
Does Sex, Skeletal Class and Mandibular Asymmetry Affect Tooth Length and Asymmetry in Tooth Length?

 , , ,
, , ,
Abstract
:1. Introduction
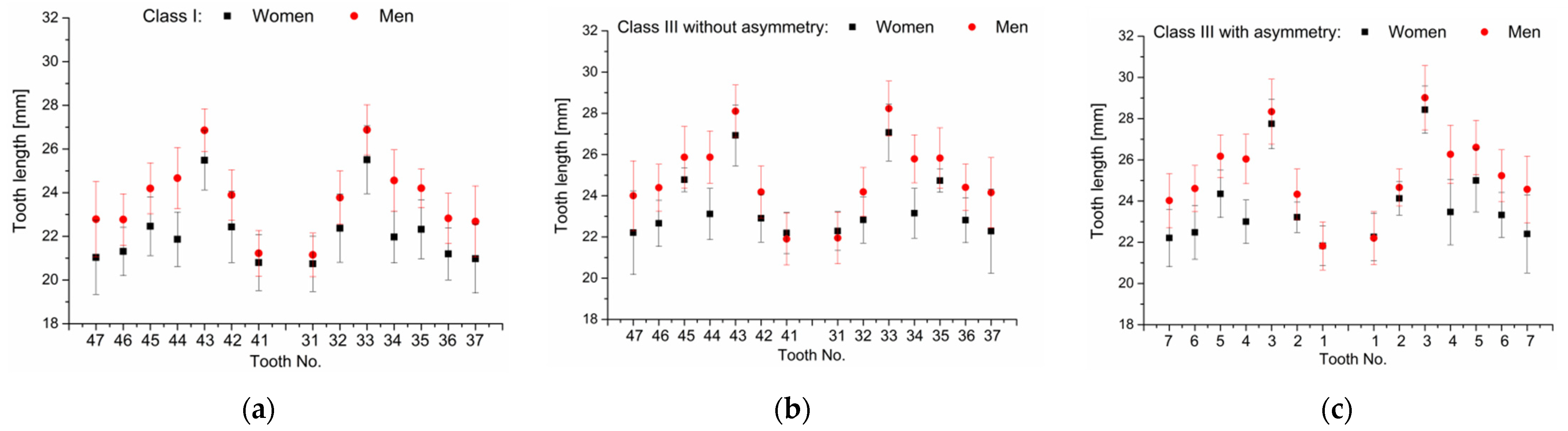
- There is no sexual dimorphism in lower tooth length;
- There are no differences in tooth length in skeletal class III patients with asymmetry depending on the side of the mandible (with/without excessive growth);
- There are no differences in tooth length between patients with class I and patients with class III without asymmetry.
2. Materials and Methods
- No history of previous orthodontic treatment;
- Complete dentition in the lower arch from at least the 2nd molar to the 2nd molar (minimum 14 teeth);
- Patients with skeletal class I and skeletal class III (with or without asymmetry);
- Generally healthy patients, with no history of bone disease (past or present).
- Incomplete root development;
- Root resorption (due to trauma or inflammation);
- Genetic defects in tooth anatomy;
- Significant damage to the tooth crown, making it impossible to assess anatomy;
- History of previous orthodontic treatment;
- Class III problem in conjunction with other skeletal malformations, which may indicate a genetic syndrome;
- No sex, age or race limitations were applied.
3. Results
3.1. Verification of Null Hypothesis No. 1: Hypothesis Rejected
3.2. Verification of Null Hypothesis No. 2: Hypothesis Confirmed
3.3. Verification of Null Hypothesis No. 3: Hypothesis Rejected
4. Discussion
Limitations of the Study
5. Conclusions
- In all three study groups, some of men’s lower teeth were longer than women’s, so null hypothesis 1 was rejected.
- Mandibular asymmetry and the resulting differences in the anatomy (length) of the alveolar part of the mandible on the right and left side did not affect the differences in the length of the teeth on the hyperplastic and non-hyperplastic side, so null hypothesis 2 was confirmed.
- In skeletal class III patients without asymmetry, some lower teeth were longer than they were in skeletal class I patients, so null hypothesis 3 was rejected.
- When creating computational models that allow for the designing of orthodontic aligners and analyzing the forces acting on teeth, software developers should account for the sex and the skeletal class of the patient. This is why current models, which do not differentiate between patients in these respects, have significant limitations and cannot be extrapolated to the whole population.
- Clinicians should account for sex as well as the skeletal class of patients when predicting the difficulty and effectiveness of an orthodontic treatment to be implemented.
- It may be advisable to create a database describing the dental anatomy of patients with different anatomical characteristics, which can be used by clinicians when examining their patients. This can enable simple individualization of orthodontic treatment without the need to take any additional, time-consuming steps.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, L.; Zhan, Q.; Zhou, J.; Kuang, Q.; Yan, X.; Zhang, X.; Shan, Y.; Li, X.; Lai, W.; Long, H. Effectiveness of an anterior mini-screw in achieving incisor intrusion and palatal root torque for anterior retraction with clear aligners: A finite element study. Angle Orthod. 2021, 91, 794–803. [Google Scholar] [CrossRef]
- Ayidağa, C.; Kamiloğlu, B. Effects of Variable Composite Attachment Shapes in Controlling Upper Molar Distalization with Aligners: A Nonlinear Finite Element Study. J. Healthc. Eng. 2021, 2021, 5557483. [Google Scholar] [CrossRef]
- Yokoi, Y.; Arai, A.; Kawamura, J.; Uozumi, T.; Usui, Y.; Okafuji, N. Effects of attachment of plastic aligner in closing of diastema of maxillary dentition by finite element method. J. Healthc. Eng. 2019, 2019, 1075097. [Google Scholar] [CrossRef]
- Barone, S.; Paoli, A.; Razionale, A.; Savignano, R. Computational design and engineering of polymeric orthodontic aligners. Int. J. Numer. Method. Biomed. Eng. 2017, 33, 2839. [Google Scholar] [CrossRef]
- Rossini, G.; Schiaffino, M.; Parrini, S.; Sedran, A.; Deregibus, A.; Castroflorio, T. Upper Second Molar Distalization with Clear Aligners: A Finite Element Study. Appl. Sci. 2020, 10, 7739. [Google Scholar] [CrossRef]
- Ma, Y.; Li, S. The optimal orthodontic displacement of clear aligner for mild. moderate and severe periodontal conditions: An in vitro study in a periodontally compromised individual using the finite element model. BMC Oral Health 2021, 21, 109. [Google Scholar] [CrossRef]
- Cortona, A.; Rossini, G.; Parrini, S.; Deregibus, A.; Castroflorio, T. Clear aligner orthodontic therapy of rotated mandibular round-shaped teeth: A finite element study. Angle Orthod. 2020, 90, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Liang, W.; Rong, Q.; Lin, J.; Xu, B. Torque control of the maxillary incisors in lingual and labial orthodontics: A 3-dimensional finite element analysis. Am. J. Orthod. Dentofac. Orthoped. 2009, 135, 316–322. [Google Scholar] [CrossRef]
- Comba, B.; Parrini, S.; Rossini, G.; Castroflorio, T.; Deregibus, A. A three-dimensional finite element analysis of upper-canine distalization with clear aligners, composite attachments, and class II elastics. J. Clin. Orthod. 2017, 51, 24–28. [Google Scholar]
- Gomez, J.P.; Peña, F.M.; Martínez, V.; Giraldo, D.C.; Cardona, C.I. Initial force systems during bodily tooth movement with plastic aligners and composite attachments—A three-dimensional finite element analysis. Angle Orthod. 2014, 85, 454–460. [Google Scholar] [CrossRef]
- Jiang, T.; Wu, R.Y.; Wang, J.K.; Wang, H.H.; Tang, G.H. Clear aligners for maxillary anterior en masse retraction: A 3D finite element study. Sci. Rep. 2020, 10, 10156. [Google Scholar] [CrossRef]
- Baek, S.-H.; Cha, H.-S.; Cha, J.-Y.; Moon, Y.-S.; Sung, S.-J. Three-dimensional finite element analysis of the deformation of the human mandible: A preliminary study from the perspective of orthodontic mini-implant stability. Korean, J. Orthod. 2012, 42, 159–168. [Google Scholar] [CrossRef] [Green Version]
- Cattaneo, P.; Dalstra, M.; Melsen, B. The finite element method: A tool to study orthodontic tooth movement. J. Dent. Res. 2005, 84, 428–433. [Google Scholar] [CrossRef]
- Hong, K.; Kim, W.-H.; Eghan-Acquah, E.; Lee, J.-H.; Lee, B.-K.; Kim, B. Efficient Design of a Clear Aligner Attachment to Induce Bodily Tooth Movement in Orthodontic Treatment Using Finite Element Analysis. Materials 2021, 14, 4926. [Google Scholar] [CrossRef]
- Kim, W.-H.; Hong, K.; Lim, D.; Lee, J.-H.; Jung, Y.J.; Kim, B. Optimal Position of Attachment for Removable Thermoplastic Aligner on the Lower Canine Using Finite Element Analysis. Materials 2020, 13, 3369. [Google Scholar] [CrossRef]
- Seo, J.-H.; Eghan-Acquah, E.; Kim, M.-S.; Lee, J.-H.; Jeong, Y.-H.; Jung, T.-G.; Hong, M.; Kim, W.-H.; Kim, B.; Lee, S.-J. Comparative Analysis of Stress in the Periodontal Ligament and Center of Rotation in the Tooth after Orthodontic Treatment Depending on Clear Aligner Thickness—Finite Element Analysis Study. Materials 2021, 14, 324. [Google Scholar] [CrossRef]
- D’Antò, V.; Bucci, R.; De Simone, V.; Ghislanzoni, L.H.; Michelotti, A.; Rongo, R. Evaluation of Tooth Movement Accuracy with Aligners: A Prospective Study. Materials 2022, 15, 2646. [Google Scholar] [CrossRef]
- Andrews, L.F. The six keys to normal occlusion. Am. J. Orthod. Dentofac. Orthoped. 1972, 6, 296–309. [Google Scholar] [CrossRef]
- Burstone, C.J.; Pryputniewicz, R.J. Holographic determination of centers of rotation produced by orthodontic forces. Am. J. Orthod. Dentofac. Orthoped. 1980, 77, 396–409. [Google Scholar] [CrossRef]
- Barone, S.; Paoli, A.; Razionale, A.V. CT segmentation of dental shapes by anatomy-driven reformation imaging and B-spline modelling. Int. J. Numer. Method. Biomed. Eng. 2015, 32, e02747. [Google Scholar] [CrossRef]
- Jacobson, A. The “Wits” appraisal of jaw disharmony. Am. J. Orthod. Dentofac. Orthoped. 1975, 67, 125–138. [Google Scholar] [CrossRef]
- Segner, D.; Hasund, A. Individualisierte Kephalometrie, 2nd ed.; Sietmar Segner Verlag: Hamburg, Germany, 1994; ISBN 3980270920. [Google Scholar]
- Paradowska-Stolarz, A. MSX1 gene in the etiology of orofacial deformities. Postepy Hig. Med. Dosw. 2015, 69, 1499–1504. [Google Scholar]
- De Coster, P.J.; Marks, L.A.; Martens, L.C.; Huysseune, A. Dental agenesis: Genetic and clinical perpectives. J. Oral. Pathol. Med. 2009, 38, 1–17. [Google Scholar] [CrossRef]
- Gershater, E.; Li, C.; Ha, P.; Chung, C.H.; Tanna, N.; Zou, M.; Zheng, Z. Genes and Pathways Associated with Skeletal Sagittal Malocclusions: A Systematic Review. Int. J. Mol. Sci. 2021, 22, 13037. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group Name | Mandibular Asymmetry | Sex | n | Age |
|---|---|---|---|---|
| Class I | - | men | 19 | 23.8 ± 2 |
| - | women | 18 | 22.9 ± 2 | |
| Class III | without asymmetry | men | 17 | 24.1 ± 3 |
| women | 14 | 23.7 ± 3 | ||
| with asymmetry | men | 13 | 25.8 ± 3 | |
| women | 11 | 24.4 ± 3 |
| Class I | Class III without Asymmetry | Class III with Asymmetry | |||||
|---|---|---|---|---|---|---|---|
| Tooth | p-Value | Mean Diff. | p-Value | Mean Diff. | Tooth | p-Value | Mean Diff. |
| 47 | * 0.006 | 1.748 | * 0.022 | 1.792 | 7 | * 0.019 | 1.817 |
| 46 | 0.055 | 1.464 | * 0.032 | 1.732 | 6 | * 0.002 | 2.127 |
| 45 | * 0.007 | 1.740 | 0.608 | 1.092 | 5 | * 0.018 | 1.828 |
| 44 | * 8.06 × 10−8 | 2.803 | * 5.36 × 10−6 | 2.760 | 4 | * 4.56 × 10−7 | 3.042 |
| 43 | 0.100 | 1.371 | 0.487 | 1.173 | 3 | 0.995 | 0.590 |
| 42 | 0.056 | 1.460 | 0.341 | 1.278 | 2 | 0.571 | 1.117 |
| 41 | 0.999 | 0.425 | 1.000 | −0.291 | 1 | 1.000 | −0.007 |
| 37 | * 0.008 | 1.701 | * 0.010 | 1.872 | 7 h | * 0.010 | 2.162 |
| 36 | * 0.014 | 1.626 | 0.063 | 1.593 | 6 h | * 0.045 | 1.909 |
| 35 | * 0.001 | 1.892 | 0.571 | 1.096 | 5 h | 0.192 | 1.606 |
| 34 | * 5.90 × 10−7 | 2.594 | * 1.06 × 10−5 | 2.640 | 4 h | * 1.04 × 10−4 | 2.804 |
| 33 | 0.091 | 1.370 | 0.475 | 1.159 | 3 h | 0.999 | 0.583 |
| 32 | 0.072 | 1.406 | 0.219 | 1.359 | 2 h | 1.000 | 0.531 |
| 31 | 1.000 | 0.408 | 1.000 | −0.337 | 1 h | 1.000 | −0.058 |
| Total: | * 1.78 × 10−8 | 1.572 | * 2.55 × 10−4 | 1.351 | Total: | * 3.96 × 10−8 | 1.432 |
| Class III with Asymmetry (Men) | Class III with Asymmetry (Women) | |||||
|---|---|---|---|---|---|---|
| Tooth | Mean ± SD [mm] | p-Value | Mean Diff. | Mean ± SD [mm] | p-Value | Mean Diff. |
| 7 | 24.02 ± 1.31 | 0.999 | 0.541 | 22.21 ± 1.39 22.40 ± 1.89 | 1.000 | 0.195 |
| 7 h | 24.56 ± 1.62 | |||||
| 6 | 24.61 ± 1.13 | 0.994 | 0.628 | 22.48 ± 1.30 | 0.947 | 0.846 |
| 6 h | 25.23 ± 1.25 | 23.33 ± 1.09 | ||||
| 5 | 26.18 ± 1.03 | 1.000 | 0.427 | 24.35 ± 1.15 | 0.994 | 0.649 |
| 5 h | 26.60 ± 1.31 | 25.00 ± 1.53 | ||||
| 4 | 26.04 ± 1.20 | 1.000 | 0.228 | 23.00 ± 1.05 | 1.000 | 0.467 |
| 4 h | 26.27 ± 1.40 | 23.47 ± 1.59 | ||||
| 3 | 28.34 ± 1.58 | 0.988 | 0.678 | 27.75 ± 1.20 | 0.991 | 0.685 |
| 3 h | 29.02 ± 1.56 | 28.43 ± 1.14 | ||||
| 2 | 24.33 ± 1.23 | 1.000 | 0.329 | 23.21 ± 0.74 | 0.907 | 0.915 |
| 2 h | 24.55 ± 0.90 | 24.13 ± 0.81 | ||||
| 1 | 21.82 ± 1.16 | 1.000 | 0.380 | 21.83 ± 0.95 | 1.000 | 0.431 |
| 1 h | 22.20 ± 1.28 | 22.26 ± 1.16 | ||||
| Total: 7 ÷ 1 | 25.05 ± 2.26 | 0.182 | 0.459 | 23.55 ± 2.18 | 0.104 | 0.598 |
| Total: 7 h ÷ 1 h | 25.51 ± 2.36 | 24.14 ± 2.36 | ||||
| Men | Women | ||||||
|---|---|---|---|---|---|---|---|
| Tooth | Class | Mean ± SD [mm] | p-Value | Mean Diff. | Mean ± SD [mm] | p-Value | Mean Diff. |
| 47 | I | 22.78 ± 1.73 | 0.073 | 1.219 | 21.03 ± 1.69 22.21 ± 2.03 | 0.164 | 1.175 |
| III | 24.00 ± 1.70 | ||||||
| 46 | I | 22.77 ± 1.18 | * 0.33 × 10−4 | 1.622 | 21.31 ± 1.11 | * 0.008 | 1.354 |
| III | 24.39 ± 1.13 | 22.66 ± 1.12 | |||||
| 45 | I | 24.20 ± 1.17 | * 7.00 × 10−4 | 1.674 | 22.46 ± 1.34 | * 3.21 × 10−6 | 2.323 |
| III | 25.87 ± 1.49 | 25.78 ± 0.58 | |||||
| 44 | I | 24.67 ± 1.40 | * 0.0214 | 1.206 | 21.86 ± 1.24 | * 0.018 | 1.249 |
| III | 25.87 ± 1.27 | 23.11 ± 1.24 | |||||
| 43 | I | 26.86 ± 0.98 | * 0.013 | 1.246 | 25.49 ± 1.35 | * 0.016 | 1.444 |
| III | 28.10 ± 1.27 | 26.93 ± 1.48 | |||||
| 42 | I | 23.89 ± 1.16 | 0.755 | 0.290 | 22.43 ± 1.63 | 0.586 | 0.472 |
| III | 24.18 ± 1.26 | 22.90 ± 1.15 | |||||
| 41 | I | 21.23 ± 1.04 | 0.196 | 0.676 | 20.80 ± 1.28 | * 0.004 | 1.393 |
| III | 21.90 ± 1.26 | 22.19 ± 1.00 | |||||
| 37 | I | 22.68 ± 1.63 | * 0.027 | 1.474 | 20.98 ± 1.57 | 0.130 | 1.303 |
| III | 24.15 ± 1.70 | 22.28 ± 2.04 | |||||
| 36 | I | 22.82 ± 1.15 | * 5.69 × 10−4 | 1.583 | 21.20 ± 1.19 | * 0.001 | 1.617 |
| III | 24.41 ± 1.13 | 22.81 ± 1.09 | |||||
| 35 | I | 24.21 ± 0.89 | * 7.79 × 10−4 | 1.618 | 22.32 ± 1.35 | * 8.99 × 10−6 | 2.414 |
| III | 25.83 ± 1.47 | 24.73 ± 9.56 | |||||
| 34 | I | 24.56 ± 1.40 | * 0.021 | 1.231 | 21.97 ± 1.18 | * 0.044 | 1.185 |
| III | 25.79 ± 1.16 | 23.15 ± 1.21 | |||||
| 33 | I | 26.88 ± 1.15 | * 0.010 | 1.366 | 25.51 ± 1.55 | * 0.011 | 1.567 |
| III | 28.23 ± 1.33 | 27.07 ± 1.38 | |||||
| 32 | I | 23.77 ± 1.22 | 0.528 | 0.411 | 22.37 ± 1.56 | 0.587 | 0.459 |
| III | 24.19 ± 1.19 | 22.83 ± 1.12 | |||||
| 31 | I | 21.15 ± 1.00 | 0.112 | 0.799 | 20.74 ± 1.27 | * 0.002 | 1.543 |
| III | 21.95 ± 1.25 | 22.29 ± 0.94 | |||||
| Total: 47 ÷ 31 | I | 23.75 ± 2.06 | * 2.54 × 10−9 | 1.172 | 22.18 ± 2.01 | * 0 | 1.393 |
| III | 24.92 ± 2.23 | 23.57 ± 2.03 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Warnecki, M.; Żak, M.; Szkoda-Poliszuk, K.; Kawala, B.; Sarul, M. Does Sex, Skeletal Class and Mandibular Asymmetry Affect Tooth Length and Asymmetry in Tooth Length? Symmetry 2022, 14, 1069. https://0-doi-org.brum.beds.ac.uk/10.3390/sym14051069
Warnecki M, Żak M, Szkoda-Poliszuk K, Kawala B, Sarul M. Does Sex, Skeletal Class and Mandibular Asymmetry Affect Tooth Length and Asymmetry in Tooth Length? Symmetry. 2022; 14(5):1069. https://0-doi-org.brum.beds.ac.uk/10.3390/sym14051069
Chicago/Turabian StyleWarnecki, Maciej, Małgorzata Żak, Klaudia Szkoda-Poliszuk, Beata Kawala, and Michał Sarul. 2022. "Does Sex, Skeletal Class and Mandibular Asymmetry Affect Tooth Length and Asymmetry in Tooth Length?" Symmetry 14, no. 5: 1069. https://0-doi-org.brum.beds.ac.uk/10.3390/sym14051069