Genotypic Characterization of Epstein Barr Virus in Blood of Patients with Suspected Nasopharyngeal Carcinoma in Ghana

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Site
2.2. Recruitment of Study Participants
2.3. Collection of Blood Samples and DNA Extraction
2.4. Positive Controls
2.5. Detection of EBV by Amplification of Epstein Barr Nuclear Antigen-1 (EBNA-1)
2.6. EBV Genotyping by Epstein Barr Nuclear Antigen 2 (EBNA-2) Nested PCR Amplification
2.7. EBV Load Quantification in Whole Blood by EBNA-1 Real-Time PCR
2.8. Statistical Analysis
3. Results
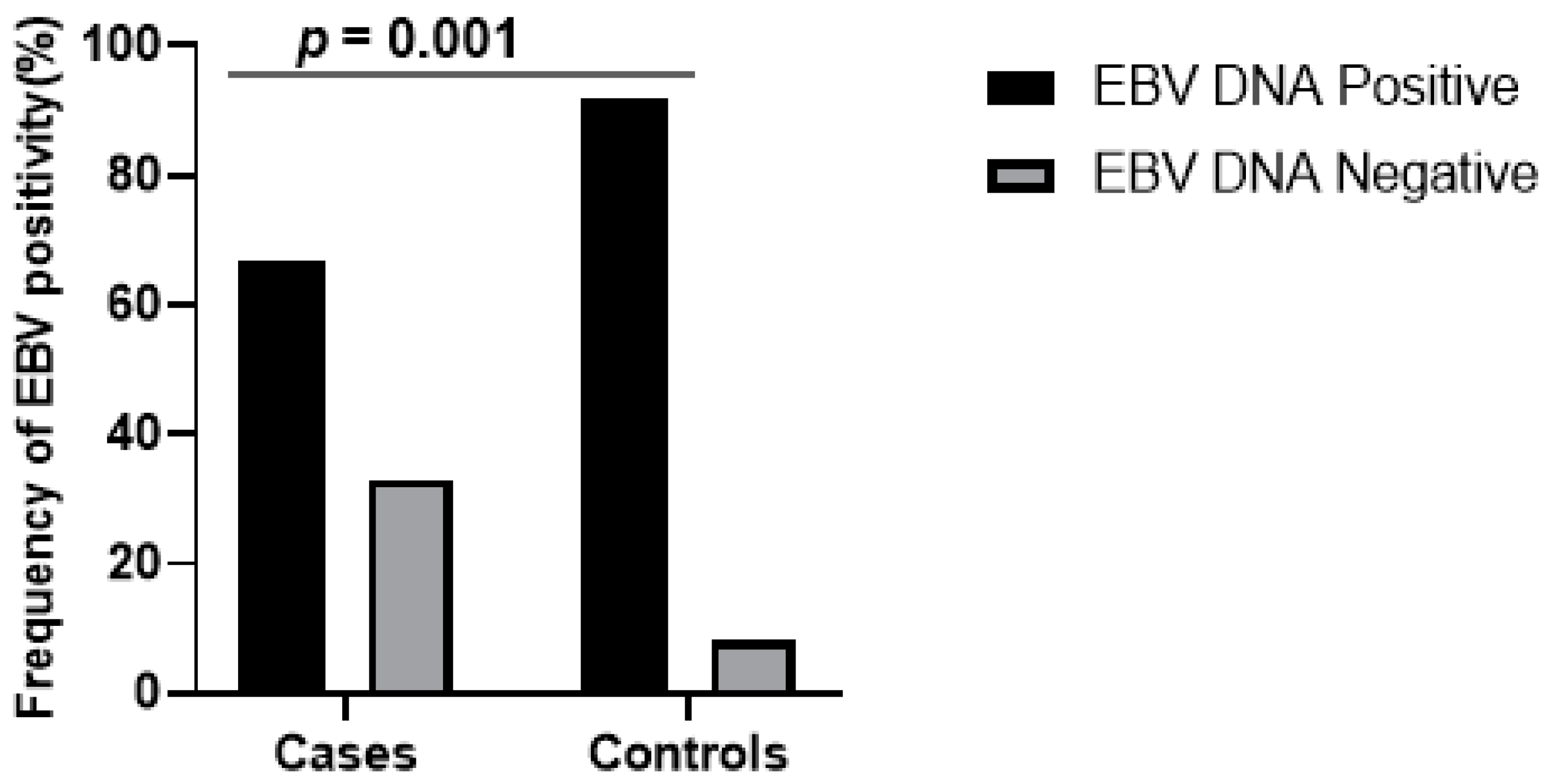
3.1. Demographics of Study Participants and Molecular Detection of EBV in Whole Blood
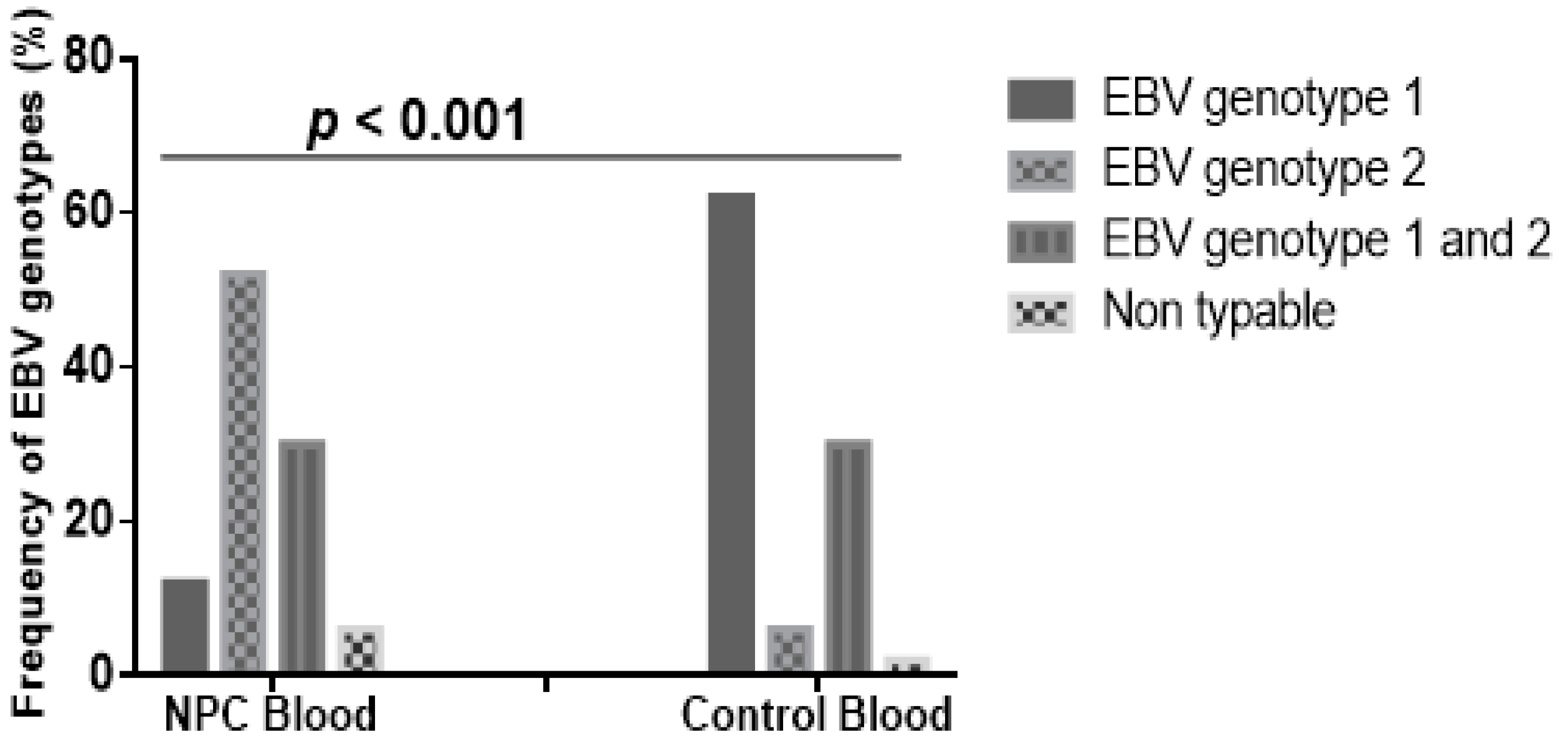
3.2. EBV Genotypes in NPC Patients and Controls of the Study Participants
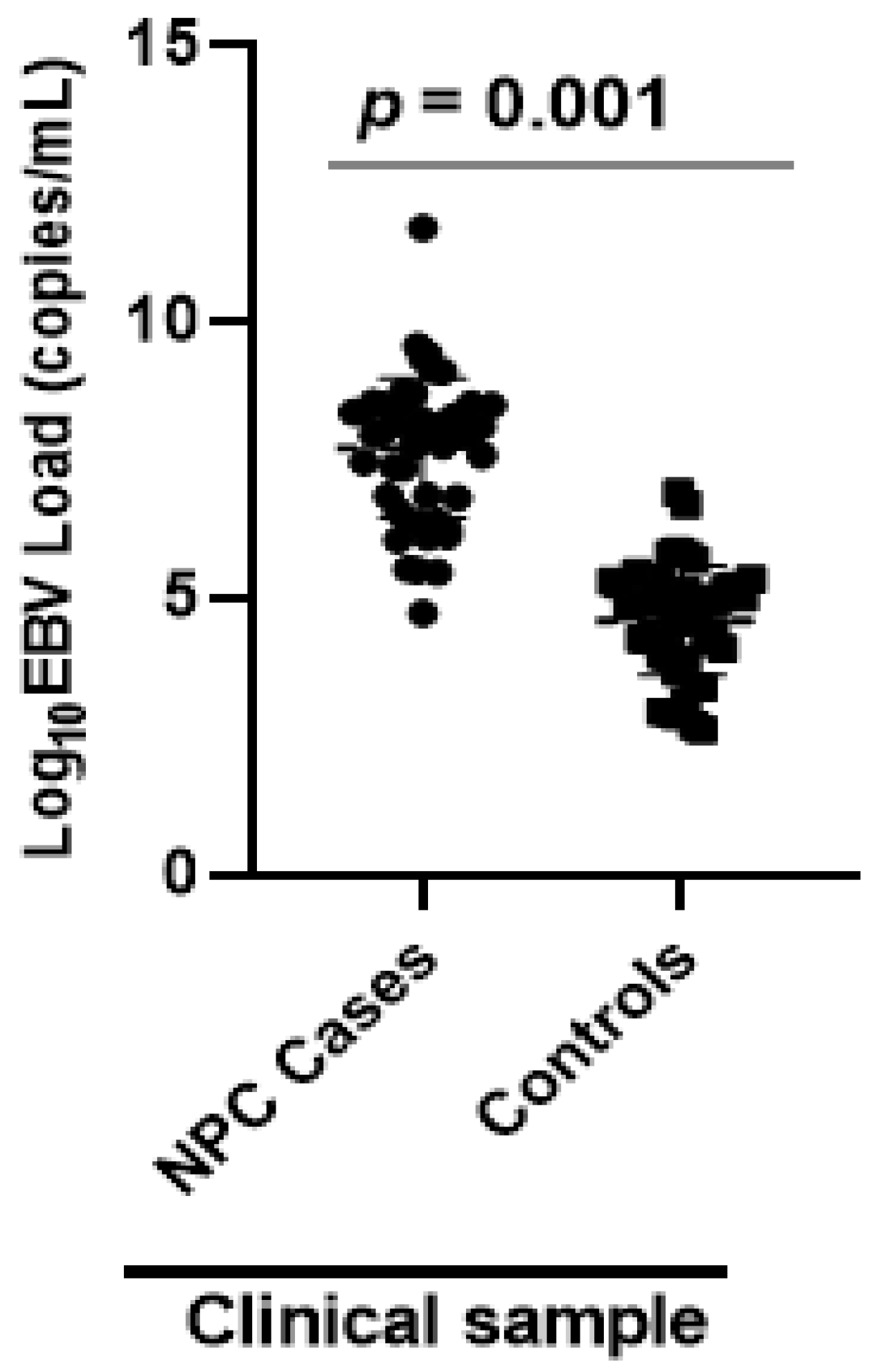
3.3. EBV Load in NPC Patients and Controls
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Disclosure
Conflicts of Interest
References
- Borthakur, P.; Kataki, K.; Keppen, C.; Khamo, V.; Medhi, S.; Deka, M. Expression of Epstein Barr Virus encoded EBNA1 and LMP1 oncoproteins in nasopharyngeal carcinomas from Northeast India. Asian Pac. J. Cancer Prev. 2016, 17, 3411–3416. [Google Scholar]
- Carle, L.N.; Ko, C.C.; Castle, J.T. Nasopharyngeal carcinoma. Head Neck Pathol. 2012, 6, 364–368. [Google Scholar] [CrossRef] [PubMed]
- Breda, E.; Catarino, R.J.F.; Azevedo, I.; Lobão, M.; Monteiro, E.; Medeiros, R. Epstein-barr virus detection in nasopharyngeal carcinoma-implications in a low-risk area. Braz. J. Otorhinolaryngol. 2010, 76, 310–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hila, L.; Farah, F.; Ayari, H.; Ferjaoui, M.; Dehria, W.; Jilani, S.B. Epidemiological study, immunohistochemistry and in situ hybridization studies of nasopharyngeal carcinomas: A Tunisian report. Pathol. Biol. 2009, 57, 427–429. [Google Scholar] [CrossRef] [PubMed]
- Larsen-Reindorf, R.; Owusu-Afriyie, O.; Acheampong, A.O.; Boakye, I.; Awuah, B. A six-year review of head and neck cancers at the Komfo Anokye Teaching Hospital, Kumasi, Ghana. Int. J. Otorhinolaryngol. Head Neck Surg. 2014, 3, 271. [Google Scholar] [CrossRef] [Green Version]
- Kitcher, E.; Yarney, J.; Gyasi, R.; Cheyuo, C. Nasopharyngeal cancer: A review of cases at the Korle-Bu Teaching Hospital. Ghana Med. J. 2004, 38, 104–108. [Google Scholar] [CrossRef]
- Brennan, B. Nasopharyngeal carcinoma. Orphanet J. Rare Dis. 2006, 1, 23. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-H.; Hu, C.-F.; Shao, Q.; Huang, M.-Y.; Hou, J.-H.; Xie, D.; Zeng, Y.X.; Shao, J.Y. Elevated expressions of survivin and VEGF protein are strong independent predictors of survival in advanced nasopharyngeal carcinoma. J. Transl. Med. 2008, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, G.; Blumenthal, M.; Katz, A. Interaction of human tumor viruses with host cell surface receptors and cell entry. Viruses 2015, 7, 2592–2617. [Google Scholar] [CrossRef] [PubMed]
- Longnecker, R.M.; Kieff, E.; Cohen, J.I. Epstein-Barr Virus. Fields Virology, 6th ed.; Wolters Kluwer Health Adis (ESP): Bridgewater, NJ, USA, 2013. [Google Scholar]
- Sathiyamoorthy, K.; Hu, Y.X.; Möhl, B.S.; Chen, J.; Longnecker, R.; Jardetzky, T.S. Structural basis for Epstein–Barr virus host cell tropism mediated by gp42 and gHgL entry glycoproteins. Nat. Commun. 2016, 7, 13557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peh, S.-C.; Kim, L.-H.; Poppema, S. Frequent presence of subtype a virus in Epstein-Barr virus-associated malignancies. Pathology 2002, 34, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, P. Cytomegalovirus. In Principles and Practice of Clinical Virology; Zuckerman, A.J., Banatvala, J.E., Pattison, J.R., Griffiths, P.D., Schoub, B.D., Eds.; John Wiley and Sons, Ltd.: West Suusex, UK, 2004. [Google Scholar]
- Klemenc, P.; Marin, J.; Šoba, E.; Gale, N.; Koren, S.; Strojan, P. Distribution of Epstein–Barr virus genotypes in throat washings, sera, peripheral blood lymphocytes and in EBV positive tumor biopsies from Slovenian patients with nasopharyngeal carcinoma. J. Med. Virol. 2006, 78, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Hatton, O.L.; Harris-Arnold, A.; Schaffert, S.; Krams, S.M.; Martinez, O.M. The interplay between Epstein–Barr virus and B lymphocytes: Implications for infection, immunity, and disease. Immunol. Res. 2014, 58, 268–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salahuddin, S.; Khan, J.; Azhar, J.; Whitehurst, C.B.; Qadri, I.; Shackelford, J.; Pagano, J.S.; Muhammad, D.; Richards, K.L. Prevalence of Epstein–Barr Virus Genotypes in Pakistani Lymphoma Patients. Asian Pac. J. Cancer Prev. 2018, 19, 3153. [Google Scholar] [CrossRef] [PubMed]
- Smatti, M.K.; Al-Sadeq, D.W.; Ali, N.H.; Pintus, G.; Abou-Saleh, H.; Nasrallah, G.K. Epstein–Barr virus epidemiology, serology, and genetic variability of LMP-1 oncogene among healthy population: An update. Front. Oncol. 2018, 8, 211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trottier, H.; Alfieri, C.; Robitaille, N.; Duval, M.; Buteau, C.; Tucci, M.; Lacroix, J. Transfusion-related Epstein-Barr virus (EBV) infection among stem cell transplant recipients: A retrospective cohort study in children. Am. Soc. Hematol. 2010, 116, 3340. [Google Scholar] [CrossRef]
- San-Juan, R.; Manuel, O.; Hirsch, H.H.; Fernandez-Ruiz, M.; Lopez-Medrano, F.; Comoli, P.; Caillard, S.; Grossi, P.; Aguado, J.M. Current preventive strategies and management of Epstein-Barr virus-related post-transplant lymphoproliferative disease in solid organ transplantation in Europe. Results of the ESGICH Questionnaire-based Cross-sectional Survey. Clin. Microbiol. Infect. 2015, 21, 604.e1–604.e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edris, A.; Mohamed, M.A.; Mohamed, N.S.; Siddig, E.E. Erratum to: Molecular Detection of Epstein—Barr virus in Nasopharyngeal Carcinoma among Sudanese population. Infect Agents Cancer 2016, 11, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banko, A.V.; Lazarevic, I.B.; Folic, M.M.; Djukic, V.B.; Cirkovic, A.M.; Karalic, D.Z.; Cupic, M.D.; Jovanovic, T.P. Characterization of the variability of Epstein-Barr virus genes in nasopharyngeal biopsies: Potential predictors for carcinoma progression. PLoS ONE 2016, 11, e0153498. [Google Scholar] [CrossRef] [PubMed]
- Ayee, R.; Ofori, M.E.O.; Wright, E.; Quaye, O. Epstein Barr Virus Associated Lymphomas and Epithelia Cancers in Humans. Int. J. Cancer 2020, 11, 1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwok, H.; Chan, K.W.; Chan, K.H.; Chiang, A.K.S. Distribution, persistence and interchange of Epstein-Barr virus strains among PBMC, plasma and saliva of primary infection subjects. PLoS ONE 2015, 10, e0120710. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.D.; Chan, A.T.; Chan, L.Y.; Leung, S.-F.; Lam, C.-W.; Huang, D.P.; Johnson, P.J. Molecular prognostication of nasopharyngeal carcinoma by quantitative analysis of circulating Epstein-Barr virus DNA. Cancer Res. 2000, 60, 6878–6881. [Google Scholar] [PubMed]
- Chen, Y.; Zhao, W.; Lin, L.; Xiao, X.; Zhou, X.; Ming, H.; Huang, T.; Liao, J.; Li, Y.; Zeng, X.; et al. Nasopharyngeal Epstein-Barr virus load: An efficient supplementary method for population-based nasopharyngeal carcinoma screening. PLoS ONE 2015, 10, e0132669. [Google Scholar] [CrossRef] [PubMed]
- He, S.S.; Wang, Y.; Bao, Y.; Cai, X.Y.; Yang, X.L.; Chen, D.M.; Chen, Y.; Lu, L.X. Dynamic changes in plasma Epstein–Barr virus DNA load during treatment have prognostic value in nasopharyngeal carcinoma: A retrospective study. Cancer Med. 2018, 7, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-C.; Wang, W.-Y.; Chen, K.Y.; Wei, Y.-H.; Liang, W.-M.; Jan, J.-S.; Jiang, R.S. Quantification of plasma Epstein–Barr virus DNA in patients with advanced nasopharyngeal carcinoma. N. Engl. J. Med. 2004, 350, 2461–2470. [Google Scholar] [CrossRef] [PubMed]
- Lay, M.-L.J.; Lucas, R.M.; Ratnamohan, M.; Taylor, J.; Ponsonby, A.-L.; Dwyer, D.E. Measurement of Epstein-Barr virus DNA load using a novel quantification standard containing two EBV DNA targets and SYBR Green I dye. Virol. J. 2010, 7, 252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shan, J.; Pow, E.H.; Tsang, P.C.; Perera, R.A.; Kwong, D.L. Comparison of two laboratory extraction techniques for the detection of E pstein–B arr virus in the saliva of nasopharyngeal carcinoma patients. J. Investig. Clin. Dent. 2014, 5, 104–108. [Google Scholar] [CrossRef]
- Stevens, S.J.; Verkuijlen, S.A.; Hariwiyanto, B.; Fachiroh, J.; Paramita, D.K.; Tan, I.B.; Haryana, S.M.; Middeldorp, J.M. Diagnostic value of measuring Epstein-Barr virus (EBV) DNA load and carcinoma-specific viral mRNA in relation to anti-EBV immunoglobulin A (IgA) and IgG antibody levels in blood of nasopharyngeal carcinoma patients from Indonesia. J. Clin. Microbiol. 2005, 43, 3066–3073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, S.J.; Pronk, I.; Middeldorp, J.M. Toward standardization of Epstein-Barr virus DNA load monitoring: Unfractionated whole blood as preferred clinical specimen. J. Clin. Microbiol. 2001, 39, 1211–1216. [Google Scholar] [CrossRef] [PubMed]
- Lourembam, D.S.; Singh, A.R.; Sharma, T.D.; Singh, T.S.; Singh, T.R.; Singh, L.S. Evaluation of risk factors for nasopharyngeal carcinoma in a high-risk area of India, the Northeastern Region. Asian Pac. J. Cancer Prev. 2015, 16, 4927–4935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adham, M.; Greijer, A.E.; Verkuijlen, S.A.; Juwana, H.; Fleig, S.; Rachmadi, L.; Malik, O.; Kurniawan, A.N.; Roezin, A.; Gondhowiardjo, S.; et al. Epstein-Barr virus DNA load in nasopharyngeal brushings and whole blood in nasopharyngeal carcinoma patients before and after treatment. Clin. Cancer Res. 2013, 19, 2175–2186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorley-Lawson, D.A.; Gross, A. Persistence of the Epstein–Barr virus and the origins of associated lymphomas. N. Engl. J. Med. 2004, 350, 1328–1337. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.A.; Zhang, J.; Chan, A.T.; Lei, K.I.; Leung, S.-F.; Chan, L.Y.; Chow, K.C.; Lo, Y.D. Molecular characterization of circulating EBV DNA in the plasma of nasopharyngeal carcinoma and lymphoma patients. Cancer Res. 2003, 63, 2028–2032. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Gene Target | Primer Name | Primer Sequence | Amplicon Size |
|---|---|---|---|
| EBNA-1 | QP1 (forward) | (GCC GGT GTG TTC GTA TAT GG) | 213 bp |
| QP2 (reverse) | (CAA AAC CTC AGC AAA TATATG AG) | ||
| EBNA-2 | First round primers | 801 bp | |
| EBNA-2F (sense) | (TGGAAACCCGTCACTCTC) | ||
| EBNA-2I (antisense) | (TAATGGCATAGGTGGAATG) | ||
| Second round primers | 250 bp 300 bp | ||
| EBNA-2C (common sense primer) | (AGGGATGCCTGGACACAAGA) | ||
| EBNA-2G (type-1 antisense) | (GCCTCGGTTGTGACAGAG) | ||
| EBNA-2B (type-2 antisense) | (TTGAAGAGTATGTCCTAAGG) | ||
| Beta globulin | B-globulin F | (ACACAACTGTGTTCACTAGC) | 119 bp |
| B-globulin R | (CAACTTCATCCACGTTCACC) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayee, R.; Ofori, M.E.O.; Tagoe, E.A.; Languon, S.; Searyoh, K.; Armooh, L.; Bilson-Amoah, E.; Baidoo, K.; Kitcher, E.; Wright, E.; et al. Genotypic Characterization of Epstein Barr Virus in Blood of Patients with Suspected Nasopharyngeal Carcinoma in Ghana. Viruses 2020, 12, 766. https://0-doi-org.brum.beds.ac.uk/10.3390/v12070766
Ayee R, Ofori MEO, Tagoe EA, Languon S, Searyoh K, Armooh L, Bilson-Amoah E, Baidoo K, Kitcher E, Wright E, et al. Genotypic Characterization of Epstein Barr Virus in Blood of Patients with Suspected Nasopharyngeal Carcinoma in Ghana. Viruses. 2020; 12(7):766. https://0-doi-org.brum.beds.ac.uk/10.3390/v12070766
Chicago/Turabian StyleAyee, Richmond, Maame Ekua Oforiwaa Ofori, Emmanuel Ayitey Tagoe, Sylvester Languon, Kafui Searyoh, Louis Armooh, Estella Bilson-Amoah, Kenneth Baidoo, Emmanuel Kitcher, Edward Wright, and et al. 2020. "Genotypic Characterization of Epstein Barr Virus in Blood of Patients with Suspected Nasopharyngeal Carcinoma in Ghana" Viruses 12, no. 7: 766. https://0-doi-org.brum.beds.ac.uk/10.3390/v12070766