
Proof-of-Concept Study of the Use of Accelerometry to Quantify Knee Joint Movement and Assist with the Diagnosis of Juvenile Idiopathic Arthritis

 ,
,
Abstract
:1. Introduction
1.1. Juvenile Idiopathic Arthritis
1.2. Approaches to Assist with JIA Diagnosis and Management
1.3. Accelerometry for Joint Movement Analysis
2. Materials and Methods
2.1. Ethical Approval
2.2. Recruitment Process
2.3. Participant Inclusion and Exclusion Criteria
- Aged ≥8 and ≤16 years old (this ensured participants were old enough to engage with the researchers and follow the demonstrated walking and flexion-extension movements).
- Confirmed diagnosis of JIA (polyarticular JIA, oligoarticular JIA, psoriatic JIA, and enthesitis-related JIA subtypes).
- Ability to engage with and use accelerometry equipment.
- Aged >16 years or <8 years.
- Diagnosis of any other previous joint condition affecting the lower limbs.
- Fracture of any bone in the previous four months.
- Diagnosis of any muscle condition (e.g., muscular dystrophy).
- Diagnosis of chronic pain syndrome.
- Diagnosis of either systemic or undifferentiated JIA (this ensured homogeneity of the population sample investigated).
- Clinician or parental concern that the participant may not be able to complete accelerometry movement analysis for any reason.
- Presence of a condition that predisposes a child to any sudden, involuntary movements such as tics or chorea (these movements may interfere with accelerometer readings).
- BMI more than 99.6th centile or below 0.4th centile. The exclusion of participants with extremes of BMI controlled for the impact of skin movement artifacts on the accelerometry.
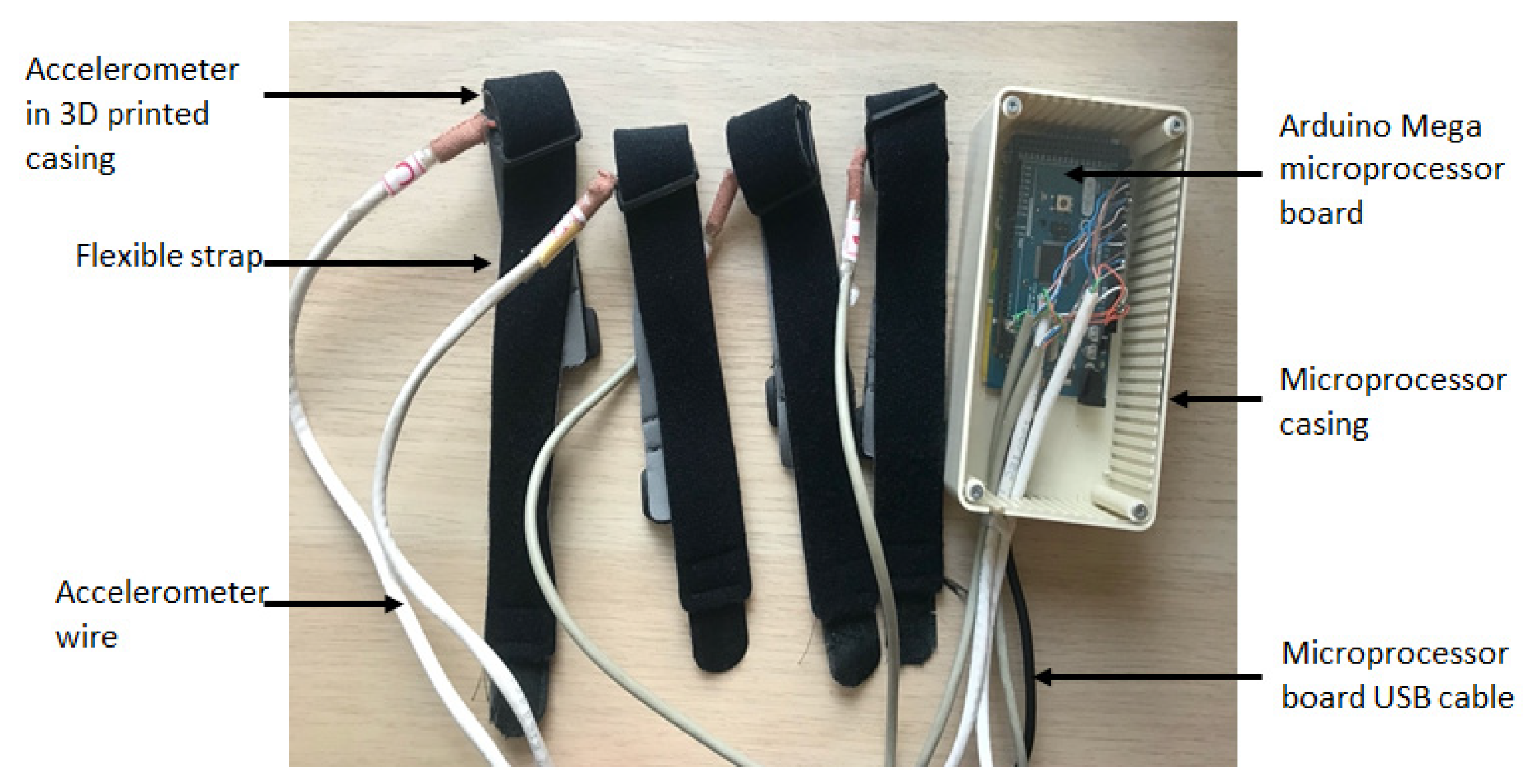
2.4. Materials
2.5. Accelerometer Data Recordings
- Maximally flex (flexion) and extend (extension) the leg with an actively inflamed knee ten times whilst lying down on a hospital bed. This was then repeated on the contralateral (control) side.
- Walk a distance of 10 m normally in a straight path. For this to be possible, a clinician walked with the participant, holding the PC that stored the data.
- Data from the left leg, flexion-extension movements;
- Data from the right leg, flexion-extension movements;
- Data from the left leg while walking;
- Data from the right leg while walking.
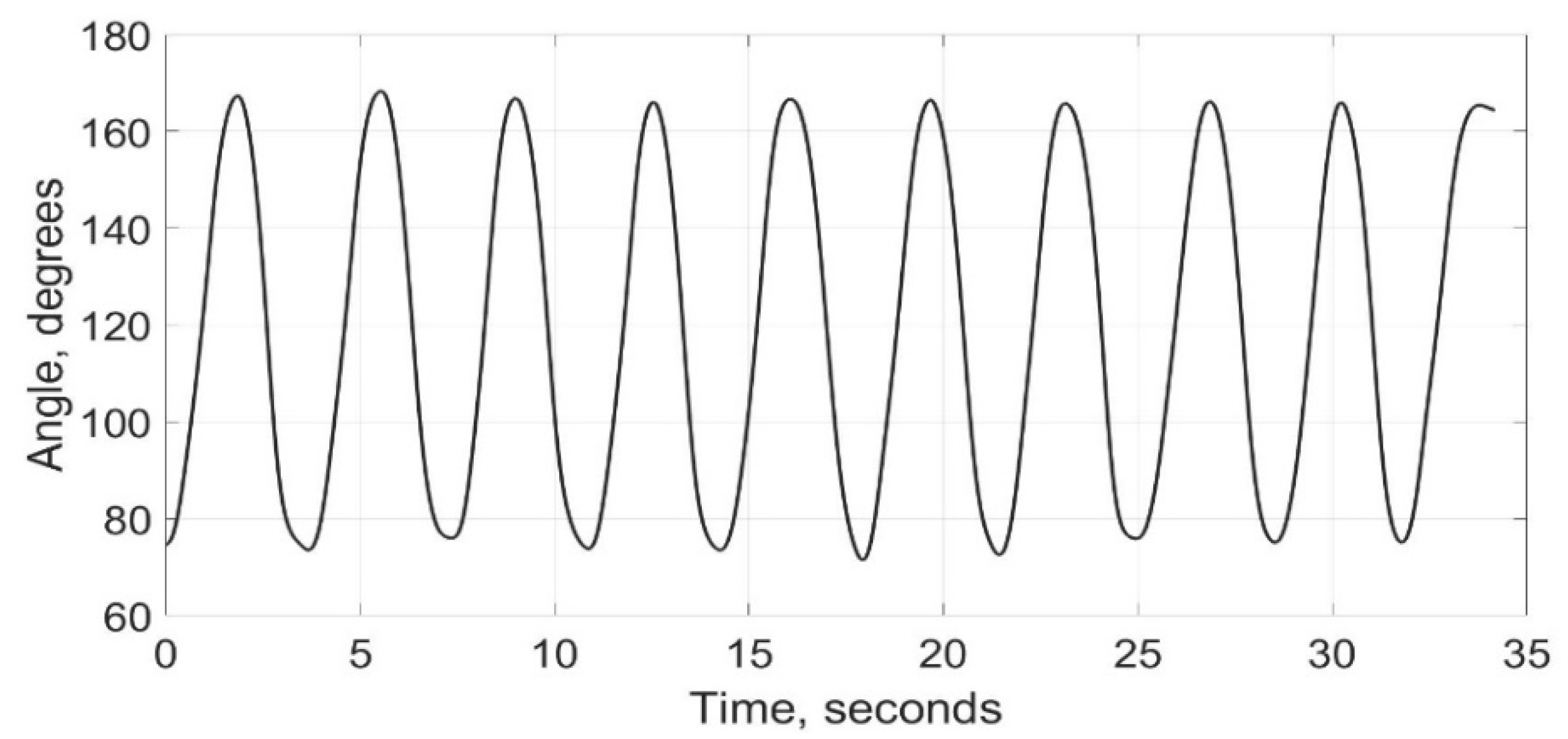
2.6. Accelerometry Data Calculations
2.7. Data Processing and Statistical Analysis
3. Results and Discussion
3.1. Participant Demographics
3.2. Overall Descriptive Analysis
3.3. Tests for Significance
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petty, R.E.; Southwood, T.R.; Manners, P.; Baum, J.; Glass, D.N.; Goldenberg, J.; He, X.; Maldonado-Cocco, J.; Orozco-Alcala, J.; Prieur, A.-M.; et al. International League of Association for Rheumatology Classification of Juvenile Idiopathic Arthritis: Second Revsion, Edmonton, 2001. J. Rheumatol. 2004, 31, 390–392. [Google Scholar]
- Malattia, C.; Martini, A. Juvenile idiopathic arthritis. In The Autoimmune Diseases, 6th ed.; Rose, N.R., Mackay, I.R., Eds.; Academic Press: Cambridge, MA, USA, 2020; Chapter 3; pp. 675–690. [Google Scholar] [CrossRef] [Green Version]
- Nwaizu, H.; Saatchi, R.; Hawley, D.P.; Ward, O. Thermal and visual imaging to assist with juvenile idiopathic arthritis examination of the knees. Technologies 2020, 8, 30. [Google Scholar] [CrossRef]
- Thierry, S.; Fautrel, B.; Lemelle, I.; Guillemin, F. Prevalence and incidence of juvenile idiopathic arthritis: A systematic review. Jt. Bone Spine 2014, 81, 112–117. [Google Scholar] [CrossRef]
- Jacobson, J.L.; Pham, J.T. Juvenile idiopathic arthritis: A focus on pharmacologic management. J. Pediatric Health Care 2018, 32, 515–528. [Google Scholar] [CrossRef] [Green Version]
- Martini, A.; Ravelli, A.; Avcin, T.; Beresford, M.W.; Burgos-Vargas, R.; Cuttica, R.; Ilowite, N.T.; Khubchandani, R.; Laxer, R.M.; Lovell, D.J.; et al. Toward new classification criteria for juvenile idiopathic arthritis: First steps: Pediatric rheumatology international trials organization international consensus. J. Rheumatol. 2019, 46, 190–197. [Google Scholar] [CrossRef] [Green Version]
- Heidari, B. Rheumatoid arthritis: Early diagnosis and treatment outcomes. Casp. J. Intern. Med. 2011, 2, 161–170. [Google Scholar]
- Prahalad, S.; Glass, D. Is juvenile rheumatoid arthritis/juvenile idiopathic arthritis different from rheumatoid arthritis? Arthritis Res. 2002, 4 (Suppl. 3), 1–8. [Google Scholar] [CrossRef] [Green Version]
- Barut, K.; Adrovic, A.; Şahin, S.; Kasapçopur, Ö. Juvenile idiopathic arthritis. Balk. Med. J. 2017, 34, 90–101. [Google Scholar] [CrossRef]
- McMahon, A.M.; Tattersall, R. Diagnosing juvenile idiopathic arthritis. Paediatr. Child Health 2011, 21, 552–557. [Google Scholar] [CrossRef]
- Hahn, Y.S.; Kim, J.G. Pathogenesis and clinical manifestations of juvenile rheumatoid arthritis. Korean J. Pediatrics 2010, 53, 921–930. [Google Scholar] [CrossRef]
- Okamoto, M.; Yokota, S.; Takei, S.; Okura, Y.; Kubota, T.; Shimizu, M.; Nozawa, T.; Iwata, N.; Umebayashi, H.; Kinjo, N.; et al. Clinical practice guidance for juvenile idiopathic arthritis (JIA). Mod. Rheumatol. 2019, 29, 41–59. [Google Scholar] [CrossRef]
- Hartmann, M.; Kreuzpointner, F.; Haefner, R.; Michels, H.; Schwirtz, A.; Haas, J.P. Effects of juvenile idiopathic arthritis on kinematics and kinetics of the lower extremities call for consequences in physical activities recommendations. Int. J. Pediatrics 2010, 2010, 835984. [Google Scholar] [CrossRef] [Green Version]
- Woolnough, L.; Pomputius, A.; Vincent, H.K. Juvenile idiopathic arthritis, gait characteristics and relation to function. Gait Posture 2021, 85, 38–54. [Google Scholar] [CrossRef]
- Foster, H.E.; Kay, L.J.; Friswell, M.; Coady, D.; Myers, A. Musculoskeletal screening examination (pGALS) for school-age children based on the adult GALS screen. Arthritis Care Res. 2006, 55, 709–716. [Google Scholar] [CrossRef]
- Magni-Manzoni, S.; Epis, O.; Ravelli, A.; Klersy, C.; Veisconti, C.; Lanni, S.; Muratore, V.; Sciré, C.A.; Rossi, S.; Montecucco, C. Comparison of clinical versus ultrasound-determined synovitis in juvenile idiopathic arthritis. Arthritis Rheum. 2009, 61, 1497–1504. [Google Scholar] [CrossRef]
- Giancane, G.; Consolaro, A.; Lanni, S.; Davi, S.; Schiappapietra, B.; Ravelli, A. Juvenile idiopathic arthritis: Diagnosis and treatment. Rheumatol. Ther. 2016, 3, 187–207. [Google Scholar] [CrossRef] [Green Version]
- Muller, L.-S.O.; Humphries, P.; Rosendahl, K. The joints in juvenile idiopathic arthritis. Insights Imaging 2015, 6, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Boros, C.; Whitehead, B. Juvenile idiopathic arthritis. Aust. Fam. Physician 2010, 39, 630–636. [Google Scholar]
- Ramos, P.C.; Ceccarelli, F.; Jousse-Joulin, S. Role of ultrasound in the assessment of juvenile idiopathic arthritis. Rheumatology 2012, 51 (Suppl. 7), 10–12. [Google Scholar] [CrossRef] [Green Version]
- Damasio, M.B.; De Horatio, L.T.; Boavida, P.; Lambot-Juhan, K.; Rosendahl, K.; Tomà, P.; Muller, L.S.O. Imaging in juvenile idiopathic arthritis (JIA): An update with particular emphasis on MRI. Acta Radiol. 2013, 54, 1015–1023. [Google Scholar] [CrossRef]
- Lerkvaleekul, B.; Jaovisidha, S.; Sungkarat, W.; Chitrapazt, N.; Fuangfa, P.; Ruangchaijatuporn, T.; Vilaiyuk, S. The comparisons between thermography and ultrasonography with physical examination for wrist joint assessment in juvenile idiopathic arthritis. Physiol. Meas. 2017, 38, 691–700. [Google Scholar] [CrossRef]
- Porter-Young, F.M.; Offiah, A.C.; Broadley, P.; Lang, I.; McMahon, A.M.; Howsley, P.; Hawley, D.P. Correction to: Inter- and intra-observer reliability of contrast-enhanced magnetic resonance imaging parameters in children with suspected juvenile idiopathic arthritis of the hip. Pediatric Radiol. 2018, 48, 1901. [Google Scholar] [CrossRef] [Green Version]
- Costa, A.F.; van der Pol, C.B.; Maralani, P.J.; McInnes, M.D.F.; Shewchuk, J.R.; Verma, R.; Hurrell, C.; Schieda, N. Gadolinium deposition in the brain: A systematic review of existing guidelines and policy statement issued by the Canadian Association of Radiologists. Can. Assoc. Radiol. J. 2018, 69, 373–382. [Google Scholar]
- Baildam, E. A commentary on TREAT: The trial of early aggressive drug therapy in juvenile idiopathic arthritis. BMC Med. 2012, 10, 59. [Google Scholar] [CrossRef] [Green Version]
- Wallace, C.A.; Giannini, E.H.; Spalding, S.J.; Hashkes, P.J.; O’Neil, K.M.; Zeft, A.S.; Szer, I.S.; Ringold, S.; Brunner, H.I.; Schanberg, L.E.; et al. Trial of early aggressive therapy in polyarticular juvenile idiopathic arthritis. Arthritis Rheum. 2012, 64, 2012–2021. [Google Scholar] [CrossRef] [Green Version]
- Nwaizu, H.; Saatchi, R.; Burke, D. Inertial measurement techniques for human Joints movement analysis. Stud. Health Technol. Inform. 2017, 242, 717–724. [Google Scholar] [CrossRef]
- Nwaizu, H.; Saatchi, R.; Burke, D. Accelerometer based human joints’ range of movement measurement. In Proceedings of the 2016 10th International Symposium on Communication Systems, Networks and Digital Signal Processing (CSNDSP), Prague, Czech Republic, 20–22 July 2016; pp. 1–6. [Google Scholar] [CrossRef]
- Fennema, M.C.; Bloomfield, R.A.; Lanting, B.A.; Birmingham, T.B.; Teeter, M.G. Repeatability of measuring knee flexion angles with wearable inertial sensors. Knee 2019, 26, 97–105. [Google Scholar] [CrossRef] [Green Version]
- McGinnis, R.S.; Patel, S.; Silva, I.; Mahadevan, N.; Dicristofaro, S.; Jortberg, E.; Ceruolo, M.; Aranyosi, A.J. Skin mounted accelerometer system for measuring knee range of motion. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 5298–5302. [Google Scholar] [CrossRef]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.S. Validity and reliability ofwearable sensors for joint angle estimation: A systematic review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef] [Green Version]
- Barden, J.M.; Clermont, C.A.; Kobsar, D.; Beauchet, O. Accelerometer-based step regularity is lower in older adults with bilateral knee osteoarthritis. Front. Hum. Neurosci. 2016, 10, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Prioreschi, A.; Hodkinson, B.; Avidon, I.; Tikly, M.; McVeigh, J.A. The clinical utility of accelerometry in patients with rheumatoid arthritis. Rheumatology 2013, 52, 1721–1727. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, T.; Yoshiuchi, K.; Inada, S.; Shirakura, K.; Wada, N.; Takeuchi, K.; Matsushita, M. Physical activity of elderly patients with rheumatoid arthritis and healthy individuals: An actigraphy study. BioPsychoSoc. Med. 2015, 9, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Andreu-Perez, J.; Garcia-Gancedo, L.; McKinnell, J.; van der Drift, A.; Powell, A.; Hamy, V.; Keller, T.; Yang, G.Z. Developing fine-grained actigraphies for rheumatoid arthritis patients from a single accelerometer using machine learning. Sensors 2017, 17, 2113. [Google Scholar] [CrossRef]
- Fenton, S.A.M.; van Zanten, J.J.C.S.V.; Duda, J.L.; Metsios, G.S.; Kitas, G.D. Sedentary behaviour in rheumatoid arthritis: Definition, measurement and implications for health. Rheumatology 2018, 57, 213–226. [Google Scholar] [CrossRef] [Green Version]
- Faria, A.C.D.; Pinheiro, G.R.C.; Neri, J.; Melo, P.L. Instrumentation for the analysis of changes in the knee joint of patients with rheumatoid arthritis: Focus on low-frequency vibrations. J. Phys. Conf. Ser. 2018, 1044, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Reddy, N.P.; Rothschild, B.M.; Mandal, M.; Gupta, V.; Suryanarayanan, S. Noninvasive acceleration measurements to characterize knee arthritis and chondromalacia. Ann. Biomed. Eng. 1995, 23, 78–84. [Google Scholar] [CrossRef]
- Reddy, N.P.; Rothschild, B.M.; Verrall, E.; Joshi, A. Noninvasive measurement of acceleration at the knee joint in patients with rheumatoid arthritis and spondyloarthropathy of the knee. Ann. Biomed. Eng. 2001, 29, 1106–1111. [Google Scholar] [CrossRef]
- Meier, R. CoolTerm [Computer Software]. 2001. Available online: https://freeware.the-meiers.org/ (accessed on 17 June 2022).
- MATLAB, The MathWorks Inc. [Computer Software]. 2021. Available online: https://uk.mathworks.com/products/matlab.html?s_tid=hp_products_matlab (accessed on 17 June 2022).
- Bakhshi, S.; Mahoor, H.M.; Davidson, B.S. Development of a body joint angle measurement system using IMU sensors. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 6923–6926. [Google Scholar]
- Djuriü-Joviþiü, M.D.; Joviþiü, N.S.; Popoviü, D.B. Kinematics of gait: New method for angle estimation based on accelerometers. Sensors 2011, 11, 10571–10585. [Google Scholar]
- Seel, T.; Raisch, J.; Schauer, T. IMU-based joint angle measurement for gait analysis. Sensors 2014, 14, 6891–6909. [Google Scholar]
- SPSS Inc. IBM SPSS Statistics Version 26 for Mac. [Computer Software]. 2021. Available online: https://www.ibm.com/uk-en/products/spss-statistics (accessed on 17 June 2022).
- Nørgaard, M.; Twilt, M.; Andersen, L.B.; Herlin, T. Accelerometry-based monitoring of daily physical activity in children with juvenile idiopathic arthritis. Scand. J. Rheumatol. 2016, 45, 179–187. [Google Scholar] [CrossRef]
- Kuntze, G.; Nesbitt, C.; Whittaker, J.L.; Nettel-Aguirre, A.; Toomey, C.; Esau, S.; Doyle-Baker, P.K.; Shank, J.; Brooks, J.; Benseler, S. Exercise therapy in juvenile idiopathic arthritis: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2018, 99, 178–193. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | JIA Subtype | Actively Inflamed Knee Joint | Clinician Observation | ||
|---|---|---|---|---|---|
| Warm | Swollen | Restricted | |||
| 1 | Oligoarticular | Right | Yes | Yes | Yes |
| 2 | Oligoarticular | Left | Yes | Yes | Yes |
| 3 | Polyarticular | Right | No | Yes | No |
| 4 | Oligoarticular | Right | No | Yes | Yes |
| 5 | Oligoarticular | Left | No | No | No |
| 6 | Oligoarticular | Left | No | Yes | Yes |
| 7 | Polyarticular | Left | No | Yes | Yes |
| Characteristic | Value |
|---|---|
| Sex 1 | |
| Male | 2 (28.6%) |
| Female | 5 (71.4%) |
| Age (years) 2 | 11.7 (2.7) |
| Body Mass Index 2 (kg/m2) | 17.7 (2.7) |
| JIA subtype 1 | |
| Oligoarticular JIA | 2 (28.6%) |
| Polyarticular JIA | 5 (71.4%) |
| Medical management at the time of recruitment 1 | |
| Ibuprofen | 1 (14.3%) |
| Methotrexate and Adalimumab | 1 (14.3%) |
| Ibuprofen and Hydroxychloroquine | 1 (14.3%) |
| None | 4 (57.1%) |
| Knee with active arthritis at the time of recruitment 1 | |
| Left knee | 3 (42.9%) |
| Right knee | 3 (42.9%) |
| None | 1 (14.3%) |
| Accelerometry Variable | Flexion-Extension | Walking | ||||
|---|---|---|---|---|---|---|
| Actively Inflamed Knee | Healthy Knee | PD (PAD) | Actively Inflamed Knee | Healthy Knee | PD (PAD) | |
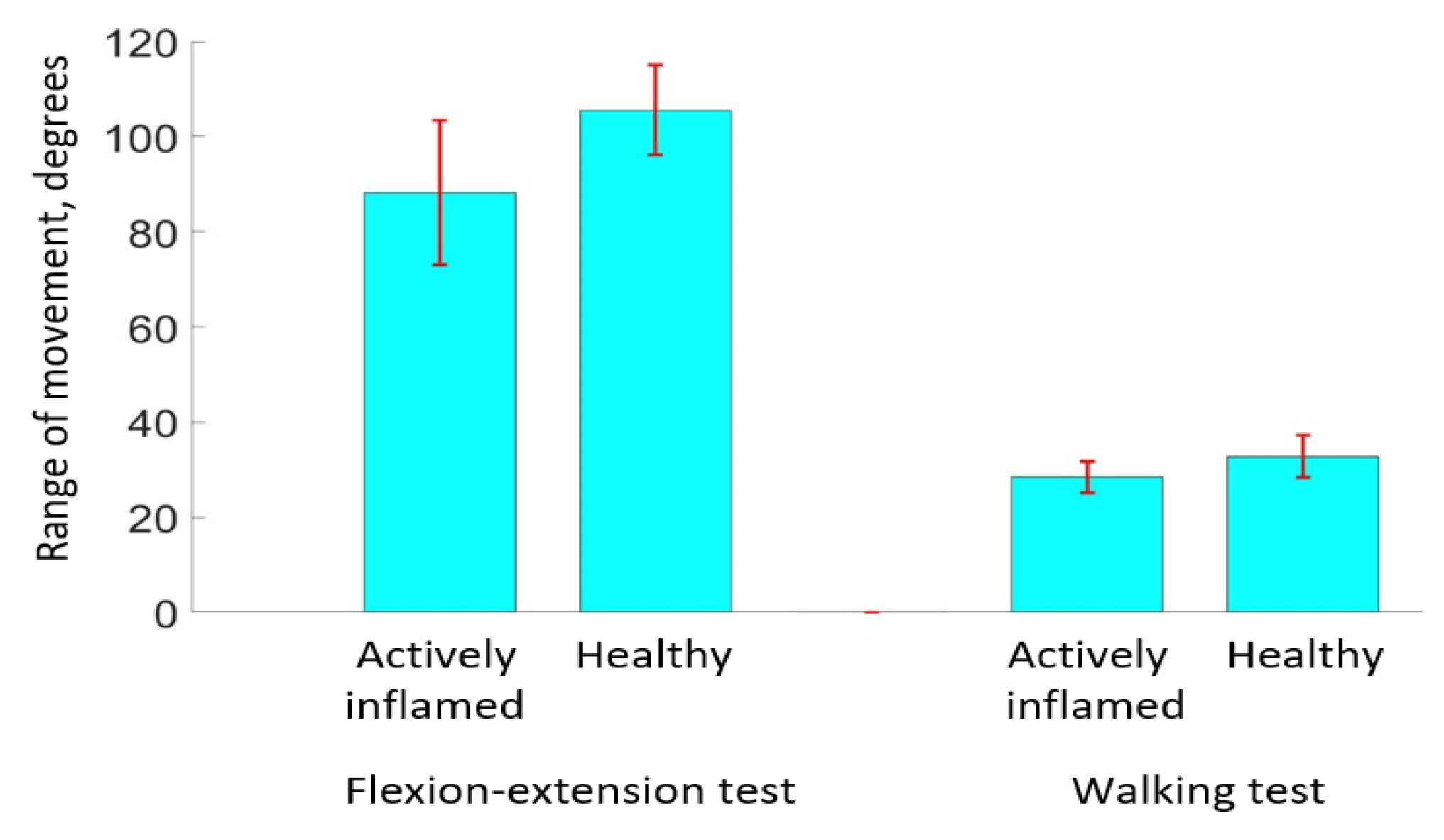
| Range of knee movement (degrees) 1 | 88.34 (16.63) | 105.59 (10.49) | 16.3% (17.8%) | 28.50 (3.62) | 32.76 (4.92) | 13.0% (13.9%) |
| Period of movement (s) 1 | 3.38 (0.75) | 3.32 (0.49) | −1.8% (1.8%) | 1.32 (0.21) | 1.33 (0.21) | 0.8% (0.8%) |
| Concordance with pGALS examination finding2 | ||||||
| Yes | 5 (83%) | 4 (67%) | ||||
| No | 1 (17%) | 2 (33%) | ||||
| Variable | Accelerometry Results | Significance | |
|---|---|---|---|
| Flexion-Extension | Walking | ||
| Range of movement (degrees) | Reduced in actively inflamed knees in 83.3% of cases (mean percentage difference 16.3%) | Reduced in actively inflamed knees in 83.3% of cases (mean percentage difference 13.0%) | Significant during flexion-extension (p-value = 0.032) Not significant during walking |
| Period of movement (seconds) | Greater in actively inflamed knees in 66.7% of cases (mean percentage difference 1.8%) | Similar in both knees in all cases (mean percentage difference 0.8%) | Not significant |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garner, A.J.; Saatchi, R.; Ward, O.; Nwaizu, H.; Hawley, D.P. Proof-of-Concept Study of the Use of Accelerometry to Quantify Knee Joint Movement and Assist with the Diagnosis of Juvenile Idiopathic Arthritis. Technologies 2022, 10, 76. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies10040076
Garner AJ, Saatchi R, Ward O, Nwaizu H, Hawley DP. Proof-of-Concept Study of the Use of Accelerometry to Quantify Knee Joint Movement and Assist with the Diagnosis of Juvenile Idiopathic Arthritis. Technologies. 2022; 10(4):76. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies10040076
Chicago/Turabian StyleGarner, Amelia Jane, Reza Saatchi, Oliver Ward, Harriet Nwaizu, and Daniel Philip Hawley. 2022. "Proof-of-Concept Study of the Use of Accelerometry to Quantify Knee Joint Movement and Assist with the Diagnosis of Juvenile Idiopathic Arthritis" Technologies 10, no. 4: 76. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies10040076