Efficacy and Safety of Lopinavir/Ritonavir for Treatment of COVID-19: A Systematic Review and Meta-Analysis

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Aim of the Study
3. Methods
3.1. Search Strategy and Selection Criteria
3.2. Inclusion Criteria
3.3. Participants
3.4. Intervention
3.5. Objectives
- Virological cure on day 7 after initiation of therapy (+ve to −ve polymerase chain reaction (PCR): non-detection of SARS-CoV-2 in nasopharyngeal swab).
- Clinical cure (time to body temperature normalization and time to cough relief).
- Radiological progression during drug treatment.
- Mortality at 28 days and death during treatment at any time.
- Safety and tolerability of lopinavir/ritonavir.
3.6. Comparisons
- lopinavir/ritonavir vs. no antiviral therapy (conventional therapy)/control.
- lopinavir/ritonavir in combination with other agents versus conventional therapy/control.
3.7. Searching Keywords
3.8. Exclusion Criteria
3.9. Data Extraction and Analysis
3.10. Risk of Biased Evaluation of Included Studies
3.11. Assessment of Heterogeneity
3.12. Statistical Analysis
4. Results
4.1. Comparison 1: Efficacy and Safety of Lopinavir-Ritonavir (LPV/RTV) versus No Antiviral Therapy (Conventional Therapy) or Control
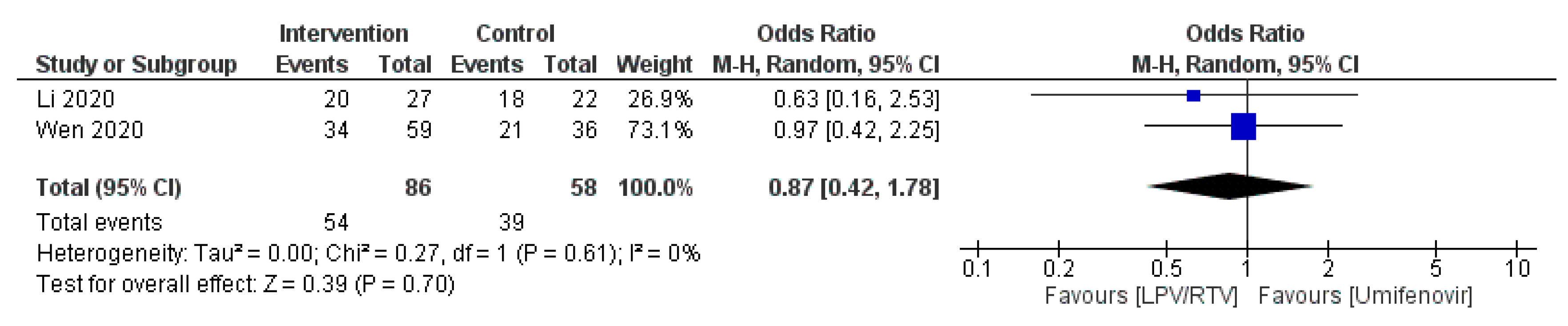
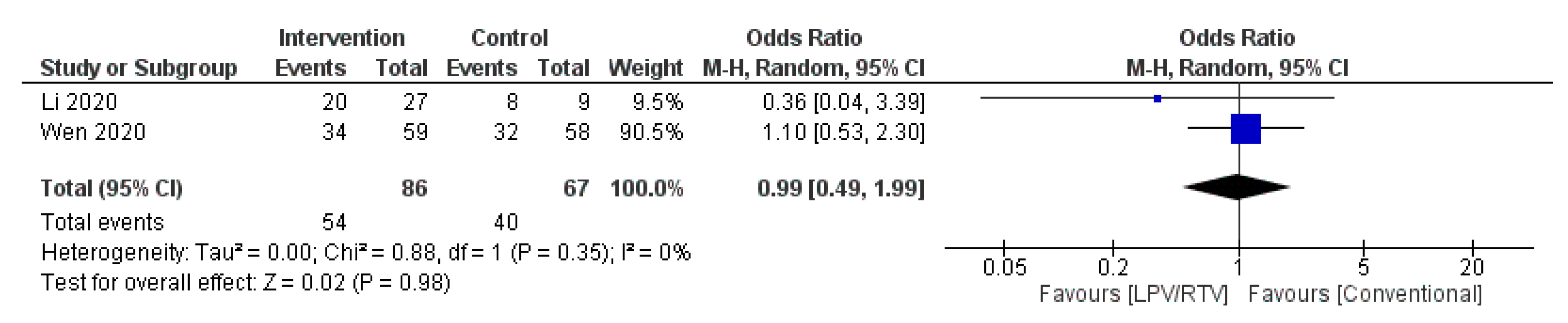
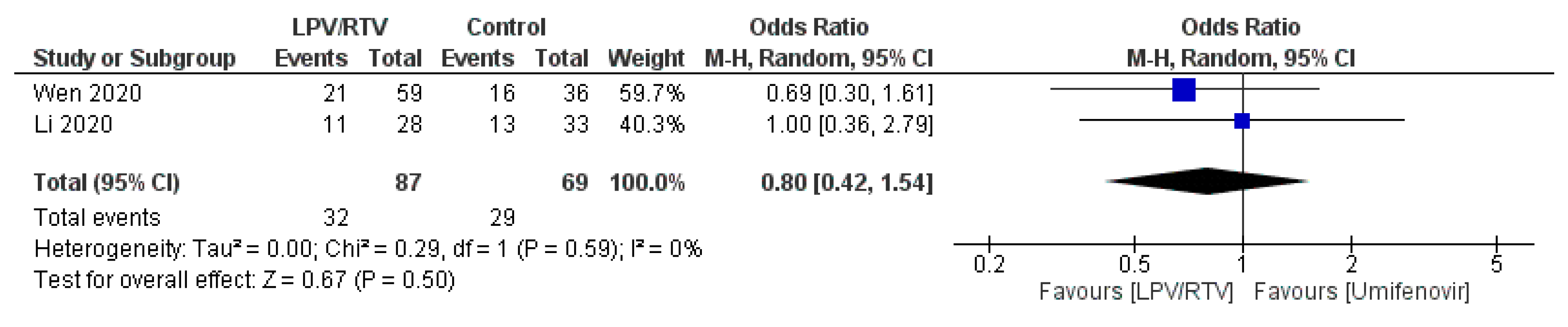
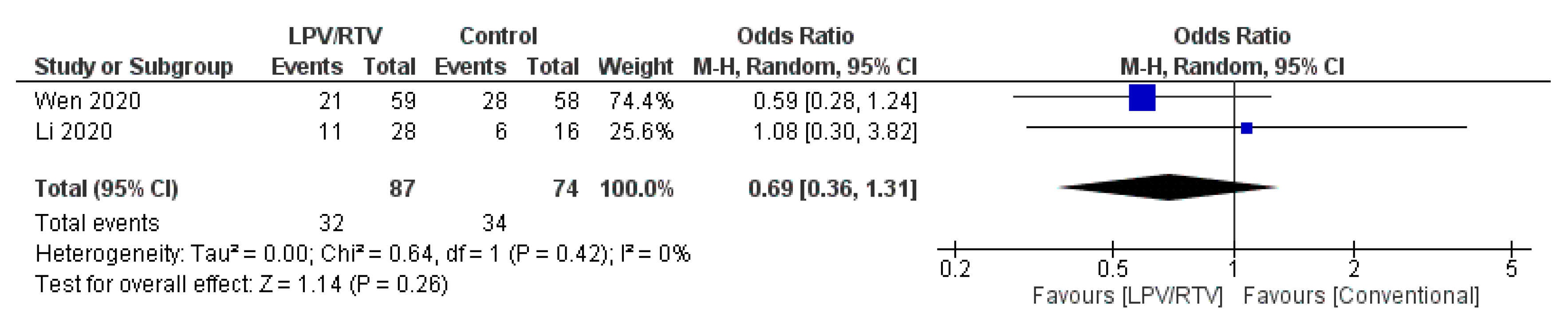
4.1.1. Virological Cure on Day 7 Post-Initiation of Therapy (+ve to −ve PCR: Non-Detection of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in Nasopharyngeal Swab)
LPV/RTV vs. Umifenovir: Virologic Cure at Day 7 Post-Initiation of Therapy
4.1.2. Clinical Cure (Time to Body Temperature Normalization and Time to Cough Relief)
Time to Body Temperature Normalization
Duration of Cough
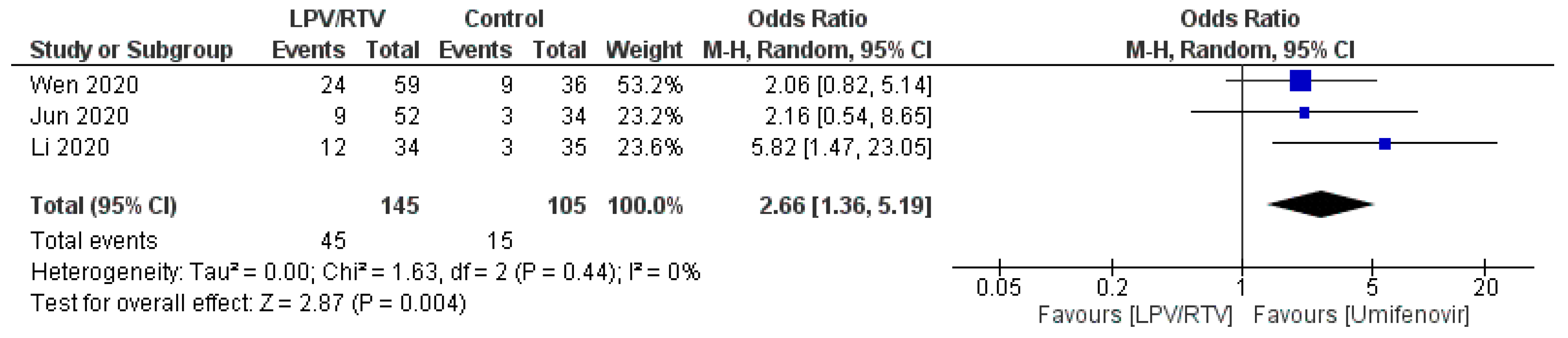
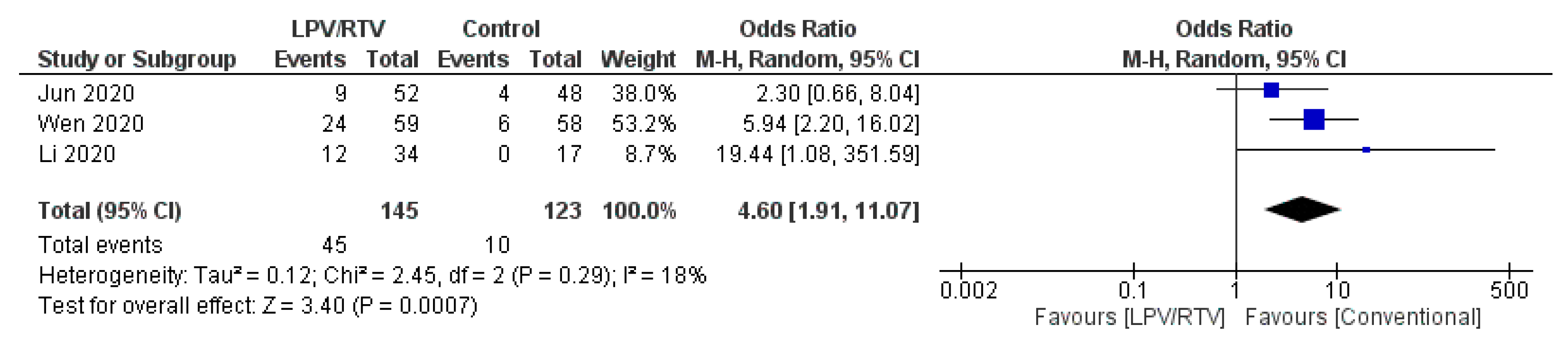
4.1.3. Radiological Progression during Drug Treatment
Rate of Improvement on Chest Computed Tomography (CT) after 7 Days of Treatment
4.1.4. Mortality at 28 Days and Death during Treatment at Any Time
Mortality at 28 Days
Death during Treatment at Any Time
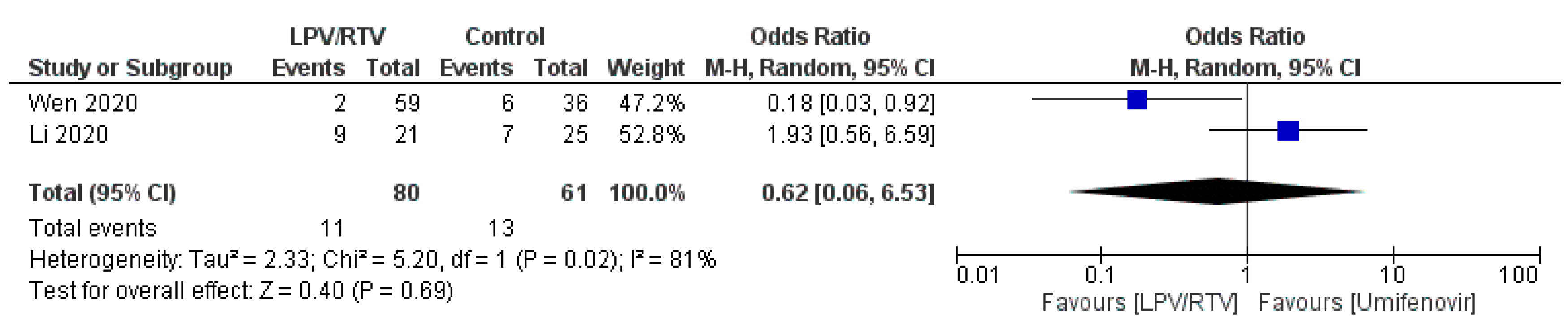
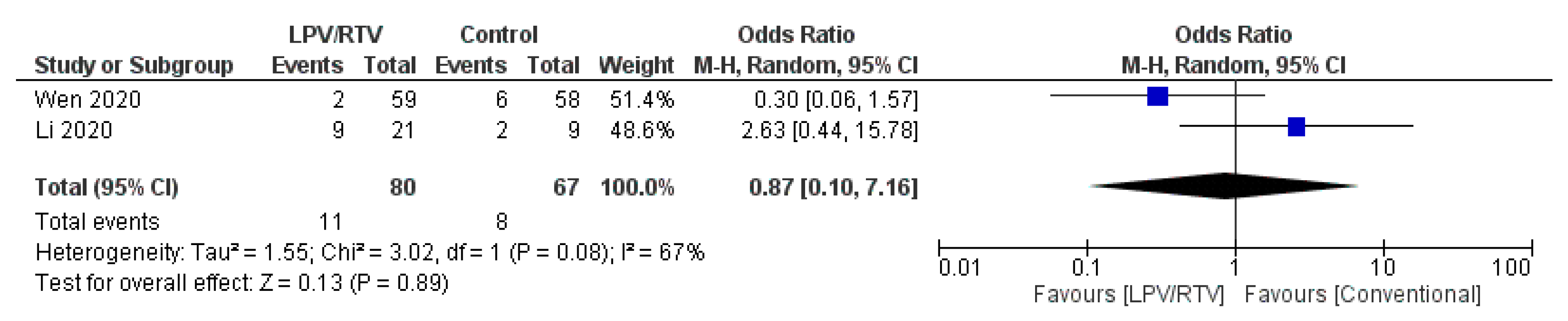
4.1.5. Safety and Tolerability
Rate of Adverse Events of Treatment: LPV/RTV vs. Umifenovir
4.2. Comparison 2: Efficacy and Safety of LPV/RTV along in Combination with Other Agents versus No Antiviral Therapy (Conventional Therapy) or Control
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| COVID-19 | coronavirus disease 2019 |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| MERS-CoV | Middle East respiratory syndrome coronavirus |
| LPV/RTV | lopinavir/ritonavir |
| PRISMA | Preferred Reporting Items for Systematic reviews and Meta-Analysis |
| RoB 2 | Version 2 of the Cochrane risk-of-bias tool for randomized trials |
| ROBINS-I | Risk of bias in non-randomized studies—of interventions |
| RT-PCR | real-time reverse transcription-polymerase chain reaction |
References
- Yang, W.; Cao, Q.; Qin, L.; Wang, X.; Cheng, Z.; Pan, A.; Dai, J.; Sun, Q.; Zhao, F.; Qu, J. Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19): A multi-center study in Wenzhou city, Zhejiang, China. J. Infect. 2020, 80, 388–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tobaigy, M.; Qashqary, S.; Al-Dahery, A.; Mujallad, A.; Hershan, M.; Kamal, N. Therapeutic management of patients with COVID-19: A systematic review. Infect. Prev. Pract. 2020, 2, 100061. [Google Scholar] [CrossRef]
- Statista. Number of Coronavirus (COVID-19) Clinical Trials for Drugs and Vaccines Worldwide as of November 12, 2020, by Type; Statista: Hamburg, Germany, 2020; Available online: https://0-www-statista-com.brum.beds.ac.uk/statistics/1119086/coronavirus-drug-trials-by-type-worldwide/?utm_campaign=Cureus%20U%20-%20Gastroenterology&utm_medium=email&utm_source=marketing_mailer (accessed on 26 November 2020).
- Mehra, M.R.; Desai, S.S.; Ruschitzka, F.; Patel, A.N. Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: A multinational registry analysis. Lancet 2020. [Google Scholar] [CrossRef]
- Mehra, M.R.; Ruschitzka, F.; Patel, A.N. Retraction—Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: A multinational registry analysis. Lancet 2020. [Google Scholar] [CrossRef]
- Coronavirus Updates: Trials to Resume of Anti-Viral Touted by Trump; BBC News: London, UK, 2020.
- Cortegiani, A.; Ippolito, M.; Ingoglia, G.; Iozzo, P.; Giarratano, A.; Einav, S.; Update, I. A systematic review on the efficacy and safety of chloroquine/hydroxychloroquine for COVID-19. J. Crit. Care 2020, 59, 176–190. [Google Scholar] [CrossRef]
- Cvetkovic, R.S.; Goa, K.L. Lopinavir/ritonavir. Drugs 2003, 63, 769–802. [Google Scholar] [CrossRef]
- Alhumaid, S.; Tobaiqy, M.; Albagshi, M.; Alrubaya, A.; Algharib, F.; Aldera, A.; Alali, J. MERS-CoV transmitted from animal-to-human vs MERSCoV transmitted from human-to-human: Comparison of virulence and therapeutic outcomes in a Saudi hospital. Trop. J. Pharm. Res. 2018, 17, 1155–1164. [Google Scholar] [CrossRef]
- Chan, J.F.-W.; Yao, Y.; Yeung, M.-L.; Deng, W.; Bao, L.; Jia, L.; Li, F.; Xiao, C.; Gao, H.; Yu, P. Treatment with lopinavir/ritonavir or interferon-β1b improves outcome of MERS-CoV infection in a nonhuman primate model of common marmoset. J. Infect. Dis. 2015, 212, 1904–1913. [Google Scholar] [CrossRef]
- Chan, K.; Lai, S.; Chu, C.; Tsui, E.; Tam, C.; Wong, M.; Tse, M.; Que, T.; Peiris, J.; Sung, J. Treatment of severe acute respiratory syndrome with lopinavir/ritonavir: A multicentre retrospective matched cohort study. Hong Kong Med. J. 2003, 9, 399–406. [Google Scholar]
- Smolders, E.J.; Te Brake, L.H.; Burger, D.M. SARS-CoV-2 and HIV protease inhibitors: Why lopinavir/ritonavir will not work for COVID-19 infection. Antivir. Ther. 2020. [Google Scholar] [CrossRef]
- Schoergenhofer, C.; Jilma, B.; Stimpfl, T.; Karolyi, M.; Zoufaly, A. Pharmacokinetics of Lopinavir and Ritonavir in Patients Hospitalized With Coronavirus Disease 2019 (COVID-19). Ann. Intern. Med. 2020, 173, 670–672. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensiv. Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M. A trial of lopinavir–ritonavir in adults hospitalized with severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef] [PubMed]
- Massachusetts General Hospital. Massachusetts General Hospital COVID-19 Treatment Guidance; Massachusetts General Hospital: Boston, MA, USA, 2020. [Google Scholar]
- MoH. Coronavirus Disease 19 (COVID-19) Guidelines, Saudi Arabia; MoH: Riyadh, Saudi Arabia, 2020.
- HPSC. Interim Public Health, Infection Prevention & Control Guidelines on the Prevention and Management of COVID-19 Cases and Outbreaks in Residential Care Facilities in Ireland; HPSC: Dublin, Ireland, 2020. [Google Scholar]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2020. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349. [Google Scholar] [CrossRef] [Green Version]
- USFDA. Coronavirus (COVID-19) Update: FDA Revokes Emergency Use Authorization for Chloroquine and Hydroxychloroquine; USFDA: Montgomery, MD, USA, 2020.
- Wang, Z.; Nayfeh, T.; Tetzlaff, J.; O’Blenis, P.; Murad, M.H. Error rates of human reviewers during abstract screening in systematic reviews. PLoS ONE 2020, 15, e0227742. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. Ottawa Hospital Research Institute: The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2020. [Google Scholar]
- Lan, X.; Shao, C.; Zeng, X.; Wu, Z.; Xu, Y. Lopinavir-ritonavir alone or combined with arbidol in the treatment of 73 hospitalized patients with COVID-19: A pilot retrospective study. MedRxiv 2020. [Google Scholar] [CrossRef]
- Li, Y.; Xie, Z.; Lin, W.; Cai, W.; Wen, C.; Guan, Y.; Mo, X.; Wang, J.; Wang, Y.; Peng, P. Efficacy and safety of lopinavir/ritonavir or arbidol in adult patients with mild/moderate COVID-19: An exploratory randomized controlled trial. Med 2020. [Google Scholar] [CrossRef]
- Horby, P.W.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Emberson, J.; Palfreeman, A.; Raw, J.; Elmahi, E.; Prudon, B. Lopinavir–ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef]
- Pan, H.; Peto, R.; Karim, Q.A.; Alejandria, M.; Restrepo, A.M.H.; García, C.H.; Kieny, M.P.; Malekzadeh, R.; Murthy, S.; Preziosi, M.-P. Repurposed antiviral drugs for COVID-19; interim WHO SOLIDARITY trial results. MedRxiv 2020. [Google Scholar] [CrossRef]
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y. Experimental treatment with favipiravir for COVID-19: An open-label control study. Engineering 2020. [Google Scholar] [CrossRef] [PubMed]
- Hung, I.F.-N.; Lung, K.-C.; Tso, E.Y.-K.; Liu, R.; Chung, T.W.-H.; Chu, M.-Y.; Ng, Y.-Y.; Lo, J.; Chan, J.; Tam, A.R. Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: An open-label, randomised, phase 2 trial. Lancet 2020, 395, 1695–1704. [Google Scholar] [CrossRef]
- Wen, C.; Xie, Z.; Li, Y.; Deng, X.; Chen, X.; Cao, Y.; Ou, X.; Lin, W.; Li, F.; Cai, W. Real-world efficacy and safety of lopinavir/ritonavir and arbidol in treating with COVID-19: An observational cohort study. Zhonghua Nei Ke Za Zhi 2020, 59, E012. [Google Scholar] [PubMed]
- Jun, C.; Yun, L.; Xiuhong, X.; Ping, L.; Feng, L.; Tao, L.; Shang, Z.; Mei, W.; Yinzhong, S.; Hongzhou, L. Efficacies of lopinavir/ritonavir and abidol in the treatment of novel coronavirus pneumonia. Chin. J. Infect. Dis. 2020, 12, E008. [Google Scholar]
- Yan, D.; Liu, X.-Y.; Zhu, Y.-N.; Huang, L.; Dan, B.-T.; Zhang, G.-J.; Gao, Y.-H. Factors associated with prolonged viral shedding and impact of Lopinavir/Ritonavir treatment in hospitalised non-critically ill patients with SARS-CoV-2 infection. Eur. Respir. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Zou, R.; Zeng, L.; Kou, S.; Lan, J.; Li, X.; Liang, Y.; Ding, X.; Tan, G.; Tang, S. The correlation between viral clearance and biochemical outcomes of 94 COVID-19 infected discharged patients. Inflamm. Res. 2020, 69, 599–606. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Z.; Lu, Z.; Xu, T.; Chen, C.; Yang, G.; Zha, T.; Lu, J.; Xue, Y. Arbidol monotherapy is superior to lopinavir/ritonavir in treating COVID-19. J. Infect. 2020, 81, e21–e23. [Google Scholar] [CrossRef]
- Ye, X.; Luo, Y.; Xia, S.; Sun, Q.; Ding, J.; Zhou, Y.; Chen, W.; Wang, X.; Zhang, W.; Du, W. Clinical efficacy of lopinavir/ritonavir in the treatment of Coronavirus disease 2019. Eur. Rev. Med. Pharm. Sci. 2020, 24, 3390–3396. [Google Scholar]
- Deng, L.; Li, C.; Zeng, Q.; Liu, X.; Li, X.; Zhang, H.; Hong, Z.; Xia, J. Arbidol combined with LPV/r versus LPV/r alone against Corona Virus Disease 2019: A retrospective cohort study. J. Infect. 2020, 81, e1–e5. [Google Scholar] [CrossRef]
- Lian, N.; Xie, H.; Lin, S.; Huang, J.; Zhao, J.; Lin, Q. Umifenovir treatment is not associated with improved outcomes in patients with coronavirus disease 2019: A retrospective study. Clin. Microbiol. Infect. 2020, 26, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Haviernik, J.; Štefánik, M.; Fojtíková, M.; Kali, S.; Tordo, N.; Rudolf, I.; Hubálek, Z.; Eyer, L.; Ruzek, D. Arbidol (Umifenovir): A broad-spectrum antiviral drug that inhibits medically important arthropod-borne flaviviruses. Viruses 2018, 10, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klement-Frutos, E.; Burrel, S.; Peytavin, G.; Marot, S.; Lê, M.P.; Godefroy, N.; Calvez, V.; Marcelin, A.-G.; Caumes, E.; Pourcher, V. Early administration of ritonavir-boosted lopinavir could prevent severe COVID-19. J. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Choy, K.-T.; Wong, A.Y.-L.; Kaewpreedee, P.; Sia, S.-F.; Chen, D.; Hui, K.P.Y.; Chu, D.K.W.; Chan, M.C.W.; Cheung, P.P.-H.; Huang, X. Remdesivir, lopinavir, emetine, and homoharringtonine inhibit SARS-CoV-2 replication in vitro. Antivir. Res. 2020, 104786. [Google Scholar] [CrossRef]
- Smith, P.F.; Dodds, M.; Bentley, D.; Yeo, K.; Rayner, C. Dosing will be a key success factor in repurposing antivirals for COVID-19. Br. J. Clin. Pharmacol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Fan, J.; Zhang, X.; Liu, J.; Yang, Y.; Zheng, N.; Liu, Q.; Bergman, K.; Reynolds, K.; Huang, S.-M.; Zhu, H. Connecting hydroxychloroquine in vitro antiviral activity to in vivo concentration for prediction of antiviral effect: A critical step in treating COVID-19 patients. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Lamontagne, F.; Agoritsas, T.; Macdonald, H.; Leo, Y.-S.; Diaz, J.; Agarwal, A.; Appiah, J.A.; Arabi, Y.; Blumberg, L.; Calfee, C.S. A living WHO guideline on drugs for covid-19. BMJ 2020, 370. [Google Scholar] [CrossRef]
- World Health Organization. Therapeutics and COVID-19: Living Guideline; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- National Institutes of Health. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines; NIH: Bethesda, MD, USA, 2020.
- Infectious Diseases Society of America. Guidelines on the Treatment and Management of Patients with COVID-19; IDSA: Arlington, VA, USA, 2020. [Google Scholar]
- WHO. Draft Landscape of COVID-19 Candidate Vaccines; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Krammer, F. SARS-CoV-2 vaccines in development. Nature 2020, 586, 516–527. [Google Scholar] [CrossRef]
- Moderna, Inc. Moderna’s COVID-19 Vaccine Candidate Meets Its Primary Efficacy Endpoint in the First Interim Analysis of the Phase 3 COVE Study; Moderna, Inc.: Cambridge, MA, USA, 2020. [Google Scholar]
- BioNTech, P.A. Pfizer and BioNTech Conclude Phase 3 Study of COVID-19 Vaccine Candidate, Meeting All Primary Efficacy Endpoints; BioNTech SE: Mainz, Germany, 2020. [Google Scholar]
- Halasz, S.; Fox, K.; Cassidy, A. AstraZeneca’s Oxford Coronavirus Vaccine is 70% Effective on Average, Data Shows, with No Safety Concerns; CNN: Atlanta, GA, USA, 2020. [Google Scholar]
- Sheahan, T.P.; Sims, A.C.; Leist, S.R.; Schäfer, A.; Won, J.; Brown, A.J.; Montgomery, S.A.; Hogg, A.; Babusis, D.; Clarke, M.O. Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS-CoV. Nat. Commun. 2020, 11, 222. [Google Scholar] [CrossRef] [Green Version]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year [Reference] from, Study Location | Study Design and Setting | Age (Year) | Male, n (%) | Population | Intervention | Control | Time from Symptom Onset to Treatment Initiation | Outcome | AEs in LPV/RTV and Control Arm | Assessment of Study Risk of Bias (Tool Used; Finding) | Remark |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Horby et al. 2020 [28]; United Kingdom | Randomized open-label controlled trial; multicenter | Mean (SD), 66.3 (15.9) | 3077 (61.1) | Clinically suspected or laboratory confirmed SARS-CoV-2 infection cases of any age Consistent characteristics across groups for age, sex, ethnicity, duration of symptoms before randomisation, amount of respiratory support at randomisation, and baseline predicted risk of death | 1616 patients received: LPV/RTV (oral): 400 mg/100 mg twice daily for 10 days or until discharge, if sooner PLUS standard care * for 10 days or until discharge, if sooner | 3424 patients received: Standard care alone * for 10 days or until discharge, if sooner | Not reported | Mortality at 28 days: 23% patients allocated to LPV/RTV and 22% patients allocated to usual care died within 28 days (RR 1.03, 95% CI 0.91–1.17; p = 0.60) Time until discharge alive from hospital: median 11 days [IQR 5 to >28] in both groups Patients discharged from hospital alive within 28 days: (RR 0.98, 95% CI 0.91–1.05; p = 0.53) Patients met the endpoint of invasive mechanical ventilation (RR 1.15, 95% CI 0.95–1.39; p = 0.15); or death (RR 1.04, 95% CI 0.93–1.16; p = 0.54) | In the LPV/RTV group, there was a serious case of elevated ALT that did not meet standard criteria for drug-induced liver injury Detailed information on non-serious adverse reactions or reasons for stopping treatment were not collected | RoB 2, low risk of bias | LPV/RTV was not associated with reductions in 28-day mortality, duration of hospital stay, or risk of progressing to invasive mechanical ventilation or death Since preliminary results of RECOVERY trial were made public, WHO has halted the LPV/RTV monotherapy and the LPV/RTV plus IFN-b combination groups of the SOLIDARITY trial |
| Pan et al. 2020 [29]; Multi-country | Randomized open-label controlled trial; multicenter | <50 years: 36.5% 50–69 years: 7% 70+ years: 20.8% | 1653 (59.6) | Hospitalized confirmed COVID-19 cases aged ≥18 years and not known to have received any study drug Patient characteristics were well balanced between the two groups | 1399 patients received: LPV/RTV (oral): 400 mg/100 mg twice daily for 10 days | 1372 patients received: standard care * | Not reported | Death (with 95% CIs and numbers dead/randomized, LPV/RTV vs. its control) was: RR 1.00 (0.79–1.25, p = 0.97; 148/1399 vs. 146/1372) Initiation of ventilation: 124 (LPV/RTV) vs. 119 (control) Patients still hospitalized at day 7: 68% (LPV/RTV) vs. 59% (control) | No death was attributed to LPV/RTV due to renal or hepatic disease | RoB 2, low risk of bias | LPV/RTV did not reduce mortality (in unventilated patients or any other subgroup of entry characteristics), initiation of ventilation or hospitalization duration |
| Cai et al. 2020 [30]; China | Nonrandomized open-label controlled trial; single center | Median (IQR), 47 (35.7–61) | 35 (43.8) | Confirmed COVID-19 cases aged 16–75 years No significant differences between the baseline characteristics of the two arms FPV treated patients were older (43 years) compared with LPV/RTV arm (49 years) All patients were moderate cases as defined by NHC [1] | 45 patients received: LPV/RTV (oral): 400 mg/100 mg twice daily on days 1–14 PLUS IFN-α1b (aerosol inhalation): 5 million IUs twice daily | 35 patients received: FPV (oral): 1600 mg twice daily on Day 1 and 600 mg twice daily on days 2–14 PLUS IFN-α1b (aerosol inhalation): 5 million IUs twice daily | Less than 7 days | Viral clearance: shorter viral clearance time for FPV arm (median (IQR), 4 (2.5–9) days versus 11 (8–13) days, p < 0.001) Chest CT changes: more imaging improvement rate in FPV arm (91.43% vs. 62.22%), p = 0.004 | FPV arm patients had less AEs compared to the LPV/RTV group (11.43% vs. 55.56%) (p < 0.001) Two patients had diarrhea, one had a liver injury, and one had a poor diet in the FPV arm There were five patients with diarrhea, five with vomiting, six with nausea, four with rash, three with liver injury, and two with chest tightness and palpitations in the LPV/RTV arm | ROBINS-I, moderate risk of bias | Two patients in the FPV group turned negative for viral RNA detection in nasopharyngeal swabs at days 18 and 21 For patients in the LPV/RTV group, the viral RNA detection all turned negative within 27 days |
| Cao et al. 2020 [15]; China | Randomized open-label controlled trial; single center | Median (IQR), 58 (49–68) | 120 (60.3) | Confirmed COVID-19, having a SaO2 of 94% or less or a ratio of the PaO2 to the FiO2 of less than 300 mmHg No important between-group differences in demographic characteristics, baseline laboratory test results, distribution of ordinal scale scores, or NEWS2 scores at enrollment | 99 patients received: LPV/RTV (oral): 400/100 mg twice daily PLUS standard care * for 14 days | 100 patients received: standard care * alone for 14 days | 13 days (IQR, 11 to 16 days) | Time to clinical improvement: no difference in the time to clinical improvement for patients in the LPV/RTV group and the standard-care * group (HR for clinical improvement, 1.31; 95% CI, 0.95 to 1.80) Mortality at 28 days was similar in the two groups (19.2% vs. 25.0%; difference, −5.8 percentage points; 95% CI, −17.3 to 5.7) Percentages of patients with detectable viral RNA at various time points were similar LPV/RTV led to a median time to clinical improvement that was shorter by 1 day than that observed with standard care* (HR, 1.39; 95% CI, 1.00 to 1.91) | GI AEs were more common in the LPV/RTV group, but serious AEs were more common in the standard care * group. LPV/RTV treatment was stopped early in 13.8% because of AEs | RoB 2, low risk of bias | Most patients were severely unwell and required urgent clinical attention Systemic glucocorticoids were administered (33.0% in patients of LPV/RTV group and 35.7% in patients of standard-care * alone group) |
| Hung et al. 2020 [31]; Hong Kong | Randomized open-label trial; multicenter | Median (IQR), 52 (32–62) | 68 (54) | Confirmed COVID-19 cases and aged at least 18 years, a NEWS2 of at least 1, and symptom duration of 14 days or less upon recruitment. Age, sex, and baseline demographics in each group were similar | 41 patients received: LPV/RTV (oral): 400/100 mg twice daily (control group) for 14 days | 86 patients received: LPV/RTV (oral): 400/100 mg twice daily PLUS Ribavirin (oral): 400 twice daily PLUS IFN-beta-1b (SCI): three doses of 8 million IUs of interferon beta-1b on alternate days (combination group); for 14 days | 5 days (IQR 3–7) | Combination group had a significantly shorter median time from start of study treatment to negative nasopharyngeal swab (7 days [IQR 5–11]) than the LPV/RTV group (12 days [8,9,10,11,12,13,14,15]; HR 4.37 [95% CI 1.86–10.24], p = 0.0010) | AEs included nausea and diarrhea with no difference between the two groups. One patient in the control group discontinued LPV/RTV because of biochemical hepatitis | RoB 2, some concerns risk of bias | No patients died during the study |
| Li et al. 2020 [27]; China | Randomized blinded trial; single center | Mean (SD), 49.4 (14.7) | 40 (46.5) | Mild/moderate confirmed COVID-19 cases aged 18–80 years Baseline characteristics of the three groups were comparable | 34 patients received: LPV/RTV (oral): 200/50 mg twice daily for 7–14 days | 35 patients received: Umifenovir (oral): 200 mg three times daily for 7–14 days OR 17 patients received no antiviral therapy (conventional) | 3.5 days (IQR, 2 to 6 days) | Rate of positive-to-negative conversion of SARS-CoV-2 nucleic acid was similar between groups (all p > 0.05) There were no differences between groups in the rates of antipyresis, cough alleviation, or improvement of chest CT at day 7 or 14 (all p > 0.05) At day 7, 23.5% patients in the LPV/RTV group, 8.6% in the umifenovir group, and 11.8% in the control group showed a deterioration in clinical status from moderate to severe/critical (p = 0.206) | Overall, 35.3% of patients in the LPV/RTV group and 14.3% in the umifenovir group experienced AEs No apparent AEs occurred in the control group | RoB 2, high risk of bias | Study was blinded to participants, physicians, and radiologists who reviewed data but open label to clinicians who recruited patients and research staff All three groups were treated with Standard care * if in need |
| Lan et al. 2020 [26]; China | Retrospective; cohort; multicenter | Mean (SD), 55.8 (15.2) | 37 (50.7) | Confirmed COVID-19 cases treated with LPV/RTV alone or combined with umifenovir Different age, sex, and baseline demographics in each group | 34 patients received: LPV/RTV (oral): 400/100 mg twice daily for 14 days | 39 patients received: LPV/RTV (oral): 400/100 mg twice daily PLUS Umifenovir (oral): 200 mg three times daily; at least for 3 days | Not reported | Treatment with LPV/RTV alone was not different from LPV/RTV combined with umifenovir in overall cure rate (92.3% and 97.1%, respectively) LPV/RTV combined with umifenovir led to a median time of hospital stay that was shorter by 1.5 days (12.5 days vs. 14 days) COVID-19 RNA clearance was 92.3% in LPV/RTV and 97.1% in combination therapies group Mean time of virus turning negative was 11.5 ± 9.0 days in combination group compared to 9.9 ± 7.5 in single therapy group | Not reported | NOS, 5 | All eligible patients received standard care * if necessary |
| Wen et al. 2020 [32]; China | Retrospective; cohort; single center | Mean (SD), 49.9 (16.1) | 81 (45.5) | Confirmed COVID-19 cases aged ≥18 years with a hospital stay longer than 14 days No statistically significant difference in baseline characteristics before treatment between patients in LPV/RTV group, umifenovir group, combination (LPV/RTV and umifenovir) group and conventional treatment (no antiviral therapy) group | 59 patients received: LPV/RTV (oral): 200/50 mg twice daily for 7 days | 36 patients received: Umifenovir (oral): 200 mg three times daily for 7 days OR 25 patients received: Combined antiviral therapies (LPV/RTV AND umifenovir; same dosages for 7 days) OR 58 patients received no antiviral therapy (conventional group) | Not reported | Time for pharyngeal swab PCR to turn negative was (10.20 ± 3.49 days) in LPV/RTV group, (10.11 ± 4.68 days) in umifenovir group, (10.86 ± 4.74 days) in LPV/RTV plus umifenovir group, and (8.44 ± 3.51 days) in conventional group No significant difference in the rate of nasopharyngeal swab new coronavirus nucleic acid conversion, clinical symptom improvement rate, and lung infection imaging improvement rate (p > 0.05). There was a statistically significant difference in the ratio of normal/mild to severe/critically severe on the 7th day in the four groups (χ2 = 9.311, p = 0.017): the combined group (24.0%), umifenovir group (16.7%), LPV/RTV group (5.4%), conventional treatment group (5.2%) | AEs in the three groups of patients using antiviral drugs was significantly higher than that in the conventional treatment group (χ2 = 14.875, p = 0.002) | NOS, 5 | All three groups were treated with standard care * if in need |
| Jun et al. 2020 [33]; China | Retrospective; cohort; single center | Median (IQR), 48 (35–62) | 69 (51.5) | Confirmed COVID-19 cases No statistically significant differences in the demographic data, clinical manifestations, laboratory examinations, and chest CT examination of patients in the LPV/RTV group, umifenovir group, and control (no antiviral therapy) group (all p > 0.05) | 52 patients received: LPV/RTV (oral): 200/50 mg twice daily for 5 days | 34 patients received: Umifenovir (oral): 200 mg three times daily for 5 days OR 48 patients received no antiviral therapy (conventional group) | Not reported | Median time for the body temperature to return to normal in the umifenovir group and the LPV/RTV group was 6 days, and the conventional group was 4 days (χ2 = 2.37, p = 0.31). Median time of viral nucleic acid negative in respiratory tract specimens of the three groups was 7 days after treatment. Viral nucleic acid negative in the LPV/RTV group was 71.8% and 82.6% in the umifenovir group, the conventional group was 77.1% (χ2 = 0.46, p = 0.79) 42.3% patients in the LPV/RTV group, 35.3% patients in the umifenovir group, and 52.1% patients in the conventional group still had progressive imaging on the 7th day after treatment (χ2 = 2.38, p = 0.30) | 17.3% in the LPV/RTV group had AEs, including nausea, diarrhea, and other GI symptoms; 8.8% in the umifenovir group had AEs, including diarrhea; 8.3% in the control group had AEs such as anorexia and diarrhea (χ2 = 2.33, p = 0.33) | NOS, 5 | All patients received IFN α2b spray therapy and standard care * |
| Yan et al. 2020 [34]; China | Retrospective; cohort; single center | Median (IQR), 52 (35–63) | 54 (45) | Confirmed COVID-19 cases and had the available RNA viral data to estimate the duration of viral shedding | 78 patients received: LPV/RTV (oral): 200/50 mg twice daily for 10 days or more | 42 patients received no antiviral therapy (conventional group) | 10 days (IQR 7–13) | Median duration of viral shedding was shorter in the LPV/RTV treatment group than that in no LPV/RTV treatment group (median, 22 days vs. 28.5 days, p = 0.02) Patients who started LPV/RTV treatment within 10 days from symptom onset had a shorter duration of SARS-CoV-2 RNA shedding than other patients who began after 10 days (median 19 days vs. 27.5 days, p < 0.001) | Not reported | NOS, 5 | Many patients received and standard care * if in need |
| Yuan et al. 2020 [35]; China | Retrospective; cohort; single center | Median (range), 40 (1–78) | 42 (45) | Confirmed COVID-19 cases of mild and/or moderate symptoms and critical conditions Significant different illness onset on the most common symptoms (fever, fatigue, and diarrhea) | 46 patients received: LPV/RTV+ IFN-α (dosages, durations were not reported) | 41 patients received: IFN-α + LPV/RTV PLUS Ribavirin; (dosages, durations were not reported) | Not reported | No significant difference in average LOS or PCR negative conversion times among different antivirus treatment groups. Correlation analysis indicated that the duration of hospital stay was significantly correlated with PCR negative conversion times in IFN-α + lopinavir/ritonavir + ribavirin group (p = 0.0215), as well as IFN-α + lopinavir/ritonavir group (p = 0.012). Average LOS and IFN treatment duration of moderate group was 14.12 (13.34–14.90) days and 14.24 (13.45–15.03) days, respectively, while those of the severe group took average 2.08 days and 1.44 days longer | Not reported | NOS, 6 | Approximately 51% were aged ≤40 year, including 2 children under 3 year |
| Zhu et al. 2020 [36]; China | Retrospective; cohort; multicenter | Mean (SD), 39.8 (17.6) | 26 (52) | Confirmed COVID-19 cases No significant difference in age and sex between the two groups | 34 patients received: LPV/RTV (oral): 200/50 mg twice daily for 7 days | 16 patients received: Umifenovir (oral): 200 mg three times daily (duration was not reported) | Not reported | No difference in fever duration between the two groups (p = 0.61). On day 14 after the admission, no viral load was detected in umifenovir group, but the viral load was found in 44.1% of patients treated with LPV/RTV. Patients in the umifenovir group had a shorter duration of positive RNA test compared to those in the LPV/RTV group (p < 0.01) | No apparent SEs were found in both groups | NOS, 6 | All patients received and standard care * if in need |
| Ye et al. 2020 [37]; China | Retrospective; cohort; single center | Range (5–68), of which 9 were <30 and 38 were >30 | 22 (46.8) | Confirmed COVID-19 cases treated with LPV/RTV or not during hospitalization Different age, sex, and baseline demographics in each group | 42 patients received: LPV/RTV (oral): 400/100 mg twice daily or 800/200 mg once daily PLUS Umifenovir (oral): 200 mg three times daily PLUS IFN-α1b (aerosol inhalation): 5 million IUs twice daily; (durations of use were not reported) | 5 patients received: Umifenovir (oral): 200 mg three times daily PLUS IFN-α1b (aerosol inhalation): 5 million IUs twice daily; (durations of use were not reported) | Not reported | Patients in the LPV/RTV group returned to normal body temperature in a shorter time (test group: 4.8 ± 1.94 days vs. control group: 7.3 ± 1.53 days, p = 0.0364) Patients in the LPV/RTV group were able to turn negative in a shorter period of time (LPV/RTV group: 7.8 ± 3.09 days vs. control group: 12.0 ± 0.82 days, p = 0.0219) | Increased level of ALT enzyme in the LPV/RTV group | NOS, 5 | All patients received and standard care * if in need |
| Deng et al. 2020 [38]; China | Retrospective; cohort; single center | Mean (SD), 44.6 (15.8) | 17 (51.5) | Confirmed COVID-19 cases of adults (≥ 18 years) with laboratory-confirmed COVID-19 without invasive ventilation Baseline clinical, laboratory, and chest CT characteristics were similar between groups | 17 patients received: LPV/RTV (oral): 400/100 mg twice daily | 16 patients received: LPV/RTV (oral): 400/100 mg twice daily PLUS Umifenovir (oral): 200 mg three times daily (until coronavirus is detected negative by RT-PCR for three times) | Not reported | SARS-CoV-2 could not be detected for 75% of patients’ nasopharyngeal specimens in the combination group after 7 days, compared with 35% in the monotherapy group (p < 0.05). After 14 days, 94% in the combination group and 52.9% in the monotherapy group, respectively, SARS-CoV-2 could not be detected (p < 0.05) Chest CT scans were improving for 69% of patients in the combination group after seven days, compared with 29% in the monotherapy group (p < 0.05) | Elevated levels of bilirubin in patients (68.7%) Digestive upsets, such as mild diarrhea and nausea were reported in patients (43.7%) | NOS, 6 | All patients received and standard care * if in need. Authors never stated which therapy group experienced AEs |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhumaid, S.; Al Mutair, A.; Al Alawi, Z.; Alhmeed, N.; Zaidi, A.R.Z.; Tobaiqy, M. Efficacy and Safety of Lopinavir/Ritonavir for Treatment of COVID-19: A Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2020, 5, 180. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5040180
Alhumaid S, Al Mutair A, Al Alawi Z, Alhmeed N, Zaidi ARZ, Tobaiqy M. Efficacy and Safety of Lopinavir/Ritonavir for Treatment of COVID-19: A Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease. 2020; 5(4):180. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5040180
Chicago/Turabian StyleAlhumaid, Saad, Abbas Al Mutair, Zainab Al Alawi, Naif Alhmeed, Abdul Rehman Zia Zaidi, and Mansour Tobaiqy. 2020. "Efficacy and Safety of Lopinavir/Ritonavir for Treatment of COVID-19: A Systematic Review and Meta-Analysis" Tropical Medicine and Infectious Disease 5, no. 4: 180. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5040180