Human Papillomavirus (HPV69/HPV73) Coinfection associated with Simultaneous Squamous Cell Carcinoma of the Anus and Presumed Lung Metastasis

 and
and 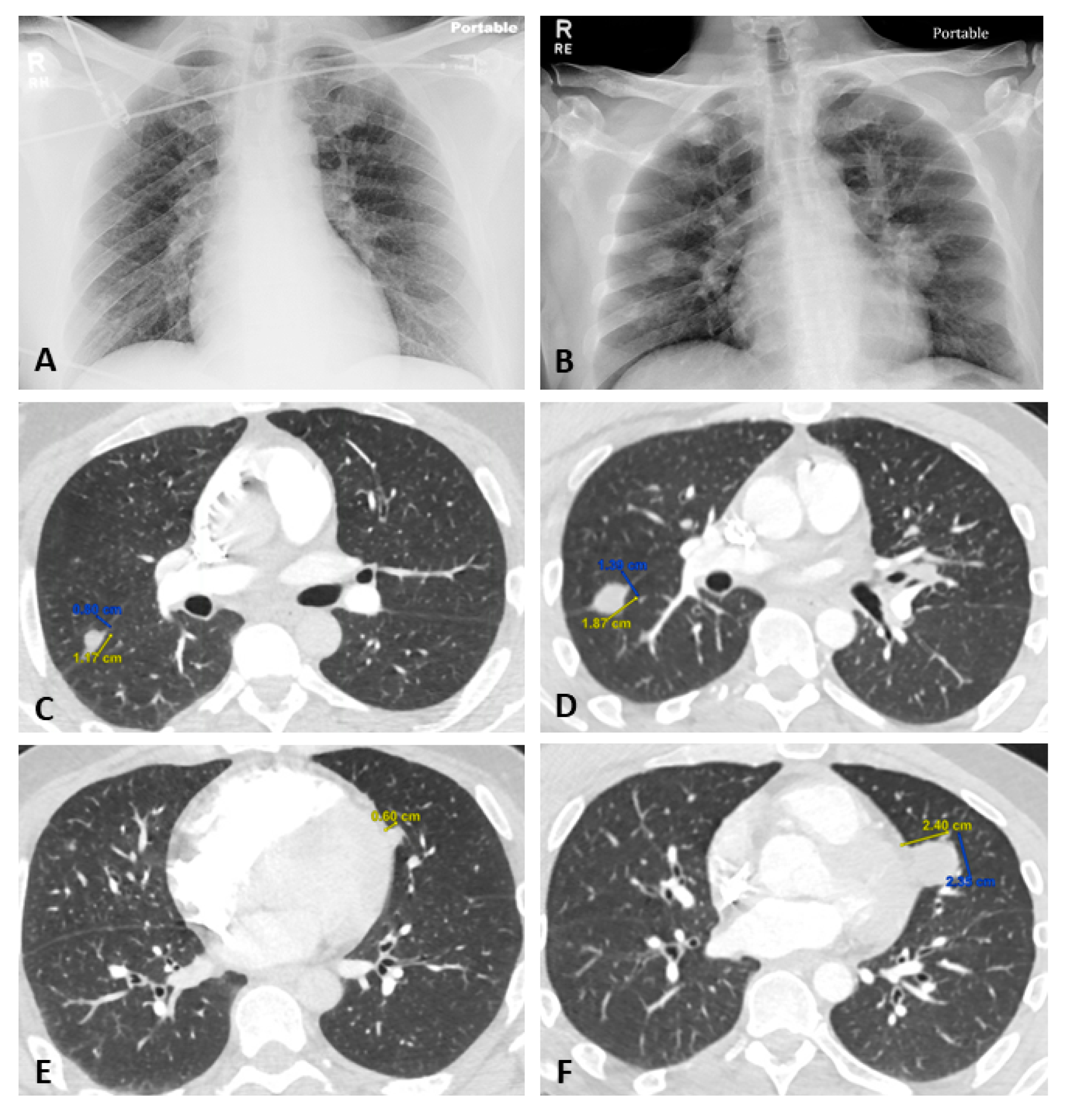{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
2.1. Case Presentation
2.2. Histopathology and Immunohistochemistry (IHC)
2.3. Polymerase Chain Reaction (PCR)
2.4. Data Analysis
3. Results
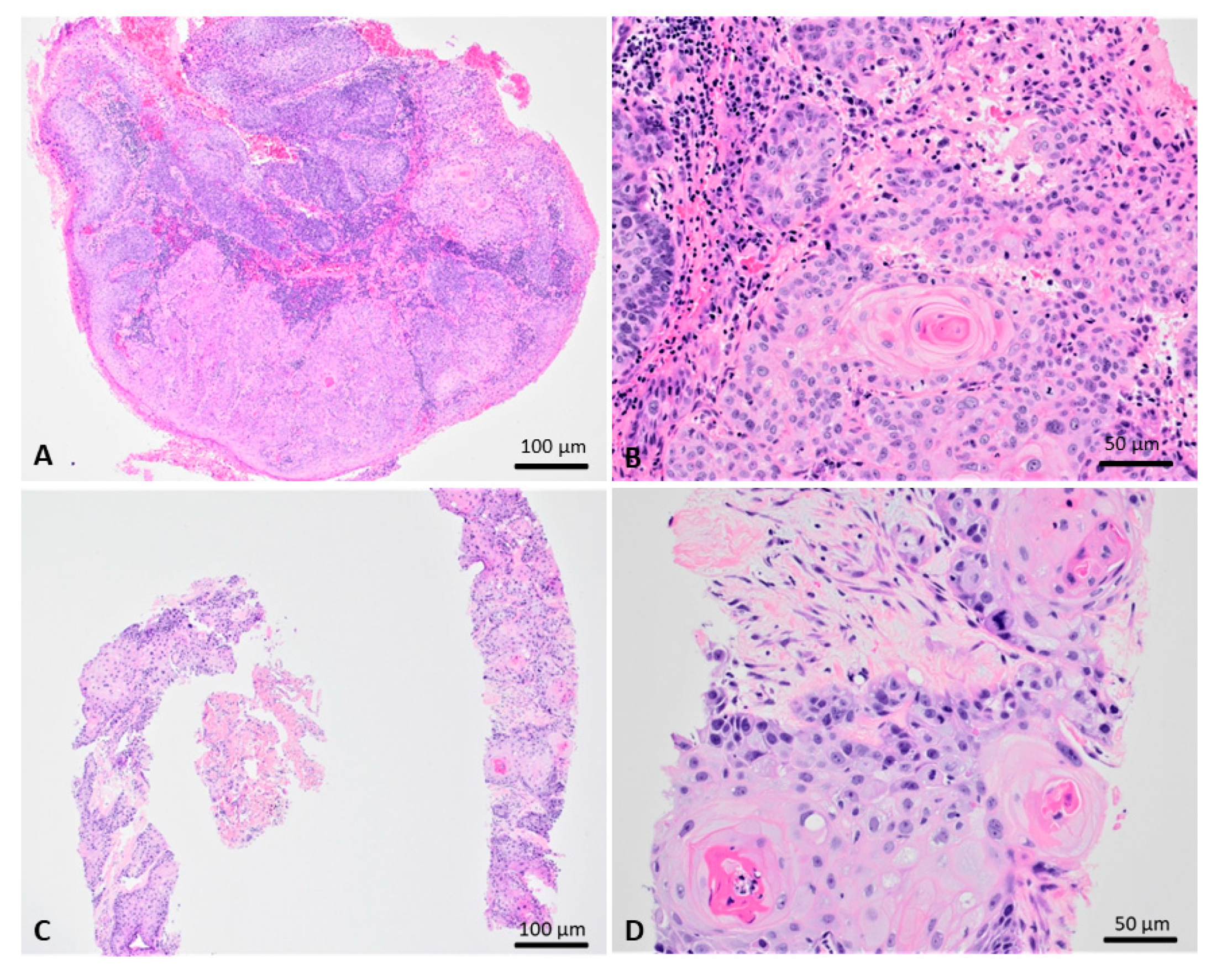
3.1. Pathological Findings
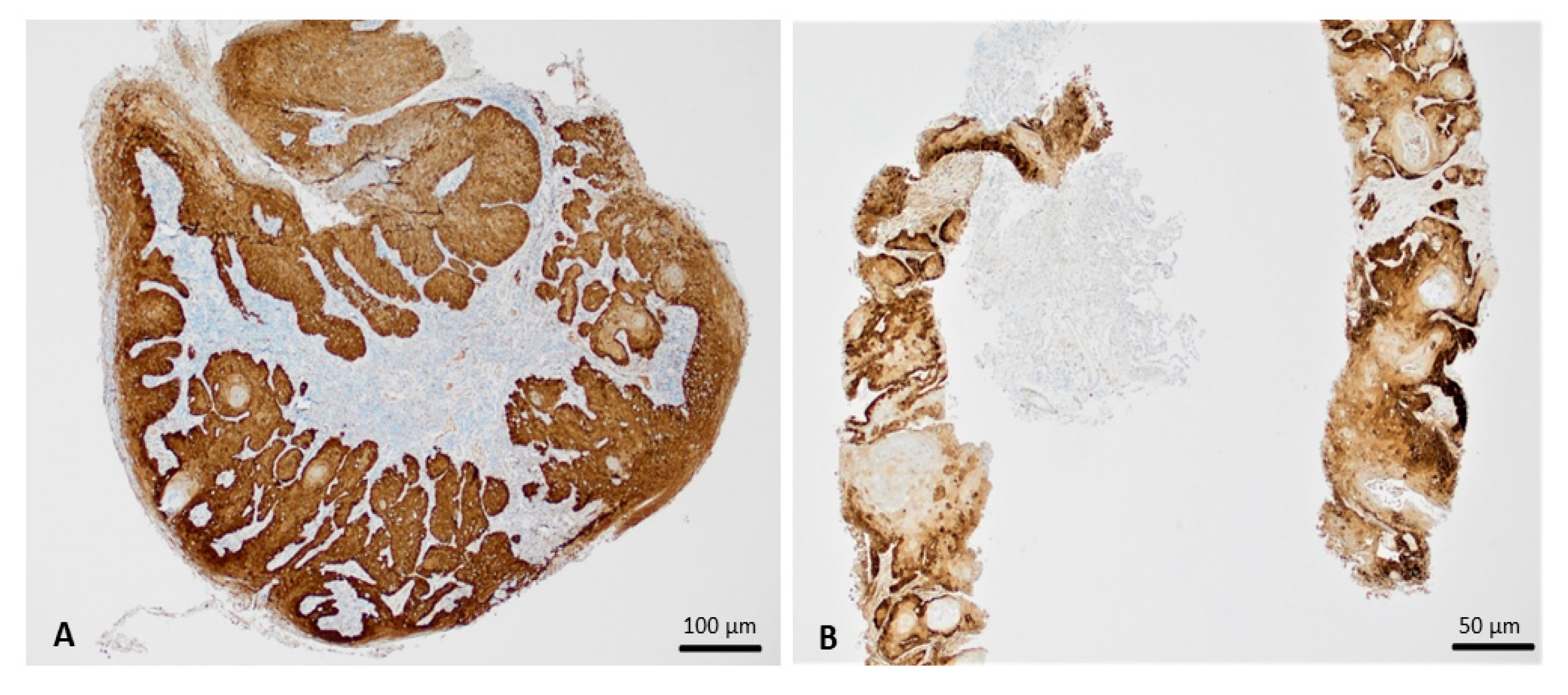
3.2. Immunohistochemistry
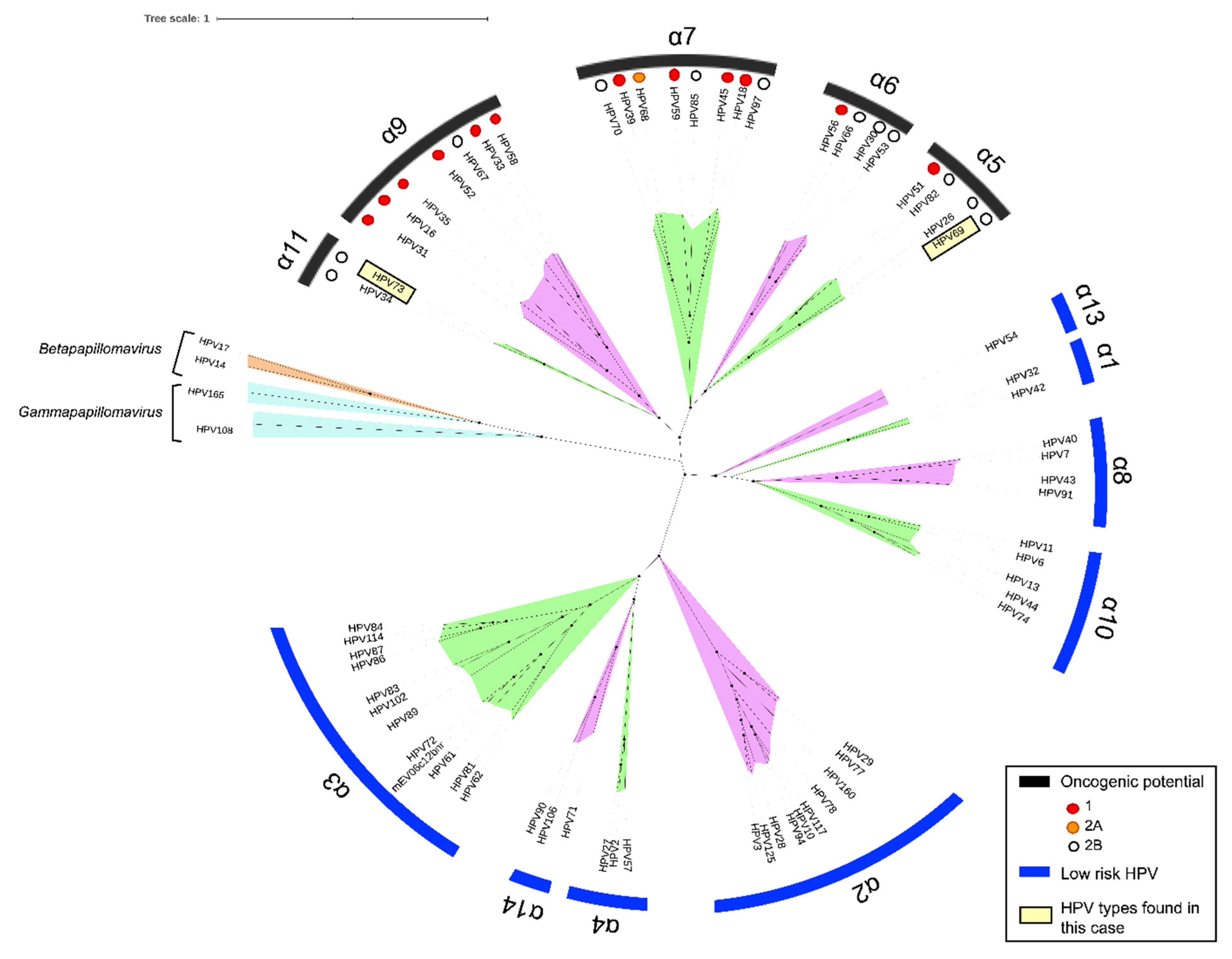
3.3. PCR and Phylogenetic Studies
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Burd, E.M. Human papillomavirus laboratory testing: The changing paradigm. Clin. Microbiol. Rev. 2016, 29, 291–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakabayashi, R.; Nakahama, Y.; Nguyen, V.; Espinoza, J.L. The host-microbe interplay in human papillomavirus-induced carcinogenesis. Microorganisms 2019, 7, 199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litwin, T.R.; Clarke, M.A.; Dean, M.; Wentzensen, N. Somatic host cell alterations in HPV carcinogenesis. Viruses 2017, 9, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houldsworth, J. FHACT: The FISH-based HPV-associated cancer test that detects nonrandom gain at four genomic loci as biomarkers of disease progression. Expert Rev. Mol. Diagn. 2014, 14, 921–934. [Google Scholar] [CrossRef] [PubMed]
- Guidry, J.T.; Scott, R.S. The interaction between human papillomaviruses and other viruses. Viruses Res. 2017, 231, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheit, T. Mucosal and cutaneous human papillomavirus infections and cancer biology. Front. Oncol. 2019, 9, 355. [Google Scholar] [CrossRef] [Green Version]
- Taberna, M.; Mena, M.; Pavón, M.A.; Alemany, L.; Gillison, M.L.; Mesía, R. Human papillomavirus-related oropharyngeal cancer. Ann. Oncol. 2017, 28, 2386–2398. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Human papillomaviruses. IARC Monogr. Eval. Carcinog. Risks Hum. 2007, 90, 1–636. [Google Scholar]
- IARC Working Group on the Evaluation of Carcinogenic Risk to Humans. Biological Agents. Lyon (FR): International Agency for Research on Cancer; 2012, (IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 100B.) Human Papillomaviruses. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK304347/ (accessed on February 2020).
- Ruel, J.; Ko, H.M.; Roda, G.; Patil, N.; Zhang, D.; Jharap, B.; Harpaz, N.; Colombel, J.F. Anal Neoplasia in Inflammatory Bowel Disease Is Associated With HPV and Perianal Disease. Clin. Transl. Gastroenterol. 2016, 7, e148. [Google Scholar] [CrossRef]
- U.S. National Library of Medicine. BLAST: Basic Local Alignment Search Tool. Available online: https://blast.ncbi.nlm.nih.gov/Blast.cgi (accessed November 2019).
- National Institute of Allergy and Infectious Diseases. PaVE: Papilloma virus genome database. Available online: https://pave.niaid.nih.gov/#search/pv_specific_blast. (accessed November 2019).
- Chang, S.Y.; Keeney, M.; Law, M.; Donovan, J.; Aubry, M.C.; Garcia, J. Detection of human papillomavirus in non–small cell carcinoma of the lung. Hum. Pathol. 2015, 46, 1592–1597. [Google Scholar] [CrossRef]
- Van Doorslaer, K.; Chen, Z.; Bernard, H.U.; et al. ICTV virus taxonomy profile: Papillomaviridae. J. Gen. Virol. 2018, 99, 989–990. [Google Scholar] [CrossRef] [PubMed]
- Amaro-Filho, S.M.; Grandissimo, A.; Usyk, M.; de Almeida, L.M.; Moreira, M.A.; Burk, R.D. HPV73 a nonvaccine type causes cervical cancer. Int. J. Cancer 2020, 146, 731–738. [Google Scholar] [CrossRef] [PubMed]
- de Sanjose, S.; Quint, W.G.V.; Alemany, L.; et al. Human papillomavirus genotype attribution in invasive cervical cancer: A retrospective cross-sectional worldwide study. Lancet Oncol. 2010, 11, 1048–1056. [Google Scholar] [CrossRef]
- Muñoz, N.; Bosch, F.X.; de Sanjose, S.; Herrero, R.; Castellsagué, X.; Shah, K.V.; Snijders, P.J.; Meijer, C.J.; International Agency for Research on Cancer Multicenter Cervical Cancer Study Group. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N. Engl. J. Med. 2003, 348, 518–527. [Google Scholar] [CrossRef] [Green Version]
- West, A.B.; Soloway, G.N.; Lizarraga, G.; Tyrrell, L.; Longley, J.B. Type 73 human papillomavirus in esophageal squamous cell carcinoma: A novel association. Cancer 1996, 77, 2440–2444. [Google Scholar] [CrossRef]
- Guldbakke, K.K.; Brodsky, J.; Liang, M.; Schanbacher, C.F. Human papillomavirus type 73 in primary and recurrent periungual squamous cell carcinoma. Dermatol. Surg. 2008, 34, 407–413. [Google Scholar] [CrossRef]
- Halec, G.; Alemany, L.; Lloveras, B.; Schmitt, M.; Alejo, M.; Bosch, F.X.; Tous, S.; Klaustermeier, J.E.; Guimerà, N.; Grabe, N.; et al. Pathogenic role of the eight probably/possibly carcinogenic HPV types 26, 53, 66, 67, 68, 70, 73 and 82 in cervical cancer. J. Pathol. 2014, 234, 441–451. [Google Scholar] [CrossRef]
- Ragin, C.; Obikoya-Malomo, M.; Kim, S.; Chen, Z.; Flores-Obando, R.; Gibbs, D.; Koriyama, C.; Aguayo, F.; Koshiol, J.; Caporaso, N.E.; et al. HPV-associated lung cancers: An international pooled analysis. Carcinogenesis 2014, 35, 1267–1275. [Google Scholar] [CrossRef]
- Argyri, E.; Tsimplaki, E.; Marketos, C.; Politis, G.; Panotopoulou, E. Investigating the role of human papillomavirus in lung cancer. Papillomavirus Res. 2017, 3, 7–10. [Google Scholar] [CrossRef]
- Kim, N.R.; Kang, M.; Lee, S.P.; Kim, H.; An, J.; Chung, D.H.; Ha, S.Y.; Cho, H.Y. Uncommon and rare human papillomavirus genotypes relating to cervical carcinomas. Korean J. Pathol. 2014, 48, 43–49. [Google Scholar] [CrossRef]
- Lee, D.; Kim, S.; Park, S.; Jin, H.; Kim, T.U.; Park, K.H.; Lee, H. Human papillomavirus prevalence in Gangwon province using reverse blot hybridization assay. Korean J. Pathol. 2011, 45, 348–353. [Google Scholar] [CrossRef]
- Lee, S.A.; Kang, D.; Seo, S.S.; Jeong, J.K.; Yoo, K.Y.; Jeon, Y.T.; Kim, J.W.; Park, N.H.; Kang, S.B.; Lee, H.P. Multiple HPV infection in cervical cancer screened by HPVDNAchip. Cancer Lett. 2003, 198, 187–192. [Google Scholar] [CrossRef]
- Mandishora, R.S.D.; Gjøtterud, K.S.; Lagström, S.; Stray-Pedersen, B.; Duri, K.; Chin’ombe, N.; Nygård, M.; Christiansen, I.K.; Ambur, O.H.; Chirenje, M.Z.; et al. Intra-host sequence variability in human papillomavirus. Papillomavirus Res. 2018, 5, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Mirabello, L.; Yeager, M.; Cullen, M. HPV16 sublineage associations with histology-specific cancer risk using HPV whole-genome sequences in 3200 women. J. Natl. Cancer Inst. 2016, 108, djw100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitt, M.; Dondog, B.; Waterboer, T.; Pawlita, M.; Tommasino, M.; Gheit, T. Abundance of multiple high-risk human papillomavirus (HPV) infections found in cervical cells analyzed by use of an ultrasensitive HPV genotyping assay. J. Clin. Microbiol. 2010, 48, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Siqueira, J.D.; Alvez, B.M.; Prellwitz, I.M.; Furtado, C.; Meyrelles, Â.R.; Machado, E.S.; Seuánez, H.N.; Soares, M.A.; Soares, E.A. Identification of novel human papillomavirus lineages and sublineages in HIV/HPV-coinfected pregnant women by next-generation sequencing. Virology 2016, 493, 202–208. [Google Scholar] [CrossRef]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shea, S.; Muñoz, M.; Ward, S.C.; Beasley, M.B.; Gitman, M.R.; Nowak, M.D.; Houldsworth, J.; Sordillo, E.M.; Ramirez, J.D.; Paniz Mondolfi, A.E. Human Papillomavirus (HPV69/HPV73) Coinfection associated with Simultaneous Squamous Cell Carcinoma of the Anus and Presumed Lung Metastasis. Viruses 2020, 12, 349. https://0-doi-org.brum.beds.ac.uk/10.3390/v12030349
Shea S, Muñoz M, Ward SC, Beasley MB, Gitman MR, Nowak MD, Houldsworth J, Sordillo EM, Ramirez JD, Paniz Mondolfi AE. Human Papillomavirus (HPV69/HPV73) Coinfection associated with Simultaneous Squamous Cell Carcinoma of the Anus and Presumed Lung Metastasis. Viruses. 2020; 12(3):349. https://0-doi-org.brum.beds.ac.uk/10.3390/v12030349
Chicago/Turabian StyleShea, Stephanie, Marina Muñoz, Stephen C. Ward, Mary B. Beasley, Melissa R Gitman, Michael D Nowak, Jane Houldsworth, Emilia Mia Sordillo, Juan David Ramirez, and Alberto E. Paniz Mondolfi. 2020. "Human Papillomavirus (HPV69/HPV73) Coinfection associated with Simultaneous Squamous Cell Carcinoma of the Anus and Presumed Lung Metastasis" Viruses 12, no. 3: 349. https://0-doi-org.brum.beds.ac.uk/10.3390/v12030349