
Assessment of the Retromolar Canal in Taiwan Subpopulation: A Cross-Sectional Cone-Beam Computed Tomography Study in a Medical Center

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dental CBCT Examinations
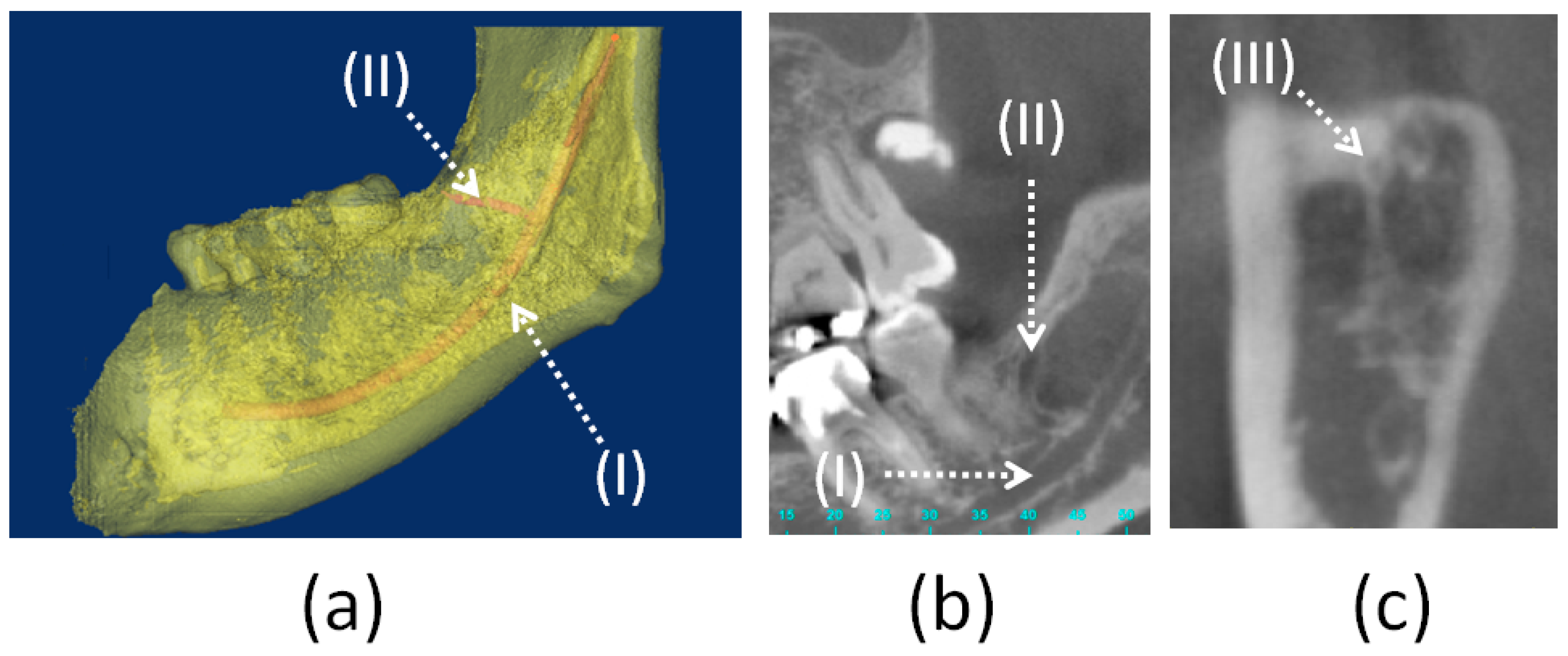
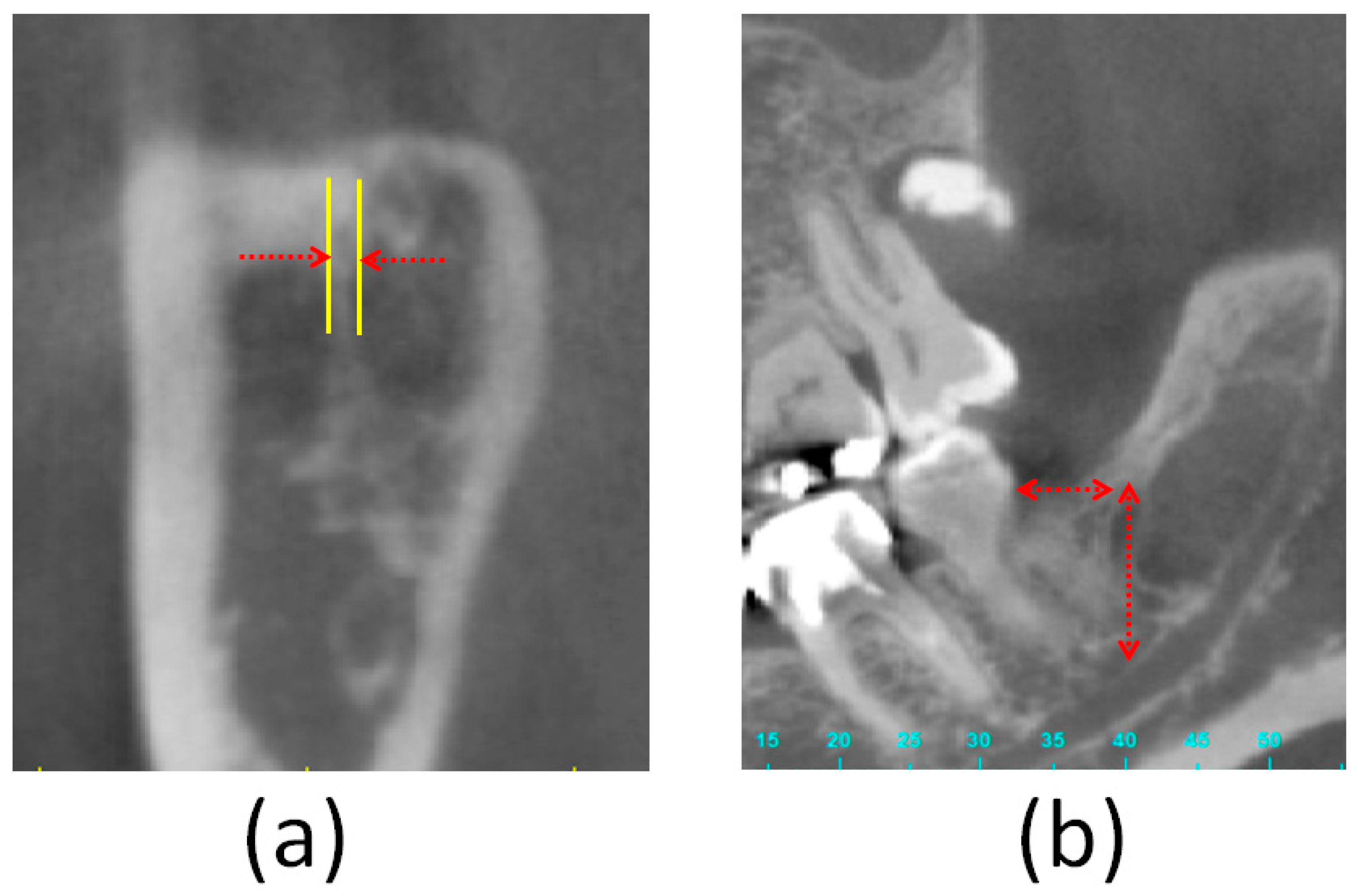
2.2. Measurement of the Prevalence of the Retromolar Canal and its Spatial Position in the Mandible
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cass, N. Book Review: Gray’s Anatomy—The Anatomical Basis of Clinical Practice, 39th ed.; SAGE Publications Sage: London, UK, 2005. [Google Scholar]
- Saravana, S.K. A study of the retromolar area and its clinical significance. Int. J. Pharma. Biosci. 2019, 10, 1–4. [Google Scholar]
- Ossenberg, N.S. Retromolar foramen of the human mandible. Am. J. Phys. Anthr. 1987, 73, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Chávez-Lomelí, M.; Lory, J.M.; Pompa, J.; Kjær, I. The Human Mandibular Canal Arises from Three Separate Canals Innervating Different Tooth Groups. J. Dent. Res. 1996, 75, 1540–1544. [Google Scholar] [CrossRef] [PubMed]
- Bilecenoglu, B.; Tuncer, N. Clinical and Anatomical Study of Retromolar Foramen and Canal. J. Oral Maxillofac. Surg. 2006, 64, 1493–1497. [Google Scholar] [CrossRef] [PubMed]
- Fukami, K.; Shiozaki, K.; Mishima, A.; Kuribayashi, A.; Hamada, Y.; Kobayashi, K. Bifid mandibular canal: Confirmation of limited cone beam CT findings by gross anatomical and histological investigations. Dentomaxillofac. Radiol. 2012, 41, 460–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyatt, W.M. Accessory mandibular canal: Literature review and presentation of an additional variant. Quintessence Int. 1996, 27, 27. [Google Scholar]
- Patil, S.; Matsuda, Y.; Nakajima, K.; Araki, K.; Okano, T. Retromolar canals as observed on cone-beam computed tomography: Their incidence, course, and characteristics. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 692–699. [Google Scholar] [CrossRef]
- Komarnitki, I.; Pliszka, H.; Roszkiewicz, P.; Chloupek, A. A morphological study of retromolar foramen and retromolar canal of modern and medieval population. Folia Morphol. 2020, 79, 580–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashsuren, O.; Choi, J.-W.; Han, W.-J.; Kim, E.-K. Assessment of bifid and trifid mandibular canals using cone-beam computed tomography. Imaging Sci. Dent. 2014, 44, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Galdames, I.S.; López, M.C.; Farias, B.L.; Urra, V.V.; Ramos, R.V. Morphometric study of the retromolar triangle. Int. J. Odontostomatol. 2007, 1, 129–132. [Google Scholar]
- Suazo, G.; Zavando, M.; Cantin, L. Retromolar Canal and Forame prevalence in dried mandibles and clinical implications. Int. J. Odontostomatol. 2008, 2, 183–187. [Google Scholar]
- Von Arx, T.; Hänni, A.; Sendi, P.; Buser, D.; Bornstein, M.M. Radiographic Study of the Mandibular Retromolar Canal: An Anatomic Structure with Clinical Importance. J. Endod. 2011, 37, 1630–1635. [Google Scholar] [CrossRef]
- Luangchana, P.; Pornprasertsuk-Damrongsri, S.; Kitisubkanchana, J.; Wongchuensoontorn, C. The retromolar canal and its variations: Classification using cone beam computed tomography. Quintessence Int. 2017, 49, 49. [Google Scholar]
- Özlem, O.; Dumlu, A. Prevalence of bifid mandibular canal according to gender, type and side. J. Dent. Sci. 2019, 14, 126–133. [Google Scholar] [CrossRef]
- Rabie, C.M.; Vranckx, M.; Rusque, M.; Deambrosi, C.; Ockerman, A.; Politis, C.; Jacobs, R. Anatomical relation of third molars and the retromolar canal. Br. J. Oral Maxillofac. Surg. 2019, 57, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Han, S.-S.; Park, C.-S. Cone beam CT findings of retromolar canals: Report of cases and literature review. Imaging Sci. Dent. 2013, 43, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Haas, L.F.; Dutra, K.; Porporatti, A.L.; Mezzomo, L.A.; Canto, G.D.L.; Flores-Mir, C.; Corrêa, M. Anatomical variations of mandibular canal detected by panoramic radiography and CT: A systematic review and meta-analysis. Dentomaxillofac. Radiol. 2016, 45, 20150310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orhan, K.; Aksoy, S.; Bilecenoglu, B.; Şakul, B.U.; Paksoy, C.S. Evaluation of bifid mandibular canals with cone-beam computed tomography in a Turkish adult population: A retrospective study. Surg. Radiol. Anat. 2010, 33, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Pyle, M.A.; Jasinevicius, T.R.; Lalumandier, J.A.; Kohrs, K.J.; Sawyer, D.R. Prevalence and implications of accessory retromolar foramina in clinical dentistry. Gen. Dent. 2000, 47, 500–503. [Google Scholar]
- Kodera, H.; Hashimoto, I. A case of mandibular retromolar canal: Elements of nerves and arteries in this canal. Anat. Sci. Int. 1995, 70, 23–30. [Google Scholar]
- Narayana, K.; Nayak, U.; Ahmed, W.; Bhat, J.; Devaiah, B. The retromolar foramen and canal in South Indian dry mandibles. Eur. J. Anat. 2020, 6, 141–146. [Google Scholar]
- Park, M.-K.; Jung, W.; Bae, J.-H.; Kwak, H.-H. Anatomical and radiographic study of the mandibular retromolar canal. J. Dent. Sci. 2016, 11, 370–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, F.M.S.; Cortez, A.L.V.; Moreira, R.W.F.; Mazzonetto, R. Complications of Intraoral Donor Site for Bone Grafting Prior to Implant Placement. Implant. Dent. 2006, 15, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Asaumi, R.; Sato, I.; Kumazawa, Y.; Yosue, T. Observation of the retromolar foramen and canal of the mandible: A CBCT and macroscopic study. Oral Radiol. 2011, 28, 10–14. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Number | Age | Which Side of Mandible | Diameter of Retromolar Foramen (mm) | Horizontal Distance from Retromolar Canal to Second Molar (mm) | Height of Retromolar Canal (mm) |
|---|---|---|---|---|---|
| Case 1 | 50~55 | Left | 1.56 | 13.89 | 12.86 |
| Case 2 | 45~50 | Right | 1.49 | 9.02 | 15.43 |
| Case 3 | 45~50 | Right | 1.14 | Missing tooth | 14.3 |
| Case 4 | 55~60 | Left | 1.57 | 8.01 | 12.83 |
| Case 5 | 20~25 | Left | 1.86 | 11.02 | 12.43 |
| Case 6 | 20~25 | Right | 1.01 | 11.58 | 15.25 |
| Case 7 | 40~45 | Right | 1.26 | 15.92 | 12.27 |
| 1.41 ± 0.30 | 11.57 ± 2.70 | 13.62 ± 1.34 |
| Researchers | Method (Sample Size) | Right Side (%) | Left Side (%) | |
|---|---|---|---|---|
| Ossenberg et al. [3] | Dry mandible (2500) | Old world | 60.0 | 25.7 |
| Bilateral: 14.3 | ||||
| New World | 25.9 | 40.5 | ||
| Bilateral: 33.5 | ||||
| Suazo et al. [12] | Dry mandible (294) | 4.8 | 4.4 | |
| Bilateral: 3.7 | ||||
| von Arx et al. [13] | CBCT (121) | 23.3 | 27.9 | |
| Orhan et al. [19] | CBCT (484) | 20.4 | 17.7 | |
| Park et al. [23] | Dry mandible (140) | 32.9 | 34.3 | |
| Narayana et al. [22] | Dry mandible (242) | 10.7 | 7.1 | |
| Bilateral: 4.1 | ||||
| This study | CBCT (68) | 11.4 | 9.1 | |
| Researcher | Measurement Approach | Population | Sample Size * | Percentage (%) | |
|---|---|---|---|---|---|
| Ossenberg et al. [3] | Dry mandible | Black Africans | 19 * | 0 | |
| Black Americans | 33 * | 0 | |||
| North American native peoples, prehistoric and present | North American native peoples | 99 * | 1.0 | ||
| Plain Indians | 435 * | 8.0 | |||
| Northern Indians | 178 * | 15.2 | |||
| Eskimo | 485 * | 8.2 | |||
| Aleut | 192 * | 15.1 | |||
| Canadian dissecting-room subjects | 11 * | 9.1 | |||
| India | 153 * | 5.9 | |||
| Italians, Siena | 86 * | 8.1 | |||
| Siberian native people | 167 * | 3.6 | |||
| Japanese | 94 * | 3.2 | |||
| Pyle et al. [20] | Dry mandible | Caucasian and African American | 475 * | 7.8 | |
| Suazo et al. [12] | Dry mandible | Brazilians | 294 * | 12.9 | |
| von Arx et al. [13] | CBCT | Not available | 121 (sides) | 25.6 | |
| Orhan et al. [19] | CBCT | Turkish | 242 * | 66.5 | |
| 484 (sides) | 46.5 | ||||
| Park et al. [23] | CBCT | Korean | 100 * | 11.5 | |
| Micro-computed tomography | Korean | 22 (sides) | 68.1 | ||
| Dry mandible | Korean | 140 (sides) | 33.6 | ||
| Narayana et al. [22] | Dry mandible | South Indian | 242 * | 21.9 | |
| This study | CBCT | Taiwanese | 68 (sides) | 10.3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, Y.-W.; Chang, W.-C.; Huang, H.-L.; Tsai, M.-T.; Fuh, L.-J.; Hsu, J.-T. Assessment of the Retromolar Canal in Taiwan Subpopulation: A Cross-Sectional Cone-Beam Computed Tomography Study in a Medical Center. Tomography 2021, 7, 219-227. https://0-doi-org.brum.beds.ac.uk/10.3390/tomography7020020
Shen Y-W, Chang W-C, Huang H-L, Tsai M-T, Fuh L-J, Hsu J-T. Assessment of the Retromolar Canal in Taiwan Subpopulation: A Cross-Sectional Cone-Beam Computed Tomography Study in a Medical Center. Tomography. 2021; 7(2):219-227. https://0-doi-org.brum.beds.ac.uk/10.3390/tomography7020020
Chicago/Turabian StyleShen, Yen-Wen, Wan-Chun Chang, Heng-Li Huang, Ming-Tzu Tsai, Lih-Jyh Fuh, and Jui-Ting Hsu. 2021. "Assessment of the Retromolar Canal in Taiwan Subpopulation: A Cross-Sectional Cone-Beam Computed Tomography Study in a Medical Center" Tomography 7, no. 2: 219-227. https://0-doi-org.brum.beds.ac.uk/10.3390/tomography7020020