Botulinum Toxin a Valuable Prophylactic Agent for Migraines and a Possible Future Option for the Prevention of Hormonal Variations-Triggered Migraines

 ,
,
Abstract
:1. Introduction
2. Material and Methods
3. Mechanism of Migraine Development
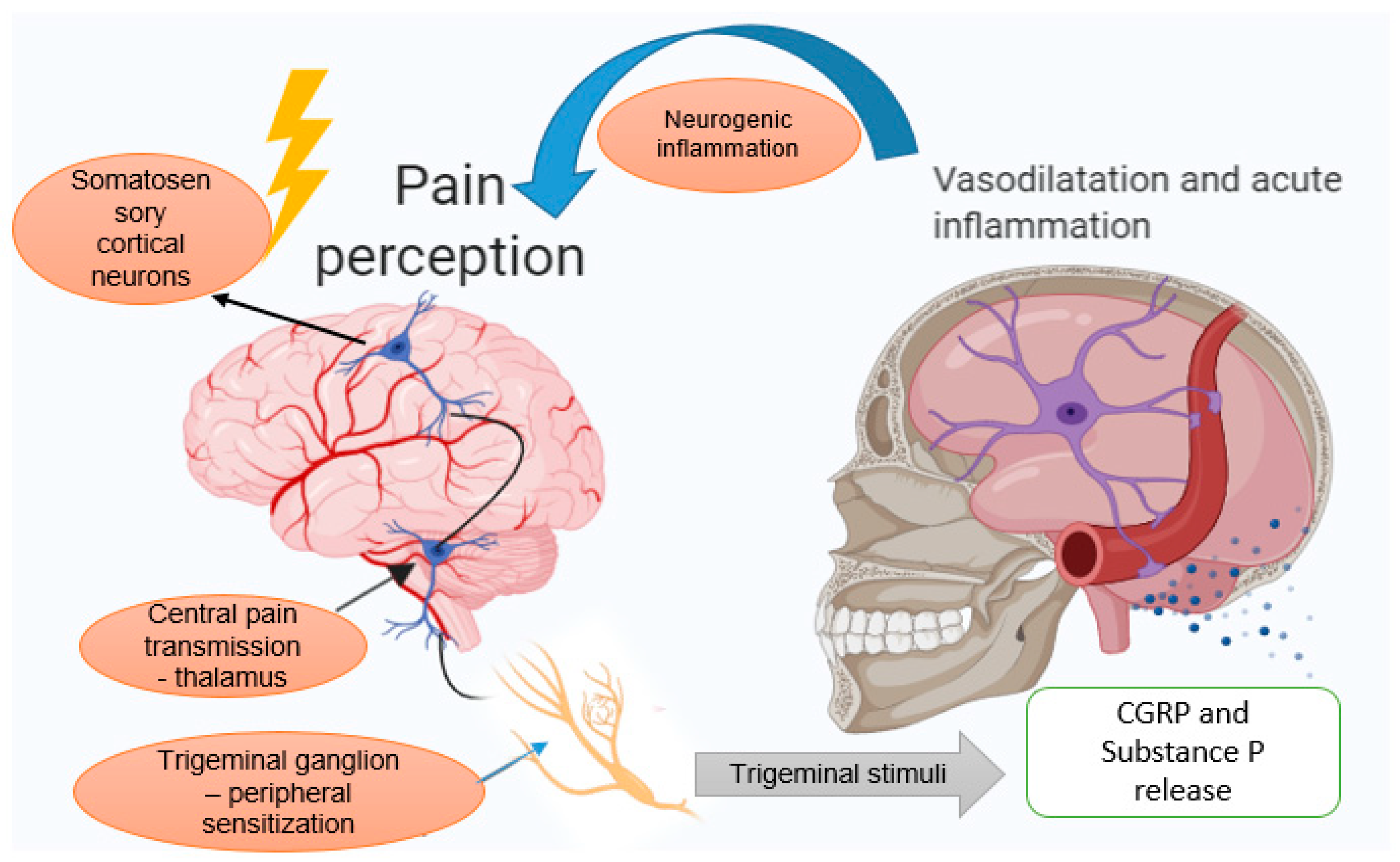
3.1. The Trigeminovascular System
3.2. Neurogenic Inflammation Theory
4. Migraine Induced by Hormonal Variations
5. Botulinum Toxin
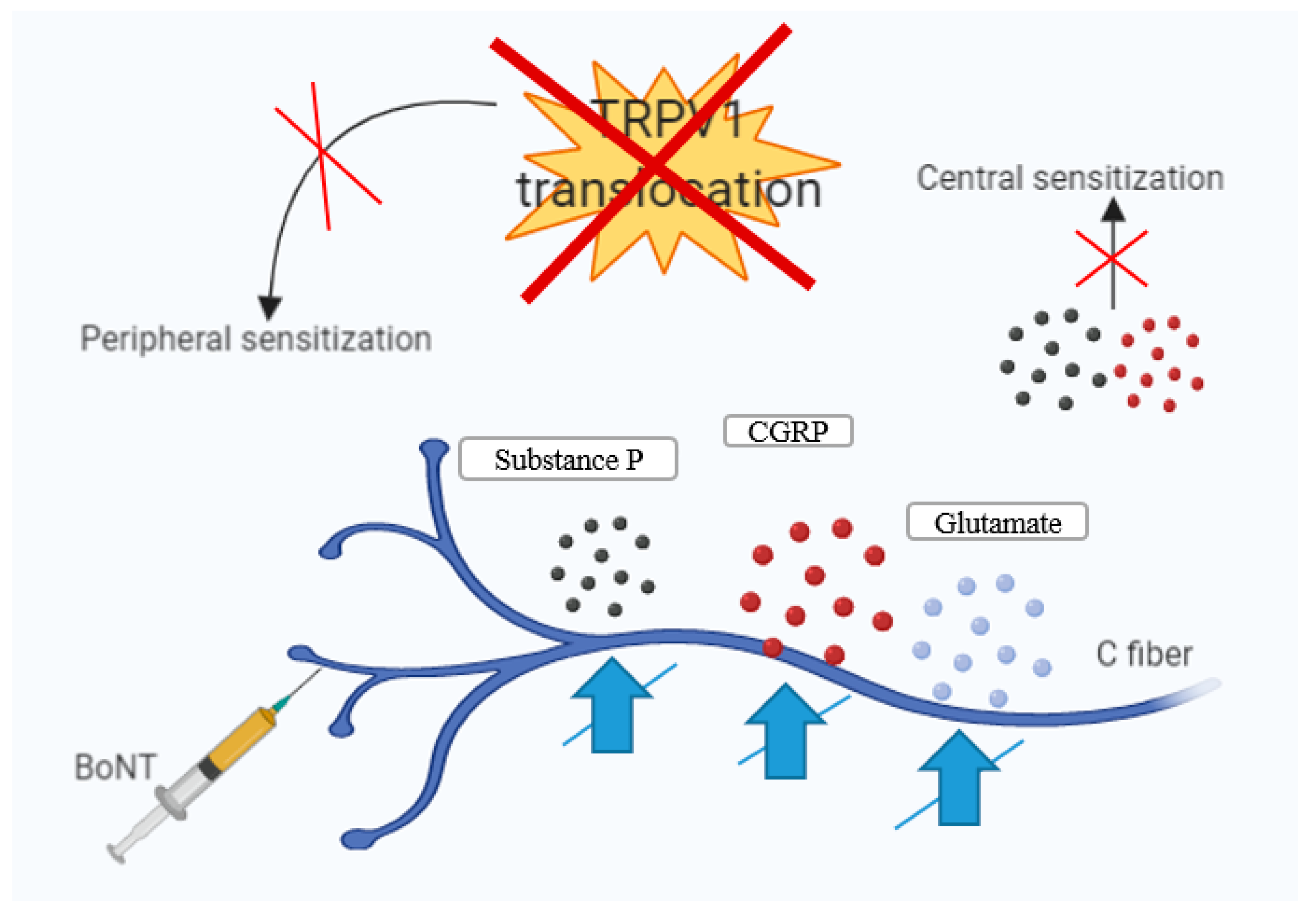
6. BoNT-A—Mechanisms of Action in Chronic Migraine
7. Results and Discussion—Clinical Studies of BoNT-A on Migraine
8. Conclusions and Future Perspectives
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ACH | Acetylcholine |
| BONT | Botulinum toxin |
| BONT-A | Botulinum toxin serotype A |
| BONT-B | Botulinum toxin serotype B |
| CGRP | Calcitonin gene-related peptide |
| CM | Chronic migraine |
| CNS | Central nervous system |
| DA | Dalton |
| E2 | Estradiol |
| EM | Episodic migraine |
| FDA | Food and Drug Administration |
| FHM | Familial hemiplegic migraine |
| FSH | Follicular-stimulant hormone |
| HC | Heavy chain |
| IL | Interleukin |
| LC | Light chain |
| MA | Migraine with aura |
| MIDAS | Migraine Disability Assessment |
| MO | Migraine without aura |
| MU | Mouse Units |
| NO | Nitric Oxide |
| NOS | Nitric oxide synthase |
| NSAID | Non-steroidal anti-inflammatory drug |
| PREEMPT | Phase III Research Evaluating Migraine Prophylaxis Therapy |
| QOL | Quality of Life |
| SNAP-25 | Synaptosomal-associated protein-25 kDa |
| SNARE | Soluble NSF attachment protein receptor |
| SP | Substance P |
| TNF-A | Tumor necrosis factor alpha |
| TRP | Transient receptor potential channel |
| TRPA1 | Transient receptor potential ankyrin 1 |
| TRVP1 | Transient receptor potential cation channel subfamily V member 1 |
| VAMP | Vesicle-associated membrane protein |
| WHO | World Health Organization |
References
- Ferrari, M.D.; Klever, R.R.; Terwindt, G.M.; Ayata, C.; van der Maagdenberg, A.M. Migraine pathophysiology: Lessons from mouse models and human genetics. Neurology 2015, 14, 65–80. [Google Scholar] [CrossRef]
- Lipton, R.B.; Steward, W.F.; Diamond, S.; Diamond, M.L.; Reed, M. Prevalence and Burden of Migraine in the United States: Data From the American Migraine Study II. Headache 2001, 41, 646–657. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, M.; Puri, V.; Puri, S. Serotonin and CGRP in Migraine. Ann. Neurosci. 2012, 19, 88–94. [Google Scholar] [CrossRef]
- Barbanti, P.; Ferroni, P. Onabotulinum toxin A in the treatment of chronic migraine: Patient selection and special considerations. J. Pain Res. 2017, 10, 2319. [Google Scholar] [CrossRef] [PubMed]
- Burch, R. Migraine and Tension-Type Headache: Diagnosis and Treatment. Med. Clin. N. Am. 2019, 103, 215–233. [Google Scholar] [CrossRef] [PubMed]
- Kors, E.; Haan, J.; Ferrari, M. Migraine genetics. Curr. Pain Headache Rep. 2003, 7, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Welch, K.M. Brain hyperexcitability: The basis for antiepileptic drugs in migraine prevention. Headache 2005, 45, S25–S32. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.J.; Fuh, J.L.; Lu, S.R.; Juang, K.D.; Wang, P.H. Migraine Prevalence During Menopausal Transition. Headache 2003, 43, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D.; Merriam, G.R. Estrogens, progestins, and headache. Neurology 1991, 41, 775–793. [Google Scholar] [CrossRef] [PubMed]
- Somerville, B.W. Estrogen withdrawal migraine. I. Duration of exposure required and attempted prophylaxis by premenstrual estrogen administration. Neurology 1975, 25, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Neri, I.; Granella, F.; Nappi, R.; Manzoni, G.C.; Facchinetti, F.; Genazzani, A.R. Characteristics of headache at menopause: A clinico-epidemiologic study. Maturitas 1993, 17, 31–37. [Google Scholar] [CrossRef]
- Whitty, C.W.; Hockaday, J.M. Migraine: A follow-up study of 92 patients. BMJ 1968, 1, 735–736. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.F.; Lipton, R.B.; Celentano, D.D.; Reed, M.L. Prevalence of migraine headache in the United States: Relation to age, income, race and other sociodemographic factors. JAMA 1992, 267, 64–69. [Google Scholar] [CrossRef] [PubMed]
- MacGregor, E.A. Migraine and the menopause. Br. Menopause Soc. J. 2006, 12, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Ibrahimi, K.; Couturier, E.G.M.; MaassenVanDenBrink, A. Migraine and perimenopause. Maturitas 2014, 78, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D.; Merriam, G. Sex hormones and headache 1999 (menstrual migraine). Neurology 1999, 53, S3–S13. [Google Scholar] [CrossRef]
- Calhoun, A.; Sutapa, F. Elimination of Menstrual-Related Migraine Beneficially Impacts Chronification and Medication Overuse. Headache 2008, 48, 1186–1193. [Google Scholar] [CrossRef]
- Martin, V.; Wernke, S.; Mandell, K.; Ramadan, N.; Kao, L.; Bean, J.; Liu, J.; Zoma, W.; Rebar, R. Defining the relationship between ovarian hormones and migraine headache. Headache 2005, 45, 1190–1201. [Google Scholar] [CrossRef]
- Lipton, R.B.; Bigal, M.E.; Diamond, M.; Freitag, F.; Reed, M.L.; Stewart, W.F. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology 2007, 68, 343–349. [Google Scholar] [CrossRef] [Green Version]
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef]
- Parikh, S.K.; Young, W.B. Migraine: Stigma in Society. Curr. Pain Headache Rep. 2019, 23, 8. [Google Scholar] [CrossRef] [PubMed]
- Evers, S.; Afra, J.; Frese, A.; Goadsby, P.J.; Linde, M.; May, A.; Sandor, P.S. EFNS guideline on the drug treatment of migraine–revised report of an EFNS task force. Eur. J. Neurol. 2009, 16, 968–981. [Google Scholar] [CrossRef] [PubMed]
- Linde, M.; Mulleners, W.M.; Chronicle, E.P.; McCrory, D.C. Gabapentin or pregabalin for the prophylaxis of episodic migraine in adults. Cochrane Database Syst. Rev. 2013, 6, 1–50. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, D.; Keam, S.J. Escitalopram. Drugs 2005, 65, 2379. [Google Scholar] [CrossRef] [PubMed]
- Tarlaci, S. Escitalopram and venlafaxine for the prophylaxis of migraine headache without mood disorders. Clin. Neuropharmacol. 2009, 32, 254–2588. [Google Scholar] [CrossRef] [PubMed]
- Burke, B.E.; Olson, R.D.; Cusack, B.J. Randomized, controlled trial of phytoestrogen in the prophylactic treatment of menstrual migraine. Biomed. Pharmacother. 2002, 56, 283–288. [Google Scholar] [CrossRef]
- Moga, M.A.; Dimienescu, O.G.; Balan, A.; Scarneciu, I.; Barabas, B.; Ples, L. Therapeutic Approaches of Botulinum Toxin in Gynecology. Toxins 2018, 10, 169. [Google Scholar] [CrossRef]
- Sarchielli, P.; Mancini, M.L.; Calabresi, P. Practical Considerations for the Treatment of Elderly Patients with Migraine. Drugs Aging. 2006, 23, 461–489. [Google Scholar] [CrossRef]
- Ramachandran, R.; Yaksh, T.L. Therapeutic use of botulinum toxin in migraine: Mechanisms of action. Br. J. Pharmacol. 2014, 171, 4177–4192. [Google Scholar] [CrossRef]
- Wheeler, A.H. Botulinum Toxin A, Adjunctive Therapy for Refractory Headaches Associated with Pericranial Muscle Tension. Headache 2003, 38, 468–471. [Google Scholar] [CrossRef]
- Brin, M.F. Botulinum toxin: Chemistry, pharmacology, toxicity, and immunology. Muscle Nerve 1997, 20, 146–168. [Google Scholar] [CrossRef]
- Nigam, P.K.; Anjana, N. Botulinum toxin. Indian J. Dermatol. 2010, 55, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. An update on new and unique uses of botulinum toxin in movement disorders. Toxicon 2018, 147, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D.; Eleopra, R. Clinical use of non-a botulinum toxins: Botulinum toxin type B. Neurotox. Res. 2006, 9, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Peroutka, S.J. Neurogenic inflammation and migraine: Implications for the therapeutics. Mol. Interv. 2005, 5, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J.; Ashina, M. Emerging migraine treatments and drug targets. Trends Pharmacol. Sci. 2011, 32, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Kainz, V.; Zhao, J.; Strassman, A.M.; Levy, D. Vascular ERK mediates migraine-related sensitization of meningeal nociceptors. Ann. Neurol. 2013, 73, 741–750. [Google Scholar] [CrossRef]
- May, A.; Goadsb, P.J. The trigeminovascular system in humans: Pathophysiologic implications for primary headache syndromes of the neural influences on the cerebral circulation. J. Cereb. Blood Flow Metab. 1999, 19, 115–127. [Google Scholar] [CrossRef]
- McNaughton, F.L.; Feindel, W.H. Innervation of Intracranial Structures: A Reappraisal. In Physiological Aspects of Clinical Neurology; Rose, F.C., Ed.; Blackwell Science: Hoboken, NJ, USA, 1977; pp. 279–293. [Google Scholar]
- Ray, B.S.; Wolff, H.G. Experimental studies on headache; pain-sensitive structures of the head and their significance in headache. Arch. Surg. 1940, 41, 813–856. [Google Scholar] [CrossRef]
- Pietrobon, D.; Moskowitz, M.A. Pathophysiology of migraine. Annu. Rev. Physiol. 2013, 75, 365–391. [Google Scholar] [CrossRef]
- Tajti, J.; Vecsei, L. The mechanism of peripheral and central sensitization in migraine. A literature review. Neuropsychopharmacol. Hung. 2009, 11, 15–21. [Google Scholar] [PubMed]
- Burstein, R.; Zhang, X.; Levy, D.; Aoki, K.R.; Brin, M.F. Selective inhibition of meningeal nociceptors by botulinum neurotoxin type A: Therapeutic implications for migraine and other pains. Cephalalgia 2014, 34, 853–869. [Google Scholar] [CrossRef] [PubMed]
- Strassman, A.M.; Raymond, S.A.; Burstein, R. Sensitization of meningeal sensory neurons and the origin of headaches. Nature 1996, 384, 560–564. [Google Scholar] [CrossRef] [PubMed]
- Mathew, N.T. Pathophysiology of chronic migraine and mode of action of preventive medications. Headache 2011, 51, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Strassman, A.M. Mechanical response properties of A and C primary afferent neurons innervating the rat intracranial dura. J. Neurophysiol. 2002, 88, 3021–3031. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Burstein, R.; Kainz, V.; Jakubowski, M.; Strassman, A.M. Mast cell degranulation activates a pain pathway underlying migraine headache. Pain 2007, 130, 166–176. [Google Scholar] [CrossRef] [Green Version]
- Eftekhari, S.; Warfvinge, K.; Blixt, F.W.; Edvinsson, L. Differentiation of nerve fibers storing CGRP and CGRP receptors in the peripheral trigeminovascular system. J. Pain 2013, 14, 1289–1303. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.C.; Strassman, A.M.; Burstein, R.; Levy, D. Sensitization and activation of intracranial meningeal nociceptors by mast cell mediators. J. Pharmacol. Exp. Ther. 2007, 322, 806–812. [Google Scholar] [CrossRef]
- Roch, M.; Messlinger, K.; Kulchitsky, V.; Tichonovich, O.; Azev, O.; Koulchitsky, S. Ongoing activity in trigeminal wide-dynamic range neurons is driven from the periphery. Neuroscience 2007, 150, 681–691. [Google Scholar] [CrossRef]
- Burstein, R.; Yamamura, H.; Malick, A.; Strassman, A.M. Chemical stimulation of the intracranial dura induces enhanced responses to facial stimulation in brain stem trigeminal neurons. J. Neurophysiol. 1998, 79, 964–982. [Google Scholar] [CrossRef]
- Schueler, M.; Messlinger, K.; Dux, M.; Neuhuber, W.L.; De, C.R. Extracranial projections of meningeal afferents and their impact on meningeal nociception and headache. Pain 2013, 154, 1622–1631. [Google Scholar] [CrossRef] [PubMed]
- Di Marzo, V.; Blumberg, P.M.; Szallasi, A. Endovanilloid signaling in pain. Curr. Opin. Neurobiol. 2002, 12, 372–379. [Google Scholar] [CrossRef]
- Uddman, R.; Tajti, J.; Hou, M.; Sundler, F.; Edvinsson, L. Neuropeptide expression in the human trigeminal nucleus caudalis and in the cervical spinal cord C1 and C2. Cephalalgia 2002, 22, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Jansen, I.; Uddman, R.; Ekman, R.; Olesen, J.; Ottosson, A.; Edvinsson, L. Distribution and effects of neuropeptide Y, vasoactive intestinal peptide, substance P, and calcitonin gene-related peptide in human middle meningeal arteries: Comparison with cerebral and temporal arteries. Peptides 1992, 13, 527–536. [Google Scholar] [CrossRef]
- Arulmani, U.; MassenVanDenBrink, A.; Villalon, C.M.; Saxena, P.R. Calcitonin gene-related peptide and its role in migraine pathophysiology. Eur. J. Pharmacol. 2004, 500, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Han, D. Association of serum levels of calcitonin gene-related peptide and cytokines during migraine attacks. Ann. Indian Acad. Neurol. 2019, 22, 277–281. [Google Scholar] [CrossRef]
- Mayberg, M.R.; Zervas, N.T.; Moskowitz, M.A. Trigeminal projections to supratentorial pial and dural blood vessels in cats demonstrated by horseradish peroxidase histochemistry. J. Comp. Neurol. 1984, 223, 46–56. [Google Scholar] [CrossRef]
- Edwards, R.M.; Stack, E.J.; Trizna, W. Calcitonin gene-related peptide stimulates adenylate cyclase and relaxes intracerebral arterioles. J. Pharmacol. Exp. Ther. 1991, 257, 1020–1024. [Google Scholar]
- Goadsby, P.J.; Edvinsson, L. The trigeminovascular system and migraine: Studies characterizing cerebrovascular and neuropeptide changes seen in humans and cats. Ann. Neurol. 1993, 33, 48–56. [Google Scholar] [CrossRef]
- Ashina, M.; Bendtsen, L.; Jensen, R.; Schifter, S.; Olesen, J. Evidence for increased plasma levels of calcitonin gene-related peptide in migraine outside of attacks. Pain 2000, 86, 133–138. [Google Scholar] [CrossRef]
- Buchanan, J.E.; Phillis, J.W. The role of nitric oxide in the regulation of cerebral blood flow. Brain Res. 1993, 610, 248–255. [Google Scholar] [CrossRef]
- Strecker, T.; Dux, M.; Messlinger, K. Nitric oxide releases calcitonin-gene-related peptide from rat dura mater encephali promoting increases in meningeal blood flow. J. Vasc. Res. 2002, 39, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Buture, A.; Gooriah, R.; Nimeri, R.; Ahmed, F. Current Understanding on Pain Mechanism in Migraine and Cluster Headache. Anesth. Pain Med. 2016, 6, e35190. [Google Scholar] [CrossRef] [PubMed]
- Lauritzen, M. On the possible relation of spreading cortical depression to classical migraine. Cephalalgia 1985, 5, 47–51. [Google Scholar] [CrossRef] [PubMed]
- DaSilva, A.F.M.; Granziera, C.; Tuch, D.S.; Snyder, J.; Vincent, M.; Hadjikhani, N. Interictal alterations of the trigeminal somatosensory pathway and PAG in migraine. Neuroreport 2007, 18, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.; Silberstein, S. Central sensitization theory of migraine: Clinical implications. Headache 2006, 46, S182–S191. [Google Scholar] [CrossRef] [PubMed]
- Buzzi, M.G.; Moskowitz, M.A. The trigeminovascular system and migraine. Pathol. Biol. 1992, 40, 313–317. [Google Scholar] [PubMed]
- Gao, Y.J.; Ji, R.R. c-Fos and pERK, which is a better marker for neuronal activation and central sensitization after noxious stimulation and tissue injury? Open Pain J. 2009, 2, 11–17. [Google Scholar] [CrossRef]
- Stewart, W.F.; Wood, C.; Reed, M.L.; Roy, J.; Lipton, R.B. Cumulative lifetime migraine incidence in women and men. Cephalalgia 2008, 28, 1170–1178. [Google Scholar] [CrossRef]
- MacGregor, E.A. Menstrual migraine: A clinical review. J. Fam. Plann. Reprod. Health Care 2007, 33, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Couturier, E.G.; Bomhof, M.A.; Neven, A.K.; Van Duijn, N.P. Menstrual migraine in a representative Dutch population sample: Prevalence, disability and treatment. Cephalalgia 2003, 23, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Sacco, S.; Ricci, S.; Degan, D.; Carolei, A. Migraine in women: The role of hormones and their impact on vascular diseases. J. Headache Pain 2012, 13, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Wöber, C.; Brannath, W.; Schmidt, K.; Kapitan, M.; Rudel, E.; Wessely, P.; Wöber-Bingöl, C. PAMINA Study Group. Cephalalgia 2007, 27, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Sulak, P.J. The perimenopause: A critical time in a woman’s life. Int. J. Fertil Menopausal Stud. 1996, 41, 85–89. [Google Scholar] [PubMed]
- Finocchi, C.; Ferrari, M. Female reproductive steroids and neuronal excitability. Neurol. Sci. 2011, 32, S31–S35. [Google Scholar] [CrossRef] [PubMed]
- MacGregor, E.A. Migraine headache in perimenopausal and menopausal women. Curr. Pain Headache Rep. 2009, 13, 399–403. [Google Scholar] [CrossRef]
- Ebner, S.; Dunbar, M.; McKinnon, R.D. Distinct Roles for PI3K in proliferation and survival of oligodedrocyte progenitor cells. J. Neurosci. Res. 2000, 62, 336–345. [Google Scholar] [CrossRef]
- Couse, J.F.; Lindzey, J.; Grandien, K.; Gustafsson, J.A.; Korach, K.S. Tissue distribution and quantitative analysis of estrogen receptor-alpha (ERα) and estrogen receptor-beta (ERβ) messenger ribonucleic acid in the wild-type and ERα–knockout mouse. Endocrinology 1997, 138, 4613–4621. [Google Scholar] [CrossRef]
- Bjornstrom, L.; Sjoberg, M. Estrogen receptor-dependent activation of AP-1 via non-genomic signaling. Nucl. Recept. 2004, 2, 3. [Google Scholar] [CrossRef]
- Simpson, D.; Hallett, M.; Ashman, E.; Comella, C.; Green, M.; Gronseth, G. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [PubMed]
- Nappi, R.E.; Berga, S.L. Migraine and reproductive life. Handbook Clin. Neurol. 2010, 97, 303–322. [Google Scholar] [CrossRef]
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum Neurotoxins: Biology, Pharmacology and Toxicology. Pharmacol. Rev. 2017, 69, 200–235. [Google Scholar] [CrossRef] [PubMed]
- Rossetto, O.; Pirazzini, M.; Montecucco, C. Botulinum neurotoxins: Genetic, structural and mechanistic insights. Nat. Rev. Microbiol. 2014, 12, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.K.; Smith, T.J. Genetic diversity within Clostridium botulinum serotypes, botulinum neurotoxin gene clusters and toxin subtypes. Curr. Top. Microbiol. Immunol. 2013, 364, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Burke, G.S. Notes on Bacillus botulinus. J. Bacteriol. 1919, 4, 555–570. [Google Scholar] [PubMed]
- Montal, M. Botulinum neurotoxin: A marvel of protein design. Annu. Rev. Biochem. 2010, 79, 591–617. [Google Scholar] [CrossRef] [PubMed]
- Turton, K.; Chaddock, J.A.; Acharya, K.R. Botulinum and tetanus neurotoxins: Structure, function and therapeutic utility. Trends Biochem. Sci. 2002, 27, 552–558. [Google Scholar] [CrossRef]
- Fischer, A.; Montal, M. Single molecule detection of intermediates during botulinum neurotoxin translocation across membranes. Proc. Natl. Acad. Sci. USA 2007, 104, 10447–10452. [Google Scholar] [CrossRef] [Green Version]
- Jahn, R.; Scheller, R.H. SNAREs-engines for membrane fusion. Nat. Rev. Mol. Cell Biol. 2006, 7, 631–643. [Google Scholar] [CrossRef]
- Sudhof, T.C.; Rothman, J.E. Membrane fusion: Grappling with SNARE and SM proteins. Science 2009, 323, 474–477. [Google Scholar] [CrossRef]
- Dolly, J.O.; Lawrence, G.W.; Meng, J.; Wang, J.; Ovsepian, S.V. Neuro-exocytosis: Botulinum toxins as inhibitory probes and versatile therapeutics. Curr. Opin. Pharmacol. 2009, 9, 326–335. [Google Scholar] [CrossRef]
- Johnson, E.A.; Montecucco, C. Botulism. In Handbook of Clinical Neurology; Andrew, G.E., Ed.; Elsevier: Amsterdam, The Netherlands, 2008; pp. 333–368. [Google Scholar]
- Montecucco, C.; Schiavo, G. Mechanism of action of tetanus and botulinum neurotoxins. Mol. Microbiol. 1994, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Argoff, C.E. A Focused Review on the Use of Botulinum Toxins for Neuropathic Pain. Clin. J. Pain. 2002, 18, S177–S181. [Google Scholar] [CrossRef] [PubMed]
- Sloop, R.R.; Bradley, A.C.; Escutin, R.O. Human response to botulinum toxin injection: Type B compared with type A. Neurology 1997, 49, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Menstrual Migraine. New York Headache Center. Available online: https://nyheadache.com/educational-materials/menstrual-migraine/ (accessed on 19 July 2019).
- Gupta, S.; Amrutkar, D.V.; Mataji, A.; Salmasi, H.; Hay-Schmidt, A.; Sheykhzade, M.; Messlinger, K.; Olesen, J.; Jansen-Olesen, I. Evidence for CGRP re-uptake in rat dura mater encephali. Br. J. Pharmacol. 2010, 161, 1885–1898. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Park, H.J. Botulinum toxin for the treatment of neuropathic pain. Toxins 2017, 9, 260. [Google Scholar] [CrossRef]
- Takasusuki, T.; Yaksh, T.L. Regulation of spinal substance p release by intrathecal calcium channel blockade. Anesthesiology 2011, 115, 153–164. [Google Scholar] [CrossRef]
- Baulmann, J.; Spitznagel, H.; Herdegen, T.; Unger, T. and Culman, J. Tachykinin receptor inhibition and c-Fos expression in the rat brain following formalin-induced pain. Neuroscience 2000, 95, 813–820. [Google Scholar] [CrossRef]
- Aoki, K.R.; Francis, J. Updates on the antinociceptive mechanism hypothesis of botulinum toxin A. Parkinsonism Relat. Disord. 2011, 17, S28–S33. [Google Scholar] [CrossRef]
- Durham, P.L.; Cady, R.; Cady, R. Regulation of Calcitonin Gene-Related Peptide Secretion From Trigeminal Nerve Cells by Botulinum Toxin Type A: Implications for Migraine Therapy. Headache 2004, 44, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K. Therapeutic use of botulinum toxin in pain treatment. Neur. Signal. 2018, 2, NS20180058. [Google Scholar] [CrossRef] [Green Version]
- Sulak, M.A.; Ghosh, M.; Sinharoy, P.; Andrei, S.R. Modulation of TRPA1 channel activity by Cdk5 in sensory neurons. Channels 2017, 12, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Cheng, J.; Zhuang, Y.; Qu, W.; Muir, J.; Liang, H.; Zhang, D. Botulinum toxin type A reduces hyperalgesia and TRPV1 expression in rats with neuropathic pain. Pain Med. 2013, 14, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Dhaliwal, H.P.; Kukreja, R.V.; Singh, B.R. The Botulinum Toxin as a Therapeutic Agent: Molecular Structure and Mechanism of Action in Motor and Sensory Systems. Semin. Neurol. 2016, 36, 10–19. [Google Scholar] [CrossRef] [Green Version]
- Lawrence, G.W.; Ovsepian, S.V.; Wang, J.; Aoki, K.R.; Dolly, J.O. Extravesicular intraneuronal migration of internalized botulinum neurotoxins without detectable inhibition of distal neurotransmission. Biochem. J. 2012, 441, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Restani, L.; Giribaldi, F.; Manich, M.; Bercsenyi, K.; Menendez, G.; Rossetto, O.; Caleo, M.; Schiavo, G. Botulinum neurotoxins A and E undergo retrograde axonal transport in primary motor neurons. PLoS Pathog. 2012, 8, e1003087. [Google Scholar] [CrossRef]
- Restani, L.; Antonucci, F.; Gianfranceschi, L.; Rossi, C.; Rossetto, O.; Caleo, M. Evidence for anterograde transport and transcytosis of botulinum neurotoxin A (BoNT/A). J. Neurosci. 2011, 31, 15650–15659. [Google Scholar] [CrossRef]
- Antonucci, F.; Rossi, C.; Gianfranceschi, L.; Rossetto, O.; Caleo, M. Long-distance retrograde effects of botulinum neurotoxin A. J. Neurosci. 2008, 28, 3689–3696. [Google Scholar] [CrossRef]
- Favre-Guilmard, C.; Auguet, M.; Chabrier, P.E. Different antinociceptive effects of botulinum toxin type A in inflammatory and peripheral polyneuropathic rat models. Eur. J. Pharmacol. 2009, 617, 48–53. [Google Scholar] [CrossRef]
- Costa, C.; Tozzi, A.; Rainero, I.; Cupini, L.M.; Calabresi, P.; Sarchielli, P. Cortical spreading depression as a target for anti-migraine agents. J. Headache Pain 2013, 14, 62. [Google Scholar] [CrossRef] [PubMed]
- Schmieg, N.; Menendez, G.; Schiavo, G.; Terenzio, M. Signalling endo-somes in axonal transport: Travel updates on the molecular highway. Semin. Cell Dev. Biol. 2014, 27, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Bach-Rojecky, L.; Salković-Petrisić, M.; Lacković, Z. Botulinum toxin type A reduces pain supersensitivity in experimental diabetic neu-ropathy: Bilateral effect after unilateral injection. Eur. J. Pharmacol. 2010, 633, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Bach-Rojecky, L.; Lacković, Z. Central origin of the antinocicep-tive action of botulinum toxin type A. Pharmacol. Biochem. Behav. 2009, 94, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Cui, M.; Khanijou, S.; Rubino, J.; Aoki, K. Subcutaneous administra-tion of botulinum toxin A reduces formalin- induced pain. Pain 2004, 107, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, T.; Goadsby, P.J. Stimulation of the greater occipital nerve induces increased central excitability of dural afferent input. Brain 2002, 125, 1496–1509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Aurora, S.K.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F.; PREEMPT Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Pooled results from the double- blind, randomized, placebo- controlled phases of the PREEMPT clinical program. Headache 2010, 50, 921–936. [Google Scholar] [CrossRef] [PubMed]
- Do, T.P.; Hvedstrup, J.; Schytz, H.W. Botulinum toxin: A review of the mode of action in migraine. Acta Neur. Scand. 2018, 137, 442–451. [Google Scholar] [CrossRef]
- Aguila, M.E.R.; Rebbeck, T.; Leaver, A.M.; Lagopoulos, J.; Brennan, P.C.; Hübscher, M.; Refshauge, K.M. The association between clinical characteristics of migraine and brain GABA levels: An explor-atory study. J. Pain 2016, 17, 1058–1067. [Google Scholar] [CrossRef]
- Janis, J.E.; Barker, J.C.; Palettas, M. Targeted Peripheral Nerve-directed Onabotulinumtoxin A Injection for Effective Long-term Therapy for Migraine Headache. Plat. Reconstr. Surg. Glob. Open 2017, 5, e1270. [Google Scholar] [CrossRef]
- Wollina, U. Botulinum Toxin Type A: Anabotulinum A, Onabotulinum A, and Incabotulinum A–Differences and Common Sense. Kosmetische Medizin 2015, 36, 112–114. [Google Scholar]
- Katsarava, Z.; Buse, D.C.; Manack, A.N.; Lipton, R.B. Defining the Differences Between Episodic Migraine and Chronic Migraine. Curr. Pain Headache Rep. 2012, 16, 86. [Google Scholar] [CrossRef] [PubMed]
- Escher, C.M.; Paracka, L.; Dressler, D.; Kollewe, K. Botulinum toxin in the management of chronic migraine: Clinical evidence and experience. Ther. Adv. Neurol. Disord. 2017, 10, 127. [Google Scholar] [CrossRef] [PubMed]
- Martin, V.T. Migraine and the menopausal transition. Neurol. Sci. 2014, 35, 65–69. [Google Scholar] [CrossRef]
- Kazerooni, R.; Lim, J.; Blake, A.; Lessig, S. IncobotulinumtoxinA for migraine: A retrospective case series. Clin. Ther. 2015, 37, 1860–1864. [Google Scholar] [CrossRef] [PubMed]
- Gazerani, P.; Pedersen, N.; Staahl, C.; Drewes, A.; Arendt-Nielsen, L. Subcutaneous Botulinum toxin type A reduces capsaicin- induced trigeminal pain and vasomotor reactions in human skin. Pain 2009, 141, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Kollewe, K.; Escher, C.M.; Wulff, D.U.; Fathi, D.; Paracka, L.; Mohammadi, B.; Karst, M.; Dressler, D. Long-term treatment of chronic migraine with OnabotulinumtoxinA: Efficacy, quality of life and tolerability in a real-life setting. J. Neural. Transm. 2016, 123, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F.; PREEMPT 1 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia 2010, 30, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.C.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; DeGryse, R.E.; Lipton, R.B.; Silberstein, S.D.; Brin, M.F.; PREEMPT 2 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia 2010, 30, 804–814. [Google Scholar] [CrossRef]
- Hienn, H.; Gonzalez, A. Migraine Headache Prophylaxis. Am. Fam. Phys. 2019, 99, 17–24. [Google Scholar]
- Cady, R.K.; Schreiber, C.P.; Porter, J.A.; Blumenfeld, A.M.; Farmer, K.U. A multi-center double-blind pilot comparison of onabotulinumtoxinA and topiramate for the prophylactic treatment of chronic migraine. Headache 2011, 51, 21–32. [Google Scholar] [CrossRef]
- Binder, W.J.; Brin, M.F.; Blitzer, A.; SChoenrock, L.D.; Pogoda, J.M. Botulinum toxin type A (BOTOX) for treatment of migraine headaches: An open-label study. Otolaryngol. Head Neck Surg. 2000, 123, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.; Mathew, N.; Saper, J.; Jenkins, S. Botulinum toxin type A as a migraine preventive treatment. For the BOTOX Migraine Clinical Research Group. Headache 2000, 40, 445–450. [Google Scholar] [CrossRef]
- Mathew, N.T.; Frishberg, B.M.; Gawel, M.; Dimitrova, R.; Gibson, J.; Turkel, C.; BOTOX CDH Study Group. Botulinum toxin type A (BOTOX) for the prophylactic treatment of chronic daily headache: A randomized, double-blind, placebo-controlled trial. Headache 2005, 45, 293–307. [Google Scholar] [CrossRef]
- Hou, M.; Xie, J.F.; Kong, H.P.; Zhang, Y.; Shao, Y.F.; Wang, C.; Ren, W.T.; Cui, G.F.; Xin, L.; Hou, Y.P. Acupoint Injection of Onabotulinumtoxin A for Migraines. Toxins 2015, 7, 4442–4454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipton, R.B.; Varon, S.F.; Grosberg, B.; McAllister, P.J.; Freitag, F.; Aurora, S.K.; Dodick, D.W.; Silberstein, S.D.; Diener, H.C.; DeGryse, R.E.; et al. OnabotulinumtoxinA improves quality of life and reduces impact of chronic migraine. Neurology 2011, 77, 1465–1472. [Google Scholar] [CrossRef] [PubMed]
- Jakubowski, M.; McAllister, P.J.; Bajwa, Z.H.; Ward, T.N.; Smith, P.; Burstein, R. Exploding vs. imploding headache in migraine prophylaxis with botulinum toxin A. Pain 2006, 125, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.L.; Kuriyama, A.; Hayashino, Y. Botulinum toxin A for prophylactic treatment of migraine and tension headaches in adults: A meta-analysis. JAMA 2012, 307, 1736–1745. [Google Scholar] [CrossRef]
- Cernuda-Morollón, E.; Ramón, C.; Larrosa, D.; Alvarez, R.; Riesco, N.; Pascual, J. Long-term experience with onabotulinumtoxinA in the treatment of chronic migraine: What happens after one year? Cephalalgia 2005, 35, 864–868. [Google Scholar] [CrossRef] [PubMed]
- Saper, J.R.; Mathew, N.T.; Loder, E.W.; DeGryse, R.; VanDenburgh, A.M. A Double-Blind, Randomized, Placebo-Controlled Comparison of Botulinum Toxin Type A Injection Sites and Doses in the Prevention of Episodic Migraine. Pain Med. 2007, 8, 478–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evers, S.; Vollmer-Haase, J.; Schwaag, S.; Rahmann, A.; Husstedt, I.W.; Frese, A. Botulinum toxin A in the prophylactic treatment of migraine—A randomized, double-blind, placebo-controlled study. Cephalalgia 2004, 24, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Vo, A.H.; Satori, R.; Jabbari, B.; Green, J.; Killgore, W.D.; Labutta, R.; Campbell, W.W. Botulinum toxin type-a in the prevention of migraine: A double-blind controlled trial. Aviat. Space Environ. Med. 2007, 78, 113–118. [Google Scholar]
- Petri, S.; Tolle, T.; Straube, A.; Pfaffenrath, V.; Stefenelli, U.; Ceballos-Baumann, A. Botulinum Toxin as Preventive Treatment for Migraine: A Randomized Double-Blind Study. Eur. Neurol. 2009, 62, 204–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chankrachang, S.; Arayawichanont, A.; Poungvarin, N.; Nidhinandana, S.; Boonkongchuen, P.; Towanabut, S.; Sithinamsuwan, P.; Kongsaengdao, S. Prophylactic Botulinum Type A Toxin Complex (Dysport®) for Migraine Without Aura. Headache 2011, 51, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Anand, K.S.; Prasad, A.; Singh, M.M.; Sharma, S.; Bala, K. Botulinum toxin type A in prophylactic treatment of migraine. Am. J. Ther. 2006, 13, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Relja, M.; Poole, A.C.; Schoenen, J.; Pascual, J.; Lei, X.; Thompson, C. A multicentre, double-blind, randomized, placebo-controlled, parallel group study of multiple treatments of botulinum toxin type A (BoNTA) for the prophylaxis of episodic migraine headaches. Cephalalgia 2007, 27, 492–503. [Google Scholar] [CrossRef] [PubMed]
- Elkind, A.H.; O’Carroll, P.; Blumenfeld, A.; DeGryse, R.; Dimitrova, R. A series of three sequential, randomized, controlled studies of repeated treatments with botulinum toxin type A for migraine prophylaxis. J. Pain 2006, 7, 688–696. [Google Scholar] [CrossRef]
- Barrientos, N.; Chana, P. Botulinum toxin type A in prophylactic treatment of migraine headaches: A preliminary study. J. Headache Pain 2003, 4, 146–151. [Google Scholar] [CrossRef]
- Freitag, F.G.; Diamond, S.; Diamond, M.; Urban, G. Botulinum Toxin Type A in the treatment of chronic migraine without medication overuse. Headache 2008, 48, 201–209. [Google Scholar] [CrossRef]
- Magalhaes, E.; Menezes, C.; Cardeal, M.; Melo, A. Botulinum toxin type A versus amitriptyline for the treatment of chronic daily migraine. Clin. Neurol. Neurosurg. 2010, 112, 463–466. [Google Scholar] [CrossRef]
- Mathew, N.T.; Jaffri, S.F. A double-blind comparison of onabotulinumtoxina (BOTOX) and topiramate (TOPAMAX) for the prophylactic treatment of chronic migraine: A pilot study. Headache 2009, 49, 1466–1478. [Google Scholar] [CrossRef] [PubMed]
- Aurora, S.K.; Winner, P.; Freeman, M.C.; Spierings, E.L.; Heiring, J.O.; DeGryse, R.E.; Van Denburgh, A.M.; Nolan, M.E.; Turkel, C.C. Onabotulinumtoxin A for treatment of chronic migraine: Pooled analyses of the 56-week PREEMPT clinical program. Headache 2011, 51, 1358–1373. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
 |  |  |  |  |  |  |
|---|---|---|---|---|---|---|
| Ophthalmic Disorders | Movement Disorders | Cosmetic Applications | Chronic Pain | Genito-Urinary System Disorders | Gastrointestinal Disorders | Other Conditions |
| Established Indications Of Bont (Approved by FDA) | Tried Applications of Bont | |||||
| Strabismus | Cervical dystonia | Wrinkles | Migraine | Chronic pelvic pain | Achalasia | Cerebral palsy |
| Concomitant misalignment | Oromandibular dystonia | Axillary Hyperhidrosis | Tension type headache | Vulvodynia | Bruxism | Spinal cord injury |
| Restrictive or myogenic strabismus | Torticollis | Lateral canthal lines | Lower back ache | Detrusor-sphincter dyssynergia | Palatal myoclonus | Various brain injuries after trauma |
| Eyelid retraction | Tardive dystonia | Glabellar lines | Myofascial pain | Spasms of perineal musculature | Chronic anal fissures | Upper-limb spasticity |
| Duane’s syndrome | Other focal dystonias | Browlift | Tennis elbow | Dyspareunia | Larynx affections | Hemifacial spasms |
| Non-concomitant Misalignment | Trigeminal neuropathy | Painful bladder syndrome | Temporomandibular joint dysfunction | Stoke-induced spasticity | ||
| Author, Reference | Study Design | No. of Patients | Type of Migraine | Dose of BoNT-A | Results | Follow-Up Period |
|---|---|---|---|---|---|---|
| Saper et al., 2007 [142] | Randomized, Double-Blind, placebo-control study | 232 patients (45 placebo) | EM | 25 U BoNT-A | Both BoNT-A and placebo had similar efficiency, and showed greater reduction of migraine severity | 3 months |
| Evers et al., 2004 [143] | Randomized, Double-Blind, placebo-control study | 60 patients (20 placebo) | EM | 16 U or 100 U BoNT-A | Both BoNT-A and placebo decreased the number of migraine days and the frequency of the attacks | 3 months |
| Vo et al., 2007 [144] | Randomized, Double-Blind, placebo-control study | 32 patients (17 placebo) | EM | 205 U BoNT-A | No significant reduction of migraine frequency and severity was registered The headache pattern index indicated a protective effect for BoNT-A against attacks severity | 3 months |
| Petri et al., 2009 [145] | Randomized, Double-Blind, placebo-control study | 127 patients (63 placebo) | EM | 80–120 U BoNT-A into cervical and pericranial muscles | BoNT-A was not useful as a prophylactic treatment; the reduction of headache did not reach statistically significance | 3 months |
| Chankrachang et al., 2011 [146] | Randomized, Double-Blind, placebo-control study | 128 patients (37 placebo) | EM | 120–240 U BoNT-A | BoNT-A was significantly useful over placebo | 8–12 weeks |
| Anand et al., 2006 [147] | Randomized, Double-Blind, placebo-control study | 32 patients (16 placebo) | EM | 50 U BoNT-A | 75% of patients reported a complete relief of the symptoms | 3 months |
| Relja et al., 2007 [148] | Randomized, Double-Blind, placebo-control study | 515 patients | EM | 75–225 U BoNT-A | Similar results in both groups | 9 months |
| Silberstein et al., 2000 [135] | Randomized, Double-Blind, placebo-control study | 123 (41 placebo) | EM | 25 U or 75 U BoNT-A | Greater results in both groups | 3 months |
| Elkind et al., 2006 [149] | Randomized, Double-Blind, placebo-control study | 182 patients (100 placebo) | EM | 7.5 U–50 U BoNT-A | No improvements in headache were noted, no differences between BoNT-A and placebo | 120 days |
| Barrientos and Chana, 2003 [150] | Randomized, Double-Blind, placebo-control study | 30 patients (15 placebo) | EM | 50 U BoNT-A | The number of attacks per day and headache frequencies were significantly reduced on day 90 | 3 months |
| Freitag et al., 2008 [151] | Randomized, Double-Blind, placebo-control study | 86 patients | CM | 100 U BoNT-A | BoNT-A was superior to placebo for both endpoints | 4 months |
| Cady et al., 2011 [133] | Randomized, Double-Blind, placebo-control study | 59 patients (30 topiramate) | CM | 300 U BoNT-A | Similar results for both BoNT-A and Topiramate | 26 weeks |
| Diener et al., 2010 [131] | Randomized, Double-Blind, placebo-control study | 679 patients (338 placebo) | CM | 155–195 U BoNT-A | All the secondary endpoints were favoured | 32 weeks |
| Binder et al., 2000 [134] | Non-randomized, open-label | 106 patients | CM | −51% of cases—complete response −38% of cases—partial response −70% of cases—improvements were observed after one hour of injection | 3 months | |
| Magalhaes et al., 2010 [152] | Randomized, Double-Blind, placebo-control study | 72 patients (23 amytriptiline) | CM | 250 U BoNT-A | No difference was observed between BoNT-A and amytriptiline effects | 90 days |
| Mathew et al., 2009 [153] | Randomized, Double-Blind, placebo-control study | 60 patients (29 topiramate) | CM | 200 U BoNT-A | Similar results for both groups. BoNT-A and Topiramate showed similar efficiency | 9 months |
| Aurora et al., 2011 [154] | Randomized, Double-Blind, placebo-control study | 1384 patients (696 placebo) | CM | 155–195 U BoNT-A | BoNT-A was efficient in improvement of the total headache days number | 56 weeks |
| Aurora et al., 2010 [130] | Randomized, Double-Blind, placebo-control study | 679 patients (338 placebo) | CM | 155–195 U BoNT-A | BoNT-A was efficient in improvement of the headache days number but no reduction in the migraine episodes was recorded | 24 weeks |
| Lipton et al., 2011 [138] | Randomized, Double-Blind, placebo-control study | 1384 patients (696 placebo) | CM | 155 U BoNT-A | Significantly reduction in headache compared to placebo | 56 weeks |
| Mathew et al., 2005 [136] | Prospective Study | 571 patients | CM | 105–260 U | 50% or more decrease in the frequency of headache days was registered at 180 days | 11 months |
| Dodick et al., 2009 [119] | Randomized, placebo-control study | 1384 patients | CM | 155–195 U | BoNT-A considerable decreased the number of pain days in comparison to placebo. | 24 weeks |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dima, L.; Bălan, A.; Moga, M.A.; Dinu, C.G.; Dimienescu, O.G.; Varga, I.; Neculau, A.E. Botulinum Toxin a Valuable Prophylactic Agent for Migraines and a Possible Future Option for the Prevention of Hormonal Variations-Triggered Migraines. Toxins 2019, 11, 465. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080465
Dima L, Bălan A, Moga MA, Dinu CG, Dimienescu OG, Varga I, Neculau AE. Botulinum Toxin a Valuable Prophylactic Agent for Migraines and a Possible Future Option for the Prevention of Hormonal Variations-Triggered Migraines. Toxins. 2019; 11(8):465. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080465
Chicago/Turabian StyleDima, Lorena, Andreea Bălan, Marius Alexandru Moga, Cătălina Georgeta Dinu, Oana Gabriela Dimienescu, Ioana Varga, and Andrea Elena Neculau. 2019. "Botulinum Toxin a Valuable Prophylactic Agent for Migraines and a Possible Future Option for the Prevention of Hormonal Variations-Triggered Migraines" Toxins 11, no. 8: 465. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080465