
The Symmetry of the Muscle Tension Signal in the Upper Limbs When Propelling a Wheelchair and Innovative Control Systems for Propulsion System Gear Ratio or Propulsion Torque: A Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
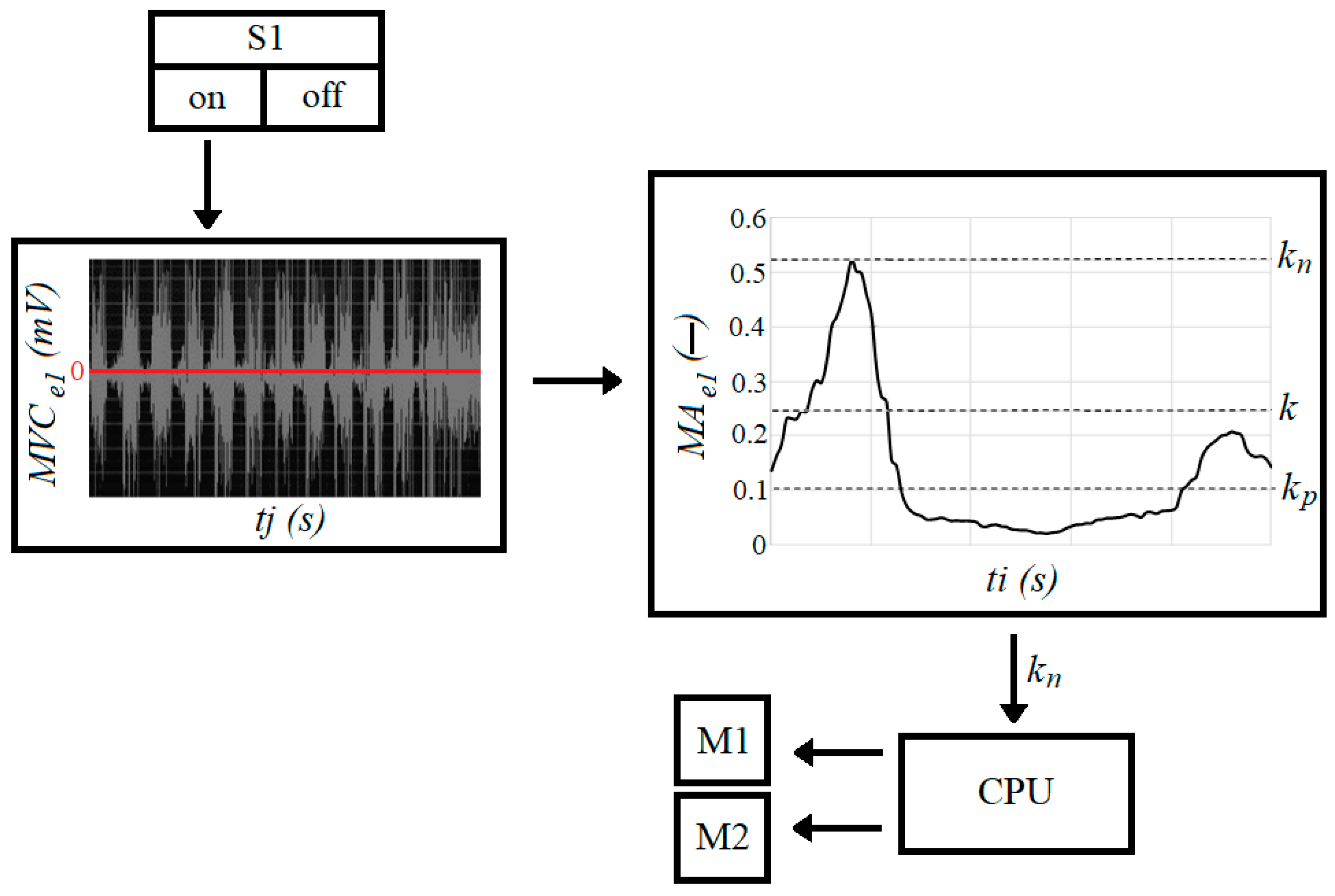
- —muscle activity (expressed in %);
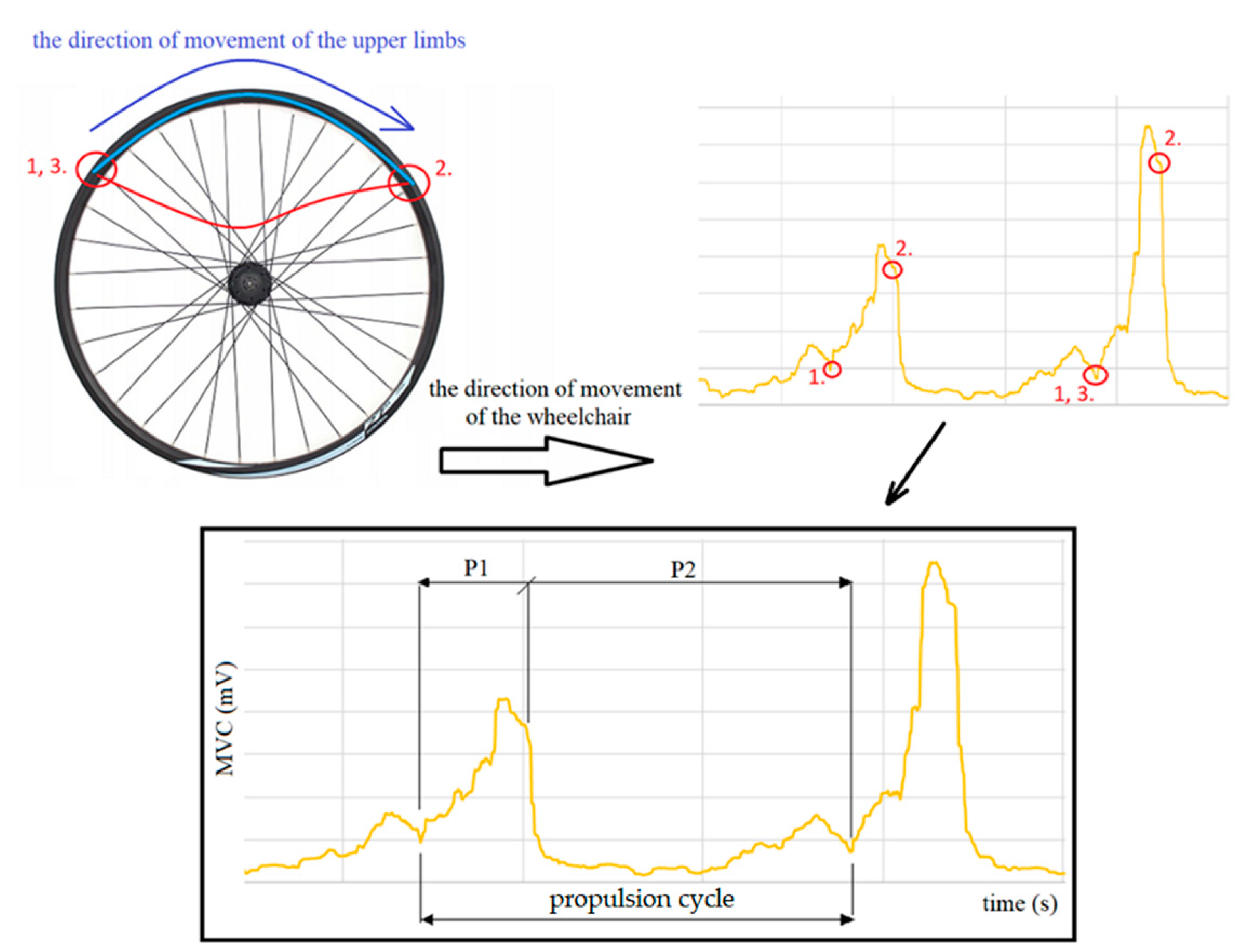
- —maximum voluntary contraction during the propulsion phase (expressed in mV);
- —maximum voluntary contraction during normalization test (expressed in mV).
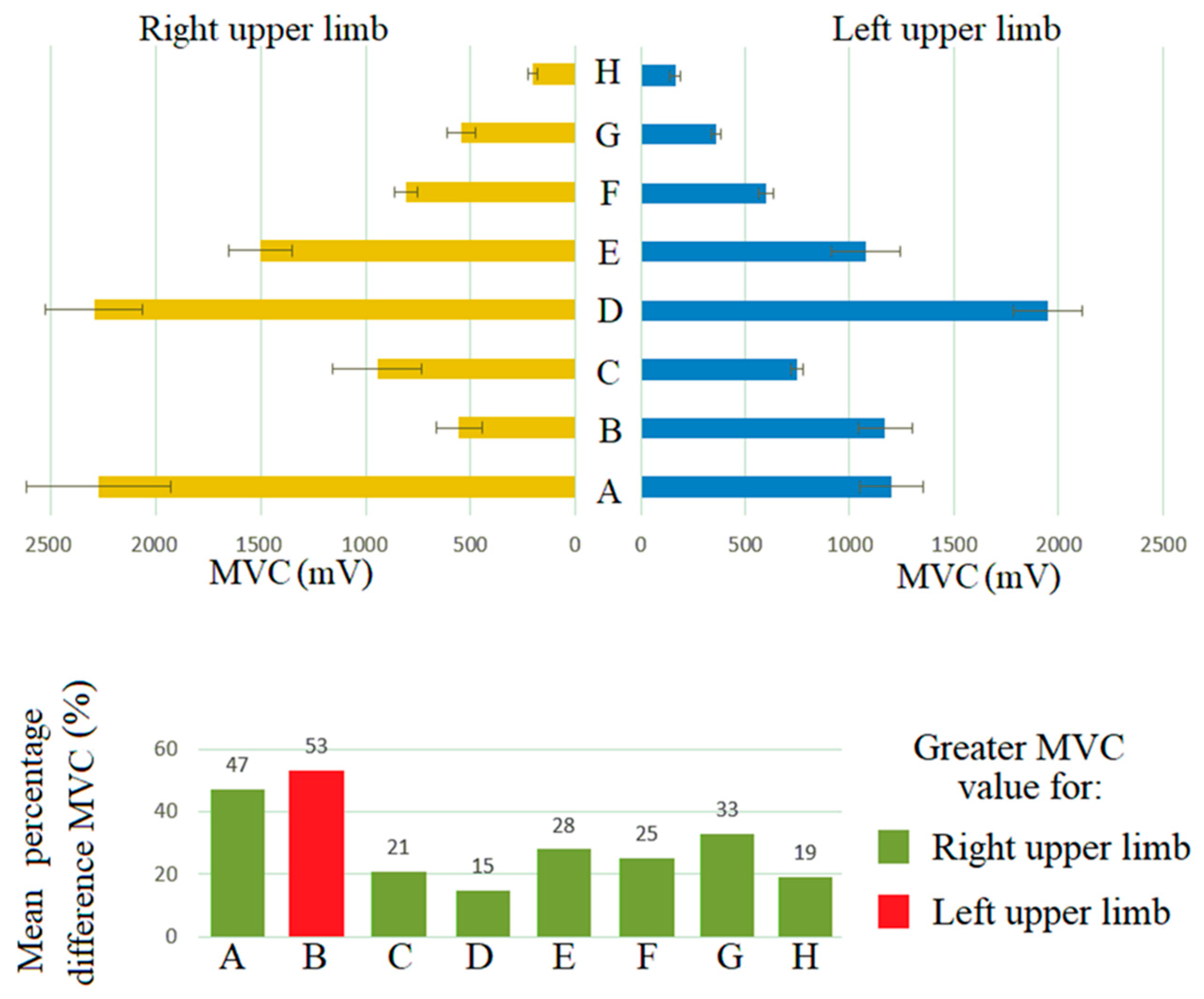
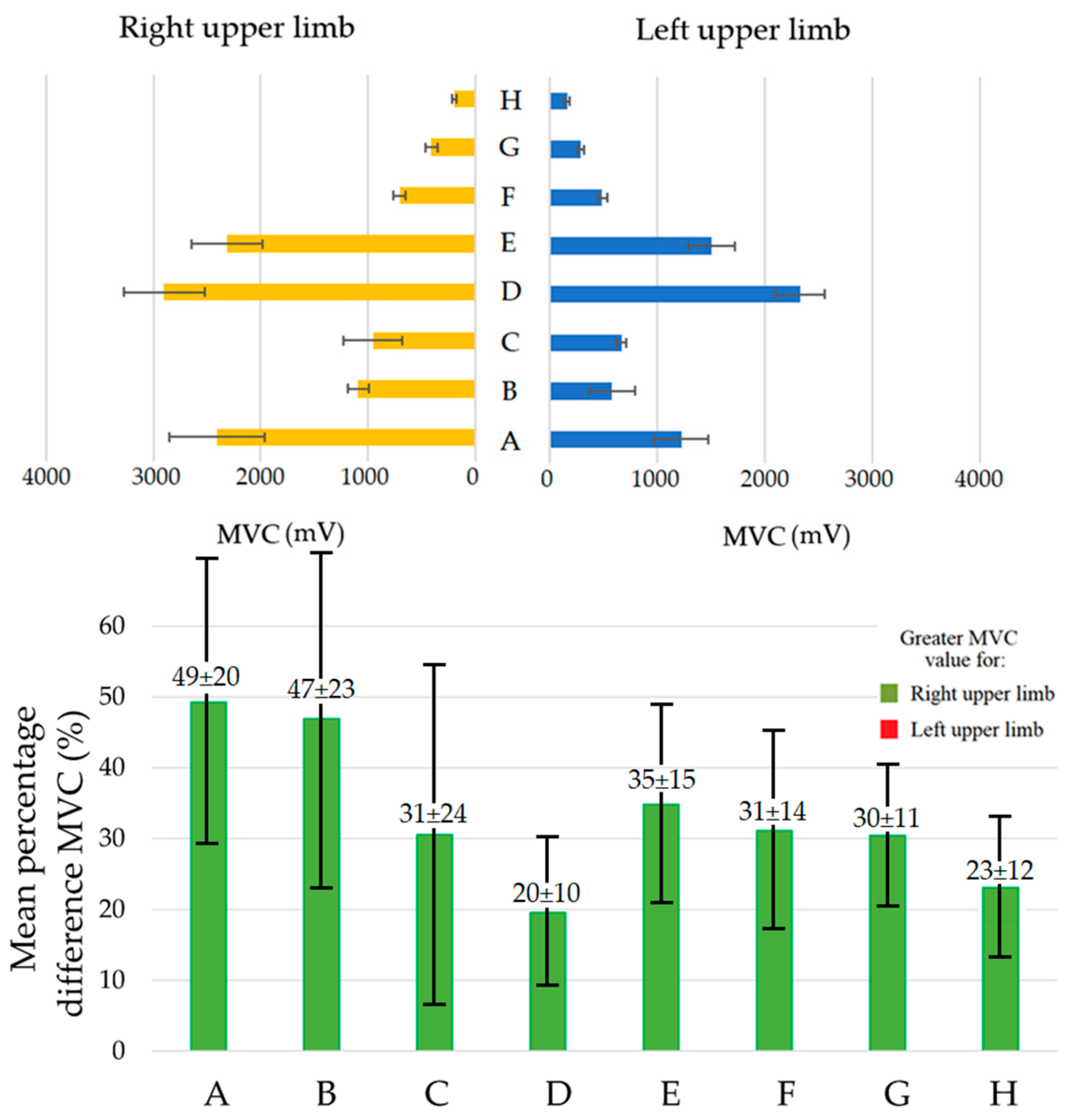
3. Results and Discussion
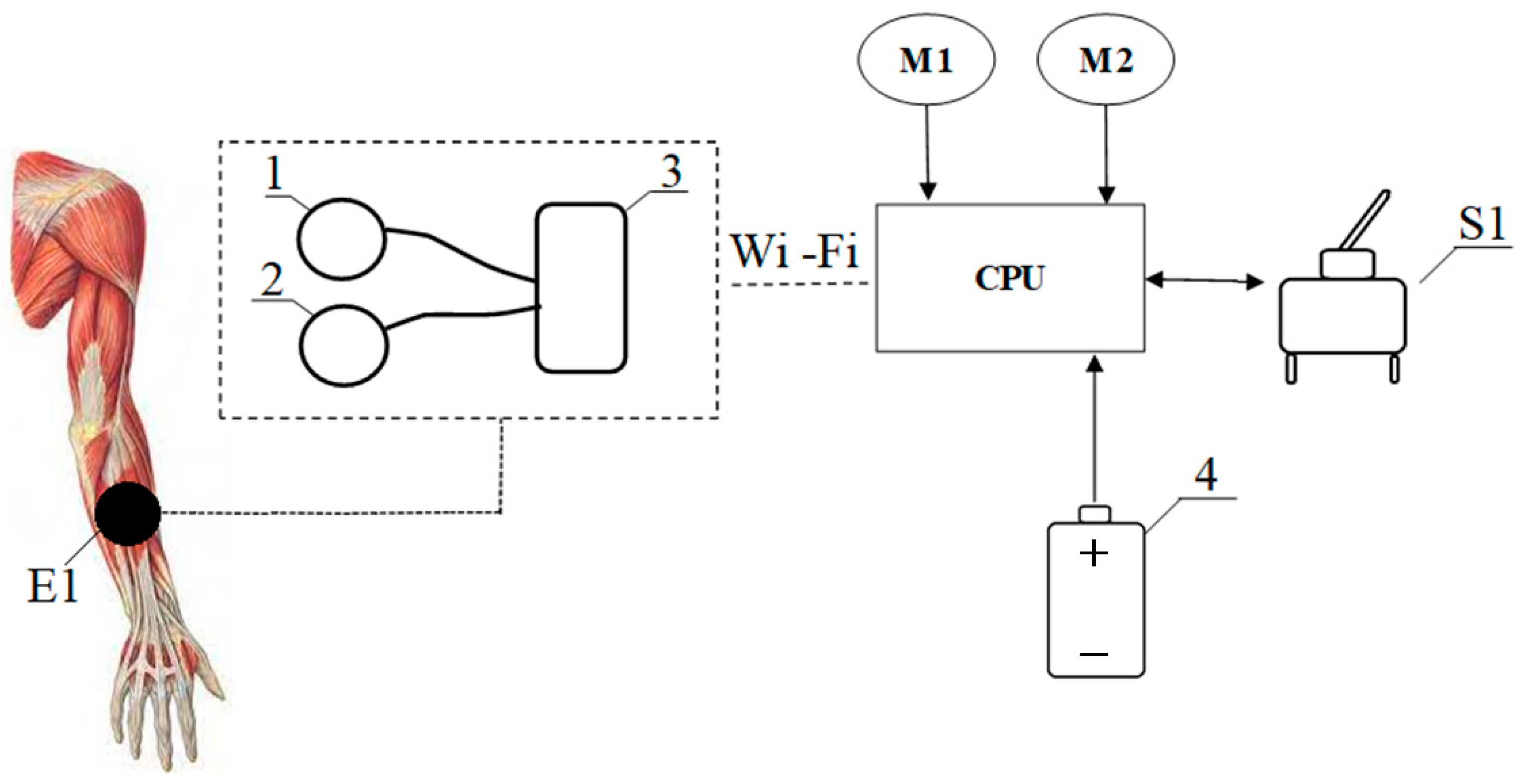
4. The Concept of an Innovative Wheelchair Design and Control Algorithm
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wieczorek, B.; Kukla, M.; Rybarczyk, D.; Warguła, Ł. Evaluation of the biomechanical parameters of human-wheelchair systems during ramp climbing with the use of a manual wheelchair with anti-rollback devices. Appl. Sci. 2020, 10, 8757. [Google Scholar] [CrossRef]
- Kilikevičius, A.; Bačinskas, D.; Selech, J.; Matijošius, J.; Kilikevičienė, K.; Vainorius, D.; Ulbrich, D.; Romek, D. The Influence of Different Loads on the Footbridge Dynamic Parameters. Symmetry 2020, 12, 657. [Google Scholar] [CrossRef]
- Rymaniak, Ł.; Kamińska, M.; Szymlet, N.; Grzeszczyk, R. Analysis of Harmful Exhaust Gas Concentrations in Cloud behind a Vehicle with a Spark Ignition Engine. Energies 2021, 14, 1769. [Google Scholar] [CrossRef]
- Gull, M.A.; Thoegersen, M.; Bengtson, S.H.; Mohammadi, M.; Andreasen Struijk, L.N.S.; Moeslund, T.B.; Bak, T.; Bai, S. A 4-DOF Upper Limb Exoskeleton for Physical Assistance: Design, Modeling, Control and Performance Evaluation. Appl. Sci. 2021, 11, 5865. [Google Scholar] [CrossRef]
- Kukla, M.; Wieczorek, B.; Warguła, Ł.; Górecki, J.; Giedrowicz, M. An Analytical Modelling of Demand for Driving Torque of a Wheelchair with Electromechanical Drive. Energies 2021, 14, 7315. [Google Scholar] [CrossRef]
- Marco-Ahulló, A.; Montesinos-Magraner, L.; Gonzalez, L.-M.; Llorens, R.; Segura-Navarro, X.; García-Massó, X. Validation of Using Smartphone Built-In Accelerometers to Estimate the Active Energy Expenditures of Full-Time Manual Wheelchair Users with Spinal Cord Injury. Sensors 2021, 21, 1498. [Google Scholar] [CrossRef]
- Giménez, C.V.; Krug, S.; Qureshi, F.Z.; O’Nils, M. Evaluation of 2D-/3D-Feet-Detection Methods for Semi-Autonomous Powered Wheelchair Navigation. J. Imaging 2021, 7, 255. [Google Scholar] [CrossRef]
- Dziewiatkowski, M.; Szpica, D.; Borawski, A. Evaluation of impact of combustion engine controller adaptation process on level of exhaust gas emissions in gasoline and compressed natural gas supply process. Eng. Rural Dev. 2020, 19, 541–548. [Google Scholar]
- Nikonova, T.; Zharkevich, O.; Dandybaev, E.; Baimuldin, M.; Daich, L.; Sichkarenko, A.; Kotov, E. Developing a Measuring System for Monitoring the Thickness of the 6 m Wide HDPE/LDPE Polymer Geomembrane with Its Continuous Flow Using Automation Equipment. Appl. Sci. 2021, 11, 10045. [Google Scholar] [CrossRef]
- Gabryelski, J.; Kurczewski, P.; Sydor, M.; Szperling, A.; Torzyński, D.; Zabłocki, M. Development of Transport for Disabled People on the Example of Wheelchair Propulsion with Cam-Thread Drive. Energies 2021, 14, 8137. [Google Scholar] [CrossRef]
- Wieczorek, B.; Kukla, M. Effects of the performance parameters of a wheelchair on the changes in the position of the centre of gravity of the human body in dynamic condition. PLoS ONE 2019, 14, e0226013. [Google Scholar] [CrossRef] [PubMed]
- Lipert, A.; Wróbel, K.; Spychała, M.; Rasmus, P.; Timler, D.; Marczak, M.; Kozłowski, R. The Effectiveness of Active Rehabilitation Camp on Physical Performance of Disabled People Moving in Wheelchairs. Int. J. Environ. Res. Public Health 2021, 18, 7572. [Google Scholar] [CrossRef] [PubMed]
- Sivakanthan, S.; Castagno, J.; Candiotti, J.L.; Zhou, J.; Sundaram, S.A.; Atkins, E.M.; Cooper, R.A. Automated Curb Recognition and Negotiation for Robotic Wheelchairs. Sensors 2021, 21, 7810. [Google Scholar] [CrossRef] [PubMed]
- Maule, L.; Luchetti, A.; Zanetti, M.; Tomasin, P.; Pertile, M.; Tavernini, M.; Guandalini, G.M.A.; De Cecco, M. RoboEye, an Efficient, Reliable and Safe Semi-Autonomous Gaze Driven Wheelchair for Domestic Use. Technologies 2021, 9, 16. [Google Scholar] [CrossRef]
- Wieczorek, B.; Kukla, M.; Warguła, Ł. The Symmetric Nature of the Position Distribution of the Human Body Center of Gravity during Propelling Manual Wheelchairs with Innovative Propulsion Systems. Symmetry 2021, 13, 154. [Google Scholar] [CrossRef]
- Sprigle, S.; Huang, M.; Misch, J. Measurement of rolling resistance and scrub torque of manual wheelchair drive wheels and casters. Assist. Technol. 2019, 34, 91–103. [Google Scholar] [CrossRef]
- Ott, J.; Wilson-Jene, H.; Koontz, A.; Pearlman, J. Evaluation of rolling resistance in manual wheelchair wheels and casters using drum-based testing. Disabil. Rehabil. Assist. Technol. 2020, 1–12. [Google Scholar] [CrossRef]
- Rietveld, T.; Mason, B.S.; Goosey-Tolfrey, V.L.; van der Woude, L.H.; de Groot, S.; Vegter, R.J. Inertial measurement units to estimate drag forces and power output during standardised wheelchair tennis coast-down and sprint tests. Sports Biomech. 2021, 1–19. [Google Scholar] [CrossRef]
- Lemaire, E.D.; O’Neill, P.A.; Desrosiers, M.M.; Robertson, D.G. Wheelchair ramp navigation in snow and ice-grit conditions. Arch. Phys. Med. Rehabil. 2010, 91, 1516–1523. [Google Scholar] [CrossRef]
- Wieczorek, B.; Kukla, M.; Warguła, Ł.; Rybarczyk, D.; Giedrowicz, M.; Górecki, J. The Impact of the Human Body Position Changes During Wheelchair Propelling on Motion Resistance Force: A Preliminary Study. J. Biomech. Eng. 2021, 143, 081008. [Google Scholar] [CrossRef]
- Wieczorek, B.; Kukla, M. Biomechanical Relationships Between Manual Wheelchair Steering and the Position of the Human Body’s Center of Gravity. J. Biomech. Eng. 2020, 142, 081006. [Google Scholar] [CrossRef]
- Zhou, H.; Hou, K.-M.; Zuo, D.; Li, J. Intelligent Urban Public Transportation for Accessibility Dedicated to People with Disabilities. Sensors 2012, 12, 10678–10692. [Google Scholar] [CrossRef] [PubMed]
- Morales, Y.; Watanabe, A.; Ferreri, F.; Even, J.; Shinozawa, K.; Hagita, N. Passenger discomfort map for autonomous navigation in a robotic wheelchair. Robot. Auton. Syst. 2018, 103, 13–26. [Google Scholar] [CrossRef]
- Rousseau-Harrison, K.; Rochette, A.; Routhier, F.; Dessureault, D.; Thibault, F.; Côté, O. Impact of wheelchair acquisition on social participation. Disabil. Rehabil. Assist. Technol. 2009, 4, 344–352. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Yap, R.C.Y. Social Impact Investing for Marginalized Communities in Hong Kong: Cases and Issues. Sustainability 2019, 11, 2831. [Google Scholar] [CrossRef] [Green Version]
- Van der Woude, L.H.; De Groot, S.; Janssen, T.W. Manual wheelchairs: Research and innovation in rehabilitation, sports, daily life and health. Med. Eng. Phys. 2006, 28, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Wieczorek, B.; Warguła, Ł.; Rybarczyk, D. Impact of a Hybrid Assisted Wheelchair Propulsion System on Motion Kinematics during Climbing up a Slope. Appl. Sci. 2020, 10, 1025. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.; Hori, Y. Disturbance attenuation control for power-assist wheelchair operation on slopes. IEEE Trans. Control Syst. Technol. 2013, 22, 828–837. [Google Scholar]
- Oh, S.; Kong, K.; Hori, Y. Operation state observation and condition recognition for the control of power-assisted wheelchair. Mechatronics 2014, 24, 1101–1111. [Google Scholar] [CrossRef]
- Jones, B.; Menaro, A.; Sparkman, J. Electromyographic Controlled Vehicles and Chairs. US Patent 10426370B2, 1 November 2019. [Google Scholar]
- Kim, D.; Lee, H. Powered Wheelchair Interface Method for the Spinal Cord Injury Person. Korea Patent 100488684B1, 11 May 2005. [Google Scholar]
- Callejas-Cuervo, M.; González-Cely, A.X.; Bastos-Filho, T. Control systems and electronic instrumentation applied to autonomy in wheelchair mobility: The state of the art. Sensors 2020, 20, 6326. [Google Scholar] [CrossRef] [PubMed]
- Jang, G.; Kim, J.; Lee, S.; Choi, Y. EMG-Based Continuous Control Scheme with Simple Classifier for Electric-Powered Wheelchair. IEEE Trans. Ind. Electron. 2016, 63, 3695–3705. [Google Scholar] [CrossRef]
- Jang, G.; Choi, Y. EMG-based continuous control method for electric wheelchair. In Proceedings of the International Conference on Intelligence Robots and Systems (IEEE/RSJ 2014), Chicago, IL, USA, 14–18 September 2014; pp. 3549–3554. [Google Scholar]
- Küçükyildiz, G.; Ocak, H.; Şayli, Ö.; Karakaya, S. Real time control of a wheelchair based on EMG and Kinect for the disabled people. In Proceedings of the Medical Technologies National Conference (TIPTEKNO 2015), Bodrum, Turkey, 15–18 October 2015; pp. 1–4. [Google Scholar]
- Kaur, A. Wheelchair control for disabled patients using EMG/EOG based human machine interface: A review. J. Med. Eng. Technol. 2021, 45, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.; Norfleet, D.A. “Wheelchair Fatigue Reducer”. Chancellor’s Honors Program Projects. 2016. Available online: https://trace.tennessee.edu/utk_chanhonoproj/1952 (accessed on 13 February 2022).
- Zukowski, L.A.; Hass, C.J.; Shechtman, O.; Christou, E.A.; Tillman, M.D. The effect of wheelchair propulsion style on changes in time spent in extreme wrist orientations after a bout of fatiguing propulsion. Ergonomics 2017, 60, 1425–1434. [Google Scholar] [CrossRef]
- Guo, L.Y.; Su, F.C.; Wu, H.W.; An, K.N. Mechanical energy and power flow of the upper extremity in manual wheelchair propulsion. Clin. Biomech. 2003, 18, 106–114. [Google Scholar] [CrossRef]
- Wang, Y.; Choi, J.; Loh, P.Y.; Muraki, S. A comparison of motor control characteristics of the dominant and non-dominant arms in response to assistive force during unilateral task. Isokinet. Exerc. Sci. 2019, 27, 313–324. [Google Scholar] [CrossRef]
- Priya, S.; Rai, M.; Joseph, D.K. Comparison between Handgrip Strength Measurement of Dominant Hand and Non Dominant Hand in Basketball Players. Indian J. Physiother. Occup. Ther. 2018, 12, 126–130. [Google Scholar] [CrossRef]
- Yuine, H.; Yoshii, Y.; Iwai, K.; Ishii, T.; Shiraishi, H. Assessment of distal radioulnar joint stabilityin healthy subjects: Changes with dominant hand, sex, andage. J. Orthop. Res. 2021, 39, 2028–2035. [Google Scholar] [CrossRef]
- Madansingh, S.I.; Fortune, E.; Morrow, M.M.; Zhao, K.D.; Cloud-Biebl, B.A. Comparing supraspinatus to acromion proximity and kinematics of the shoulder and thorax between manual wheelchair propulsion styles: A pilot study. Clin. Biomech. 2020, 74, 42–50. [Google Scholar] [CrossRef]
- Briley, S.J.; Vegter, R.J.; Goosey-Tolfrey, V.L.; Mason, B.S. Scapular kinematic variability during wheelchair propulsion is associated with shoulder pain in wheelchair users. J. Biomech. 2020, 113, 110099. [Google Scholar] [CrossRef]
- Sasaki, M.; Ota, Y.; Hase, K.; Stefanov, D.; Yamaguchi, M. Simulation model of a lever-propelled wheelchair. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 6923–6926. [Google Scholar]
- Yu, C.H.; Tseng, C.Y. Research on gear-change control technology for the clutchless automatic–manual transmission of an electric vehicle. Proc. Inst. Mech. Eng. Part D J. Automob. Eng. 2013, 227, 1446–1458. [Google Scholar] [CrossRef]
- Hung, N.B.; Sung, J.; Lim, O. A simulation and experimental study of operating performance of an electric bicycle integrated with a semi-automatic transmission. Appl. Energy 2018, 221, 319–333. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Gender | Height | Weight | Age | Dominant Hand | Push Force | Experience | Region of Spinal Cord Injury |
|---|---|---|---|---|---|---|---|---|
| cm | kg | Years | - | N | - | - | ||
| P1 | male | 183 | 90 | 32 | right | 364 | ■■■■□ | lumbar |
| P2 | male | 171 | 67 | 25 | right | 282 | ■■■■■ | sacral |
| P3 | male | 169 | 72 | 30 | right | 263 | ■■■□□ | sacral |
| P4 | male | 185 | 72 | 36 | right | 321 | ■■□□□ | lumbar |
| P5 | male | 179 | 88 | 32 | right | 321 | ■■■■□ | lumbar |
| P6 | male | 188 | 74 | 36 | right | 291 | ■□□□□ | lumbar |
| P7 | male | 173 | 87 | 31 | right | 296 | ■■□□□ | sacral |
| P8 | male | 174 | 81 | 35 | right | 247 | ■■■■□ | sacral |
| P9 | male | 175 | 110 | 31 | right | 333 | ■■■■□ | lumbar |
| P10 | male | 183 | 100 | 32 | right | 329 | ■■■□□ | sacral |
| Muscle | Limb | Measurement Test | Mean MVC | |||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |||
| mV | mV | |||||||
| Biceps muscle (A) | R | 1883.0 | 2061.0 | 2039.0 | 2395.0 | 2537.0 | 2721.0 | 2272.67 ± 343.95 |
| L | 1417.0 | 1356.0 | 1116.0 | 1096.0 | 1101.0 | 1111.0 | 1199.5 ± 153.53 | |
| Triceps muscle (B) | R | 687.9 | 589.7 | 384.7 | 522.5 | 625.0 | 513.6 | 553.9 ± 110.6 |
| L | 1086.0 | 1069.0 | 1100.0 | 1110.0 | 1344.0 | 1321.0 | 1171.67 ± 131.76 | |
| Deltoid middle head muscle (C) | R | 1202.0 | 1132.0 | 890.2 | 982.8 | 720.0 | 724.5 | 941.92 ± 212.31 |
| L | 744.5 | 780.5 | 758.7 | 744.4 | 768.3 | 697.3 | 748.95 ± 30.32 | |
| Long extensor muscle of the wrist (D) | R | 2128.0 | 2137.0 | 2115.0 | 2292.0 | 2676.0 | 2423.0 | 2295.17 ± 233.16 |
| L | 1769.0 | 1837.0 | 1942.0 | 1881.0 | 2110.0 | 2162.0 | 1950.17 ± 163.19 | |
| Deltoid front head muscle (E) | R | 1369.0 | 1530.0 | 1376.0 | 1567.0 | 1743.0 | 1426.0 | 1501.83 ± 150.21 |
| L | 1294.0 | 1119.0 | 915.1 | 896.8 | 1169.0 | 1078.0 | 1078.65 ± 163.19 | |
| Deltoid back head muscle (E) | R | 865.3 | 787.6 | 789.3 | 789.7 | 868.0 | 731.2 | 805.18 ± 55.2 |
| L | 586.3 | 565.7 | 651.3 | 619.1 | 574.2 | 606.2 | 600.47 ± 33.40 | |
| Trapezius muscle (G) | R | 634.9 | 553.1 | 569.9 | 547.4 | 450.3 | 489.1 | 540.78 ± 67.62 |
| L | 341.5 | 341.4 | 385.2 | 367.1 | 343.1 | 387.9 | 361.03 ± 23.14 | |
| Subcapsular muscle (H) | R | 190.2 | 188.7 | 194.7 | 187.2 | 238.5 | 225.6 | 204.15 ± 23.23 |
| L | 157.5 | 147.1 | 145.9 | 147.7 | 193.7 | 204.0 | 165.98 ± 27.28 | |
| Muscle | Limb | Patient | Mean MVC | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |||
| mV | mV | |||||||||||
| Biceps muscle (A) | R | 2273 ± 344 | 1958 ± 327 | 2447 ± 413 | 2156 ± 310 | 2283 ± 311 | 3265 ± 413 | 2679 ± 447 | 2141 ± 361 | 2994 ± 430 | 1903 ± 258 | 2410 ± 445 |
| L | 1200 ± 154 | 1356 ± 154 | 1228 ± 169 | 1206 ± 169 | 881 ± 123 | 1167 ± 161 | 1763 ± 200 | 1395 ± 192 | 1151 ± 161 | 881 ± 123 | 1223 ± 254 | |
| Triceps muscle (B) | R | 554 ± 111 | 1058 ± 100 | 935 ± 109 | 1232 ± 133 | 1196 ± 94 | 1506 ± 122 | 855 ± 98 | 1001 ± 100 | 1066 ± 97 | 1478 ± 113 | 1088 ± 95 |
| L | 1172 ± 132 | 531 ± 341 | 381 ± 292 | 627 ± 382 | 531 ± 306 | 565 ± 392 | 525 ± 275 | 346 ± 313 | 460 ± 330 | 638 ± 378 | 577 ± 215 | |
| Deltoid middle head muscle (C) | R | 942 ± 212 | 1064 ± 144 | 926 ± 160 | 826 ± 129 | 677 ± 144 | 898 ± 190 | 1517 ± 206 | 926 ± 160 | 1219 ± 190 | 533 ± 114 | 953 ± 274 |
| L | 749 ± 30 | 695 ± 98 | 645 ± 94 | 663 ± 98 | 684 ± 98 | 621 ± 98 | 624 ± 88 | 615 ± 90 | 640 ± 95 | 684 ± 98 | 662 ± 42 | |
| Long extensor muscle of the wrist (D) | R | 2295 ± 233 | 2992 ± 482 | 2538 ± 413 | 2796 ± 420 | 3613 ± 464 | 2956 ± 420 | 2650 ± 426 | 2834 ± 461 | 3025 ± 454 | 3291 ± 423 | 2899 ± 375 |
| L | 1950 ± 163 | 2223 ± 186 | 2194 ± 173 | 2276 ± 186 | 2743 ± 200 | 2486 ± 177 | 2113 ± 177 | 2428 ± 192 | 2408 ± 197 | 2490 ± 181 | 2331 ± 226 | |
| Deltoid front head muscle (E) | R | 1502 ± 150 | 2494 ± 180 | 2133 ± 171 | 2413 ± 170 | 2597 ± 165 | 2367 ± 184 | 2219 ± 160 | 2298 ± 185 | 2413 ± 170 | 2702 ± 171 | 2314 ± 331 |
| L | 1079 ± 163 | 1779 ± 547 | 1382 ± 519 | 1372 ± 526 | 1637 ± 482 | 1692 ± 540 | 1567 ± 482 | 1482 ± 557 | 1345 ± 516 | 1742 ± 512 | 1508 ± 218 | |
| Deltoid back head muscle (E) | R | 805 ± 55 | 709 ± 138 | 671 ± 131 | 695 ± 135 | 738 ± 131 | 600 ± 126 | 701 ± 137 | 679 ± 132 | 655 ± 127 | 764 ± 135 | 702 ± 58 |
| L | 600 ± 33 | 441 ± 86 | 502 ± 85 | 489 ± 87 | 448 ± 86 | 467 ± 85 | 436 ± 85 | 515 ± 87 | 483 ± 86 | 454 ± 87 | 483 ± 49 | |
| Trapezius muscle (G) | R | 541 ± 68 | 431 ± 268 | 399 ± 241 | 405 ± 255 | 342 ± 261 | 377 ± 265 | 404 ± 251 | 422 ± 255 | 411 ± 258 | 333 ± 255 | 406 ± 57 |
| L | 361 ± 23 | 263 ± 118 | 273 ± 109 | 264 ± 111 | 264 ± 118 | 303 ± 120 | 259 ± 117 | 289 ± 115 | 290 ± 121 | 261 ± 117 | 283 ± 31 | |
| Subcapsular muscle (H) | R | 204 ± 23 | 175 ± 103 | 179 ± 102 | 170 ± 101 | 229 ± 106 | 212 ± 104 | 179 ± 105 | 181 ± 103 | 172 ± 102 | 229 ± 106 | 193 ± 23 |
| L | 166 ± 27 | 134 ± 313 | 136 ± 320 | 139 ± 323 | 184 ± 327 | 202 ± 341 | 146 ± 341 | 137 ± 323 | 142 ± 330 | 190 ± 337 | 157 ± 26 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Warguła, Ł.; Marciniak, A. The Symmetry of the Muscle Tension Signal in the Upper Limbs When Propelling a Wheelchair and Innovative Control Systems for Propulsion System Gear Ratio or Propulsion Torque: A Pilot Study. Symmetry 2022, 14, 1002. https://0-doi-org.brum.beds.ac.uk/10.3390/sym14051002
Warguła Ł, Marciniak A. The Symmetry of the Muscle Tension Signal in the Upper Limbs When Propelling a Wheelchair and Innovative Control Systems for Propulsion System Gear Ratio or Propulsion Torque: A Pilot Study. Symmetry. 2022; 14(5):1002. https://0-doi-org.brum.beds.ac.uk/10.3390/sym14051002
Chicago/Turabian StyleWarguła, Łukasz, and Agnieszka Marciniak. 2022. "The Symmetry of the Muscle Tension Signal in the Upper Limbs When Propelling a Wheelchair and Innovative Control Systems for Propulsion System Gear Ratio or Propulsion Torque: A Pilot Study" Symmetry 14, no. 5: 1002. https://0-doi-org.brum.beds.ac.uk/10.3390/sym14051002