
Spatially and Temporally Resolved Ambient PM2.5 in Relation to Preterm Birth

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
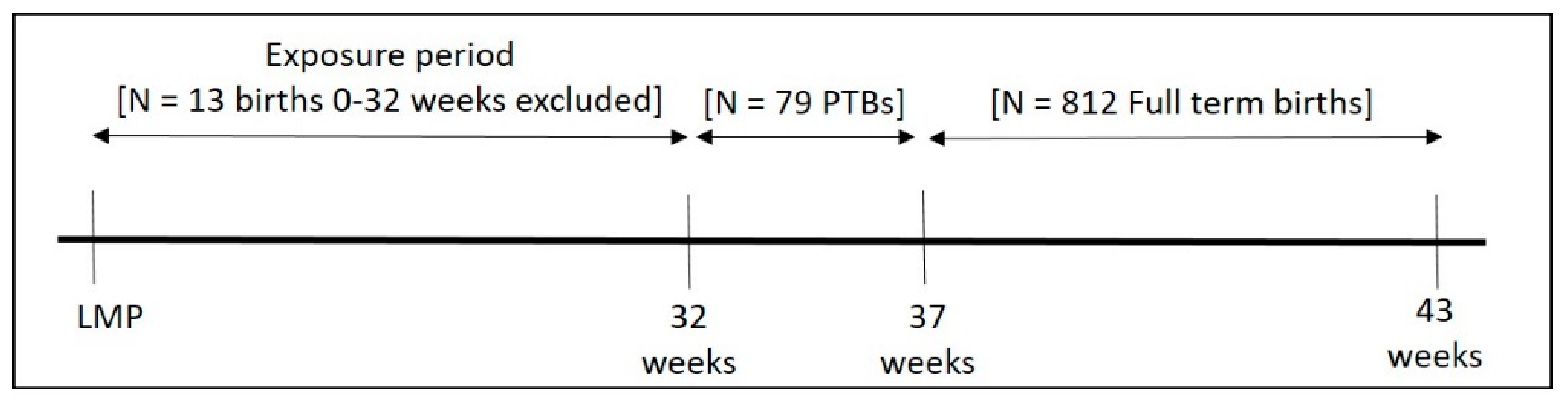
2.1. Study Sample
2.2. Fine Particulate Matter Exposure
2.3. Gestational Age at Birth
2.4. Covariates
2.5. Statistical Analysis
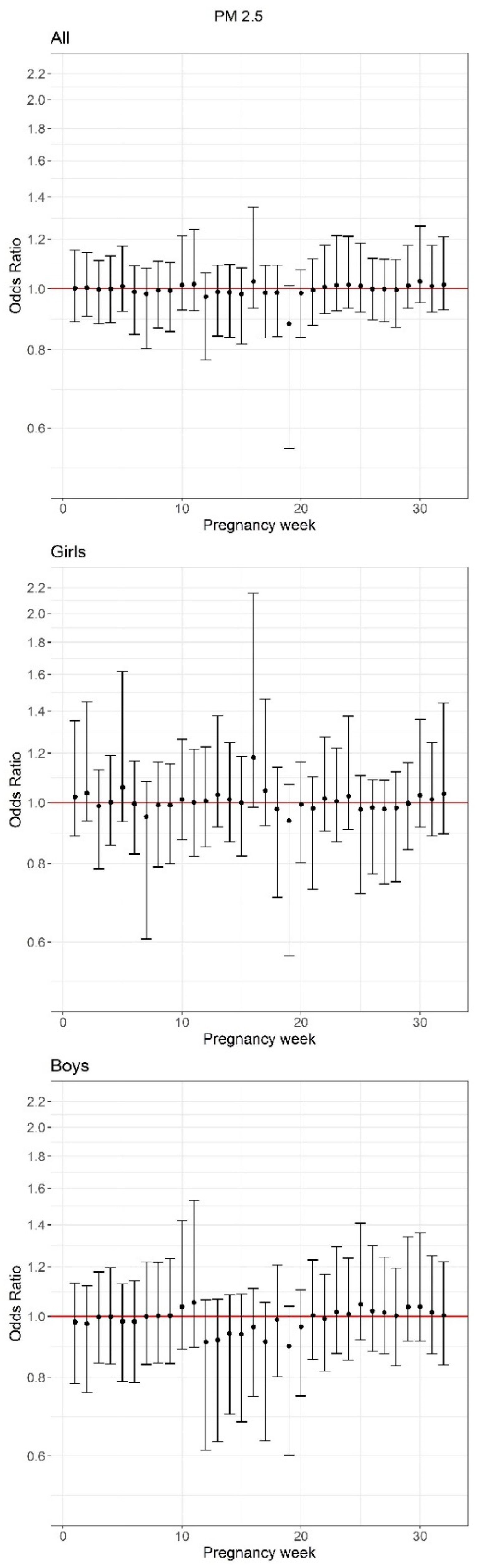
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K. Births: Final Data for 2019; National Vital Statistics Reports; National Center for Health Statistics: Hyattsville, MD, USA, 2021; Volume 70. [Google Scholar]
- Crump, C.; Sundquist, J.; Winkleby, M.A.; Sundquist, K. Gestational age at birth and mortality from infancy into mid-adulthood: A national cohort study. Lancet Child Adolesc. Health 2019, 3, 408–417. [Google Scholar] [CrossRef]
- Markopoulou, P.; Papanikolaou, E.; Analytis, A.; Zoumakis, E.; Siahanidou, T. Preterm Birth as a Risk Factor for Metabolic Syndrome and Cardiovascular Disease in Adult Life: A Systematic Review and Meta-Analysis. J. Pediatr. 2019, 210, 69–80. [Google Scholar] [CrossRef]
- Moster, D.; Lie, R.T.; Markestad, T. Long-term medical and social consequences of preterm birth. N. Engl. J. Med. 2008, 359, 262–273. [Google Scholar] [CrossRef] [Green Version]
- Petrou, S.; Eddama, O.; Mangham-Jefferies, L. A structured review of the recent literature on the economic consequences of preterm birth. Arch. Dis. Child.-Fetal Neonatal Ed. 2010, 96, F225–F232. [Google Scholar] [CrossRef]
- Klepac, P.; Locatelli, I.; Korošec, S.; Künzli, N.; Kukec, A. Ambient air pollution and pregnancy outcomes: A comprehensive review and identification of environmental public health challenges. Environ. Res. 2018, 167, 144–159. [Google Scholar] [CrossRef] [PubMed]
- Stieb, D.M.; Chen, L.; Eshoul, M.; Judek, S. Ambient air pollution, birth weight and preterm birth: A systematic review and meta-analysis. Environ. Res. 2012, 117, 100–111. [Google Scholar] [CrossRef]
- Wilson, A.; Chiu, Y.-H.M.; Hsu, H.-H.L.; Wright, R.; Wright, R.J.; Coull, B.A. Bayesian distributed lag interaction models to identify perinatal windows of vulnerability in children’s health. Biostatistics 2017, 18, 537–552. [Google Scholar] [CrossRef] [Green Version]
- Wright, R. Environment, susceptibility windows, development, and child health. Curr. Opin. Pediatr. 2017, 29, 211–217. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.H.; Warren, J.L.; Darrow, L.A.; Reich, B.J.; Waller, L.A. Assessment of critical exposure and outcome windows in time-to-event analysis with application to air pollution and preterm birth study. Biostatistics 2015, 16, 509–521. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Benmarhnia, T.; Zhang, H.; Knibbs, L.D.; Sheridan, P.; Li, C.; Bao, J.; Ren, M.; Wang, S.; He, Y.; et al. Identifying windows of susceptibility for maternal exposure to ambient air pollution and preterm birth. Environ. Int. 2018, 121, 317–324. [Google Scholar] [CrossRef]
- Warren, J.; Fuentes, M.; Herring, A.; Langlois, P. Spatial-Temporal Modeling of the Association between Air Pollution Exposure and Preterm Birth: Identifying Critical Windows of Exposure. Biometrics 2012, 68, 1157–1167. [Google Scholar] [CrossRef] [Green Version]
- Chu, C.; Zhu, Y.; Liu, C.; Chen, R.; Yan, Y.; Ren, Y.; Li, X.; Wang, J.; Ge, W.; Kan, H.; et al. Ambient fine particulate matter air pollution and the risk of preterm birth: A multicenter birth cohort study in China. Environ. Pollut. 2021, 287, 117629. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Xu, J.; Chen, D.; Sun, P.; Ma, X. The association between air pollution and preterm birth and low birth weight in Guangdong, China. BMC Public Health 2019, 19, 3. [Google Scholar] [CrossRef]
- Inkster, A.; Fernández-Boyano, I.; Robinson, W. Sex Differences Are Here to Stay: Relevance to Prenatal Care. J. Clin. Med. 2021, 10, 3000. [Google Scholar] [CrossRef]
- Ghosh, R.; Rankin, J.; Pless-Mulloli, T.; Glinianaia, S. Does the effect of air pollution on pregnancy outcomes differ by gender? A systematic review. Environ. Res. 2007, 105, 400–408. [Google Scholar] [CrossRef]
- Brunst, K.J.; Sanchez-Guerra, M.; Chiu, Y.-H.M.; Wilson, A.; Coull, B.A.; Kloog, I.; Schwartz, J.; Brennan, K.J.; Enlow, M.B.; Wright, R.O.; et al. Prenatal particulate matter exposure and mitochondrial dysfunction at the maternal-fetal interface: Effect modification by maternal lifetime trauma and child sex. Environ. Int. 2018, 112, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Just, A.C.; Arfer, K.B.; Rush, J.; Dorman, M.; Shtein, A.; Lyapustin, A.; Kloog, I. Advancing methodologies for applying machine learning and evaluating spatiotemporal models of fine particulate matter (PM2.5) using satellite data over large regions. Atmos. Environ. 2020, 239, 117649. [Google Scholar] [CrossRef]
- Carrión, D.; Arfer, K.B.; Rush, J.; Dorman, M.; Rowland, S.T.; Kioumourtzoglou, M.-A.; Kloog, I.; Just, A.C. A 1-km hourly air-temperature model for 13 northeastern U.S. states using remotely sensed and ground-based measurements. Environ. Res. 2021, 200, 111477. [Google Scholar] [CrossRef] [PubMed]
- Ada, M.L.; Hacker, M.R.; Golen, T.H.; Haviland, M.; Shainker, S.A.; Burris, H.H. Trends in provider-initiated versus spontaneous preterm deliveries, 2004–2013. J. Perinatol. 2017, 37, 1187–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Textor, J.; van der Zander, B.; Gilthorpe, M.S.; Liśkiewicz, M.; Ellison, G.T. Robust causal inference using directed acyclic graphs: The R package ‘dagitty’. Int. J. Epidemiol. 2017, 45, 1887–1894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloog, I. Air pollution, ambient temperature, green space and preterm birth. Curr. Opin. Pediatr. 2019, 31, 237–243. [Google Scholar] [CrossRef]
- Warren, J.L.; Kong, W.; Luben, T.; Chang, H.H. Critical window variable selection: Estimating the impact of air pollution on very preterm birth. Biostatistics 2019, 21, 790–806. [Google Scholar] [CrossRef]
- Gehring, U.; Wijga, A.H.; Fischer, P.; de Jongste, J.C.; Kerkhof, M.; Koppelman, G.H.; Smit, H.A.; Brunekreef, B. Traffic-related air pollution, preterm birth and term birth weight in the PIAMA birth cohort study. Environ. Res. 2011, 111, 125–135. [Google Scholar] [CrossRef]
- Hannam, K.; McNamee, R.; Baker, P.; Sibley, C.; Agius, R. Air pollution exposure and adverse pregnancy outcomes in a large UK birth cohort: Use of a novel spatio-temporal modelling technique. Scand. J. Work. Environ. Health 2014, 40, 518–530. [Google Scholar] [CrossRef] [Green Version]
- Lavigne, E.; Yasseen, A.S.; Stieb, D.M.; Hystad, P.; van Donkelaar, A.; Martin, R.; Brook, J.R.; Crouse, D.; Burnett, R.T.; Chen, H.; et al. Ambient air pollution and adverse birth outcomes: Differences by maternal comorbidities. Environ. Res. 2016, 148, 457–466. [Google Scholar] [CrossRef] [Green Version]
- Pereira, G.; Bell, M.L.; Lee, H.J.; Koutrakis, P.; Belanger, K. Sources of Fine Particulate Matter and Risk of Preterm Birth in Connecticut, 2000–2006: A Longitudinal Study. Environ. Health Perspect. 2014, 122, 1117–1122. [Google Scholar] [CrossRef] [Green Version]
- Qian, Z.; Liang, S.; Yang, S.; Trevathan, E.; Huang, Z.; Yang, R.; Wang, J.; Hu, K.; Zhang, Y.; Vaughn, M.; et al. Ambient air pollution and preterm birth: A prospective birth cohort study in Wuhan, China. Int. J. Hyg. Environ. Health 2016, 219, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Ren, C.; Delfino, R.J.; Chung, J.; Wilhelm, M.; Ritz, B. Association between Local Traffic-Generated Air Pollution and Preeclampsia and Preterm Delivery in the South Coast Air Basin of California. Environ. Health Perspect. 2009, 117, 1773–1779. [Google Scholar] [CrossRef]
- Tanner, J.P.; Salemi, J.L.; Stuart, A.L.; Yu, H.; Jordan, M.M.; Duclos, C.; Cavicchia, P.; Correia, J.A.; Watkins, S.M.; Kirby, R.S. Uncertainty in maternal exposures to ambient PM2.5 and benzene during pregnancy: Sensitivity to exposure estimation decisions. Spat. Spatio-Temporal Epidemiol. 2016, 17, 117–129. [Google Scholar] [CrossRef]
- Rappazzo, K.M.; Daniels, J.L.; Messer, L.C.; Poole, C.; Lobdell, D. Exposure to Fine Particulate Matter during Pregnancy and Risk of Preterm Birth among Women in New Jersey, Ohio, and Pennsylvania, 2000–2005. Environ. Health Perspect. 2014, 122, 992–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Symanski, E.; Davila, M.; McHugh, M.K.; Waller, D.K.; Zhang, X.; Lai, D. Maternal Exposure to Fine Particulate Pollution During Narrow Gestational Periods and Newborn Health in Harris County, Texas. Matern. Child Health J. 2014, 18, 2003–2012. [Google Scholar] [CrossRef] [Green Version]
- Yuan, L.; Zhang, Y.; Wang, W.; Chen, R.; Liu, Y.; Liu, C.; Kan, H.; Gao, Y.; Tian, Y. Critical windows for maternal fine particulate matter exposure and adverse birth outcomes: The Shanghai birth cohort study. Chemosphere 2020, 240, 124904. [Google Scholar] [CrossRef]
- Sheridan, P.; Ilango, S.; Bruckner, T.A.; Wang, Q.; Basu, R.; Benmarhnia, T. Ambient Fine Particulate Matter and Preterm Birth in California: Identification of Critical Exposure Windows. Am. J. Epidemiol. 2019, 188, 1608–1615. [Google Scholar] [CrossRef]
- Altman, M.R.; Baer, R.J.; Jelliffe-Pawlowski, L.L. Patterns of Preterm Birth among Women of Native Hawaiian and Pacific Islander Descent. Am. J. Perinatol. 2018, 36, 1256–1263. [Google Scholar] [CrossRef]
- Darrow, L.A.; Klein, M.; Flanders, W.D.; Waller, L.A.; Correa, A.; Marcus, M.; Mulholland, J.A.; Russell, A.G.; Tolbert, P.E. Ambient air pollution and preterm birth: A time-series analysis. Epidemiology 2009, 20, 689–698. [Google Scholar] [CrossRef] [Green Version]
- Jalaludin, B.; Mannes, T.; Morgan, G.; Lincoln, D.; Sheppeard, V.; Corbett, S. Impact of ambient air pollution on gestational age is modified by season in Sydney, Australia. Environ. Health 2007, 6, 16. [Google Scholar] [CrossRef] [Green Version]
- Wilhelm, M.; Ghosh, J.K.; Su, J.; Cockburn, M.; Jerrett, M.; Ritz, B. Traffic-related air toxics and preterm birth: A population-based case-control study in Los Angeles county, California. Environ. Health 2011, 10, 89. [Google Scholar] [CrossRef] [Green Version]
- Wilhelm, M.; Ritz, B. Local Variations in CO and Particulate Air Pollution and Adverse Birth Outcomes in Los Angeles County, California, USA. Environ. Health Perspect. 2005, 113, 1212–1221. [Google Scholar] [CrossRef] [Green Version]
- Blum, J.L.; Chen, L.-C.; Zelikoff, J.T. Exposure to Ambient Particulate Matter during Specific Gestational Periods Produces Adverse Obstetric Consequences in Mice. Environ. Health Perspect. 2017, 125, 77020. [Google Scholar] [CrossRef] [Green Version]
- Veras, M.M.; Damaceno-Rodrigues, N.R.; Caldini, E.; Ribeiro, A.A.C.M.; Mayhew, T.M.; Saldiva, P.; Dolhnikoff, M. Particulate Urban Air Pollution Affects the Functional Morphology of Mouse Placenta1. Biol. Reprod. 2008, 79, 578–584. [Google Scholar] [CrossRef] [Green Version]
- Nääv, Å.; Erlandsson, L.; Isaxon, C.; Frostner, E.Å.; Ehinger, J.; Sporre, M.; Krais, A.M.; Strandberg, B.; Lundh, T.; Elmér, E.; et al. Urban PM2.5 Induces Cellular Toxicity, Hormone Dysregulation, Oxidative Damage, Inflammation, and Mitochondrial Interference in the HRT8 Trophoblast Cell Line. Front. Endocrinol. 2020, 11, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, E.Y.; Patterson, P.H. Activation of the maternal immune system induces endocrine changes in the placenta via IL-6. Brain Behav. Immun. 2011, 25, 604–615. [Google Scholar] [CrossRef] [Green Version]
- Keenan-Devlin, L.S.; Caplan, M.; Freedman, A.; Kuchta, K.; Grobman, W.; Buss, C.; Adam, E.K.; Entringer, S.; Miller, G.E.; Borders, A.E.B. Using principle component analysis to examine associations of early pregnancy inflammatory biomarker profiles and adverse birth outcomes. Am. J. Reprod. Immunol. 2021, 86, e13497. [Google Scholar] [CrossRef]
- Braun, D.A.; Ishii, Y.; Walsh, A.; Van Allen, E.M.; Wu, C.J.; Shukla, S.A.; Choueiri, T.K. Clinical Validation of PBRM1 Alterations as a Marker of Immune Checkpoint Inhibitor Response in Renal Cell Carcinoma. JAMA Oncol. 2019, 5, 1631–1633. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All (n = 891, 100%) | Preterm (n = 79, 8.9%) | Term (n = 812, 91.1%) | |
|---|---|---|---|
| Maternal age | 29.1 ± 5.8 | 30.4 ± 6.0 | 28.9 ± 5.8 |
| Race/ethnicity | |||
| White, non-Hispanic | 147 (16.5) | 9 (6.1) | 138 (93.9) |
| White-Hispanic | 317 (35.6) | 33 (10.4) | 284 (89.6) |
| Black/Black-Hispanic | 385 (43.2) | 35 (9.1) | 350 (90.9) |
| Other | 42 (4.7) | 2 (4.8) | 40 (95.2) |
| Education | |||
| <High school | 183 (20.5) | 20 (10.9) | 163 (89.1) |
| High school degree | 444 (49.8) | 39 (8.8) | 405 (91.2) |
| >High school | 264 (29.6) | 20 (7.6) | 244 (92.4) |
| Parity | |||
| Nulliparous | 303 (34.0) | 16 (5.3) | 287 (94.7) |
| Multiparous | 588 (66.0) | 63 (10.7) | 525 (89.3) |
| Smoke exposure a | |||
| Yes | 100 (11.2) | 11 (11.0) | 89 (89.0) |
| No | 791 (88.8) | 68 (8.6) | 723 (91.4) |
| PM2.5 (µg/m3) b | 8.13 (1.10) | 8.12 (1.11) | 8.13 (1.10) |
| Temperature (C) b | 12.10 (4.31) | 12.50 (4.16) | 12.10 (4.33) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cowell, W.; Colicino, E.; Zhang, X.; Ledyard, R.; Burris, H.H.; Hacker, M.R.; Kloog, I.; Just, A.; Wright, R.O.; Wright, R.J. Spatially and Temporally Resolved Ambient PM2.5 in Relation to Preterm Birth. Toxics 2021, 9, 352. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9120352
Cowell W, Colicino E, Zhang X, Ledyard R, Burris HH, Hacker MR, Kloog I, Just A, Wright RO, Wright RJ. Spatially and Temporally Resolved Ambient PM2.5 in Relation to Preterm Birth. Toxics. 2021; 9(12):352. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9120352
Chicago/Turabian StyleCowell, Whitney, Elena Colicino, Xueying Zhang, Rachel Ledyard, Heather H. Burris, Michele R. Hacker, Itai Kloog, Allan Just, Robert O. Wright, and Rosalind J. Wright. 2021. "Spatially and Temporally Resolved Ambient PM2.5 in Relation to Preterm Birth" Toxics 9, no. 12: 352. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9120352