The Impact of the Course of Disease before Botulinum Toxin Therapy on the Course of Treatment and Long-Term Outcome in Cervical Dystonia


Abstract
:1. Introduction
2. Results
2.1. Demographical Data, Treatment Related Data and Outcome of the Entire Cohort
2.2. Correlation Analysis of Demographical and Treatment Related Data
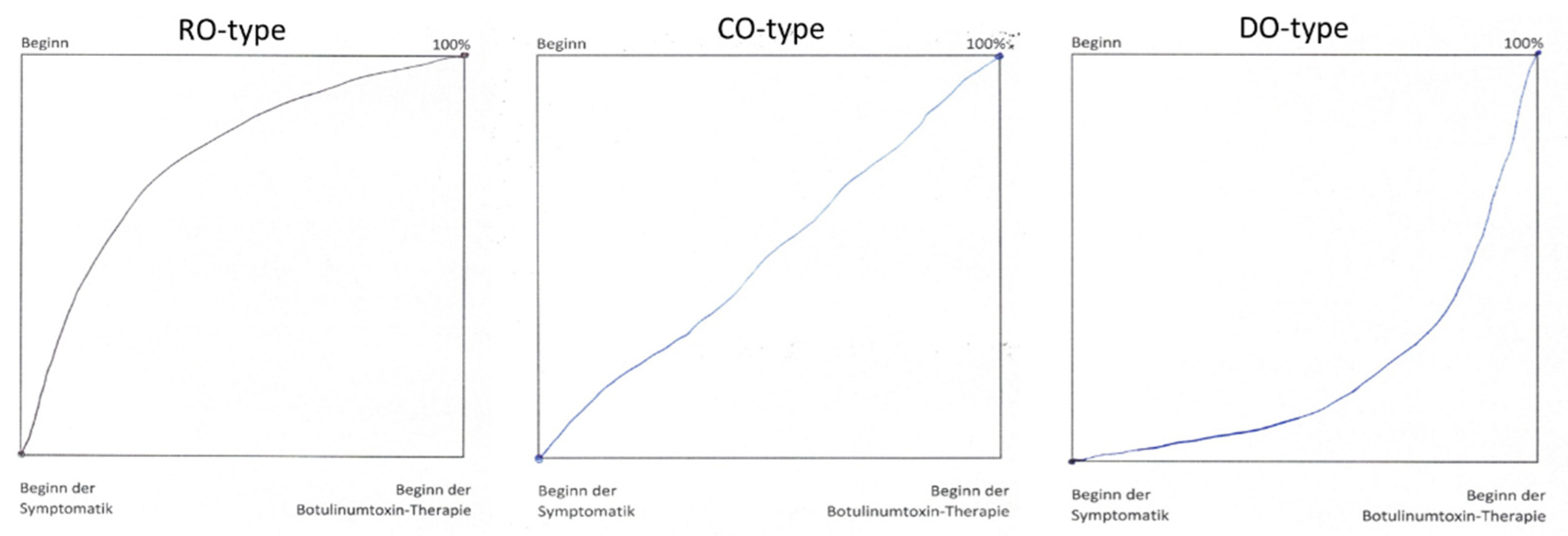
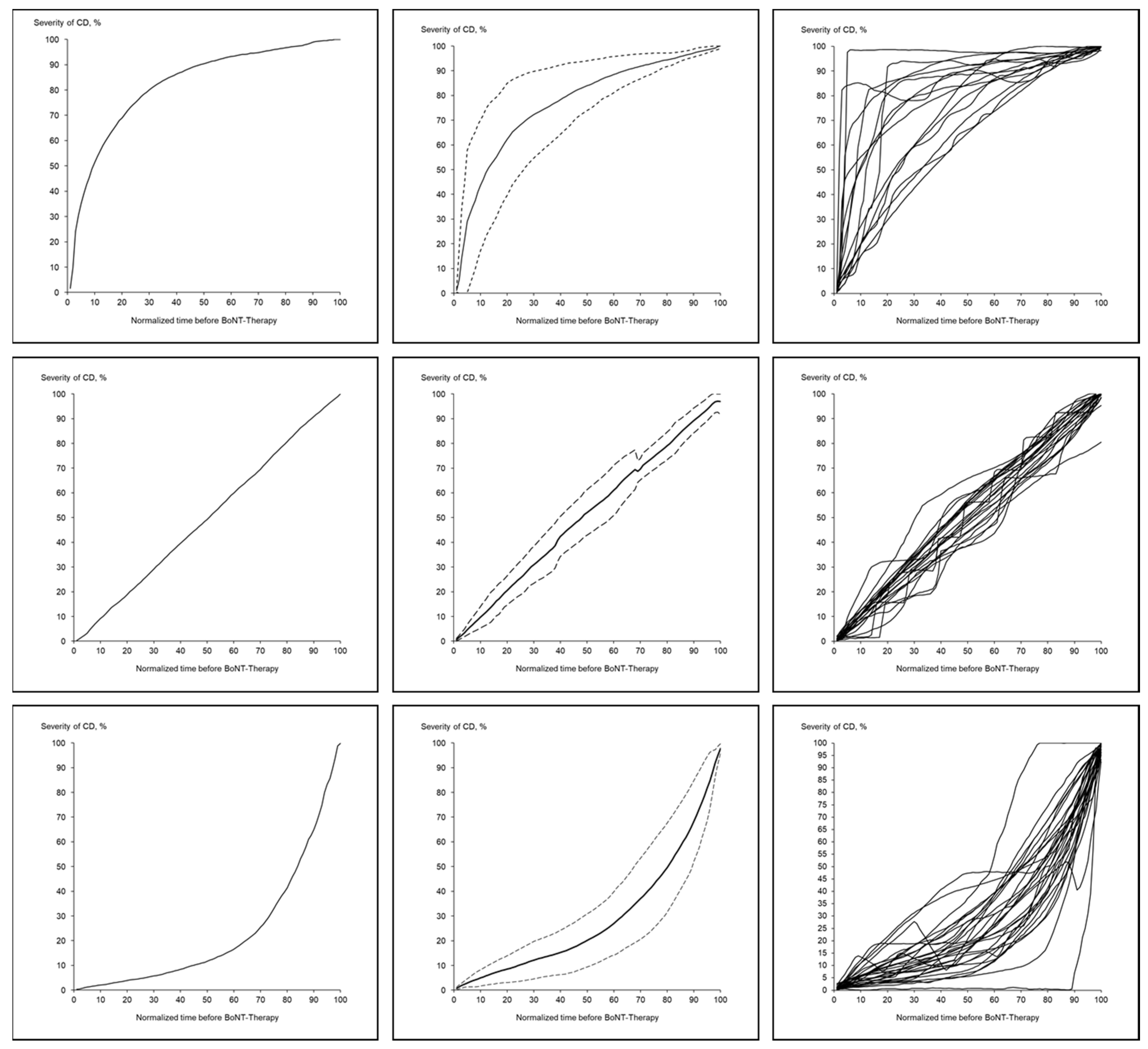
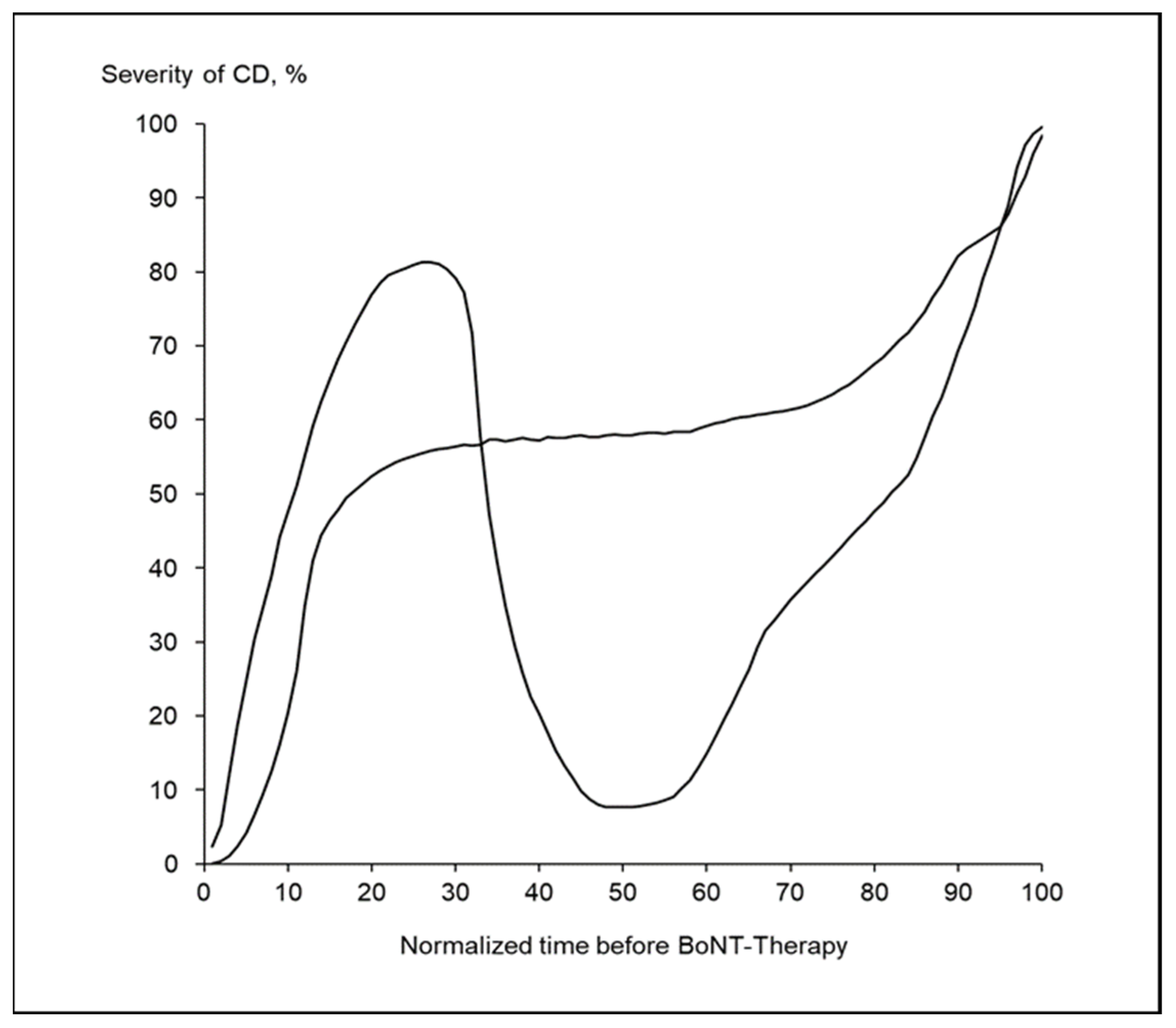
2.3. Three Main and One Exceptional CoDB-Graph Type
2.4. Comparison of Patient-Subgroups Classified According to the CoDB-Graph Type
3. Discussion
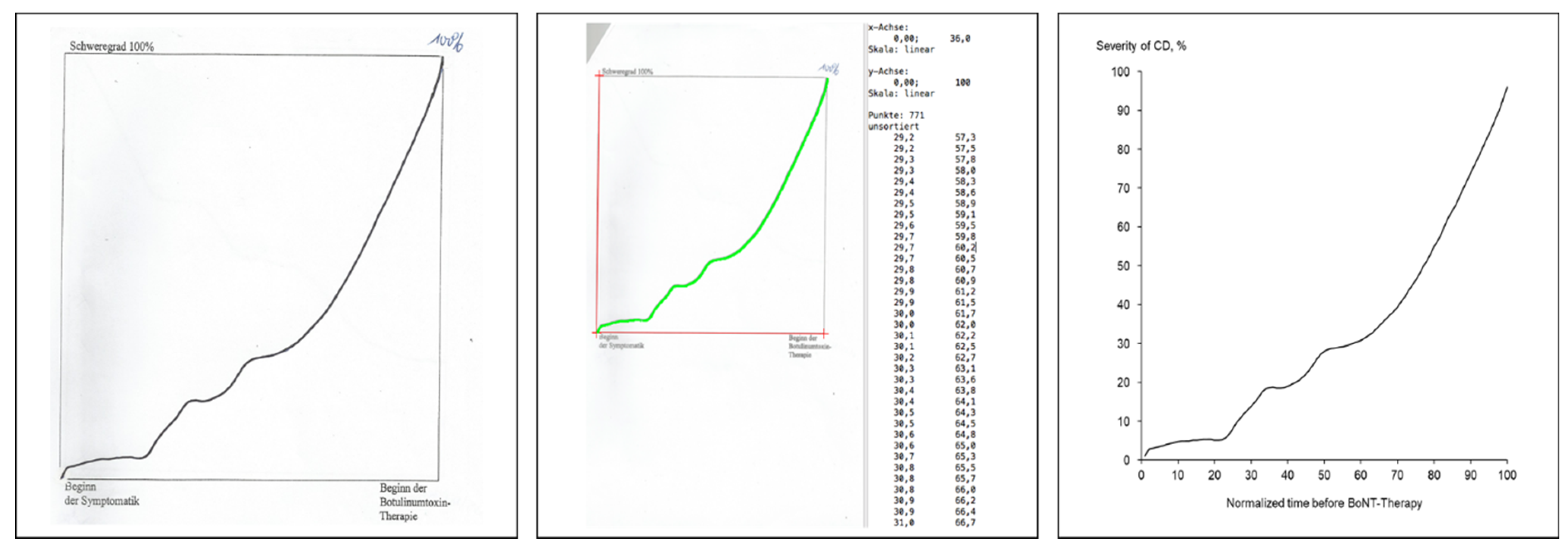
3.1. General Remark on CoDB-Graph Drawing
3.2. The Frequency of the Four Different CoDB-Graph Types
3.3. Clinical Differences between the Three RO, CO- and DO-Patient Subgroups
3.4. Differences in the Initiation of BoNT Treatment across the RO-, CO-, and the DO-Group
3.5. Differences in Dose Adjustment during BoNT Treatment across the RO-, CO-, and the DO-Group
3.6. Differences in Outcome between the RO-, CO- and DO-Patient Subgroups
4. Concluding Remarks
5. Strengths and Limitations of the Study
6. Materials and Methods
6.1. Patients and Treatment-Related Data
6.2. Drawing of the Course of Disease Graphs (CoD-Graphs)
6.3. Classification of the CoDB-Graphs
6.4. Statistics
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Epidemiological Study of Dystonia in Europe Collaborative Group. Sex-related influences on the frequency and age of onset of primary dystonia. Neurology 1999, 53, 1871–1873. [Google Scholar] [CrossRef]
- Steeves, T.D.; Day, L.; Dykeman, J.; Jette, N.; Pringsheim, T. The prevalence of primary dystonia: A systematic review and meta-ananlysis. Mov. Disord. 2012, 27, 1789–1796. [Google Scholar] [CrossRef] [PubMed]
- Contarino, M.F.; Van Den Dool, J.; Balash, Y.; Bhatia, K.; Giladi, N.; Koelman, J.H.; Lokkegaard, A.; Marti, M.J.; Postma, M.; Relja, M.; et al. Clinical Practice: Evidence-Based Recommendations for the Treatment of Cervical Dystonia with Botulinum Toxin. Front. Neurol. 2017, 8, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, S.; Sharma, S. Meige’s syndrome: History, epidemiology, clinical features, pathogenesis and treatment. J. Neurol. Sci. 2017, 372, 162–170. [Google Scholar] [CrossRef]
- Epidemiological Study of Dystonia in Europe (ESDE) Collaborative Group. A prevalence study of primary dystonia in eight European countries. J. Neurol. 2000, 247, 787–792. [Google Scholar] [CrossRef]
- Nutt, J.G.; Muenter, M.D.; Aronson, A.; Kurland, L.T.; Melton, L.J. Epidemiology of focal and generalized dystonia in Rochester, Minnesota. Mov. Disord. 1988, 3, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.B.; Duarte, G.S.; Marques, R.E.; Rodrigues, F.B.; Ferreira, J.; Sampaio, C.; Moore, A.P.; Costa, J. Botulinum toin type A therapy for cervical dystonia. Cochrane Database Syst. Rev. 2020, 11, CD003633. [Google Scholar] [CrossRef]
- Chan, J.; Brin, M.; Fahn, S. Idiopathic cervical dystonia: Clinical characteristics. Mov. Disord. 1991, 6, 119–126. [Google Scholar] [CrossRef]
- Albanese, A.; Bhatia, K.; Bressman, S.B.; Delong, M.R.; Fahn, S.; Fung, V.S.C.; Hallett, M.; Jankovic, J.; Jinnah, H.A.; Klein, C.; et al. Phenomenology and classification of dystonia: A consensus update. Mov. Disord. 2013, 28, 863–873. [Google Scholar] [CrossRef] [Green Version]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jankovic, J.; et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dressler, D.; Saberi, A.; Rosales, R.L. Botulinum toxin therapy of dystonia. J. Neural Transm. 2021, 128, 531–537. [Google Scholar] [CrossRef]
- Tsui, J.K.; Eisen, A.; Stoessl, A.J.; Calne, S.; Calne, D.B. Double-blind study of botulinum toxin in spasmodic torticollis. Lancet 1986, 2, 245–247. [Google Scholar] [CrossRef]
- Kessler, K.R.; Skutta, M.; Benecke, R. German Dystonia Study Group. Long-term treatment of cervical dystonia with botulinum toxin A: Efficacy, safety, and antibody frequency. J. Neurol. 1999, 246, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Mejia, N.I.; Vuong, K.D.; Jankovic, J. Long-term botulinum toxin efficacy, safety, and immunogenicity. Mov. Disord. 2005, 20, 592–597. [Google Scholar] [CrossRef]
- Benecke, P.; Jost, W.H.; Kanovsky, P.; Ruzicka, E.; Comes, G.; Grafe, S. A new botulinum toxin type A free of complexing proteins for treatment of cervical dystonia. Neurology 2005, 64, 1949–1951. [Google Scholar] [CrossRef]
- Brashear, A.; Bergan, K.; Wojcieszek, J.; Siemers, E.R.; Ambrosius, W. Patients’perception of stopping or continuing treatment of cervical dystonia with botulinum toxin type A. Mov. Disord. 2000, 15, 150–153. [Google Scholar] [CrossRef]
- Hsiung, G.Y.; Das, S.K.; Ranawaya, R.; Lafontaine, A.L.; Suchowersky, O. Long-term efficacy of botulinum toxin A in treatment of various movement disorders over a 10-year period. Mov. Disord. 2002, 17, 1288–1293. [Google Scholar] [CrossRef] [PubMed]
- Haussermann, P.; Marczoch, S.; Klinger, C.; Landgrebe, M.; Conrad, B.; Ceballos-Baumann, A. Long-term follow-up of cervical dystonia patients treated with botulinum toxin A. Mov. Disord. 2004, 19, 303–308. [Google Scholar] [CrossRef]
- Skogseid, I.M.; Kerty, E. The course of cervical dystonia and patient satisfaction with long-term botulinum toxin A treatment. Eur. J. Neurol. 2005, 12, 163–170. [Google Scholar] [CrossRef]
- Gill, C.E.; Manus, N.D.; Pelster, M.W.; Cook, J.A.; Title, W.; Molinari, A.L.; Charles, D. Continuation of long-term care for cervical dystonia at an academic movement disorder clinic. Toxins 2013, 5, 776–783. [Google Scholar] [CrossRef] [Green Version]
- Jinnah, H.A.; Comella, C.L.; Perlmutter, J.; Lungu, C.; Hallett, M. Longitudinal studies of botulinum toxin in cervical dystonia: Why do patients discontinue therapy? Toxicon 2018, 147, 89–95. [Google Scholar] [CrossRef]
- Linder-Lucht, M.; Kirschner, J.; Herrmann, J.; Geth, K.; Korinthenberg, R.; Berweck, S.; Heinen, F.; Mall, V. Why do children with cerebral palsy discontinue therapy with botulinum toxin A? Dev. Med. Child Neurol. 2006, 48, 319–320. [Google Scholar]
- Samadzadeh, S.; Brauns, R.; Hefter, H. The Extreme Ends of the Treatment Response Spectrum to Botulinum Toxin in Cervical Dystonia. Toxins 2021, 13, 22. [Google Scholar] [CrossRef]
- Dressler, D. Clinical presentation and management of antibody-induced failure of botulinum toxin therapy. Mov. Disord. 2004, 19 (Supp. Sl), S92–S100. [Google Scholar] [CrossRef]
- Maia, F.M.; Kanashiro, A.K.; Chien, H.F.; Gonçalves, L.R.; Barbosa, E.R. Clinical changes of cervical dystonia pattern in long-term botulinum toxin treated patients. Park. Relat. Disord. 2010, 16, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Hefter, H.; Schomaeker, I.; Schomaecker, M.; Samadzadeh, S. Disease progression of idiopathic cervical dystonia in spite of improvement after botulinum toxin therapy. Front. Neurol. 2020, 11, 588395. [Google Scholar] [CrossRef] [PubMed]
- Bellows, S.; Jankovic, J. Immunogenicity associated with botulinum toxin treatment. Toxins 2019, 11, 491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jinnah, H.A.; Goodmann, E.; Rosen, A.R.; Evatt, M.; Freeman, A.; Factor, S. Botulinum toxin treatment failures in cervical dystonia: Causes, management, and outcomes. J. Neurol. 2016, 263, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Erbguth, F.; Claus, D.; Jaspert, A.; Druschky, A.; Neundorfer, B. Which patients discontinue treatment with botulinum toxin in cervical dystonia? Mov. Disord. 1995, 10, 37. [Google Scholar]
- Hefter, H.; Blondin, D.; Kahlen, U.; Moll, M.; Antoch, G.; Schek, J. CT-guided intramuscular botulinum toxin A injections into the deep anterior neck muscles in patients with pure antecaput or antecollis. Basal Ganglia 2012, 2, 97–101. [Google Scholar] [CrossRef]
- Hefter, H.; Rosenthal, D.; Moll, M. High Botulinum Toxin-Neutralizing Antibody Prevalence Under Long-Term Cervical Dystonia Treatment. Mov. Disord. Clin. Pract. 2016, 3, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Albrecht, P.; Jansen, A.; Lee, J.I.; Moll, M.; Ringelstein, M.; Rosenthal, D.; Bigalke, H.; Aktas, O.; Hartung, H.P.; Hefter, H. High prevalence of neutralizing antibodies after long-term botulinum neurotoxin therapy. Neurology 2019, 92, e48–e54. [Google Scholar] [CrossRef]
- Samadzadeh, S.; Ürer, B.; Brauns, R.; Rosenthal, D.; Lee, J.-I.; Albrecht, P.; Hefter, H. Clinical Implications of Difference in Antigenicity of Different Botulinum Neurotoxin Type A Preparations: Clinical Take-Home Messages from Our Research Pool and Literature. Toxins 2020, 12, 499. [Google Scholar] [CrossRef]
- Lange, O.; Bigalke, H.; Dengler, R.; Wegner, F.; DeGroot, M.; Wohlfarth, K. Neutralizing antibodies and secondary therapy failure after treatment with botulinum toxin type A: Much ado about nothing? Clin. Neuropharmacol. 2009, 32, 213–218. [Google Scholar] [CrossRef]
- Bellows, S.; Jankovic, J. Reply to Comment on Re-Visiting Immunogenicity Associated with Botulinum Toxin Treatment. Toxins 2019, 11, 491. Toxins 2020, 12, 72. [Google Scholar] [CrossRef] [Green Version]
- Sethi, K.D.; Rodriguez, R.; Olayinka, B. Satisfaction with botulinum toxin treatment: A cross-sectional survey of patients with cervical dystonia. J. Med. Econ. 2012, 15, 419–423. [Google Scholar] [CrossRef]
- Jahanshahi, M.; Marion, M.-H.; Marsden, C.D. Natural History of adult-onset idiopathic torticollis. Arch. Neurol. 1990, 47, 548–552. [Google Scholar] [CrossRef]
- Van Zandijke, M. Cervical dystonia (spasmodic torticollis). Some aspects of the natural history. Acta Neurol. Bel. 1995, 95, 210–215. [Google Scholar]
- Greene, P.; Kang, U.J.; Fahn, S. Spread of symptoms in idiopathic torsion dystonia. Mov. Disord. 1995, 10, 143–152. [Google Scholar] [CrossRef]
- Benecke, R.; Moore, P.; Dressler, D.; Naumann, M. Cervical and axial dystonia. In Handbook of Botulinum Toxin Treatment, 2nd ed.; Moore, P., Naumann, M., Eds.; Blackwell Science: Malden, MA, USA, 2003; pp. 158–194. [Google Scholar]
- Lizzarga, K.J.; Al-Shorafat, D.; Fox, S. Update on current and emerging therapies for dystonia. Neurodegener. Dis. Manag. 2019, 9, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Isaias, I.U.; Volkmann, J.; Kupsch, A.; Burgunder, J.M.; Ostrem, J.L.; Alterman, R.L.; Mehdorn, H.M.; Schönecker, T.; Krauss, J.K.; Starr, P.; et al. Factors predicting protracted improvement after pallidal DBS for primary dystonia: The role of age and disease duration. J. Neurol. 2011, 258, 1469–1476. [Google Scholar] [CrossRef]
- Volkmann, J.; Müller, J.; Deuschl, G.; Kühn, A.A.; Krauss, J.K.; Poewe, W.; Timmermann, L.; Falk, D.; Kupsch, A.; Kiviet, A.; et al. Pallidal neurostimulation in patients with mediation-refractory cervical dystonia: A randomized, sham-controlled trial. Lancet Neurol. 2014, 13, 875–884. [Google Scholar] [CrossRef]
- Hefter, H.; Samadzazeh, S.; Rosenthal, D. The impact of the initial severity on later outcome: Retrospective analysis of a large cohort of botulinum toxin naïve patients with idiopathic cervical dystonia. J. Neurol. 2021, 268, 206–213. [Google Scholar] [CrossRef]
- Lowenstein, D.H.; Aminoff, M.J. The clinical course of spasmodic torticollis. Neurology 1988, 38, 530–532. [Google Scholar] [CrossRef]
- Meares, R. Natural history of spasmodic torticollis, and effect of surgery. Lancet 1971, 17, 149–151. [Google Scholar] [CrossRef]
- Mainka, T.; Erro, R.; Rothwell, J.; Kühn, A.A.; Bhatia, K.P.; Ganos, C. Remission in dystonia—Systematic review of the literature and meta-analysis. Parkinsonosm Relat. Disord. 2019, 66, 9–15. [Google Scholar] [CrossRef]
- Hefter, H.; Benecke, R.; Erbguth, F.; Jost, W.; Reichel, G.; Wissel, J. An open-label cohort study of the improvement of quality of life and pain in de novo cervical dystonia patients after injections with 500 U botulinum toxin A (Dysport). BMJ Open 2013, 3, e001853. [Google Scholar] [CrossRef] [Green Version]
- Moll, M.; Rosenthal, D.; Hefter, H. Quality of life in long-term botulinum toxin treatment of cervical dystonia: Results of a cross sectional study. Parkinsonism Relat. Disord. 2018, 57, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Leplow, B.; Böttcher, M.; Schönfeld, R. Botulinum-Toxin-Therapie bei Torticollis spasmodicus. Der Nervenarzt 2013, 84, 493–497. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | RO | CO | DO | ALL | Significance-Level | |
|---|---|---|---|---|---|---|
| n | 16 | 23 | 30 | 74 | ||
| female/male | 9/7 | 19/4 | 18/12 | 49/25 | 0.13; n.s. | |
| AGE (years) | MV/SD | 57.0/8.6 | 61.0/13.3 | 61.1/12.1 | 60.2/11.6 | 0.49; n.s. |
| MIN–MAX | 41.7–76.5 | 28.7–81.3 | 43.4–87.0 | 28.7–87.0 | ||
| AOS (years) | MV/SD | 42.9/11.6 | 48.8/12.5 | 43.6/12.9 | 45.26/12.5 | 0.24; n.s. |
| MIN–MAX | 21.4–61.8 | 26.8–73.4 | 14.7–64.6 | 14.7–73.4 | ||
| DURS (months) | MV/SD | 34.0/29.3 | 46.1/74.0 | 105.2/114.5 | 68.9/91.5 | p < 0.01 |
| MIN–MAX | 3.0–97.0 | 1.0–324.2 | 2.0–438.2 | 1.0-438.2 | ||
| DURT (months) | MV/SD | 144.2/101.6 | 102.3/72.6 | 107.8/71.1 | 115.7/80.3 | 0.25; n.s. |
| MIN–MAX | 11.05–321.2 | 6.1–270.3 | 0.6–282.3 | 0.6–321.2 | ||
| IDOSE (uDU) | MV/SD | 205.2/96.5 | 155.2/62.8 | 160.6/80.1 | 166.3/80.6 | 0.14; n.s. |
| MIN–MAX | 35.0–450.0 | 31.3–300.0 | 75.0–500.0 | 31.3–500.0 | ||
| ADOSE (uDU) | MV/SD | 212.3/112.7 | 212.8/108.5 | 238.8/116.2 | 217.9/114.7 | 0.65; n.s. |
| MIN–MAX | 50.0–450.0 | 40.0–400.0 | 95.0–500.0 | 15.0–500.0 | ||
| INDOSE (uDU) | MV/SD | 7.2/49.9 | 64.8/77.4 | 73.2/100.1 | 50.6/87.2 | p < 0.05 |
| MIN–MAX | −100.0–100.0 | 0.0–275.0 | −50.0–275.0 | −110.0–275.0 | ||
| ITSUI | MV/SD | 9.2/1.8 | 8.3/1.9 | 9.2/3.1 | 8.9/2.4 | 0.75; n.s. |
| MIN–MAX | 8.0–12.0 | 5.0–10.0 | 4.0–13.0 | 4.0–13.0 | ||
| ATSUI | MV/SD | 4.7/3.1 | 4.5/2.5 | 4.2/2.6 | 4.4/2.6 | 0.83; n.s. |
| MIN–MAX | 0.0–10.0 | 0.0–10.0 | 0.0–9.0 | 0.0–10.0 | ||
| IMPTSUI | MV/SD | 4.6/3.1 | 3.7/2.7 | 5.1/5.0 | 3.9/3.8 | 0.37; n.s. |
| MIN–MAX | 0.0–10.0 | 0.0–8.0 | −2.0–13.0 | −2.0–13.0 | ||
| IMPQ | MV/SD | 56.7/30.5 | 35.7/26.4 | 40.8/33.6 | 42.9/31.3 | 0.10; n.s. |
| MIN–MAX | 0.0–90.0 | −20.0–90.0 | −30.0–90.0 | −30.0–90.0 | ||
| IMPD | MV/SD | 66.0/29.9 | 37.0/25.0 | 41.0/35.0 | 46.0/32.0 | p < 0.02 |
| MIN–MAX | 8.0–98.0 | −20.0–75.0 | −30.0–92.0 | −30.0–98.0 | ||
| AGE | AOS | DURS | DURT | IDOSE | ADOSE | INDOSE | ITSUI | ATSUI | IMPQ | IMPD | IMPTSUI | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | . | 0.654 | 0.264 | 0.257 | −0.253 | −0.414 | −0.230 | 0.170 | −0.010 | 0.070 | 0.090 | 0.012 |
| AOS | 0.009 | . | −0.281 | −0.244 | −0.190 | −0.297 | −0.130 | −0.180 | −0.070 | 0.120 | 0.140 | −0.100 |
| DURS | 0.030 | 0.020 | . | 0.242 | −0.180 | −0.200 | −0.210 | 0.150 | 0.220 | −0.230 | −0.230 | −0.090 |
| DURT | 0.030 | 0.040 | 0.050 | . | 0.263 | −0.010 | −0.080 | 0.070 | 0.050 | 0.180 | 0.200 | 0.017 |
| IDOSE | 0.040 | . | . | 0.040 | . | 0.677 | 0.020 | 0.120 | 0.376 | 0.140 | 0.100 | −0.100 |
| ADOSE | 0.009 | 0.020 | . | . | 0.009 | . | 0.652 | 0.080 | 0.497 | 0.030 | −0.040 | −0.018 |
| INDOSE | . | . | . | . | . | 0.009 | . | −0.050 | 0.326 | −0.040 | −0.140 | −0.100 |
| ITSUI | . | . | . | . | . | . | . | . | 0.011 | 0.400 | 0.360 | 0.601 |
| ATSUI | . | . | . | . | 0.009 | 0.009 | 0.010 | . | . | −0.437 | −0.340 | −0.709 |
| IMPQ | . | . | 0.050 | . | . | . | . | . | 0.009 | . | 0.951 | 0.749 |
| IMPD | . | . | . | . | . | . | . | . | 0.010 | 0.009 | . | 0.020 |
| IMPTSUI | . | . | . | . | . | . | . | 0.009 | 0.001 | 0.009 | . | . |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hefter, H.; Schomaecker, I.; Schomaecker, M.; Rosenthal, D.; Samadzadeh, S. The Impact of the Course of Disease before Botulinum Toxin Therapy on the Course of Treatment and Long-Term Outcome in Cervical Dystonia. Toxins 2021, 13, 493. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070493
Hefter H, Schomaecker I, Schomaecker M, Rosenthal D, Samadzadeh S. The Impact of the Course of Disease before Botulinum Toxin Therapy on the Course of Treatment and Long-Term Outcome in Cervical Dystonia. Toxins. 2021; 13(7):493. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070493
Chicago/Turabian StyleHefter, Harald, Isabelle Schomaecker, Max Schomaecker, Dietmar Rosenthal, and Sara Samadzadeh. 2021. "The Impact of the Course of Disease before Botulinum Toxin Therapy on the Course of Treatment and Long-Term Outcome in Cervical Dystonia" Toxins 13, no. 7: 493. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070493