Evaluation of the Cortical Deformation Induced by Distal Cantilevers Supported by Extra-Short Implants: A Finite Elements Analysis Study

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
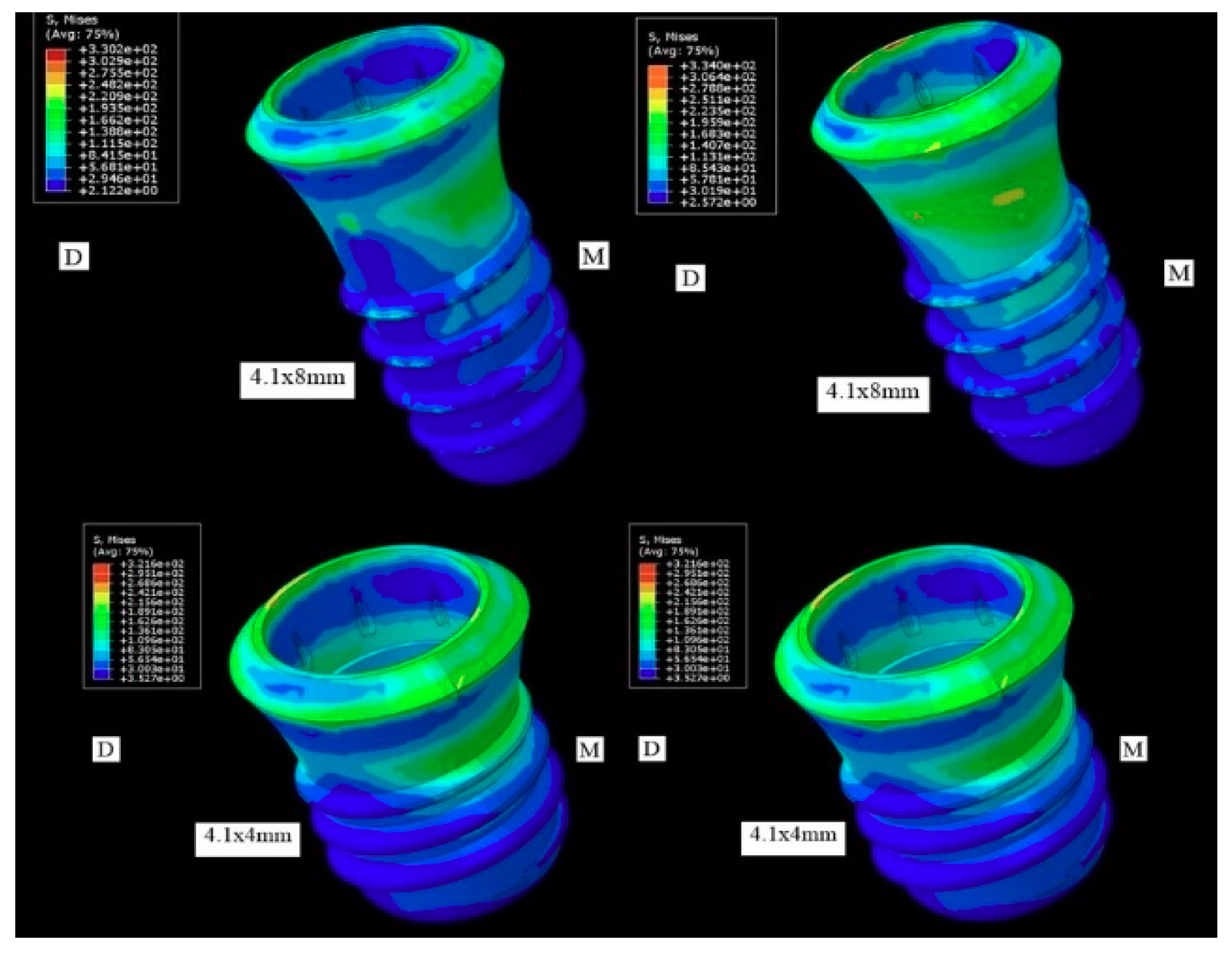
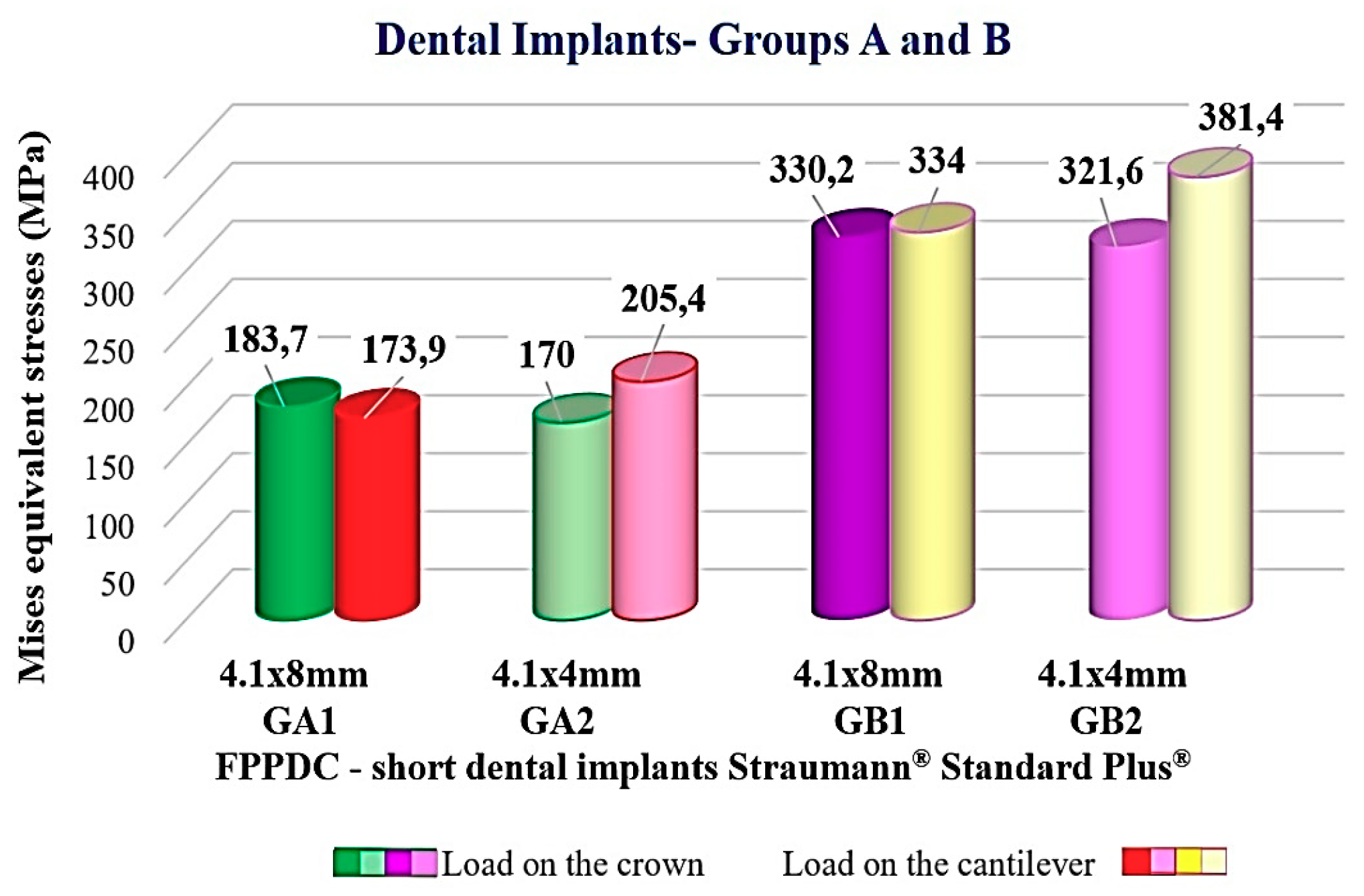
3.1. Distribution of the Tensions in the Implant
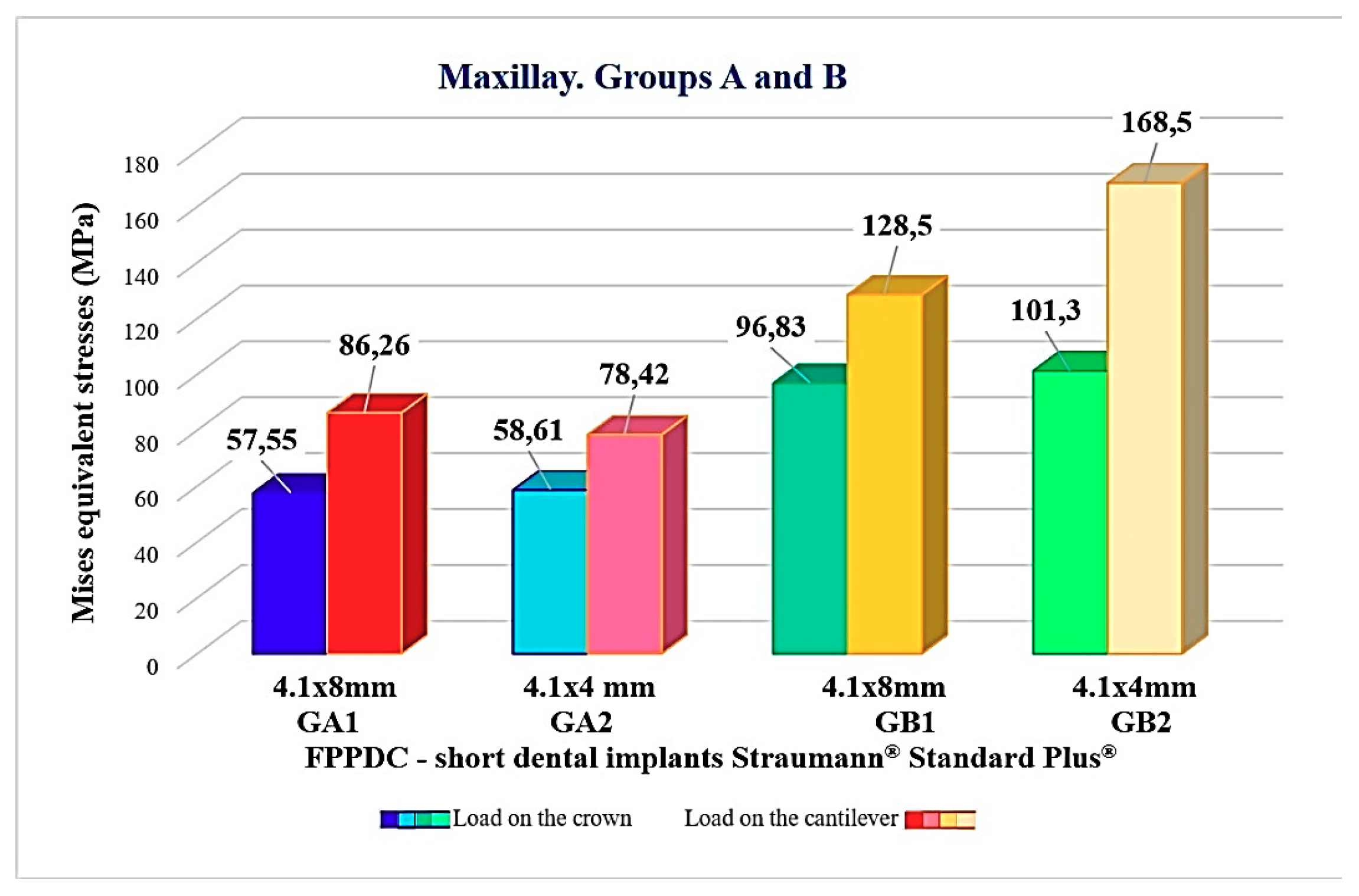
3.2. Distribution of the Tensions in the Solid Model
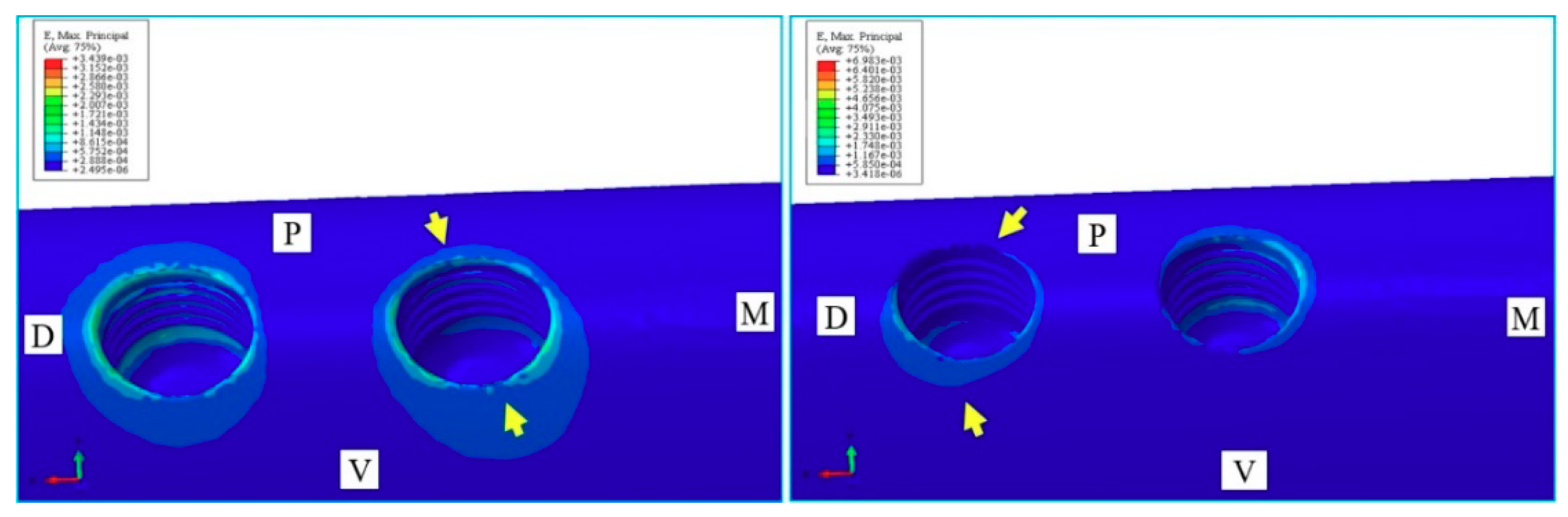
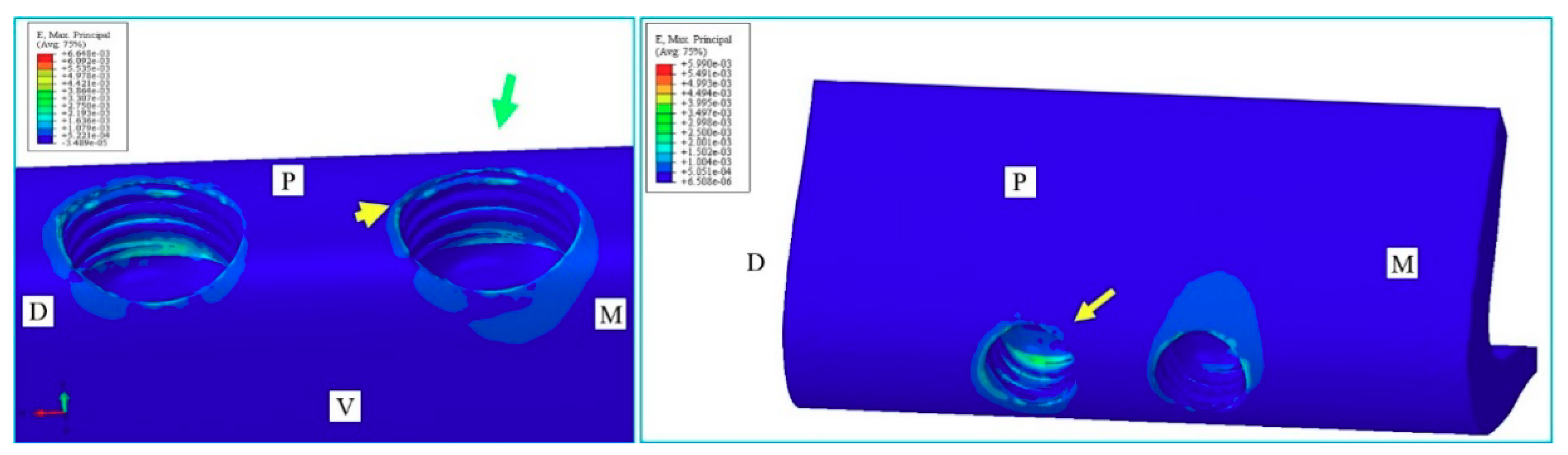
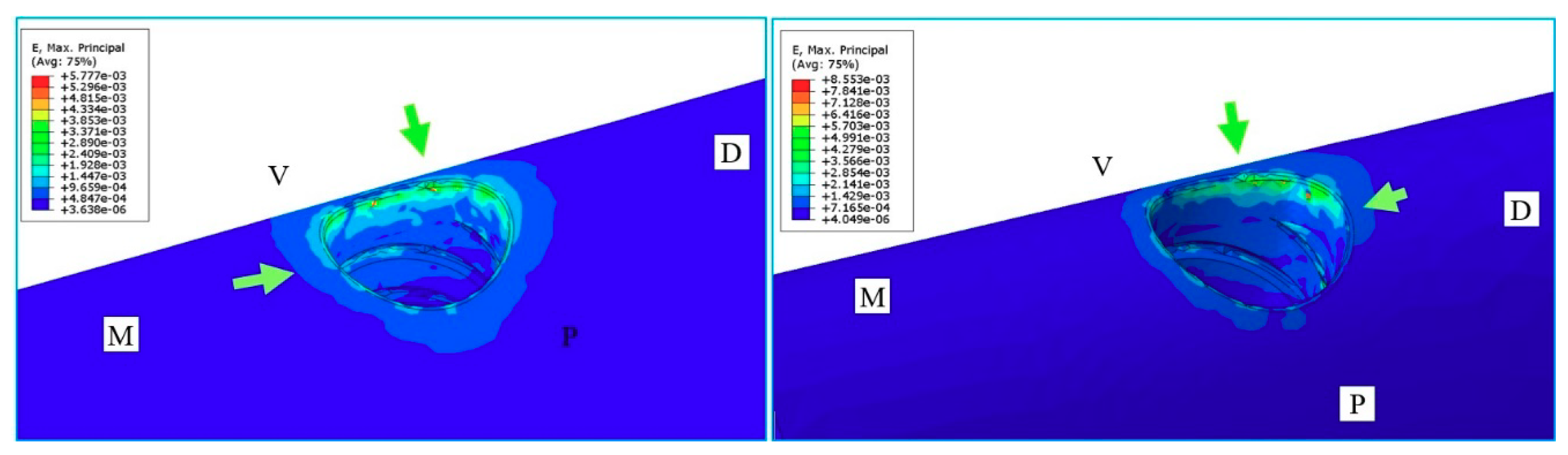
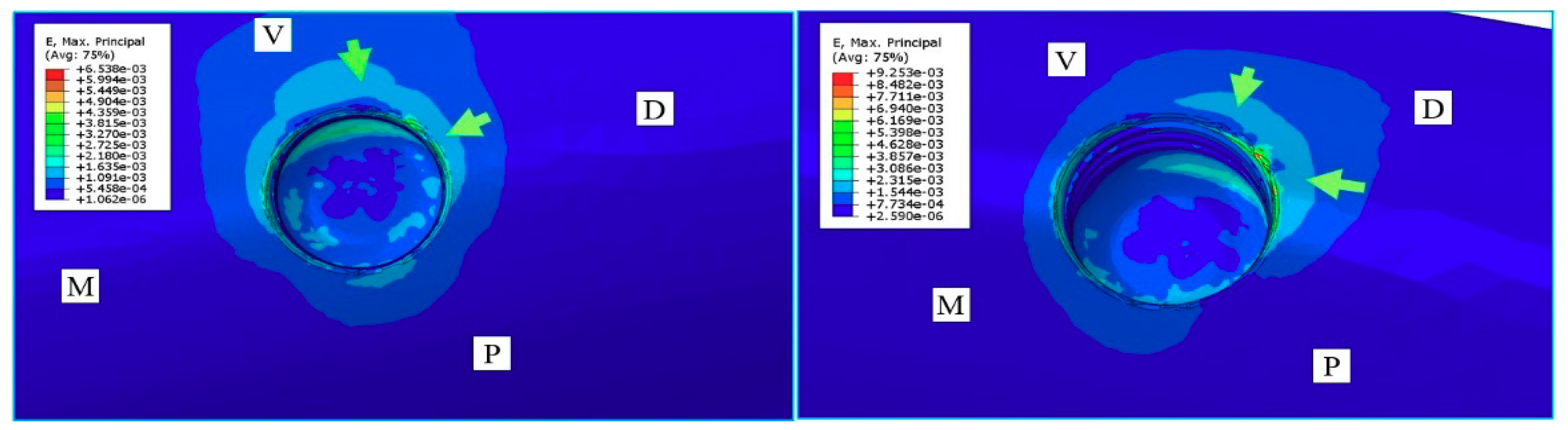
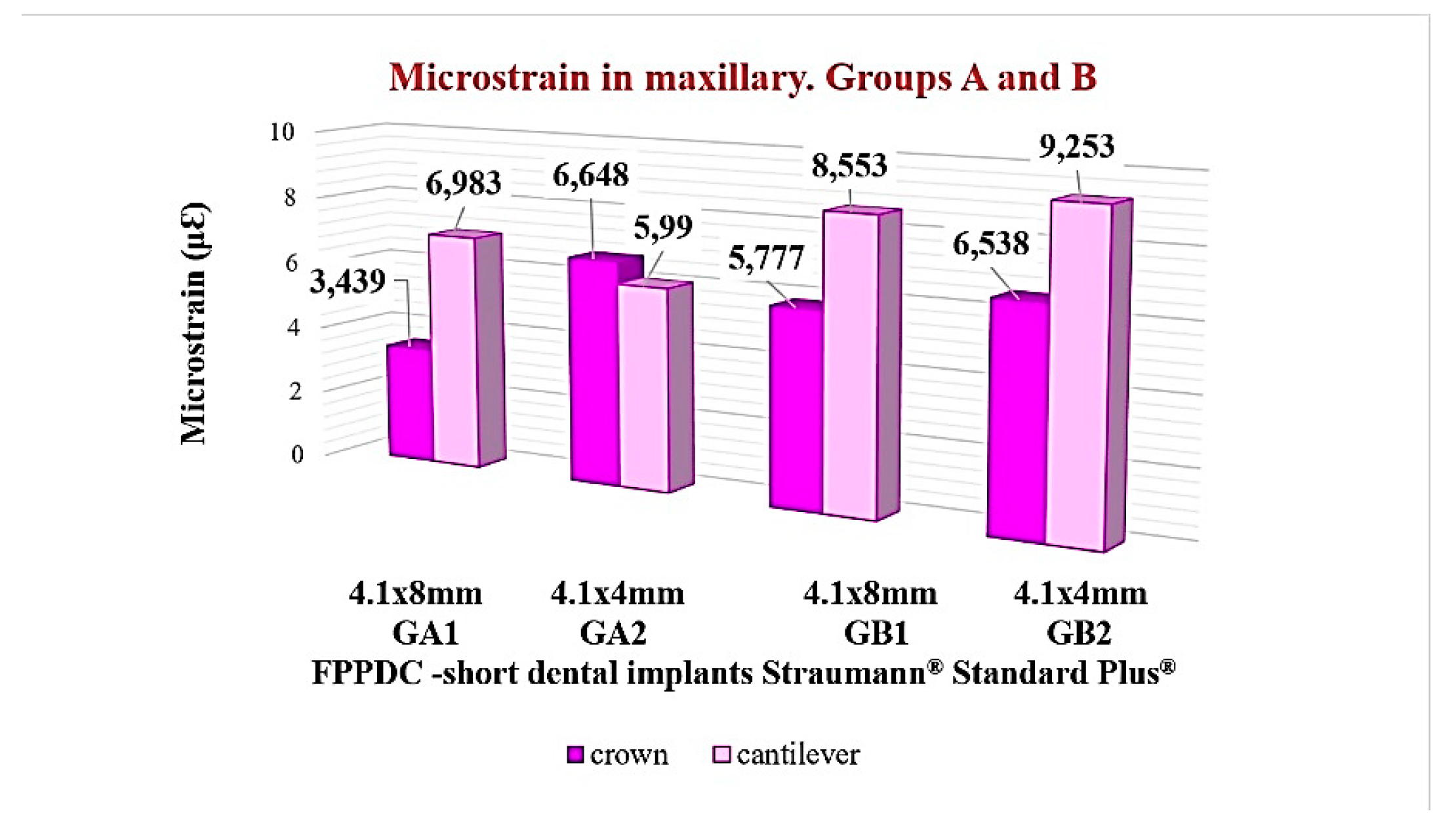
3.3. Bone Behavior
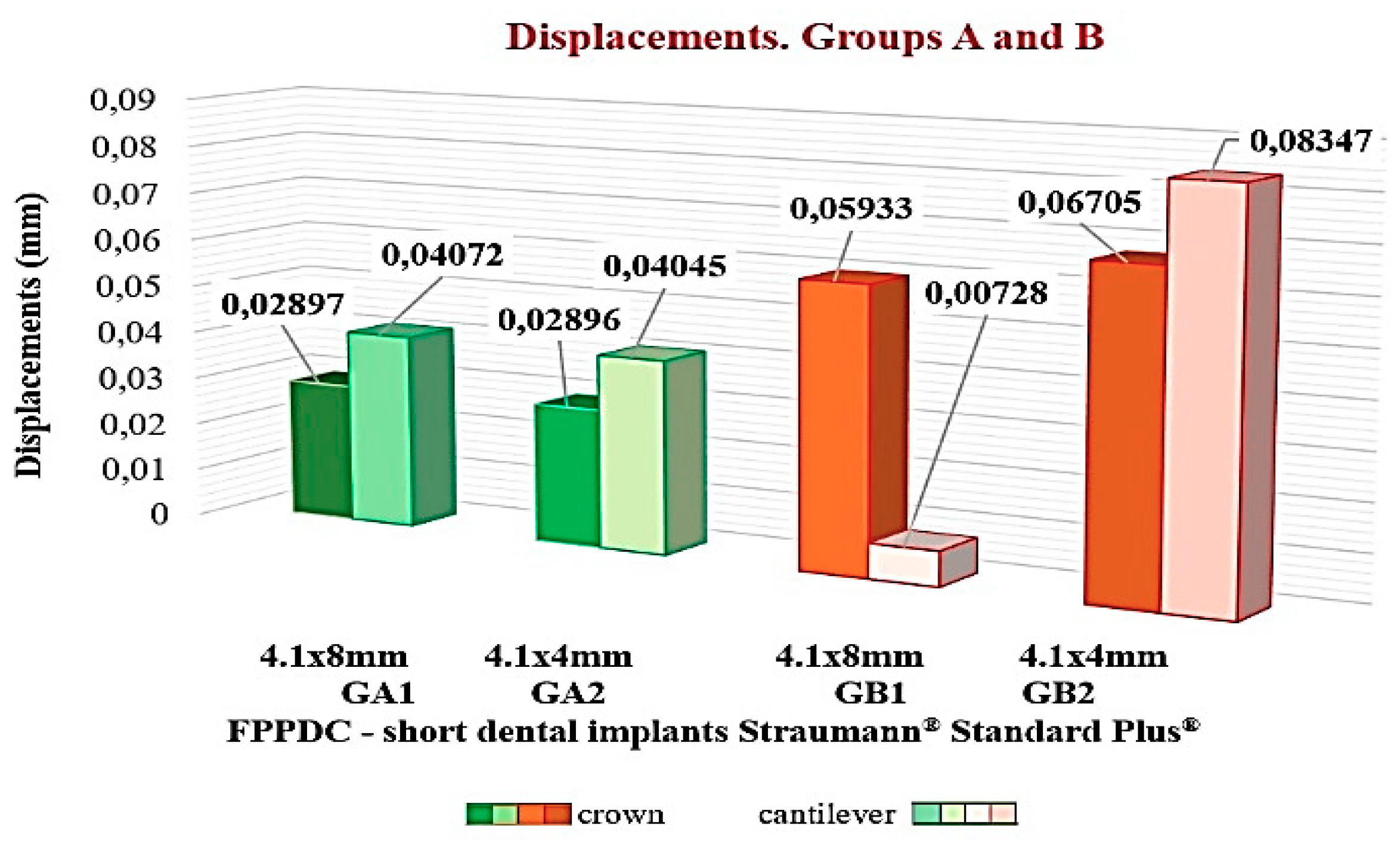
3.4. Prosthesis Behavior
4. Discussion
5. Conclusions
- -
- PPFIVD on two extra-short dental implants could be used as a viable option;
- -
- The tensions are distributed in the cervical third of the implants and to the implant/abutment interface in the form of micro deformations;
- -
- PPFIVD over single extra short implants of 4.1 × 4 mm possess a high risk or mechanical failure; and
- -
- The forces generated during the functional load in the posterior area of the maxilla would affect the prosthetic restoration with distal cantilever and would affect the peri-implant bone that surrounds the extra-short dental implants.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brånemark, P.I. Osseointegration and its experimental background. J. Prosthet. Dent. 1983, 50, 399–410. [Google Scholar] [CrossRef]
- Cervino, G.; Romeo, U.; Lauritano, F.; Bramanti, E.; Fiorillo, L.; D’Amico, C.; Milone, D.; Laino, L.; Campolongo, F.; Rapisarda, S.; et al. Fem and Von Mises Analysis of OSSTEM® Dental Implant Structural Components: Evaluation of Different Direction Dynamic Loads. Open Dent. J. 2018, 12, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Moraschini, V.; Poubel, L.; Ferreira, V.; Barboza Edos, S. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez, J.C.; Tahhan, M.J.; Zamar, J.A. Performance of Double Acid-Etched Surface External Hex Titanium Implants in relation to One-and Two-Stage Surgical Procedures. J. Periodontol. 2003, 74, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.H.; Hyde, B.; Hurst, M.; Harris, B.T.; Lin, W.S. Polyetherketoneketone (PEKK), a framework material for complete fixed and removable dental prostheses: A clinical report. J. Prosthet. Dent. 2018, 119, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Siddiqui, F. Applications of polyetheretherketone (PEEK) in oral implantology and prosthodontics. J. Prosthodont. Res. 2016, 60, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Thoma, S.D.; Cha, J.K.; Jung, U.W. Treatment concepts for the posterior maxilla and mandible: Short implants vs long implants in augmented bone. J. Periodont. Implant Sci. 2017, 47, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Raviv, E.; Turcotte, A.; Harel Raviv, M. Short dental implants in reduced alveolar bone height. Quintessence Int. 2010, 41, 505–509. [Google Scholar]
- Felice, P.; Checchi, L.; Barausse, C.; Pistilli, R.; Sammartino, G.; Masi, I.; Ippolito, D.R.; Esposito, M. Posterior jaws rehabilitated with partial prostheses supported by 4.0 × 4.0 mm or by longer implants: One-year post-loading results from a multicenter randomized controlled trial. Eur. J. Oral Implantol. 2016, 9, 35–45. [Google Scholar]
- Blanes, R.J.; Bernard, J.P.; Blanes, Z.M.; Belser, U.C. A 10-year prospective study of ITI dental implants placed in the posterior region. II: Influence of the crown-to-implant ratio and different prosthetic treatment modalities on crestal bone loss. Clin. Oral Implants Res. 2007, 18, 707–714. [Google Scholar] [CrossRef]
- Urdaneta, R.A.; Rodriguez, S.; McNeil, D.C.; Weed, M.; Chuang, S.K. The effect of increased Crown-to-Implant Ratio on Single Tooth Locking Taper Implants. Int. J. Oral Maxillofac. Implants 2010, 25, 709–743. [Google Scholar]
- Zurdo, J.; Romao, C.; Wennstrom, J.L. Survival and complication rates of implant-supported fixed partial dentures with cantilevers: A systematic review. Clin. Oral Implants Res. 2009, 20, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Brägger, U. Mechanical and technical risks in implant therapy. Int. J. Oral Maxillofac. Implants 2009, 24, 69–85. [Google Scholar] [PubMed]
- Wolff, J.; Narra, N.; Antalainen, A.K.; Valášek, J.; Kaiser, J.; Sándor, G.K.; Marcián, P. Finite element analysis of bone loss around failing implants. Mater. Des. 2014, 61, 177–184. [Google Scholar] [CrossRef]
- Cicciù, M.; Cervino, G.; Milone, D.; Risitano, G. FEM Investigation of the Stress Distribution over Mandibular Bone Due to Screwed Overdenture Positioned on Dental Implants. Materials 2018, 11, 1512. [Google Scholar]
- Lauritano, F.; Runci, M.; Cervino, G.; Fiorillo, L.; Bramanti, E.; Cicciù, M. Three-dimensional evaluation of different prosthesis retention systems using finite element analysis and the Von Mises stress test. Minerva Stomatol. 2016, 65, 353–367. [Google Scholar] [PubMed]
- Sahin, S.; Cehreli, M.C.; Yalcin, E. The influence of functional forces on the biomechanics of implant-supported prosthesis—A review. J. Dent. 2002, 30, 271–282. [Google Scholar] [CrossRef]
- Mellal, A.; Wiskott, H.W.; Botsis, J.; Scherer, S.S.; Belser, U.C. Stimulating effect of implant loading on the surrounding bone. Comparison of three numerical models and validation by in vivo data. Clin. Oral Implants Res. 2004, 15, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Geng, J.P.; Tan, K.B.C.; Liu, G.R. Application of finite element analysis in implant dentistry: A review of the literature. J. Prosthet. Dent. 2001, 85, 585–598. [Google Scholar] [CrossRef]
- Sohn, B.S.; Heo, S.J.; Koak, J.Y.; Kim, S.K.; Lee, S.Y. Strain of implants depending on occlusion types in mandibular implant-supported fixed prostheses. J. Adv. Prosthodont. 2011, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Fernández Bodereau, E., Jr.; Fernández Bodereaum, E. Prótesis a Puente. Selección y valoración de places. In Prótesis Fija e Implantes. Práctica Clínica; Ed Avances Médico-Dentales SL: Madrid, Spain, 1996; pp. 295–320. [Google Scholar]
- Fazi, G.; Tellini, S.; Vangi, D.; Branchi, R. Three-dimensional finite element analysis of different implant configuration for mandibular fixed prosthesis. Int. J. Oral Maxillofac. Implants 2011, 26, 752–759. [Google Scholar] [PubMed]
- Turner, M.J. Stiffness and Deflection Analysis of Complex Structures. J. Aeronaut. Sci. 1956, 23, 805–823. [Google Scholar] [CrossRef]
- Okumura, N.; Stegaroiu, R.; Kitamura, E.; Kurokawa, K.; Nomura, S. Influence of maxillary cortical bone thickness, implant design and implant diameter on stress around implants: A three-dimensional finite element analysis. J. Prosthodont. Res. 2010, 54, 133–142. [Google Scholar] [CrossRef] [PubMed]
- De Almeida, E.O.; Rocha, E.P.; Freitas, A.C., Jr.; Freitas, M.M., Jr. Finite Element Stress Analysis of Edentulous Mandibles with Different Bone Types Supporting Multiple-Implant Superstructures. Int. J. Oral Maxillofac. Implants 2010, 25, 1108–1114. [Google Scholar] [PubMed]
- Romeo, E.; Tomasi, C.; Finini, I.; Casentini, P.; Lops, D. Implant-supported fixed cantilever prosthesis in partially edentulous jaws: A cohort prospective study. Clin. Oral Implants Res. 2009, 20, 1278–1285. [Google Scholar] [CrossRef] [PubMed]
- Céa, J. Approximation Variationnelle des Problèmes aux Limites. Ann. Inst. Fourier. 1964, 14, 345–444. [Google Scholar] [CrossRef]
- Sotto Maior, B.S.; Senna, P.M.; da Silva, W.J.; Rocha, E.P.; Del Bel Cury, A.A. Influence of crown-to-implant ratio. Retention system, restorative material, and occlusal loading on stress concentrations in single short implants. Int. J. Oral Maxillofac. Implants 2012, 27, 13–18. [Google Scholar]
- Bolle, C.; Felice, P.; Barausse, C.; Pistilli, V.; Trullenque-Eriksson, A.; Esposito, M. 4 mm long vs longer implants in augmented bone in posterior atrophic jaws: 1-Year post-loading results from a multicentre randomized controlled trial. Eur. J. Oral Implantol. 2018, 11, 31–47. [Google Scholar]
- Toti, P.; Marchionni, S.; Menchini-Fabris, G.B.; Marconcini, S.; Covani, U.; Barone, A. Surgical techniques used in the rehabilitation of partially edentulous patients with atrophic posterior mandible: A systematic review and meta-analysis of randomized controlled clinical trials. J. Craniomaxillofac. Surg. 2017, 45, 1236–1245. [Google Scholar] [CrossRef]
- Tabrizi, R.; Arabion, H.; Aliabadi, E.; Hasanzadeh, F. Does increasing the number of short implants reduce marginal bone loss in the posterior mandible? A prospective study. Br. J. Oral Maxillofac. Surg. 2016, 54, 731–735. [Google Scholar] [CrossRef]
- Gastaldi, G.; Felice, P.; Pistilli, V.; Barausse, C.; Ippolito, D.R.; Esposito, M. Posterior atrophic jaws rehabilitated with prostheses supported by 5 × 5 mm implants with a nanostructured calcium-incorporated titanium surface o by longer implants in augmented bone. 3-Year results from a randomized controlled trial. Eur. J. Oral Implantol. 2018, 11, 49–61. [Google Scholar] [PubMed]
- Chou, H.Y.; Müftü, S.; Bozkava, D. Combined effects of implants insertion depth and alveolar bone quality on peri-implant bone strain induced by a wide-diameter, short implant, and a narrow-diameter, long implant. J. Prosthet. Dent. 2010, 104, 293–300. [Google Scholar] [CrossRef]
- Sahrmann, P.; Schoen, P.; Naenni, N.; Jung, R.; Attin, T.; Schmidlin, P.R. Peri-implant Bone Density around Implants of Different Length: A 3-year Follow-up of Randomized Clinical Trial. J. Clin. Periodontol. 2017, 44, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Peixoto, R.F.; Macedo, A.P.; Martinelli, J.; Faria, A.C.; Tiossi, R.; Ribeiro, R.F.; de Mattos, M.D. A Digital Image Correlation Analysis of Strain Generated by 3-Unit Implant-Supported Fixed Dental Prosthesis: An In Vitro Study. Implant Dent. 2017, 26, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Esfahrood, Z.R.; Ahmadi, L.; Karami, E.; Asghari, S. Short dental implants in the posterior maxilla: A review of the literature. J. Korean Assoc. Oral Maxillofac. Surg. 2017, 43, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Lemos, C.A.; Ferros-Alves, M.L.; Okamoto, R.; Mendonca, M.R.; Pellizzer, E.P. Short dental implants vs standard dental implants placed in the posterior jaw: A systematic review and meta-analysis. J. Dent. 2016, 47, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Block, J.; Matalon, S.; Tanase, G.; Ormianer, Z. Effect of Restorative Configurations and Occlusal Schemes on Strain Levels on Bone Surrounding Implants. Implant Dent. 2017, 26, 574–580. [Google Scholar] [CrossRef]
- De Souza Batista, V.E.; Verri, F.R.; Almeida, D.A.; Santiago Junior, J.F.; Lemos, C.A.; Pellizzer, E.P. Finite element analysis of implant-supported prosthesis with pontic and cantilever in the posterior maxilla. Comput. Methods Biomech. Biomed. Eng. 2017, 20, 663–670. [Google Scholar] [CrossRef]
- Ormianer, Z.; Matalon, S.; Block, J.; Kohen, J. Dental Implant Thread Design and the Consequences on Long-Term Marginal Bone Loss. Implant Dent. 2016, 25, 471–477. [Google Scholar] [CrossRef]
- Villarinho, E.A.; Triches, D.F.; Alonso, F.R.; Mezzomo, L.A.M.; Teixeira, E.R.; Shinkai, R.S.A. Risk factors for single crowns supported by shorts (6-mm) implants in the posterior region: A prospective clinical and radiographic study. Clin. Implant Dent. Relat. Res. 2017, 19, 671–680. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Models | Amount of Elements | Number of Nodes | Types of Elements | Bone Height (mm) | Implants Dimensions (mm) |
|---|---|---|---|---|---|
| Two implants | 321,066 | 65,826 | Tetrahedron | 9 | 4.1 × 8 |
| Two implants | 424,672 | 85,442 | Tetrahedron | 5 | 4.1 × 4 |
| An implant | 199,443 | 40,776 | Tetrahedron | 9 | 4.1 × 8 |
| An implant | 264,076 | 53,261 | Tetrahedron | 5 | 4.1 × 4 |
| Models | Crown (MPa) | Cantilever (MPa) | Load (N) | Implant Dimensions (mm) |
|---|---|---|---|---|
| A Two implants | 183.7 | 173.9 | 100 | 4.1 × 8 |
| 170 | 205.4 | 100 | 4.1 × 4 | |
| B An implant | 330.2 | 334 | 100 | 4.1 × 8 |
| 321.6 | 381.4 | 100 | 4.1 × 4 |
| Models | Crown (MPa) | Cantilever (MPa) | Load (N) | Implant Dimensions (mm) |
|---|---|---|---|---|
| A Two implants | 57.55 | 86.26 | 100 | 4.1 × 8 |
| 58.61 | 78.42 | 100 | 4.1 × 4 | |
| B An implant | 96.83 | 128.5 | 100 | 4.1 × 8 |
| 101.3 | 168.5 | 100 | 4.1 × 4 |
| Models | Crown (Maximum Tensile) με | Cantilever (Maximum Tensile) με | Load (N) | Implants Dimensions (mm) |
|---|---|---|---|---|
| A Two implants | 3.439 | 6.983 | 100 | 4.1 × 8 |
| 6.648 | 5.990 | 100 | 4.1 × 4 | |
| B An implant | 5.777 | 8.553 | 100 | 4.1 × 8 |
| 6.538 | 9.253 | 100 | 4.1 × 4 |
| Models | Displacement Crown (mm) | Displacement Cantilever (mm) | Load (N) | Implant Dimensions (mm) |
|---|---|---|---|---|
| A Two short implants | 0.02897 | 0.04072 | 100 | 4.1 × 8 |
| 0.02896 | 0.04045 | 100 | 4.1 × 4 | |
| B A short implant | 0.05933 | 0.00728 | 100 | 4.1 × 8 |
| 0.06705 | 0.08347 | 100 | 4.1 × 4 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Bodereau, E.; Flores, V.Y.; Delgado-Ruiz, R.A.; Aragoneses, J.M.; Calvo-Guirado, J.L. Evaluation of the Cortical Deformation Induced by Distal Cantilevers Supported by Extra-Short Implants: A Finite Elements Analysis Study. Symmetry 2018, 10, 762. https://0-doi-org.brum.beds.ac.uk/10.3390/sym10120762
Fernández-Bodereau E, Flores VY, Delgado-Ruiz RA, Aragoneses JM, Calvo-Guirado JL. Evaluation of the Cortical Deformation Induced by Distal Cantilevers Supported by Extra-Short Implants: A Finite Elements Analysis Study. Symmetry. 2018; 10(12):762. https://0-doi-org.brum.beds.ac.uk/10.3390/sym10120762
Chicago/Turabian StyleFernández-Bodereau, Enrique, Viviana Yolanda Flores, Rafael Arcesio Delgado-Ruiz, Juan Manuel Aragoneses, and José Luis Calvo-Guirado. 2018. "Evaluation of the Cortical Deformation Induced by Distal Cantilevers Supported by Extra-Short Implants: A Finite Elements Analysis Study" Symmetry 10, no. 12: 762. https://0-doi-org.brum.beds.ac.uk/10.3390/sym10120762