Dental Implant Failure Rate and Marginal Bone Loss in Transplanted Patients: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
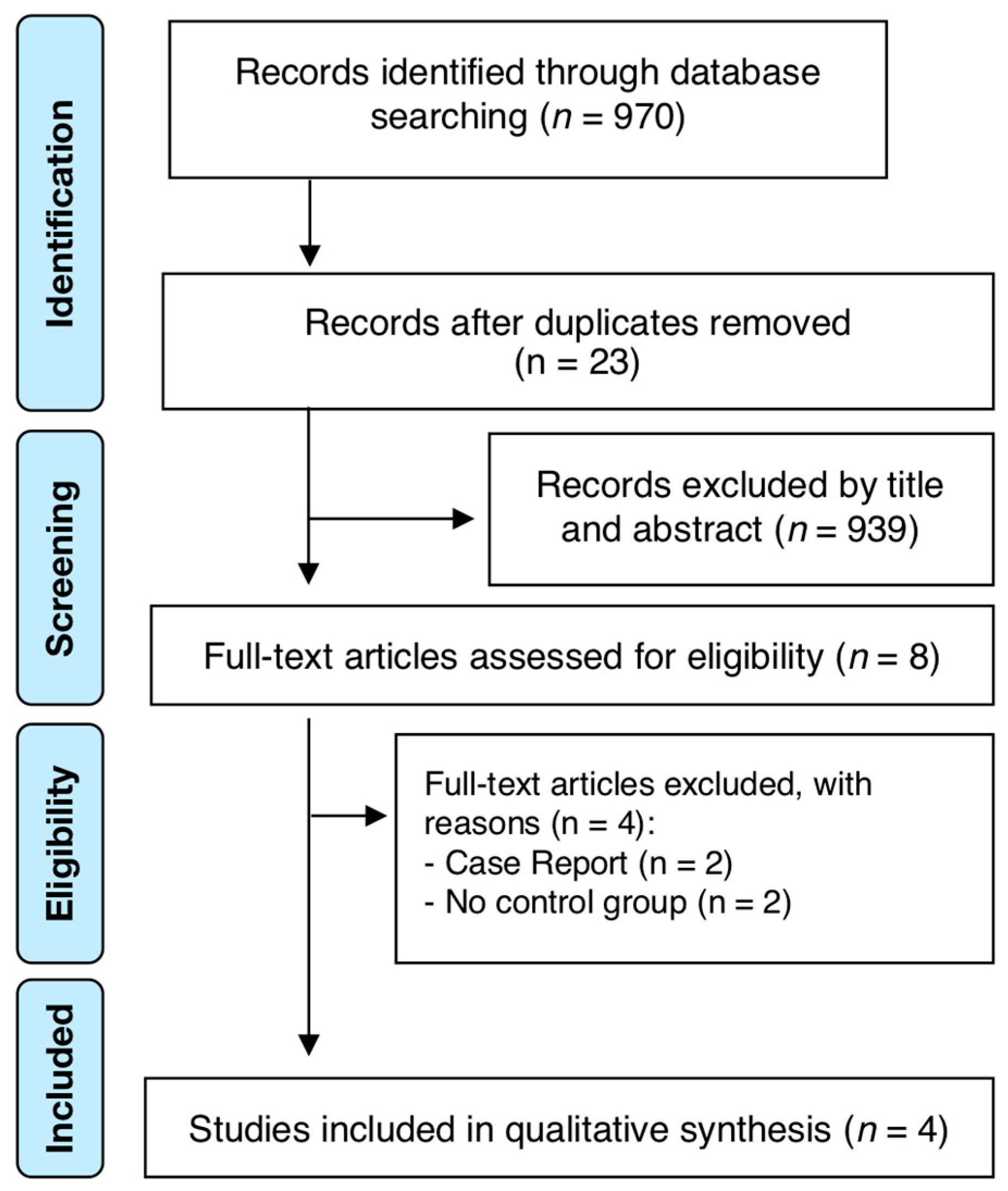
2. Materials and Methods
2.1. Protocol and Registration
2.2. Focus Question and Eligibility Criteria
- P (Population): Solid-organ transplanted adult humans (≥18 years old).
- I (Intervention): Dental implant placement.
- C (Comparator): Adult healthy controls.
- O (Outcome): Implant failure rate and marginal bone loss.
- Randomized clinical trials (RCTs) and non-RCTs (retrospective and prospective case-control and cohort studies)
- Studies reporting implant survival, or otherwise failure, in transplanted patients, with or without non-transplanted patients as reference
- Studies reporting marginal bone loss data
- Defined SOT patients
- Studies reporting follow-up period of placed dental implants
- Studies with follow-ups of at least 6 months after placement of the dental implant.
2.3. Search Strategy
2.4. Study Process
2.5. Risk of Bias (RoB) in Individual Studies
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Risk of Bias (RoB) in Individual Studies
3.3. Synthesis of Results
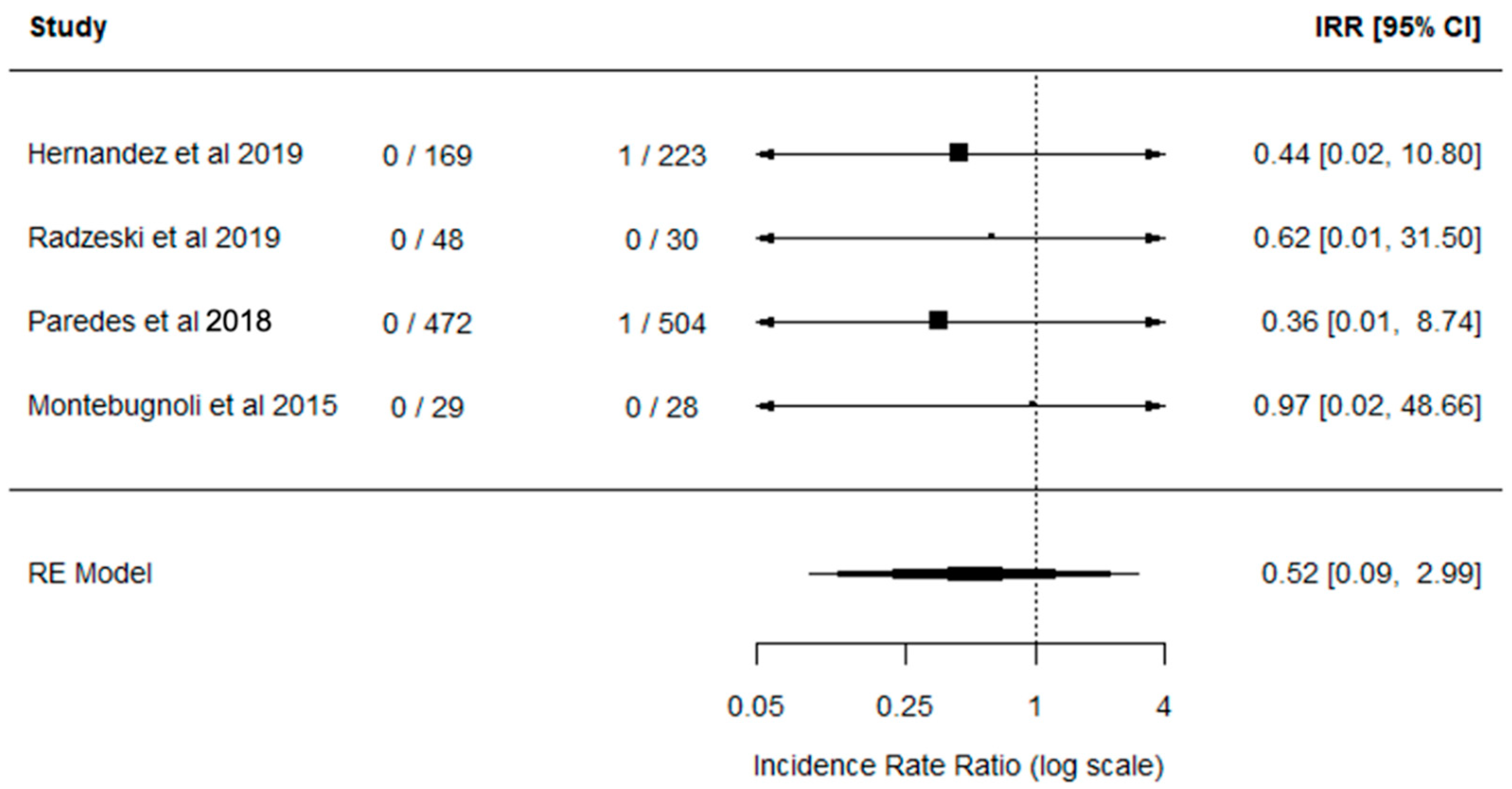
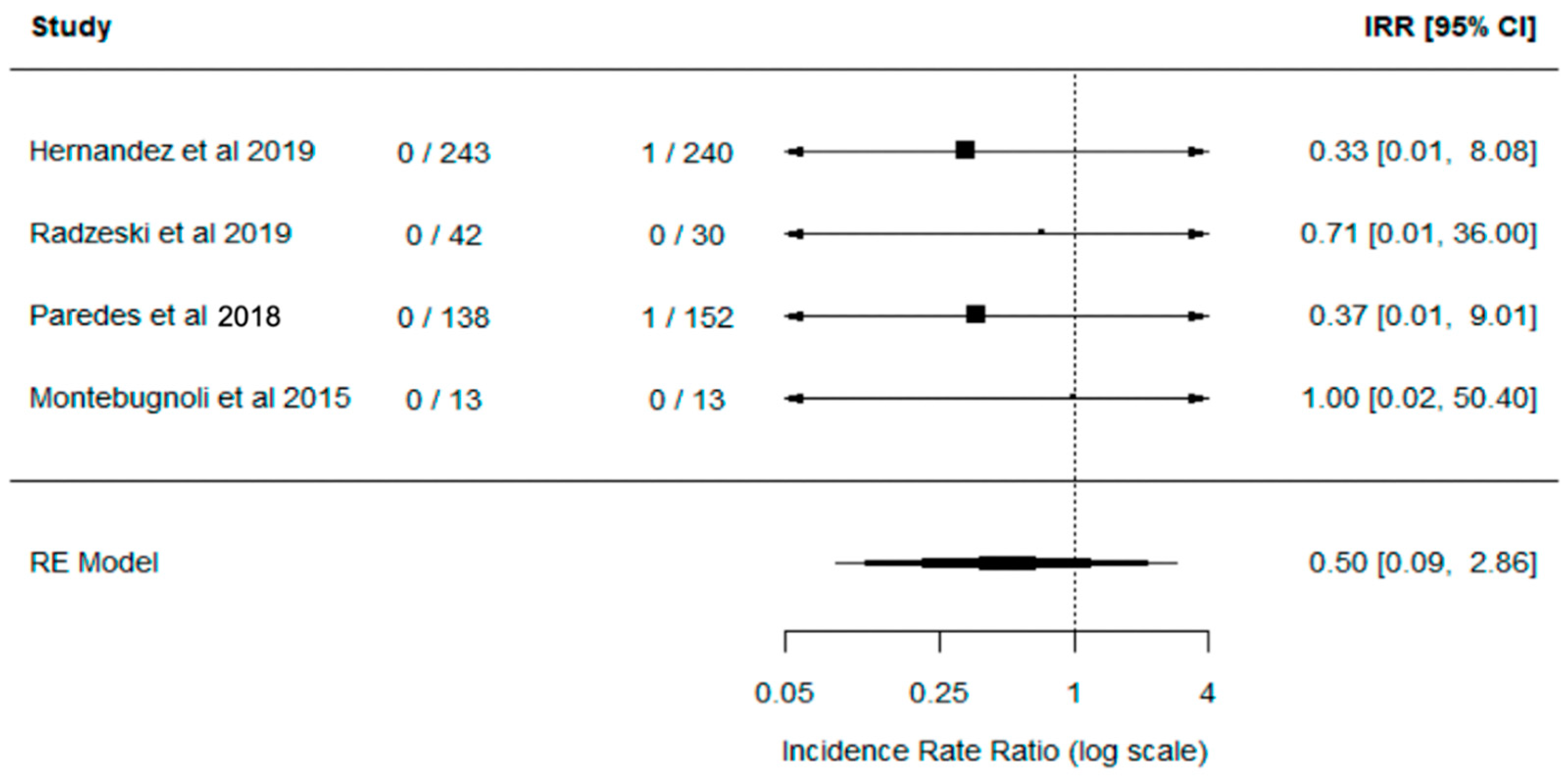
3.3.1. Implant Failure Rate
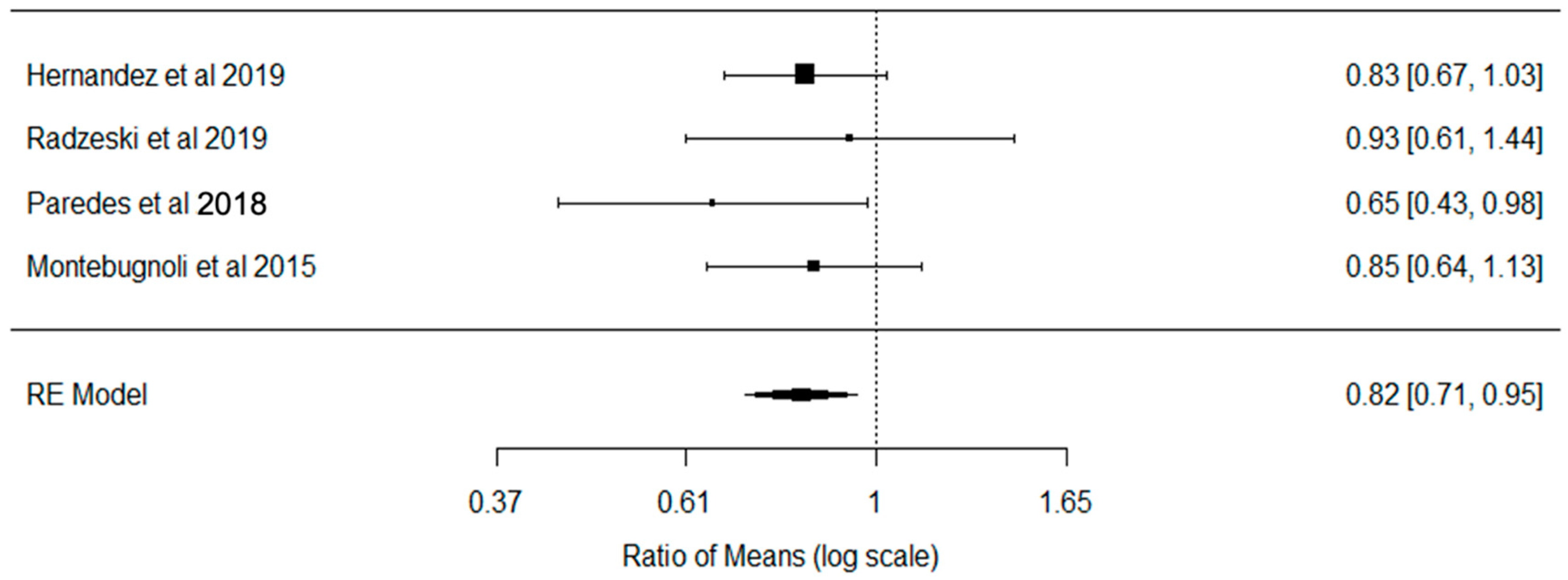
3.3.2. Marginal Bone Loss
4. Discussion
4.1. Summary of Main Findings
4.2. Quality of the Evidence, Limitations, and Potential Biases in the Review Process
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Jung, R.E.; Zembic, A.; Pjetursson, B.E.; Zwahlen, M.; Thoma, D.S. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin. Oral Implant. Res. 2012, 23, 2–21. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin. Oral Implant. Res. 2012, 23, 22–38. [Google Scholar] [CrossRef] [PubMed]
- Hjalmarsson, L.; Gheisarifar, M.; Jemt, T. A systematic review of survival of single implants as presented in longitudinal studies with a follow-up of at least 10 years. Eur. J. Oral Implantol. 2016, 9, S155–S162. [Google Scholar] [PubMed]
- Bornstein, M.M.; Cionca, N.; Mombelli, A. Systemic conditions and treatments as risks for implant therapy. Int. J. Oral Maxillofac. Implant. 2009, 24, 12–27. [Google Scholar]
- Roos-Jansaker, A.-M.; Lindahl, C.; Renvert, H.; Renvert, S. Nine- to fourteen-year follow-up of implant treatment. Part II: Presence of peri-implant lesions. J. Clin. Periodontol. 2006, 33, 290–295. [Google Scholar]
- Diz, P.; Scully, C.; Sanz, M. Dental implants in the medically compromised patient. J. Dent. 2013, 41, 195–206. [Google Scholar] [CrossRef]
- Scully, C.; Hobkirk, J.; Dios, P.D. Dental endosseous implants in the medically compromised patient. J. Oral Rehabil. 2007, 34, 590–599. [Google Scholar] [CrossRef]
- Heckmann, S.M.; Heckmann, J.G.; Linke, J.J.; Hohenberger, W.; Mombelli, A. Implant Therapy Following Liver Transplantation: Clinical and Microbiological Results After 10 Years. J. Periodontol. 2004, 75, 909–913. [Google Scholar] [CrossRef]
- Mombelli, A.; Cionca, N. Systemic diseases affecting osseointegration therapy. Clin. Oral Implant. Res. 2006, 17, 97–103. [Google Scholar] [CrossRef]
- Guggenheimer, J.; Eghtesad, B.; Stock, D.J. Dental management of the (solid) organ transplant patient. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2003, 95, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Hernández, G.; Jiménez, C.; Arriba, L.; Moreno, E.; Lucas, M. Resolution of oral ulcerations after decreasing the dosage of tacrolimus in a liver transplantation recipient. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2001, 92, 526–531. [Google Scholar] [CrossRef] [PubMed]
- GODT 2016. Available online: http://www.transplant-observatory.org/download/2016-activity-data-report/ (accessed on 2 June 2020).
- Kritikos, A.; Manuel, O. Bloodstream infections after solid-organ transplantation. Virulence 2016, 7, 329–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fishman, J.A. Infection in Organ Transplantation. Am. J. Transpl. 2017, 17, 856–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Severe Periodontitis in 1990–2010. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef]
- Machado, V.; Botelho, J.; Lopes, J.; Patrão, M.; Alves, R.; Chambrone, L.; Alcoforado, G.; Mendes, J.J. Periodontitis impact in interleukin-6 serum levels in solid organ transplanted patients: A systematic review and meta-analysis. Diagnostics 2020, 10, 184. [Google Scholar] [CrossRef] [Green Version]
- De Molon, R.S.; Sakakura, C.E.; Faeda, R.S.; Sartori, R.; Palhares, D.; Margonar, R.; Marcantonio, E. Effect of the long-term administration of Cyclosporine A on bone healing around osseointegrated titanium implants: A histomorphometric study in the rabbit tibia. Microsc. Res. Tech. 2017, 80, 1000–1008. [Google Scholar] [CrossRef]
- Duarte, P.M.; Filho, G.R.N.; Sallum, E.A.; de Toledo, S.; Sallum, A.W.; Nociti, F.H. The Effect of an Immunosuppressive Therapy and Its Withdrawal on Bone Healing Around Titanium Implants. A Histometric Study in Rabbits. J. Periodontol. 2001, 72, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- Sakakura, C.E.; Margonar, R.; Holzhausen, M.; Nociti, F.H.; Alba, R.C.; Marcantonio, E. Influence of Cyclosporin A Therapy on Bone Healing Around Titanium Implants: A Histometric and Biomechanic Study in Rabbits. J. Periodontol. 2003, 74, 976–981. [Google Scholar] [CrossRef]
- Sakakura, C.E.; Margonar, R.; Sartori, R.; Morais, J.A.N.D.; Marcantonio, E. The Influence of Cyclosporin A on Mechanical Retention of Dental Implants Previously Integrated to the Bone: A Study in Rabbits. J. Periodontol. 2006, 77, 2059–2062. [Google Scholar] [CrossRef]
- López-Pintor, R.M.; Hernández, G.; de Arriba, L.; de Andrés, A. Lip cancer in renal transplant patients. Oral Oncol. 2011, 47, 68–71. [Google Scholar] [CrossRef]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J. Clin. Periodontol. 2018, 45, S278–S285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patini, R.; Staderini, E.; Lajolo, C.; Lopetuso, L.; Mohammed, H.; Rimondini, L.; Rocchetti, V.; Franceschi, F.; Cordaro, M.; Gallenzi, P. Relationship between oral microbiota and periodontal disease: A systematic review. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 5775–5788. [Google Scholar] [PubMed]
- Staderini, E.; Patini, R.; Guglielmi, F.; Camodeca, A.; Gallenzi, P. How to Manage Impacted Third Molars: Germectomy or Delayed Removal? A Systematic Literature Review. Med. (B. Aires) 2019, 55, 79. [Google Scholar]
- Cajanding, R. Immunosuppression following organ transplantation. Part 2: Complications and their management. Br. J. Nurs. 2018, 27, 1059–1065. [Google Scholar]
- Gu, L.; Yu, Y.C. Clinical outcome of dental implants placed in liver transplant recipients after 3 years: A case series. Transplant. Proc. 2011, 43, 2678–2682. [Google Scholar] [CrossRef] [PubMed]
- Paredes, V.; López-Pintor, R.M.; Torres, J.; de Vicente, J.C.; Sanz, M.; Hernández, G. Implant treatment in pharmacologically immunosuppressed liver transplant patients: A prospective-controlled study. Clin. Oral Implant. Res. 2018, 29, 28–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández, G.; Paredes, V.; López-Pintor, R.M.; de Andrés, A.; de Vicente, J.C.; Sanz, M. Implant treatment in immunosuppressed renal transplant patients: A prospective case-controlled study. Clin. Oral Implant. Res. 2019, 30, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Montebugnoli, L.; Venturi, M.; Cervellati, F. Bone response to submerged implants in organ transplant patients: A prospective controlled study. Int. J. Oral Maxillofac. Implant. 2012, 27, 1494–1500. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6. [Google Scholar] [CrossRef]
- Radzewski, R.; Osmola, K. The use of dental implants in organ transplant patients undergoing immunosuppressive therapy: An overview of publications. Implant Dent. 2016, 25, 541–546. [Google Scholar] [CrossRef]
- Montebugnoli, L.; Venturi, M.; Cervellati, F.; Servidio, D.; Vocale, C.; Pagan, F.; Landini, M.P.; Magnani, G.; Sambri, V. Peri-Implant Response and Microflora in Organ Transplant Patients 1 Year after Prosthetic Loading: A Prospective Controlled Study. Clin. Implant Dent. Relat. Res. 2015, 17, 972–982. [Google Scholar] [CrossRef] [PubMed]
- Howe, M.S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Moraschini, V.; Poubel, L.A.D.C.; Ferreira, V.F.; Barboza, E.D.S.P. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Duttenhoefer, F.; Fuessinger, M.A.; Beckmann, Y.; Schmelzeisen, R.; Groetz, K.A.; Boeker, M. Dental implants in immunocompromised patients: A systematic review and meta-analysis. Int. J. Implant Dent. 2019, 5, 1–12. [Google Scholar] [CrossRef]
- Patini, R.; Staderini, E.; Camodeca, A.; Guglielmi, F.; Gallenzi, P. Case Reports in Pediatric Dentistry Journals: A Systematic Review about Their Effect on Impact Factor and Future Investigations. Dent. J. 2019, 7, 103. [Google Scholar] [CrossRef] [Green Version]
- Anderson-Smits, C.; Baker, E.R.; Hirji, I. Coinfection rates and clinical outcome data for cytomegalovirus and Epstein-Barr virus in post-transplant patients: A systematic review of the literature. Transpl. Infect. Dis. 2020, 1–14. [Google Scholar] [CrossRef]
- Akram, Z.; Al-Aali, K.A.; Alrabiah, M.; Alonaizan, F.A.; Abduljabbar, T.; AlAhmari, F.; Javed, F.; Vohra, F. Current weight of evidence of viruses associated with peri-implantitis and peri-implant health: A systematic review and meta-analysis. Rev. Med. Virol. 2019, 29, e2042. [Google Scholar] [CrossRef]
- Gonçalves, P.F.; Filho, G.D.R.N.; Sallum, E.A.; Sallum, A.W.; Junior, F.H.N. Immunosuppressant therapy and bone loss in ligature-induced periodontitis: A study in rats. Pesqui. Odontolog. Bras. 2003, 17, 46–50. [Google Scholar] [CrossRef] [Green Version]
- Duarte, P.M.; Filho, G.R.N.; Sallum, E.A.; Sallum, A.W.; Júnior, F.H.N. Short-term immunosuppressive therapy does not affect the density of the pre-existing bone around titanium implants placed in rabbits. Pesqui. Odontolog. Bras. 2003, 17, 362–366. [Google Scholar] [CrossRef] [Green Version]
- Sivakumar, I.; Arunachalam, S.; Choudhary, S.; Buzayan, M.M. Does HIV infection affect the survival of dental implants? A systematic review and meta-analysis. J. Prosthet. Dent. 2020, 1–8. [Google Scholar] [CrossRef]
- Alsaadi, G.; Quirynen, M.; Komárek, A.; van Steenberghe, D. Impact of local and systemic factors on the incidence of late oral implant loss. Clin. Oral Implant. Res. 2008, 19, 670–676. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) (Country) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Score (Risk of Bias) |
|---|---|---|---|---|---|---|---|---|---|
| Hernández et al. (2019) (Spain) [28] | a | a | a | a | a/b | b | a | a | 9 (Low) |
| Radzewski and Osmola (2019) (Poland) [31] | d | c | a | a | a/b | b | a | a | 7 (Low) |
| Paredes et al. (2018) (Spain) [27] | a | a | a | a | a/b | b | a | a | 9 (Low) |
| Montebugnoli et al. (2015) (Italy) [32] | c | c | a | a | a/b | b | a | a | 7 (Low) |
| Study | Effect Size | SOT Sample | Control | Exclusion Criteria | Clinical Environment | Immunotherapy | Implant Characteristics | Implant Follow-Up | Outcome | Funding Sources |
|---|---|---|---|---|---|---|---|---|---|---|
| Hernández et al. (2019) (Spain) [28] | Implant failure incidence rate and MBL | 25 partially edentulous Renal SOT who received 79 dental implants | 28 matched controls who received 86 dental implants | Suffering from untreated periodontitis, being smokers, or having a medical history of radiotherapy, severe or uncontrolled metabolic diseases, or lack of compliance. | Private practice | Prednisone, Tacrolimus + Mycophenolate Mofetil (15 patients) Prednisone, Cyclosporine A + Mycophenolate Mofetil (9 patients) Prednisone, Cyclosporine A + Azathioprine (2 patients) Prednisone + Tacrolimus or Prednisone plus Cyclosporine A (2 patients) | Ti Unite, Nobel Biocare 3.75/4.00 or 5.00 mm diameter and 8/8.5/10/11.5/13 or 15 mm length | Mean follow-up of 9.7 years | Implant survival rate was over 98% in both test and control groups. Slightly increased marginal bone loss in the control group. | Dentaid S. L. provided partial support |
| Radzewski and Osmola (2019) (Poland) [31] | Implant failure incidence rate and MBL | 21 organ transplant immunosuppressed patients (Kidney, Pancreas, and Liver) who received 24 dental implants | 15 matched controls who received 15 dental implants | Patients with active periodontal disease, substantial occlusion disorders, bone diseases, blood coagulation disorders, untreated dyslipidemia, or were a smoker. | University based | Tacrolimus (majority) or Cyclosporine, Sirolimus, or Mycophenolate Mofetill, Sirolimus (12 patients) | Naturactis; ETK, Sallanches, France | 2 years | Implant stability and bone loss were not any different from those in healthy people. | N/A |
| Paredes et al. (2018) (Spain) [27] | Implant failure incidence rate and MBL | 14 pharmacologically immunosuppressed Liver TP with 48 dental implants | 16 matched controls who received 53 dental implants | Suffering from active periodontitis, being smokers, or having a medical history of radiotherapy, severe or uncontrolled metabolic diseases, or lack of compliance. | Private practice | Prednisone + Cyclosporin A + Azathioprine (2 patients) Prednisone + Cyclosporin A + Mycophenolate Mofetil (5 patients) Prednisone + Tacrolimus + Mycophenolate Mofetil (8 patients) Prednisone + Cyclosporin A (1 patient) | Ti Unite ®; Nobel Biocare S.A., Gothenburg, Sweden 3.75, 4, & 5 mm diameter | Mean follow-up of +8 years | 100% implant survival in liver transplant patients after the pharmacological immunosuppression | Dentaid S. L. provided partial support |
| Montebugnoli et al. (2015) (Italy) [32] | MBL | 13 organ-transplanted (11 hearts, two livers) patients who received 29 submerged dental implants | 15 matched controls who received 15 dental implants | Previous irradiation of the head and neck region, alcohol or drug abuse, or psychiatric disorders that made it difficult to obtain informed consent, severe bruxism or clenching habits, smoking, and cyclosporine-induced gingival overgrowth. | University based | Cyclosporin (11 patients) and Tacrolimus (2 patients) | Standard tapered implants with anodized surfaces (NobelReplace Tapered Groovy, Nobel Biocare AB, Gothenburg, Sweden). +3.5 mm diameter and +8 mm length | 1 year | Implant failure and bone loss were equivalent to those in control | No funding |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paraizo, M.; Botelho, J.; Machado, V.; Mendes, J.J.; Alves, R.; Mascarenhas, P.; Cardoso, J.M. Dental Implant Failure Rate and Marginal Bone Loss in Transplanted Patients: A Systematic Review and Meta-Analysis. Transplantology 2020, 1, 85-96. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology1020008
Paraizo M, Botelho J, Machado V, Mendes JJ, Alves R, Mascarenhas P, Cardoso JM. Dental Implant Failure Rate and Marginal Bone Loss in Transplanted Patients: A Systematic Review and Meta-Analysis. Transplantology. 2020; 1(2):85-96. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology1020008
Chicago/Turabian StyleParaizo, Marcela, João Botelho, Vanessa Machado, José João Mendes, Ricardo Alves, Paulo Mascarenhas, and José Maria Cardoso. 2020. "Dental Implant Failure Rate and Marginal Bone Loss in Transplanted Patients: A Systematic Review and Meta-Analysis" Transplantology 1, no. 2: 85-96. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology1020008