
Persistent Neutropenia after ABOi Kidney Transplantation: A Case Report

 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
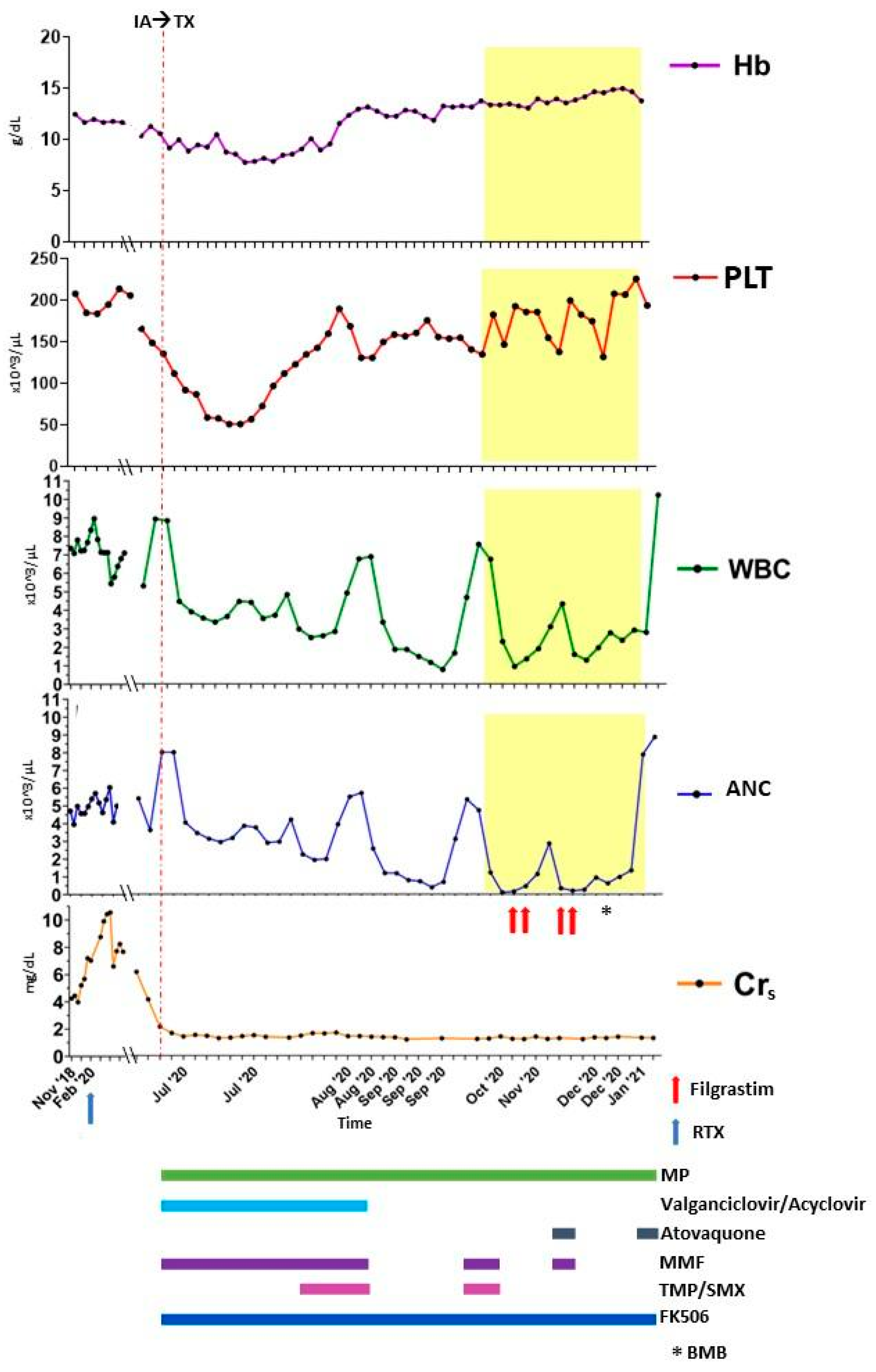
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zafrani, L.; Truffaut, L.; Kreis, H.; Etienne, D.; Rafat, C.; Lechaton, S.; Anglicheau, D.; Zuber, J.; Ciroldi, M.; Thervet, E.; et al. Incidence, risk factors and clinical consequences of neutropenia following kidney transplantation: A retrospective study. Am. J. Transpl. 2009, 9, 1816–1825. [Google Scholar] [CrossRef] [PubMed]
- Alraddadi, B.; Nierenberg, N.E.; Price, L.L.; Chow, J.K.; Poutsiaka, D.D.; Rohrer, R.J.; Cooper, J.T.; Freeman, R.B.; Snydman, D.R. Characteristics and outcomes of neutropenia after orthotopic liver transplantation. Liver Transpl. 2016, 22, 217–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosengarten, D.; Fakterman, M.; Raviv, Y.; Rusanov, V.; Fox, B.; Kramer, M. Neutropenia Following Lung Transplantation. J. Hear Lung Transplant. 2015, 34, S255. [Google Scholar] [CrossRef]
- Chow, J.K.; Ruthazer, R.; Boucher, H.W.; Nierenberg, N.; Vest, A.R.; DeNofrio, D.; Snydman, D.R. Factors Associated with Neutropenia Post-Heart Transplantation. J. Hear Lung Transpl. 2020, 39, S482. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/pii/S1053249820300577 (accessed on 15 May 2021). [CrossRef]
- Hartmann, E.L.; Gatesman, M.; Roskopf-Somerville, J.; Stratta, R.; Farney, A.; Sundberg, A. Management of leukopenia in kidney and pancreas transplant recipients. Clin. Transplant. 2008, 22, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Rose-Felker, K.; Mukhtar, A.; Kelleman, M.S.; Deshpande, S.R.; Mahle, W.T. Neutropenia in pediatric heart transplant recipients. Pediatr. Transpl. 2018, 22, e13130. [Google Scholar] [CrossRef]
- Barry, M.; Chandra, S.; Hymes, K.B. Principles and Practice of Transplant Infectious Diseases. Princ. Pract. Transpl. Infect. Dis. 2019, 10, 199–207. [Google Scholar]
- Brum, S.; Nolasco, F.; Sousa, J.; Ferreira, A.; Possante, M.; Pinto, J.R.; Barroso, E.; Santos, J.R. Leukopenia in Kidney Transplant Patients with the Association of Valganciclovir and Mycophenolate Mofetil. Transpl. Proc. 2008, 40, 752–754. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/pii/S0041134508001577 (accessed on 15 May 2021). [CrossRef]
- Keisu, M.; Wiholm, B.-E.; Palmblad, J. Trimethoprim-sulphamethoxazole-associated blood dyscrasias. Ten years’ experience of the Swedish spontaneous reporting system. J. Intern. Med. 1990, 228, 353–360. [Google Scholar] [CrossRef]
- Newburger, P.E.; Dale, D.C. Evaluation and Management of Patients with Isolated Neutropenia. Semin Hematol. 2013, 50, 198–206. [Google Scholar] [CrossRef] [Green Version]
- Martín-Gandul, C.; Pérez-Romero, P.; González-Roncero, F.M.; Berdaguer, S.; Gómez, M.A.; Lage, E.; Sánchez, M.; Cisneros, J.M.; Cordero, E. Clinical impact of neutropenia related with the preemptive therapy of CMV infection in solid organ transplant recipients. J. Infect. 2014, 69, 500–506. [Google Scholar] [CrossRef]
- Gladziwa, U.; Hermans, M.M.H.; Naami, A.; Maastricht, A.H. Unexpected rate of severe leucopenia with the association of mycophenolate mofetil and valganciclovir in kidney transplant recipients. Nephrol. Dial. Transplant. 2007, 22, 671–672. [Google Scholar]
- Hong, J.C.; Kahan, B.D. Sirolimus-Induced Thrombocytopenia and Leukopenia in Renal Transplant Recipients: Risk Factors, Incidence, Progression, and Management. Transplantation 2000, 69, 2085–2090. [Google Scholar] [CrossRef] [PubMed]
- De Rycke, A.; Dierickx, D.; Kuypers, D.R. Tacrolimus-induced neutropenia in renal transplant recipients. Clin. J. Am. Soc. Nephrol. 2011, 6, 690–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clément, J.; Taton, B.; Merville, P.; Viallard, J.F.; Lazaro, E.; Couzi, L.; Rivière, E. Two cases of tacrolimus-induced neutropenia: A probably diagnosed cause of neutropenia after solid-organ transplantation. Clin. Transplant. 2018, 32, e13295. [Google Scholar] [CrossRef] [PubMed]
- Boxer, L.A.; Bolyard, A.A.; Marrero, T.M.; Tran, E.L.; Bonilla, M.A.; Newburger, P.E.; Dale, D.C. Is There a Role for Anti-Neutrophil Antibody Testing in Predicting Spontaneous Resolution of Neutropenia in Young Children. Blood 2015, 126, 2211. [Google Scholar] [CrossRef]
- Akhtari, M.; Curtis, B.; Waller, E.K. Autoimmunity Reviews Autoimmune neutropenia in adults. Autoimmun. Rev. 2009, 9, 62–66. [Google Scholar] [CrossRef]
- Chang, M.Y.; Lin, S.F.; Wu, S.C.; Yang, W.C. Myelodysplastic syndrome: The other cause of anemia in end-stage renal disease patients undergoing dialysis. Sci. Rep. 2020, 10, 1–9. [Google Scholar]
- Weng, C.H.; Lu, K.Y.; Hu, C.C.; Huang, W.H.; Wang, I.K.; Yen, T.H. Bone Marrow Pathology Predicts Mortality in Chronic Hemodialysis Patients. BioMed Res. Int. 2015, 2015, 160382. [Google Scholar] [CrossRef]
- Brown, A.E. Neutropenia, Fever, and Infection. Am. J. Med. 1984, 76, 421–428. [Google Scholar] [CrossRef]
- Knoll, G.A.; MacDonald, I.; Khan, A.; Van Walraven, C. Mycophenolate mofetil dose reduction and the risk of acute rejection after renal transplantation. J. Am. Soc. Nephrol. 2003, 14, 2381–2386. [Google Scholar] [CrossRef] [Green Version]
- Schmaldienst, S.; Bekesi, G.; Deicher, R.; Franz, M.; Hörl, W.H.; Pohanka, E. Recombinant human granulocyte colony-stimulating factor after kidney transplantation: A retrospective analysis to evaluate the benefit or risk of immunostimulation. Transplantation 2000, 69, 527–531. [Google Scholar] [CrossRef]
- Davidson, M.; Min, Y.I.; Holbrook, J.T.; Van Natta, M.L.; Murphy, R.; Jabs, D.A.; Welch, W.; Meinert, C.L. Use of filgrastim as adjuvant therapy in patients with AIDS-related cytomegalovirus retinitis. AIDS 2002, 16, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Kuritzkes, D.R.; Parenti, D.; Ward, D.J.; Rachlis, A.; Wong, R.J.; Mallon, K.P.; Rich, W.J.; Jacobson, M.A. Filgrastim prevents severe neutropenia and reduces infective morbidity in patients with advanced HIV infection: Results of a randomized, multicenter, controlled trial. Aids 1998, 12, 65–74. [Google Scholar] [CrossRef]
- Gregorini, M.; Castello, M.; Rampino, T.; Bosio, F.; Bedino, G.; Esposito, P.; Borroni, G.; Dal Canton, A. GM-CSF contributes to prompt healing of ecthyma gangrenosum lesions in kidney transplant recipient. J. Nephrol. 2012, 25, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Meier-Kriesche, H.U.; Shaw, L.M.; Korecka, M.; Kaplan, B. Pharmacokinetics of mycophenolic acid in renal insufficiency. Ther. Drug Monit. 2000, 22, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, B.; Meier-Kriesche, H.U.; Friedman, G.; Mulgaonkar, S.; Gruber, S.; Korecka, M.; Brayman, K.L.; Shaw, L.M. The effect of renal insufficiency on mycophenolic acid protein binding. J. Clin. Pharmacol. 1999, 39, 715–720. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andenna, G.G.; Gregorini, M.; Elena, C.; Fusi, M.; Colangelo, R.; Pattonieri, E.F.; Grignano, M.A.; Libetta, C.; Rampino, T. Persistent Neutropenia after ABOi Kidney Transplantation: A Case Report. Transplantology 2021, 2, 183-190. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2020017
Andenna GG, Gregorini M, Elena C, Fusi M, Colangelo R, Pattonieri EF, Grignano MA, Libetta C, Rampino T. Persistent Neutropenia after ABOi Kidney Transplantation: A Case Report. Transplantology. 2021; 2(2):183-190. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2020017
Chicago/Turabian StyleAndenna, Gabriele Gualtiero, Marilena Gregorini, Chiara Elena, Miriam Fusi, Rosa Colangelo, Eleonora Francesca Pattonieri, Maria Antonietta Grignano, Carmelo Libetta, and Teresa Rampino. 2021. "Persistent Neutropenia after ABOi Kidney Transplantation: A Case Report" Transplantology 2, no. 2: 183-190. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2020017