countries that were first exposed to the outbreak. By contrast, countries in the set with above-median fatality rates are characterised by a late response. This set contains countries with an older population with at least one other health condition (asthma, chronic obstructive pulmonary disease, diabetes, and heart problems) in Europe, while the association with smoking patterns is uncertain.
Moreover, the many interactions and trade-offs between containment measures significantly add complexity to the decision-making on combatting the COVID-19 pandemic. For example, suspending international flights is a prerequisite in two configurations related to below-median deaths (BMD1 and BMD2). By the same token, the restriction of only (but not suspended) international flights is present in two configurations leading to above-median deaths (AMD1 and AMD2). In configuration BMD4, in which only international flights were restricted, the countries (Hungary and Finland) seem to have compensated for the outcome of this decision by closing their borders quickly enough to appear in the set of countries with below-median fatalities. Therefore, we may conclude that the decision to suspend international flights might be critical in successful virus control.
The adoption of various measures at different speeds in the member states has depended not only on a health risk assessment but on an estimation of possible economic losses. The biggest challenge in decision-making in health risk prevention is to strike a balance between reducing the risk of viral transmission and the economic costs, through the sustainable development goals [4,27]. Given the varying death statistics in individual member states, it may be argued that the COVID-19 pandemic is an asymmetric health shock. Still, the global socioeconomic disruption suggests a symmetrical shock at the economic level. The EU is expected to act quickly and together to prevent the crisis from becoming a long-term demand-side crisis, which would signal its deepening and transformation into a structural one. Especially in the area of public health, we expect that globalisation will prevent any achievement of the pre-crisis level and thus restructuring will occur. For example, health diagnostics and medical treatments performed in other countries have been completely interrupted during the pandemic. Once the situation returns to normal, quarantine will probably still be required before referring a patient abroad and after a patient comes home. International medical treatment will therefore slow down, and health professionals from individual countries will need to undertake specific specialist training to acquire knowledge and develop skills that are currently lacking in their own country. Moreover, the role of the public healthcare system is expected to be strengthened as experts call for an institutionalised private–public sector partnership for future critical cases such as epidemic emergencies [28].
However, this research is subject to some limitations. The main limitation is that the results are restricted to European countries and by the conditions included in the study. Therefore, future studies could add other relevant conditions like health spending, the availability of medical equipment, and potential protective factors (e.g., plasma 25(OH)D concentrations reflecting the dietary intake of vitamin D) [29,30,31]. Likewise, it would be worthwhile to examine a link between the share of private and public healthcare systems in each country. During the pandemic, we can observe a growing preference for public hospitals [32]. However, in the most affected regions of Italy, the National Healthcare Service suffered financial cuts, privatisation, and a deprivation of human and technical resources [28]. This unexpected situation is certainly bringing new challenges to our current healthcare systems.
Author Contributions
Conceptualization: K.P.; data curation: R.S.-E.; formal analysis: K.P.; funding acquisition: K.P.; investigation: K.P. and Renata Slabe-Erker; methodology: K.P.; project administration: R.S.-E.; software: K.P.; supervision: K.P.; validation: K.P.; visualization: R.S.-E.; writing—original draft: K.P. and R.S.-E.; writing—review and editing: K.P. and R.S.-E. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Slovenian Research Agency (Grant No. P5-0096) and the APC was funded by Slovenian Research Agency (Grant No. P5-0096).
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A.

{kind=link}
Table A1.
Detailed description of the outcome variable and its antecedents by countries.
| TOTAL DEATHS 1 | SPEED OF RESPONSE 2 | STATE OF EMERGENCY | INTERNATIONAL FLIGHTS | LOCKDOWN | BORDERS AND TRAVEL | |
|---|---|---|---|---|---|---|
| Austria (AT) | AMD | Before. | No. | Restricted. Austrian Airlines grounded until April 19. | Yes. Internal movement banned, except to go to work, go shopping, or visit health facilities. Schools, universities, restaurants and large shops closed. | Open, but checks and screenings. |
| Belgium (BE) | AMD | After. | No. | Brussels Airlines is grounded. Some airlines flying but with reduced service. | Yes, except to go to work, supermarkets, health facilities and to care for other people. | Closed for "non-essential" travel. |
| Bulgaria (BG) | BMD | Before. | Yes. | Stopped. | Yes. Restrictions on internal movement. | Restrictions, travel screenings at airports since March 8. |
| Croatia (HR) | BMD | Before. | No. | Stopped. | No national lockdown, but restrictions. | Restrictions. |
| Cyprus (CY) | BMD | Before. | No. | Stopped. | Yes, internal movement banned except to go work, grocery shopping and medical treatments or to the bank. Curfew from 9 p.m. to 6 a.m. | Closed |
| Czech Rep. (CZ) | BMD | Before. | Yes. | Stopped. | Yes, national quarantine order, but essential shopping and visiting family allowed. More shops allowed to reopen as of April 9 and travel restrictions eased for workers in critical infrastructure. | Closed. |
| Denmark (DK) | AMD | Before. | Yes. | Stopped. | No national lockdown, but schools, restaurants and many shops closed until May 10. | Closed. |
| Estonia (EE) | BMD | Before. | Yes. | Stopped. | No national lockdown, but many shops closed. | Restrictions, health screenings at borders. |
| Finland (FI) | BMD | Before. | Yes. | Restricted. | Yes. Restrictions on internal movement. | Yes. Traveling abroad banned until April 13. |
| France (FR) | AMD | After. | Yes. | Restricted. | Yes. Provide form for authorities when outside. | Open. |
| Germany (DE) | AMD | After. | No. | Restricted. | Partial lockdown, with rules differing across states. Many shops closed. | Closed for "non-essential" travel. Checks at borders. |
| Greece (EL) | BMD | Before. | No. | Restricted. Aegean Airlines has suspended all international flights, apart from weekly flights to Brussels. | Yes. Internal movement banned except to go to work, grocery shopping and for medical reasons. Curfew on island of Mykonos. | Borders with neighboring Albania, North Macedonia and Turkey are closed. |
| Hungary (HU) | BMD | Before. | Yes. | Restricted. | No national lockdown, but all citizens asked to stay at home. Compulsory home quarantine order can be issued. | Closed. |
| Ireland (IE) | AMD | After. | No. | Restricted. | Yes, except for grocery shopping and essential family visits. Non-essential shops closed. | No. |
| Italy (IT) | AMD | After. | Yes. | Restricted. | Yes, strict lockdown and non-essential production halted. Bookshops, stationary shops and stores for children clothes allowed to reopen as of April 14. | Open, but all neighboring countries have restricted entry. |
| Luxembourg (LU) | BMD | After. | Yes. | Stopped. | No national lockdown, but non-essential shops closed and home working advised. | No. |
| Netherlands (NL) | AMD | After. | No. | Restricted. | Yes, but exceptions for shopping. | Restrictions for Non-EU citizens. |
| Poland (PL) | BMD | Before. | No. | Stopped. | Yes. Non-essential movement banned. | Closed. |
| Portugal (PT) | AMD | Before. | Yes. | Restricted. | Yes. Non-essential movement banned. | Restrictions at border with Spain. |
| Romania (RO) | BMD | Before. | Yes. | Stopped to Italy, Spain, Germany and France. | Yes. Restrictions. | Restrictions. |
| Slovakia (SK) | BMD | Before. | Yes. | Stopped. | No, but all schools closed. | Closed. |
| Slovenia (SI) | BMD | Before. | No. | Stopped. | Yes. Non-essential movement banned. | Restrictions. |
| Spain (ES) | AMD | After. | Yes. | Restricted. All flights to and from Italy stopped. | Yes. National lockdown extended, non-essential economic activity stopped. Certain sectors allowed to work again as of April 14. | Restrictions. |
| Sweden (SE) | AMD | After. | No. | Restricted. | No. | Ban on non-essential travel since March 17. |
| United Kingdom (UK) | AMD | After. | No. | Restricted. | Yes, non-essential movement banned, exceptions for necessary shopping, medical treatment and travelling to work. | No. |
Note: 1 Total deaths as of 15th April 2020: AMD – above-median deaths, BMD – below-median deaths; 2 Speed of response: Before – first measure was implemented before first death, After – first measure was implemented after first death. Sources: Worldometer; Politico - Coronavirus in Europe and Blavatnik School of Government, University of Oxford: Oxford COVID-19 Government Response Tracker.
References
- World Health Organization. Strengthening the Health System Response to COVID-19; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Pandemic Influenza Preparedness and Response; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- World Health Organization. Pandemic Influenza Risk Management WHO Interim Guidance; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- McNeil, D. The Virus Can Be Stopped, but Only With Harsh Steps, Experts Say. Available online: https://www.nytimes.com/2020/03/22/health/coronavirus-restrictions-us.html (accessed on 23 March 2020).
- Kraemer, M.U.G.; Yang, C.-H.; Gutierrez, B.; Wu, C.-H.; Klein, B.; Pigott, D.M.; du Plessis, L.; Faria, N.R.; Li, R.; Hanage, W.P.; et al. The effect of human mobility and control measures on the COVID-19 epidemic in China. Science 2020, 368, 493–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, K.R. China’s new Covid-19 hotspot on Russian border raises tensions between two allies. Available online: https://www.newsweek.com/china-russia-tensions-border-coronavirus-1498785 (accessed on 19 April 2020).
- Wilder-Smith, A.; Chiew, C.J.; Lee, V.J. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect. Dis. 2020, 20, e102–e107. [Google Scholar] [CrossRef] [Green Version]
- Qin, Y.; Zhao, M.J.; Tan, Y.Y.; Li, X.Q.; Zheng, J.D.; Peng, Z.B.; Feng, L.Z. History of influenza pandemics in China during the past century. Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39, 1028–1031. [Google Scholar] [PubMed]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Lazzerini, M.; Putoto, G. COVID-19 in Italy: Momentous decisions and many uncertainties. Lancet Glob. Health 2020, 8, E641–E642. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Population Reference Bureau Countries With the Oldest Populations in the World. Available online: https://www.prb.org/countries-with-the-oldest-populations/ (accessed on 23 March 2020).
- Statista Life Expectancy at Birth in Italy from 2002 to 2019, by Gender. Available online: https://0-www-statista-com.brum.beds.ac.uk/statistics/568929/life-expectancy-at-birth-by-gender-in-italy/ (accessed on 24 March 2020).
- Rhodes, A.; Ferdinande, P.; Flaatten, H.; Guidet, B.; Metnitz, P.G.; Moreno, R.P. The variability of critical care bed numbers in Europe. Intensive Care Med. 2012, 38, 1647–1653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blavatnik School of Government, University of Oxford, [database] Oxford COVID-19 Government Response Tracker. Available online: https://www.bsg.ox.ac.uk/research/research-projects/oxford-covid-19-government-response-tracker (accessed on 4 April 2020).
- Politico, [database] Coronavirus in Europe. Available online: https://www.politico.eu/article/europes-coronavirus-lockdown-measures-compared/ (accessed on 4 April 2020).
- Worldometer, [database] Reported Cases and Deaths by Country, Territory, or Conveyance. Available online: https://www.worldometers.info/coronavirus/ (accessed on 4 April 2020).
- Hale, T.; Webster, S.; Petherick, A.; Phillips, T.; Kira, B. Data use policy: Creative commons attribution CC by standard. 2020. Available online: https://www.bsg.ox.ac.uk/research/research-projects/coronavirus-government-response-tracker (accessed on 29 April 2020).
- Rihoux, B.; De Meur, G. Crisp-set qualitative comparative analysis (csQCA). In Configurational Comparative Methods: Qualitative Comparative Analysis (QCA) and Related Techniques; Benoît Rihoux, C.C.R., Ed.; Sage Publications: Shozende Oaks, CA, USA, 2009; pp. 33–68. [Google Scholar]
- Rihoux, B.; Ragin, C. Configurational Comparative Methods: Qualitative Comparative Analysis (QCA) and Related Techniques; Sage Publications: Shozende Oaks, CA, USA, 2012. [Google Scholar]
- Ragin, C.C.; Davey, S. fs/QCA [Computer Program], Version 2.5. University of Arizona, Tucson. 2009. Available online: http://www.socsci.uci.edu/~cragin/fsQCA/software.shtml. (accessed on 17 January 2010).
- Legewie, N. An introduction to applied data analysis with qualitative comparative analysis. Forum. Qual. Soc. Res. 2013, 14. [Google Scholar] [CrossRef]
- Schneider, C.Q.; Wagemann, C. Set-Theoretic Methods: A User’s Guide for Qualitative Comparative Analysis and Fuzzy Sets in Social Science; Cambridge University Press: Cambridge, UK, 2012. [Google Scholar]
- Ragin, C. Redisigning Social Inquiry: Fuzzy Sets and Beyond; University of Chicago Press: Chicago, IL, USA, 2008; ISBN 9780226702735. [Google Scholar]
- Rihoux, B.; Ragin, C.C. Configurational Comparative Methods: QCA and Related Techniques; SAGE: Los Angeles, CA, USA, 2009; ISBN 1412942357. [Google Scholar]
- Gong, B.; Zhang, S.; Yuan, L.; Chen, K.Z. A balance act: Minimizing economic loss while controlling novel coronavirus pneumonia. Available online: https://0-www-tandfonline-com.brum.beds.ac.uk/doi/full/10.1080/23812346.2020.1741940 (accessed on 23 March 2020).
- Armocida, B.; Formenti, B.; Ussai, S.; Palestra, F.; Missoni, E. The Italian health system and the COVID-19 challenge. Lancet Public Health 2020, 5, E253. [Google Scholar] [CrossRef]
- Ilie, P.C.; Stefanescu, S.; Smith, L. The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality. Aging Clin. Exp. Res. 2020, 1, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Crowe, F.L.; Steur, M.; Allen, N.E.; Appleby, P.N.; Travis, R.C.; Key, T.J. Plasma concentrations of 25-hydroxyvitamin D in meat eaters, fish eaters, vegetarians and vegans: Results from the EPIC-Oxford study. Public Health Nutr. 2011, 14, 340–346. [Google Scholar] [CrossRef] [Green Version]
- Alipio, M. Vitamin D Supplementation could Possibly Improve Clinical Outcomes of Patients Infected with Coronavirus-2019 (COVID-2019). Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3571484 (accessed on 9 April 2020).
- IBIS World Effects of COVID-19 on Global Healthcare Systems. Available online: https://www.ibisworld.com/industry-insider/coronavirus-insights/effects-of-covid-19-on-global-healthcare-systems/ (accessed on 16 April 2020).
Figure 1.
COVID-19 public health measures.

Table 1.
A list of countries with the corresponding country codes included in the study.
| Country Name | Country Code |
|---|---|
| Austria | AT |
| Belgium | BE |
| Bulgaria | BG |
| Croatia | HR |
| Cyprus | CY |
| Czech Rep. | CZ |
| Denmark | DK |
| Estonia | EE |
| Finland | FI |
| France | FR |
| Germany | DE |
| Greece | EL |
| Hungary | HU |
| Ireland | IE |
| Italy | IT |
| Luxembourg | LU |
| Netherlands | NL |
| Poland | PL |
| Portugal | PT |
| Romania | RO |
| Slovakia | SK |
| Slovenia | SI |
| Spain | ES |
| Sweden | SE |
| United Kingdom | UK |
Table 2.
Coding and describing the conditions and outcomes.
| Condition/Outcome | Codification | Description |
|---|---|---|
| Above-median deaths (outcome) | AMD | 1 = more than 44 deaths per 1,000,000 population |
| Below-median deaths (outcome) | BMD | 0 = less than 44 deaths per 1,000,000 population |
| Speed of response | TIMING | 0 = first measure (school closure or public event cancellation) taken after first death, 1 = first measure taken before first death |
| State of emergency | EMERGENCY | 0 = no, 1 = yes |
| Borders and travel | BORDERS | 0 = restrictions, 1 = closed/banned |
| International flights | FLIGHTS | 0 = restricted, 1 = suspended |
| Lockdown | LOCKDOWN | 0 = no/partial lockdown, 1= yes |
Table 3.
Truth table.
| Row | Conditions | No. of Cases | CASE | Raw Consistency (Outcome) | ||||
|---|---|---|---|---|---|---|---|---|
| LOCKDOWN | EMERGENCY | BORDERS | FLIGHTS | TIMING | ||||
| 1 | 0 | 1 | 0 | 1 | 0 | 1 | LU | 100% (1) |
| 2 | 0 | 1 | 1 | 1 | 1 | 2 | SK, DK | 50% |
| 3 | 1 | 1 | 0 | 1 | 1 | 1 | BG | 100% (0) |
| 4 | 1 | 0 | 1 | 1 | 1 | 2 | PL, CY | 100% (0) |
| 5 | 0 | 0 | 0 | 1 | 1 | 1 | HR | 100% (0) |
| 6 | 0 | 1 | 1 | 0 | 1 | 1 | HU | 100% (0) |
| 7 | 1 | 1 | 1 | 0 | 1 | 1 | FI | 100% (0) |
| 8 | 1 | 0 | 0 | 0 | 1 | 2 | EL, AT 1 | 100% (0) |
| 9 | 1 | 1 | 1 | 1 | 1 | 1 | CZ | 100% (0) |
| 10 | 1 | 1 | 0 | 0 | 1 | 2 | RO, PT | 50% |
| 11 | 1 | 0 | 0 | 1 | 1 | 1 | SI | 100% (0) |
| 12 | 0 | 0 | 1 | 0 | 0 | 1 | DE | 100% (0) |
| 13 | 1 | 0 | 0 | 0 | 0 | 3 | IE, NL, UK | 100% (1) |
| 14 | 0 | 0 | 0 | 0 | 0 | 1 | SE | 100% (1) |
| 15 | 1 | 1 | 0 | 0 | 0 | 3 | FR, IT, ES | 100% (1) |
| 16 | 1 | 0 | 1 | 0 | 0 | 1 | BE | 100% (1) |
| 17 | 0 | 1 | 0 | 1 | 1 | 1 | EE | 100% (0) |
Note: The rows use the following labelling system: 1 = set membership, 0 = no set membership. Since they do not add empirical evidence, rows 25-17 are not shown in the above table. 1 Austria is a country with a median death rate. The decision to place it in the group of member states with below-median deaths (BMD) is due to the fact that the number of deaths in Austria is below the average in the observed countries (98 deaths/1 million population).
Table 4.
Individual conditions: test of necessity.
| Condition | Consistency for Above-Median Deaths | Consistency for Below-Median Deaths |
|---|---|---|
| LOCKDOWN | 0.67 | 0.69 |
| EMERGENCY | 0.50 | 0.54 |
| BORDERS | 0.25 | 0.46 |
| FLIGHTS | 0.17 | 0.80 |
| TIMING | 0.17 | 1 (cov.: 0.87) |
| lockdown | 0.33 | 0.31 |
| emergency | 0.50 | 0.46 |
| borders | 0.75 | 0.54 |
| flights | 0.83 | 0.33 |
| timing | 0.83 | 0.00 |
Note: Capital letters denote the condition’s presence; lower-case ones point to the condition’s absence.
Table 5.
Configurations for above-median deaths (AMD) with a consistency cut-off of 1.
| Condition | Configurations | ||
|---|---|---|---|
| AMD1 | AMD2 | AMD3 | |
| TIMING | ⊗ | ⊗ | ⊗ |
| LOCKDOWN | ● | ⊗ | |
| EMERGENCY | ⊗ | ● | |
| BORDERS | ⊗ | ⊗ | |
| FLIGHTS | ⊗ | ⊗ | ● |
| Consistency | 1 | 1 | 1 |
| Raw coverage | 0.50 | 0.50 | 0.08 |
| Unique coverage | 0.25 | 0.25 | 0.08 |
| Solution consistency 1 | 1 | ||
| Solution coverage 2 | 0.83 | ||
Table 6.
Configurations for below-median deaths (BMD) with a consistency cut-off of 1.
| Condition | Configurations | |||
|---|---|---|---|---|
| BMD1 | BMD2 | BMD3 | BMD4 | |
| TIMING | ● | ● | ● | ● |
| LOCKDOWN | ● | ● | ||
| EMERGENCY | ⊗ | ● | ||
| BORDERS | ⊗ | ⊗ | ● | |
| FLIGHTS | ● | ● | ⊗ | |
| Consistency | 1 | 1 | 1 | 1 |
| Raw coverage | 0.31 | 0.38 | 0.23 | 0.15 |
| Unique coverage | 0.15 | 0.23 | 0.15 | 0.15 |
| Solution consistency 1 | 1 | |||
| Solution coverage 2 | 0.85 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Primc, K.; Slabe-Erker, R. The Success of Public Health Measures in Europe during the COVID-19 Pandemic. Sustainability 2020, 12, 4321. https://0-doi-org.brum.beds.ac.uk/10.3390/su12104321
AMA Style
Primc K, Slabe-Erker R. The Success of Public Health Measures in Europe during the COVID-19 Pandemic. Sustainability. 2020; 12(10):4321. https://0-doi-org.brum.beds.ac.uk/10.3390/su12104321
Chicago/Turabian StylePrimc, Kaja, and Renata Slabe-Erker. 2020. "The Success of Public Health Measures in Europe during the COVID-19 Pandemic" Sustainability 12, no. 10: 4321. https://0-doi-org.brum.beds.ac.uk/10.3390/su12104321
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.