
Conservative Treatment in Tracheobronchial Injuries—An Institutional Report



Division of Thoracic Surgery, “A. Businco” Oncology Hospital, A.R.N.A.S. “G. Brotzu”, 09121 Cagliari, Italy
*
Author to whom correspondence should be addressed.
Surgeries 2021, 2(3), 237-243; https://0-doi-org.brum.beds.ac.uk/10.3390/surgeries2030024
Submission received: 14 June 2021
/
Revised: 25 June 2021
/
Accepted: 29 June 2021
/
Published: 1 July 2021
Abstract
:Tracheobronchial injuries are rare but potentially high-impact events with significant morbidity and mortality. Common etiologies include blunt or penetrating trauma, often combined with various complex injuries, while iatrogenic injury usually occurs during operation, intubation, or bronchoscopy. An early and accurate diagnosis and a multidisciplinary approach in a center experienced in treating airway lesions are essential to obtain favorable results. For a long time, surgery has been considered the treatment of choice for post-traumatic airway lesions. However, recent reports have shown a paradigm shift in the management of tracheal injury towards a conservative approach, especially in treating iatrogenic lesions. In our experience of 11 consecutive patients, although there are still definitive indications for surgery, we demonstrated the effectiveness of conservative treatment in patients with mixed varieties of tracheal injury by etiology, extension, and complications.
1. Introduction
Tracheobronchial injuries (TBI) are potentially life-threatening clinical scenarios occurring after blunt and penetrating thoracic traumas or, more rarely, after iatrogenic procedures. The formers are mostly caused by sharp objects, such as knives, ice picks, or gunshot wounds [1]. The latters can occur during endotracheal intubations, surgery, endoscopic tracheobronchial procedures, or percutaneous tracheostomy [2]. Unfortunately, many patients die before a blunt or penetrating tracheal injury diagnosis can be obtained unless promptly recognized and treated. Therefore, the incidence of lesions due to this etiology could be underestimated [3]. About 0.005% of all intubations have a tracheal tear complication. This incidence increases up to 0.19% in patients intubated with a double-lumen tube and up to 1% during percutaneous dilatational tracheostomy [4]. Although well-known and extensively reported in the literature, the best evidence practice for the management needs clarification. Historically, surgical repair has been considered the gold-standard treatment [5]. However, a conservative approach has been described in selected cases, although it did not exceed the 50% in the reported series [6]. We describe herein the results of non-interventional conservative treatment in a consecutive series of selected TBI patients independently of etiology, location, or size of injury or diagnostic delay.
2. Materials and Methods
We retrospectively reviewed the clinical records of 11 patients with tracheobronchial injuries between February 2015 and March 2021, diagnosed in our Division. Nine female patients (81.8%) reported iatrogenic lesions by endotracheal-tube (ETT) placement, while two (18.2%) combined stab wound injuries were observed in male patients (mean age 49.4 years, SD ± 19.5). The diagnosis was carried out by computed tomographic (CT) scan and were assessed by flexible bronchoscopy in all the cases. The time comprised between the iatrogenic intubation or trauma and the endoscopic evaluation was defined as diagnostic delay (DL).
In order to identify the size and location of TBI, a bronchoscopy was mandatory in all the cases. According to Cardillo classification (Table 1), all patients with TBI in our series were defined level I to level IIIA lesions, without signs of oesophageal injury or mediastinitis [7].
The most common sign observed in our series was the respiratory impairment and the subcutaneous emphysema, radiologically associated with pneumomediastinum, pneumothorax (PNX), and or hemothorax. Therefore, we placed a chest tube when clinically needed and removed it without evidence of continuous air leak or bleeding for almost 24 h.
The eligibility criteria for conservative treatment included: (i) refusal of the operation by the patient or the legal guardian, (ii) bad physical condition in severely ill patients, (iii) non-progressive mediastinal and/or subcutaneous emphysema, and (iv) absence of esophageal injury. This management was the chosen treatment independently of the injury length, location, cause, and DL.
The conservative procedure consisted of intubation with a well-matched ETT (large bore, low-pressure-high-volume-cuff) for 7–10 days with varying ventilation modalities, depending on each patient’s situation. For small upper tracheal tears, the cuff of the ETT was advanced distally to the lesion to exclude the ventilator overpressure on the damaged wall, avoiding cuff hyperinflation. When the length or location of the injury did not allow this management, slight inflation of the cuff was necessary to keep the gap between the wound edges open and prevent retention with the continuous measurement of the cuff pressure. For selected TBI and clinical scenarios without severe complications, the conservative treatment in patients spontaneously breathing was the initial approach.
Blood and serum analyses were performed daily to assess patients’ clinical status and monitoring infection index in the intensive care unit. The bronchoscopic control every other day and broad-spectrum antibiotic therapy to determine the state of the tear’s healing and clean up the situs before being woken and moved to the ward 24 h after the extubation, completed the procedure.
Two patients did not need intubation due to permissive clinical conditions and were managed conservatively in the spontaneous breath, with broad-spectrum antibiotic therapy, steroids, cough suppressant, parenteral nutrition for the first two days, and in-ward monitoring.
If no other incidences were detected, we performed a bronchoscopy assessment on the discharge day and month one and month three follow-up.
Statistical Analysis
Postoperative outcomes were tested based on different variables. Categorical variables were described as frequencies and percentages, while mean values and standard deviation (SD) were used to express quantitative variables. Pearson’s correlation coefficient and Kruskal-Wallis test were used as appropriate. All statistical tests were two-tailed, with a significance level of 0.05. MedCalc Statistical Software version 20.008 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org, accessed on 30 June 2021) was used for the analysis.
3. Results
As reported in Table 2, all patients with TBI treated conservatively survived, and the management was effective in all the cases. In addition, no radiological evidence of mediastinitis on thoracic CT scan or progressive TBI signs and symptoms were noted in the following days.
In the iatrogenic TBI group, from the mere point of the tear extension, the mean length was 3.2 cm (SD ± 1.15). On the other hand, the thickness of the lesions classified according to Cardillo showed a predominance of II level (55.6%), followed by three cases of IIIA level (33.3%) and one only I level case (11.1%).
In one of the two patients who received penetrating TBI, we found a cartilaginous wound combined with an IIIA membranous pars lesion (2 cm), while in the other patient, we detected only an anterior trachea wall injury.
All the TBI diagnoses suffered from a mean DL of 16.5 h (SD ± 13.4) who did not statistically significantly affected the ETT length of stay (mean 8.3 days, SD ± 1.4) and the LOS (mean 14.2 days, SD ± 2.6).
Chest tubes were placed in six patients (54.5%) needing PNX treatment, and this procedure did not statistically affect the tested outcomes.
In our series, we did not find a correlation between TBI length or site and the LOS. Conversely, morphological characteristics of the lesion were statistically significantly associated with the LOS (p = 0.040).
Finally, the associated presenting symptoms or signs reported in Table 1 were not statistically correlated with the LOS and MV length.
All the patients were asymptomatic three months after the procedure, and light scars were the only visible sequelae. One patient showed at first control (30-days) small granuloma quickly cauterized by laser without revealing any stenosis (Figure 1).
4. Discussion
TBI are life-threatening conditions, independently from their etiologies, and surgical repair is still considered the best treatment. However, there are not high-level recommendations to support this choice [8].
Known risk factors for TBI include female sex and the increasing age of patients undergoing surgery [9]. The high number of TBI cases reported in our Institution during such a short time may be related to the lack of other general thoracic surgery centers where interventional bronchoscopy is performed all over our region.
As mentioned in our series, the iatrogenic TBI is the most frequent scenario. It is often sustained by emergency intubation, inadequate ETT diameter, inappropriate use of stylets, balloon overinflation damaging the tracheal mucosa, vigorous and persistent coughing of the patient when awakening from general anesthesia [9].
We support the idea that (i) an injury caused by ETT usually occurs in the cervicothoracic membranous wall, (ii) the damages caused by sudden movements of ETT due to the coughing or neck movements occur more often in the distal membranous wall near the carina, whereas (iii) the injuries caused by blunt or penetrating traumas are frequently located in the cartilaginous cervical part of the trachea due to the shield provided by the sternum and chest rib cage [6].
In our series, the minimum delay between diagnosis and procedure allows considering improbable another mechanism that is not a direct injury in patients who underwent intubation. Likewise, the airway procedures were performed in all but two cases (stab-wounds injuries) in our series and were rated as complicated by the anesthesiologist in six patients.
The higher incidence of TBI in female patients we reported, also confirmed by the literature, is probably explainable by the shorter average tracheal length in women leading to the risk of ETT oversizing.
When a tracheal lesion is confirmed, anesthesiologists and thoracic surgeons should quickly assess an individualized therapy regime, avoiding any delay in diagnosis to limit the risk of complications as mediastinitis and PNX [10].
The diagnostic delay in our series is related to the fact that many patients (n = 10) were transferred to our Division from other hospitals with only suspected diagnoses. Nevertheless, the DL was similar to those of other reported series [6,9].
Lesions discovered during an open thoracic surgery procedure are repaired at the same time [10] and, even if the diagnosis time does not seem to influence a not negligible intrinsic mortality rate, the delayed surgical repair of the tear doubles the risk of death in patients whose tracheal rupture is detected after surgery [11]. In those patients with severe comorbidities, surgical closure via open chest surgery showed a mortality of up to 71% [5].
Thus, over the past 20 years, non-operative management of TBI has been suggested for selected patients in the following circumstances: stable vital signs, easy achievement of adequate functional respiratory status under mechanical or spontaneous ventilation, absence of sepsis, short ruptures, and delayed diagnosis [12]. Other suggested criteria for conservative treatment include the following: absence of esophageal injury, minimal mediastinal air, and non-progressive pneumomediastinum or subcutaneous emphysema [13].
Another unclear aspect playing a fundamental role in deciding on the correct approach was the range of TBI length that should be treated surgically or conservatively, especially in those injuries between 2 and 4 cm. This can be better determined now based on anatomy, clinical status, comorbidities, and on-site expertise [14].
In spontaneously breathing patients, at the time of diagnosis, medical treatment includes a broad-spectrum antibiotic therapy against the tracheobronchial flora, antitussive agents, antiseptic, anti-inflammatory aerosol therapy, and chest tube insertion if required [6].
In all cases where mechanical ventilation is needed (at the time of diagnosis) due to acute respiratory failure, coma, or multi-organ failure, conservative management provides positioning the tracheal tube distal to the tracheal lesion, continuously monitoring the cuff pressure, and intercostal drain insertion, if required. This strategy is effective in patients with lacerations in the cervical part of the trachea. In patients mechanically ventilated with lacerations close to the carina, it is not easy to position the cuff distal to the tracheal rupture and avoid dislocation of the tube tip into the mediastinum. Therefore, the tube must be sited close to the carina, under bronchoscopy with continuous cuff pressure monitoring, for a limited period [15].
As described in our case series, the conservative approach to TBI was independent of the defect length, as reported in the most extensive case series in the literature [6,12,16]. Conversely, the depth of transmural involvement and the morphology of the injury should represent a more precise staging system in helping the decision-making process. In all our TBI cases, no level IIIB was found, and a conservative approach was considered a safe treatment as described by Cardillo et al. [7]. In addition, the extension of the tracheal wall lesion was the only variable determining a lengthening of the in-hospital stay in our patient series as a result of slower “per primam” healing.
5. Conclusions
In the absence of guidelines, TBI remains a challenging clinical entity to manage. In the event of a tracheal tear, an initial conservative approach might be appropriate with intense monitoring and proper surgical consult, and it should be considered a valuable alternative to the well-established operative treatment. We hope that more studies in the future can aid in bridging the current gap in knowledge regarding the optimal management and role of less-invasive therapies among this set of patients.
Author Contributions
Conceptualization: R.C. and P.A.F.; methodology: R.C. and P.A.F.; software P.A.F.; validation: R.C., S.S., M.P.-S. and P.A.F.; formal analysis: P.A.F.; investigation: R.C. and P.A.F.; resources: R.C., S.S., M.P.-S. and P.A.F.; data curation: R.C., S.S., M.P.-S. and P.A.F.; writing—original draft preparation: R.C., S.S., M.P.-S. and P.A.F.; writing—review and editing: R.C., S.S., M.P.-S. and P.A.F.; visualization: R.C., S.S., M.P.-S. and P.A.F.; supervision: P.A.F.; project administration: P.A.F.; funding acquisition: none to declare. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki. Ethical review and approval were waived for this study due to its retrospective observatory nature.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors would like to acknowledge the nurse staff operating in our Division of Thoracic Surgery, in particular: Bonaria Tatti, Raimonda Pintus, and Fabrizio Aresu.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lyons, J.D.; Feliciano, D.V.; Wyrzykowski, A.D.; Rozycki, G.S. Modern Management of Penetrating Tracheal Injuries. Am. Surg. 2013, 79, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Carretta, A.; Ciriaco, P.; Bandiera, A.; Negri, G. Diagnostic and therapeutic approach to post-traumatic tracheobronchial injuries. Signa Vitae 2021, 17, 10–19. [Google Scholar]
- Kummer, C.; Netto, F.S.; Rizoli, S.; Yee, D. A review of traumatic airway injuries: Potential implications for airway assessment and management. Injury 2007, 38, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Misak, V.B.; Beraković, A.P.; Vukusić, I.; Kogler, J.; Pazanin, L.; Ozegović, S.O. Postintubation tracheal injuries—Case series and literature review. Acta Clin. Croat. 2012, 51, 467–471. [Google Scholar] [PubMed]
- Hofmann, H.; Rettig, G.; Radke, J.; Neef, H.; Silber, R. Iatrogenic ruptures of the tracheobronchial tree. Eur. J. Cardio Thorac. Surg. 2002, 21, 649–652. [Google Scholar] [CrossRef] [Green Version]
- Jougon, J.; Ballester, M.; Choukroun, E.; Dubrez, J.; Reboul, G.; Velly, J.F. Conservative treatment for postintubation tracheobron-chial rupture. Ann. Thorac. Surg. 2000, 69, 216–220. [Google Scholar] [CrossRef]
- Cardillo, G.; Carbone, L.; Carleo, F.; Batzella, S.; Jacono, R.D.; Lucantoni, G.; Galluccio, G. Tracheal lacerations after endotracheal intubation: A proposed morphological classification to guide non-surgical treatment. Eur. J. Cardio Thorac. Surg. 2010, 37, 581–587. [Google Scholar] [CrossRef]
- Marty-Ané, C.H.; Picard, E.; Jonquet, O.; Mary, H. Membranous tracheal rupture after endotracheal intubation. Ann. Thorac. Surg. 1995, 60, 1367–1371. [Google Scholar] [CrossRef]
- Kaloud, H.; Prause, G.; List, W.F.; Smolle-Juettner, F.-M. Iatrogenic Ruptures of the Tracheobronchial Tree. Chest 1997, 112, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Miñambres, E.; Burón, J.; Ballesteros, M.A.; Llorca, J.; Muñoz, P.; Castro, A.G. Tracheal rupture after endotracheal intubation: A literature systematic review. Eur. J. Cardio Thorac. Surg. 2009, 35, 1056–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, T.; Volz, K.; Dienemann, H.; Hoffmann, H. Incidence and treatment modalities of tracheobronchial injuries in Germany. Interact. Cardiovasc. Thorac. Surg. 2009, 8, 571–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conti, M.; Pougeoise, M.; Wurtz, A.; Porte, H.; Fourrier, F.; Ramon, P.; Marquette, C.-H. Management of Postintubation Tracheobronchial Ruptures. Chest 2006, 130, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Ross, H.M.; Grant, F.J.; Wilson, R.S.; Burt, M.E. Nonoperative Management of Tracheal Laceration During Endotracheal Intubation. Ann. Thorac. Surg. 1997, 63, 240–242. [Google Scholar] [CrossRef]
- Grewal, H.S.; Dangayach, N.S.; Ahmad, U.; Ghosh, S.; Gildea, T.; Mehta, A.C. Treatment of Tracheobronchial Injuries. Chest 2019, 155, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Deja, M.; Menk, M.; Heidenhain, C.; Spies, C.D.; Heymann, A.; Weidemann, H.; Branscheid, D.; Weber-Carstens, S. Strategies for diagnosis and treatment of iatrogenic tracheal ruptures. Minerva Anestesiol. 2011, 77, 1155–1166. [Google Scholar] [PubMed]
- Andrés, A.G.C.; Díez, F.J.M.; Herrero, P.A.; Gude, V.D.H.; Cabrero, E.L.; de Miguel Porch, E.; De Nicolás, J.L.M. Successful conservative management in iatrogenic tracheobronchial injury. Ann. Thorac. Surg. 2005, 79, 1872–1878. [Google Scholar] [CrossRef] [PubMed]
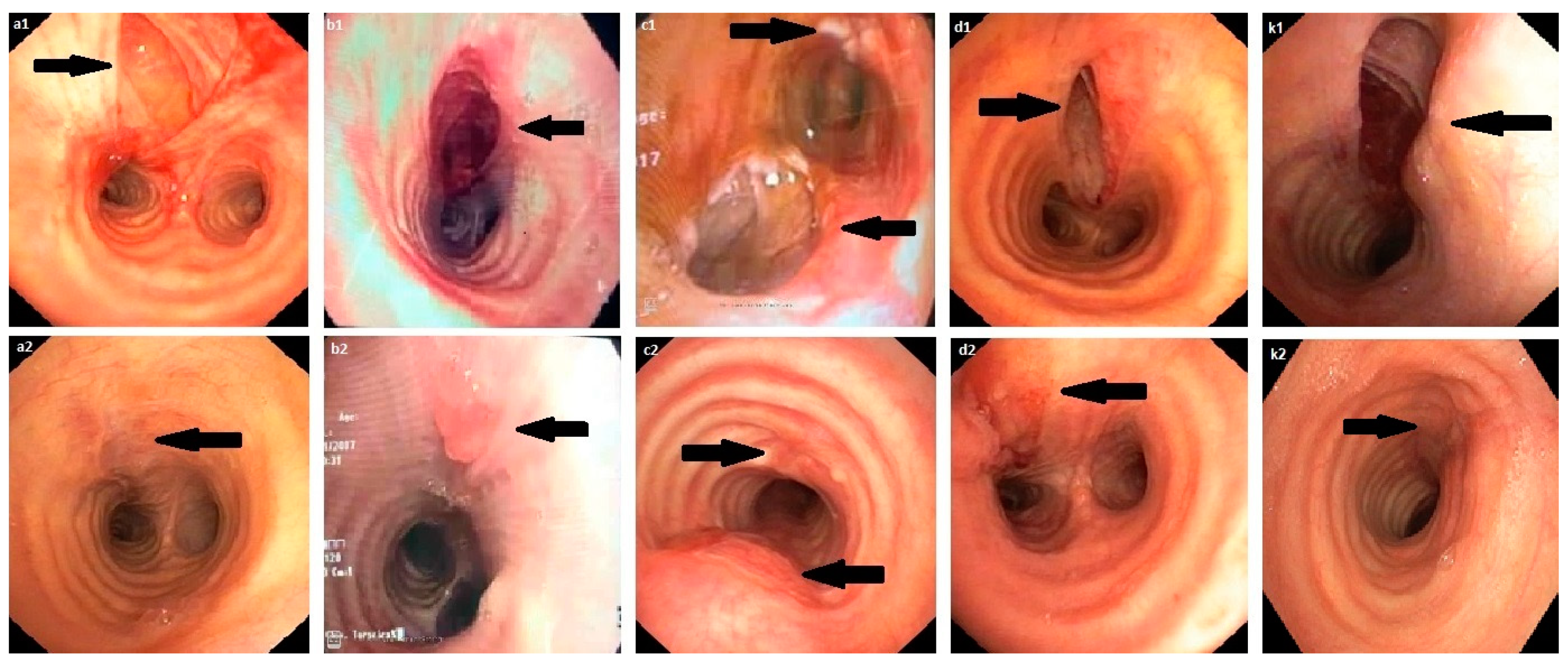
Figure 1.
Endoscopic findings at the time of diagnosis and one month after in patients with tracheobronchial injuries (Division of Thoracic Surgery, “A. Businco” Oncology Hospital, Cagliari, Italy). From (a1–k1): endoscopic TBI visualization at time of diagnosis in patients as listed in Table 2; form (a2–k2): endoscopic visualization of TBI one month after diagnosis in patients as listed in Table 2.
Figure 1.
Endoscopic findings at the time of diagnosis and one month after in patients with tracheobronchial injuries (Division of Thoracic Surgery, “A. Businco” Oncology Hospital, Cagliari, Italy). From (a1–k1): endoscopic TBI visualization at time of diagnosis in patients as listed in Table 2; form (a2–k2): endoscopic visualization of TBI one month after diagnosis in patients as listed in Table 2.


{kind=link}
Table 1.
Proposal for classification of postintubation tracheal lesion made by Cardillo et al. [7] in 2010.
Table 1.
Proposal for classification of postintubation tracheal lesion made by Cardillo et al. [7] in 2010.
| Level | Definition |
|---|---|
| Level I | Mucosal or submucosal tracheal involvement without mediastinal emphysema or oesophageal injury |
| Level II | Tracheal lesion up to the muscular wall with subcutaneous or mediastinal emphysema without oesophageal injury or mediastinitis |
| Level IIIA | Complete laceration of the tracheal wall with oesophageal or mediastinal soft-tissue hernia without oesophageal injury or mediastinitis |
| Level IIIB | Any laceration of the tracheal wall with oesophageal injury or mediastinitis |
Table 2.
Patients’ characteristics, endoscopic findings, and outcomes.
| Case | Sex | Age (Years) | Etiology | Reason for Intubation | Difficult Intubation | Presenting Symptoms/Radiological Findings | CT/Duration (Days) | Endoscopic Findings/Site | Classification sec. Cardillo et al. [7] | Length (cm) | DL (Hours) | Type of Treatment | MV Length (Days) | LOS (Days) | Endoscopic Follow-Up (3 Months) | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| a. | F | 56 | IAT | Hysterectomy | Yes | RI, SE, ME, PNX | No | linear tear TTMP-RB | II | 3.5 | 8 | CT—ETT | 7 | 11 | Scar | UR |
| b. | F | 65 | IAT | RI during cystoscopy | Yes—EM | RI, SE, ME, PNX | Yes/2 | linear tear TTMP | II | 6 | 12 | CT—ETT | 9 | 13 | Scar | UR |
| c. | M | 18 | SW | N/A | N/A | RI, SE, ME, PNX, HT | Yes/3 | linear lesion CTMP/circular lesion CTCP | IIIA/I | 2 / 1 | 2 | CT—ETT | 10 | 15 | Scar | UR |
| d. | F | 76 | IAT | Cholecystectomy | No | RI, SE, ME, PNX | Yes/3 | 3 cm TTMP | IIIA | 3 | 24 | CT—ETT | 10 | 15 | Scar | UR |
| e. | F | 41 | IAT | Mastectomy | Yes | RI, SE, ME, PNX | Yes/3 | Linear tear TTMP | II | 2.5 | 12 | CT—ETT | 8 | 15 | Scar | UR |
| f. | M | 19 | SW | N/A | N/A | RI, SE, ME, PNX | No | Circular lesion CTMP | II | 1 | 1 | CT—ETT | 7 | 11 | Scar | UR |
| g. | F | 36 | IAT | Mammoplasty | No | RI | No | Linear tear CTMP | I | 2 | 24 | CT—SB | N/A | 15 | N/A | UR |
| h. | F | 52 | IAT | Cardiac surgery | Yes | RI, SE, ME, PNX | Yes/2 | Linear tear TTMP | IIIA | 2.5 | 8 | CT—ETT | 10 | 16 | Scar | UR |
| i. | F | 72 | IAT | Pneumonia | No | RI, SE, ME | No | Linear tear TTMP | II | 3 | 48 | CT—ETT | 7 | 16 | Scar | UR |
| j. | F | 48 | IAT | Thyroidectomy | Yes | RI | Yes/3 | Linear tear CTMP | I | 2 | 18 | CT—ETT | 7 | 10 | Scar | UR |
| k. | F | 60 | IAT | VC polypectomy | Yes | SE, ME | No | Linear tear CTMP | IIIA | 4.5 | 24 | CT—SB | N/A | 18 | N/A | UR |
F: female; M: male; IAT: iatrogenic injury; SW: stab-wound injury; VC: vocal cord; RI: respiratory impairment; EM: emergency intubation; SE: subcutaneous emphysema; ME: mediastinal emphysema; PNX: pneumothorax; HT: hemothorax; CTMP: cervical trachea membranous pars; CTCP: cervical trachea cartilaginous pars; TTMP: thoracic tracheal membranous pars; RB: right bronchus; CT: conservative treatment; MV: mechanical ventilation; SB: spontaneous breathing; UR: uneventful recovery.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Cherchi, R.; Sarais, S.; Pinna-Susnik, M.; Ferrari, P.A. Conservative Treatment in Tracheobronchial Injuries—An Institutional Report. Surgeries 2021, 2, 237-243. https://0-doi-org.brum.beds.ac.uk/10.3390/surgeries2030024
AMA Style
Cherchi R, Sarais S, Pinna-Susnik M, Ferrari PA. Conservative Treatment in Tracheobronchial Injuries—An Institutional Report. Surgeries. 2021; 2(3):237-243. https://0-doi-org.brum.beds.ac.uk/10.3390/surgeries2030024
Chicago/Turabian StyleCherchi, Roberto, Sabrina Sarais, Matteo Pinna-Susnik, and Paolo Albino Ferrari. 2021. "Conservative Treatment in Tracheobronchial Injuries—An Institutional Report" Surgeries 2, no. 3: 237-243. https://0-doi-org.brum.beds.ac.uk/10.3390/surgeries2030024