
The Relationship between Metabolic Syndrome and Plasma Metals Modified by EGFR and TNF-α Gene Polymorphisms



Abstract
:1. Introduction
2. Materials and Methods
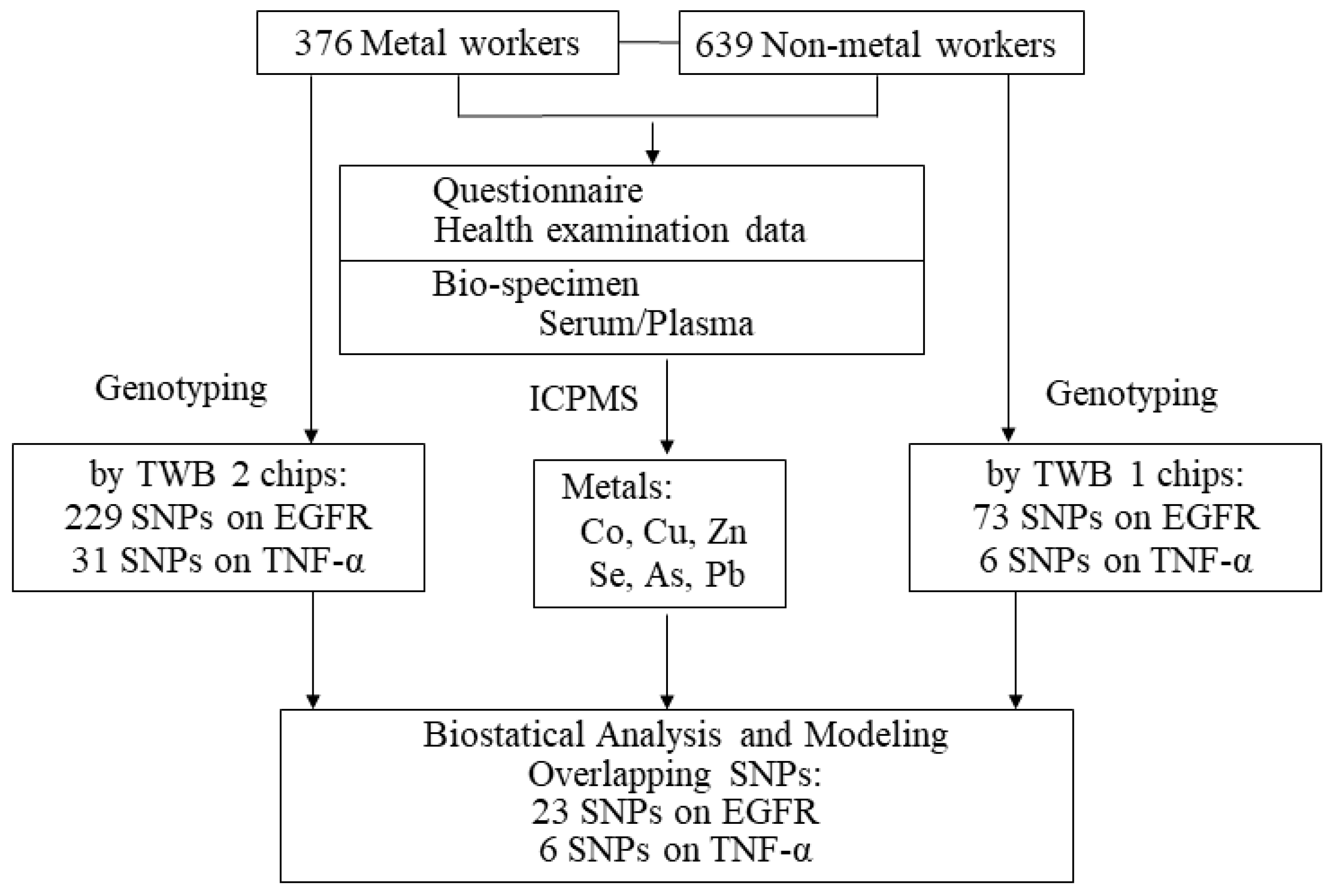
2.1. Study Population and Definition of Metabolic Syndrome
2.2. Analyses of Plasma Metals
2.3. Genotyping
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.W.; D’Agostino, R.B.; Parise, H.; Sullivan, L.; Meigs, J.B. Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus. Circulation 2005, 112, 3066–3072. [Google Scholar] [CrossRef] [PubMed]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [Green Version]
- Ranasinghe, P.; Mathangasinghe, Y.; Jayawardena, R.; Hills, A.P.; Misra, A. Prevalence and trends of metabolic syndrome among adults in the asia-pacific region: A systematic review. BMC Public Health 2017, 17, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.H.; Hsiao, H.P.; Chiu, Y.W.; Shih, N.H.; Chuang, H.Y.; Huang, C.T. Maternal diabetes or hypertension and lifestyle factors may be associated with metabolic syndrome: A population-based study in Taiwan. Kaohsiung J. Med. Sci. 2014, 30, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulka, C.M.; Persky, V.W.; Daviglus, M.L.; Durazo-Arvizu, R.A.; Argos, M. Multiple metal exposures and metabolic syndrome: A cross-sectional analysis of the National Health and Nutrition Examination Survey 2011–2014. Environ. Res. 2019, 168, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Wen, W.L.; Wang, C.W.; Wu, D.W.; Chen, S.C.; Hung, C.H.; Kuo, C.H. Associations of Heavy Metals with Metabolic Syndrome and Anthropometric Indices. Nutrients 2020, 12, 2666. [Google Scholar] [CrossRef]
- Rhee, S.Y.; Hwang, Y.C.; Woo, J.T.; Sinn, D.H.; Chin, S.O.; Chon, S.; Kim, Y.S. Blood lead is significantly associated with metabolic syndrome in Korean adults: An analysis based on the Korea National Health and Nutrition Examination Survey (KNHANES), 2008. Cardiovasc. Diabetol. 2013, 12, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panchal, S.K.; Wanyonyi, S.; Brown, L. Selenium, Vanadium, and Chromium as Micronutrients to Improve Metabolic Syndrome. Curr. Hypertens. Rep. 2017, 19, 10. [Google Scholar] [CrossRef]
- Rotter, I.; Kosik-Bogacka, D.; Dolegowska, B.; Safranow, K.; Lubkowska, A.; Laszczynska, M. Relationship between the concentrations of heavy metals and bioelements in aging men with metabolic syndrome. Int. J. Environ. Res. Public Health 2015, 12, 3944–3961. [Google Scholar] [CrossRef] [Green Version]
- Povel, C.M.; Boer, J.M.; Reiling, E.; Feskens, E.J. Genetic variants and the metabolic syndrome: A systematic review. Obes. Rev. 2011, 12, 952–967. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.E.; Walker, M. Genetics of Insulin Resistance and the Metabolic Syndrome. Curr. Cardiol. Rep. 2016, 18, 75. [Google Scholar] [CrossRef] [Green Version]
- Lin, E.; Kuo, P.H.; Liu, Y.L.; Yang, A.C.; Kao, C.F.; Tsai, S.J. Association and interaction of APOA5, BUD13, CETP, LIPA and health-related behavior with metabolic syndrome in a Taiwanese population. Sci. Rep. 2016, 6, 36830. [Google Scholar] [CrossRef] [Green Version]
- Schlessinger, J. Ligand-induced, receptor-mediated dimerization and activation of EGF receptor. Cell 2002, 110, 669–672. [Google Scholar] [CrossRef] [Green Version]
- Beltowski, J.; Lowicka, E. EGF receptor as a drug target in arterial hypertension. Mini Rev. Med. Chem. 2009, 9, 526–538. [Google Scholar] [CrossRef]
- Fernandez-Patron, C. Therapeutic potential of the epidermal growth factor receptor transactivation in hypertension: A convergent signaling pathway of vascular tone, oxidative stress, and hypertrophic growth downstream of vasoactive G-protein-coupled receptors? Can. J. Physiol. Pharmacol. 2007, 85, 97–104. [Google Scholar] [CrossRef]
- Scheving, L.A.; Zhang, X.; Garcia, O.A.; Wang, R.F.; Stevenson, M.C.; Threadgill, D.W.; Russell, W.E. Epidermal growth factor receptor plays a role in the regulation of liver and plasma lipid levels in adult male mice. Am. J. Physiol. Gastrointest. Liver Physiol. 2014, 306, G370–G381. [Google Scholar] [CrossRef] [Green Version]
- Choung, S.; Kim, J.M.; Joung, K.H.; Lee, E.S.; Kim, H.J.; Ku, B.J. Epidermal growth factor receptor inhibition attenuates non-alcoholic fatty liver disease in diet-induced obese mice. PLoS ONE 2019, 14, e0210828. [Google Scholar] [CrossRef]
- Bhushan, B.; Michalopoulos, G.K. Role of epidermal growth factor receptor in liver injury and lipid metabolism: Emerging new roles for an old receptor. Chem. Biol. Interact. 2020, 324, 109090. [Google Scholar] [CrossRef]
- Li, Z.; Li, Y.; Overstreet, J.M.; Chung, S.; Niu, A.; Fan, X.; Wang, S.; Wang, Y.; Zhang, M.Z.; Harris, R.C. Inhibition of Epidermal Growth Factor Receptor Activation Is Associated With Improved Diabetic Nephropathy and Insulin Resistance in Type 2 Diabetes. Diabetes 2018, 67, 1847–1857. [Google Scholar] [CrossRef] [Green Version]
- Moon, Y.S.; Kim, D.H.; Song, D.K. Serum tumor necrosis factor-alpha levels and components of the metabolic syndrome in obese adolescents. Metabolism 2004, 53, 863–867. [Google Scholar] [CrossRef]
- Kwaifa, I.K.; Bahari, H.; Yong, Y.K.; Noor, S.M. Endothelial Dysfunction in Obesity-Induced Inflammation: Molecular Mechanisms and Clinical Implications. Biomolecules 2020, 10, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borst, S.E. The role of TNF-alpha in insulin resistance. Endocrine 2004, 23, 177–182. [Google Scholar] [CrossRef]
- Srikanthan, K.; Feyh, A.; Visweshwar, H.; Shapiro, J.I.; Sodhi, K. Systematic Review of Metabolic Syndrome Biomarkers: A Panel for Early Detection, Management, and Risk Stratification in the West Virginian Population. Int. J. Med. Sci. 2016, 13, 25–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; He, L.; Zhang, X. -308G/A polymorphism of tumor necrosis factor alpha (TNF-alpha) gene and metabolic syndrome susceptibility: A meta-analysis. Sci. Rep. 2021, 11, 3840. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Delgado, F.; Alcala-Diaz, J.F.; Garcia-Rios, A.; Delgado-Lista, J.; Ortiz-Morales, A.; Rangel-Zuniga, O.; Tinahones, F.J.; Gonzalez-Guardia, L.; Malagon, M.M.; Bellido-Munoz, E.; et al. Polymorphism at the TNF-alpha gene interacts with Mediterranean diet to influence triglyceride metabolism and inflammation status in metabolic syndrome patients: From the CORDIOPREV clinical trial. Mol. Nutr. Food Res. 2014, 58, 1519–1527. [Google Scholar] [CrossRef]
- Tchounwou, P.B.; Yedjou, C.G.; Patlolla, A.K.; Sutton, D.J. Heavy metal toxicity and the environment. Exp. Suppl. 2012, 101, 133–164. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Zhou, Y.; Wang, D.; Guo, Y.; Wang, B.; Xu, Y.; Chen, W. Associations between essential metals exposure and metabolic syndrome (MetS): Exploring the mediating role of systemic inflammation in a general Chinese population. Environ. Int. 2020, 140, 105802. [Google Scholar] [CrossRef]
- Guo, X.; Yang, Q.; Zhang, W.; Chen, Y.; Ren, J.; Gao, A. Associations of blood levels of trace elements and heavy metals with metabolic syndrome in Chinese male adults with microRNA as mediators involved. Environ. Pollut. 2019, 248, 66–73. [Google Scholar] [CrossRef]
- Chen, C.H.; Yang, J.H.; Chiang, C.W.K.; Hsiung, C.N.; Wu, P.E.; Chang, L.C.; Chu, H.W.; Chang, J.; Song, I.W.; Yang, S.L.; et al. Population structure of Han Chinese in the modern Taiwanese population based on 10,000 participants in the Taiwan Biobank project. Hum. Mol. Genet. 2016, 25, 5321–5331. [Google Scholar] [CrossRef] [Green Version]
- Moy, F.M.; Bulgiba, A. The modified NCEP ATP III criteria maybe better than the IDF criteria in diagnosing Metabolic Syndrome among Malays in Kuala Lumpur. BMC Public Health 2010, 10, 678. [Google Scholar] [CrossRef] [Green Version]
- Hwang, L.C.; Bai, C.H.; Chen, C.J. Prevalence of obesity and metabolic syndrome in Taiwan. J Formos. Med. Assoc. 2006, 105, 626–635. [Google Scholar] [CrossRef] [Green Version]
- Taiwan Biobank. Available online: https://www.twbiobank.org.tw/new_web_en/index.php (accessed on 24 July 2021).
- Purcell, S.; Neale, B.; Todd-Brown, K.; Thomas, L.; Ferreira, M.A.; Bender, D.; Maller, J.; Sklar, P.; de Bakker, P.I.; Daly, M.J.; et al. PLINK: A tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 2007, 81, 559–575. [Google Scholar] [CrossRef] [Green Version]
- Anderson, C.A.; Pettersson, F.H.; Clarke, G.M.; Cardon, L.R.; Morris, A.P.; Zondervan, K.T. Data quality control in genetic case-control association studies. Nat. Protoc. 2010, 5, 1564–1573. [Google Scholar] [CrossRef] [Green Version]
- Wellcome Trust Case Control, C. Genome-wide association study of 14,000 cases of seven common diseases and 3,000 shared controls. Nature 2007, 447, 661–678. [Google Scholar] [CrossRef] [Green Version]
- Gaetke, L.M.; Chow, C.K. Copper toxicity, oxidative stress, and antioxidant nutrients. Toxicology 2003, 189, 147–163. [Google Scholar] [CrossRef]
- Frohlich, M.; Imhof, A.; Berg, G.; Hutchinson, W.L.; Pepys, M.B.; Boeing, H.; Muche, R.; Brenner, H.; Koenig, W. Association between C-reactive protein and features of the metabolic syndrome: A population-based study. Diabetes Care 2000, 23, 1835–1839. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.H.; Huang, J.J.; Kung, W.S.; Lee, S.S.; Sun, H.Y.; Chuang, H.Y. The Association of Serum TNF-alpha Levels and Blood Multi-Elements Modified by TNF-alpha Gene Polymorphisms in Metal Industrial Workers. Int. J. Environ. Res. Public Health 2019, 16, 4079. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.M.; Wu, M.J.; Lin, Y.H.; Chen, J. Association of epidermal growth factor receptor (EGFR) gene polymorphisms with endometriosis. Medicine 2019, 98, e15137. [Google Scholar] [CrossRef]
- Dong, L.M.; Brennan, P.; Karami, S.; Hung, R.J.; Menashe, I.; Berndt, S.I.; Yeager, M.; Chanock, S.; Zaridze, D.; Matveev, V.; et al. An analysis of growth, differentiation and apoptosis genes with risk of renal cancer. PLoS ONE 2009, 4, e4895. [Google Scholar] [CrossRef] [Green Version]
- Jou, Y.S.; Lo, Y.L.; Hsiao, C.F.; Chang, G.C.; Tsai, Y.H.; Su, W.C.; Chen, Y.M.; Huang, M.S.; Chen, H.L.; Chen, C.J.; et al. Association of an EGFR intron 1 SNP with never-smoking female lung adenocarcinoma patients. Lung Cancer 2009, 64, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Hajeer, A.H.; Hutchinson, I.V. Influence of TNFalpha gene polymorphisms on TNFalpha production and disease. Hum. Immunol. 2001, 62, 1191–1199. [Google Scholar] [CrossRef]
- Emara, M.; El-Edel, R.; Fathy, W.M.; Aboelkhair, N.T.; Watany, M.M.; Abou-Elela, D.H. Study the Association of Tumor Necrosis Factor Promoter Polymorphism with Type 2 Diabetic Nephropathy. Mediat. Inflamm. 2020, 2020, 1498278. [Google Scholar] [CrossRef]
- Gupta, S.; Mehndiratta, M.; Kalra, S.; Kalra, O.P.; Shukla, R.; Gambhir, J.K. Association of tumor necrosis factor (TNF) promoter polymorphisms with plasma TNF-alpha levels and susceptibility to diabetic nephropathy in North Indian population. J. Diabetes Complicat. 2015, 29, 338–342. [Google Scholar] [CrossRef]
- Daijo, K.; Nakahara, T.; Inagaki, Y.; Nanba, M.; Nishida, Y.; Uchikawa, S.; Kodama, K.; Oya, K.; Morio, K.; Fujino, H.; et al. Risk factors for histological progression of non-alcoholic steatohepatitis analyzed from repeated biopsy cases. J. Gastroenterol. Hepatol. 2020, 35, 1412–1419. [Google Scholar] [CrossRef]
- Catalani, S.; Leone, R.; Rizzetti, M.C.; Padovani, A.; Apostoli, P. The role of albumin in human toxicology of cobalt: Contribution from a clinical case. ISRN Hematol. 2011, 2011, 690620. [Google Scholar] [CrossRef] [Green Version]
- Hess, S.Y.; Peerson, J.M.; King, J.C.; Brown, K.H. Use of serum zinc concentration as an indicator of population zinc status. Food Nutr. Bull. 2007, 28, S403–S429. [Google Scholar] [CrossRef]
- Alfthan, G.; Neve, J. Reference values for serum selenium in various areas-evaluated according to the TRACY protocol. J. Trace Elem. Med. Biol. 1996, 10, 77–87. [Google Scholar] [CrossRef]
- Yue, X.; Jiang, X.; Zou, H.; Li, G.; Wang, J.; Liu, Y. Association of hepatocellular carcinoma risk with polymorphisms in tumour necrosis factor alpha gene in a Chinese Han population. Int. J. Immunogenet. 2020, 47, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Fabris, M.; Di Poi, E.; D’Elia, A.; Damante, G.; Sinigaglia, L.; Ferraccioli, G. Tumor necrosis factor-alpha gene polymorphism in severe and mild-moderate rheumatoid arthritis. J. Rheumatol. 2002, 29, 29–33. [Google Scholar] [PubMed]
- Matys, T.; Szymanska-Chabowska, A.; Bogunia-Kubik, K.; Smyk, B.; Kaminska, M.; Mazur, G.; Poreba, R.; Gac, P. The Relationship Between Selected CNR1, MC4R, LEP, FTO and VDR Gene Polymorphisms and Several Basic Toxicological Parameters Among Persons Occupationally Exposed to Arsenic, Cadmium and Lead. J. Clin. Med. 2020, 9, 1040. [Google Scholar] [CrossRef] [Green Version]
- Li, C.Y.; Sung, F.C. A review of the healthy worker effect in occupational epidemiology. Occup. Med. 1999, 49, 225–229. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.D.; Chang, C.H.; Tai, T.Y.; Chen, J.F.; Chuang, L.M. Incidence and prevalence rates of diabetes mellitus in Taiwan: Analysis of the 2000–2009 Nationwide Health Insurance database. J. Formos. Med. Assoc. 2012, 111, 599–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total n = 1015 | Non-MetS n = 834 | MetS n = 181 | p Value |
|---|---|---|---|---|
| Worker group | <0.001 | |||
| Metal workers | 376 (37.0) | 276 (33.1) | 100 (55.2) | |
| Non-metal workers | 639 (63.0) | 558 (66.9) | 81 (44.8) | |
| Gender | <0.001 | |||
| Male | 520 (51.2) | 402 (48.2) | 118 (65.2) | |
| Female | 495 (48.8) | 432 (51.8) | 63 (34.8) | |
| Smoking | 213 (21.0) | 150 (18.0) | 63 (34.8) | <0.001 |
| Drinking alcohol | 37 (3.7) | 27 (3.3) | 10 (5.7) | 0.096 |
| Age (year) | 43.76 ± 10.11 | 43.25 ± 10.07 | 46.07 ± 9.98 | 0.001 |
| BMI (kg/m2) | 24.41 ± 3.96 | 23.62 ± 3.33 | 28.09 ± 4.51 | <0.001 |
| WC (cm) | 81.72 ± 11.19 | 79.47 ± 9.88 | 92.20 ± 11.01 | <0.001 |
| SBP (mmHg) | 117.98 ± 16.68 | 115.52 ± 15.55 | 129.29 ± 17.07 | <0.001 |
| DBP (mmHg) | 72.19 ± 11.45 | 70.84 ± 10.97 | 78.41 ± 11.60 | <0.001 |
| Sugar (mg/dL) | 94.52 ± 25.39 | 90.58 ± 15.01 | 112.68 ± 46.74 | <0.001 |
| TG (mg/dL) | 126.55 ± 117.25 | 101.38 ± 62.14 | 242.55 ± 207.63 | <0.001 |
| HDL-C (mg/dL) | 51.59 ± 13.91 | 54.30 ± 13.15 | 39.10 ± 9.93 | <0.001 |
| TC (mg/dL) | 202.24 ± 37.33 | 200.00 ± 36.39 | 212.59 ± 39.87 | <0.001 |
| Uric acid (mg/dL) | 5.76 ± 1.55 | 5.59 ± 1.49 | 6.47 ± 1.58 | <0.001 |
| ALT (IU/L) | 26.16 ± 19.63 | 24.05 ± 18.49 | 35.90 ± 21.77 | <0.001 |
| Creatinine (mg/dL) | 0.77 ± 0.18 | 0.77 ± 0.18 | 0.81 ± 0.17 | 0.003 |
| Co (μg/L) | 0.85 ± 0.29 | 0.85 ± 0.30 | 0.87 ± 0.25 | 0.286 |
| Cu (μg/L) | 1001.97 ± 270.83 | 992.99 ± 270.19 | 1043.74 ± 270.63 | 0.023 |
| Zn (μg/L) | 849.68 ± 275.77 | 840.16 ± 277.27 | 893.98 ± 264.95 | 0.018 |
| Se (μg/L) | 207.54 ± 107.33 | 198.82 ± 102.99 | 247.69 ± 117.62 | <0.001 |
| As (μg/L) | 6.07 ± 8.07 | 5.99 ± 8.63 | 6.47 ± 4.65 | 0.463 |
| Pb (μg/L) | 0.33 ± 0.52 | 0.30 ± 0.49 | 0.48 ± 0.63 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, T.-H.; Kung, W.-S.; Sun, H.-Y.; Huang, J.-J.; Lu, J.-Y.; Luo, K.-H.; Chuang, H.-Y. The Relationship between Metabolic Syndrome and Plasma Metals Modified by EGFR and TNF-α Gene Polymorphisms. Toxics 2021, 9, 225. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9090225
Chen T-H, Kung W-S, Sun H-Y, Huang J-J, Lu J-Y, Luo K-H, Chuang H-Y. The Relationship between Metabolic Syndrome and Plasma Metals Modified by EGFR and TNF-α Gene Polymorphisms. Toxics. 2021; 9(9):225. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9090225
Chicago/Turabian StyleChen, Tzu-Hua, Wei-Shyang Kung, Hung-Yu Sun, Joh-Jong Huang, Jia-Yi Lu, Kuei-Hau Luo, and Hung-Yi Chuang. 2021. "The Relationship between Metabolic Syndrome and Plasma Metals Modified by EGFR and TNF-α Gene Polymorphisms" Toxics 9, no. 9: 225. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9090225