
Global Utilization Trends of Direct Acting Antivirals (DAAs) during the COVID-19 Pandemic: A Time Series Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Source
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Blach, S.; Zeuzem, S.; Manns, M.; Altraif, I.; Duberg, A.-S.; Muljono, D.H.; Waked, I.; Alavian, S.M.; Lee, M.-H.; Negro, F.; et al. Global prevalence and genotype distribution of hepatitis C virus infection in 2015: A modelling study. Lancet Gastroenterol. Hepatol. 2017, 2, 161–176. [Google Scholar] [CrossRef] [Green Version]
- Shepard, C.W.; Finelli, L.; Alter, M.J. Global epidemiology of hepatitis C virus infection. Lancet Infect. Dis. 2005, 5, 558–567. [Google Scholar] [CrossRef]
- Shakeri, A.; Srimurugathasan, N.; Suda, K.J.; Gomes, T.; Tadrous, M. Spending on Hepatitis C Antivirals in the United States and Canada, 2014 to 2018. Value Health 2020, 23, 1137–1141. [Google Scholar] [CrossRef]
- Buckley, G.J.; Strom, B.L. Eliminating the Public Health Problem of Hepatitis B and C in the United States: Phase One Report; The National Academies Press: Washington, DC, USA, 2016; ISBN 0309437997. [Google Scholar]
- Holmes, J.A.; Rutledge, S.M.; Chung, R.T. Direct-acting antiviral treatment for hepatitis C. Lancet 2019, 393, 1392–1394. [Google Scholar] [CrossRef]
- Van Der Meer, A.J.; Veldt, B.J.; Feld, J.J.; Wedemeyer, H.; Dufour, J.F.; Lammert, F.; Duarte-Rojo, A.; Heathcote, E.J.; Manns, M.P.; Kuske, L.; et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. J. Am. Med. Assoc. 2012, 308, 2584–2593. [Google Scholar] [CrossRef]
- Janjua, N.Z.; Chong, M.; Kuo, M.; Woods, R.; Wong, J.; Yoshida, E.M.; Sherman, M.; Butt, Z.A.; Samji, H.; Cook, D.; et al. Long-term effect of sustained virological response on hepatocellular carcinoma in patients with hepatitis C in Canada. J. Hepatol. 2017, 66, 504–513. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Combating Hepatitis B and C to Reach Elimination by 2030: Advocacy Brief; World Health Organization: Geneva, Switzerland, 2016; Available online: http://apps.who.int/iris/bitstream/hadle/10665/206453/WHO_HIV_2016.04_eng.pdf?sequence=1 (accessed on 25 January 2021).
- Myers, S.; Khosa, G.; Kuo, I.F.; Janzen, D.; Alessi-Severini, S. Moving towards universal coverage of direct-acting antiviral therapies for hepatitis c infection in canada: An environmental scan of canadian provinces and international jurisdictions. J. Pharm. Pharm. Sci. 2018, 21, 271s–308s. [Google Scholar] [CrossRef]
- Lanièce Delaunay, C.; Greenwald, Z.R.; Minoyan, N.; Artenie, A.A.; Jeong, D.; Marathe, G.; Saeed, Y.A.; Kolla, G.; Kunden, R.D.; Okwor, C.I.A.; et al. Striving toward hepatitis C elimination in the era of COVID-19. Can. Liver J. 2021, 4, e20200027. [Google Scholar] [CrossRef]
- Wingrove, C.; Ferrier, L.; James, C.; Wang, S. The impact of COVID-19 on hepatitis elimination. Lancet Gastroenterol. Hepatol. 2020, 5, 792–794. [Google Scholar] [CrossRef]
- Gamkrelidze, I.; Pawlotsky, J.M.; Lazarus, J.V.; Feld, J.J.; Zeuzem, S.; Bao, Y.; Gabriela Pires dos Santos, A.; Sanchez Gonzalez, Y.; Razavi, H. Progress towards hepatitis C virus elimination in high-income countries: An updated analysis. Liver Int. 2021, 41. [Google Scholar] [CrossRef] [PubMed]
- IQVIA MIDAS. Available online: https://www.iqvia.com/solutions/commercialization/brand-strategy-and-management/market-measurement/midas (accessed on 25 January 2020).
- Durup, D.; Schaffalitzky de Muckadell, P.; Strom, C.C. Evaluation of the reported rates of hypersensitivity reactions associated with iron dextran and ferric carboxymaltose based on global data from VigiBaseTM and IQVIATM MIDAS® over a ten-year period from 2008 to 2017. Expert Rev. Hematol. 2020, 13, 557–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IQVIA. IQVIA Quality Assurance: Acts 2019. 2020. Available online: https://www.iqvia.com/-/media/iqvia/pdfs/library/publications/2019-acts-annual-report.pdf?_=1625260787299 (accessed on 29 January 2021).
- Jackson, C.; Hsia, Y.; Bielicki, J.A.; Ellis, S.; Stephens, P.; Wong, I.C.K.; Sharland, M. Estimating global trends in total and childhood antibiotic consumption, 2011–2015. BMJ Glob. Health 2019, 4, e001241. [Google Scholar] [CrossRef] [Green Version]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef] [Green Version]
- United Nations. World Economic Situation and Prospects 2021; United Nations: Geneva, Switzerland, 2020. Available online: https://www.un.org/development/desa/dpad/wp-content/uploads/sites/45/WESP2021_FullReport.pdf (accessed on 30 January 2021).
- United Nations (UN). Population Division World Population Prospects. Available online: https://population.un.org/wpp/ (accessed on 3 March 2021).
- Jandoc, R.; Burden, A.M.; Mamdani, M.; Lévesque, L.E.; Cadarette, S.M. Interrupted time series analysis in drug utilization research is increasing: Systematic review and recommendations. J. Clin. Epidemiol. 2015, 68, 950–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaffer, A.L.; Dobbins, T.A.; Pearson, S.A. Interrupted time series analysis using autoregressive integrated moving average (ARIMA) models: A guide for evaluating large-scale health interventions. BMC Med. Res. Methodol. 2021, 21, 1–12. [Google Scholar] [CrossRef]
- Moynihan, R.; Sanders, S.; Michaleff, Z.A.; Scott, A.M.; Clark, J.; To, E.J.; Jones, M.; Kitchener, E.; Fox, M.; Johansson, M.; et al. Impact of COVID-19 pandemic on utilisation of healthcare services: A systematic review. BMJ Open 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Kondili, L.A.; Marcellusi, A.; Ryder, S.; Craxì, A. Will the COVID-19 pandemic affect HCV disease burden? Dig. Liver Dis. 2020, 52, 947–949. [Google Scholar] [CrossRef] [PubMed]
- Konstantelos, N.; Shakeri, A.; McCormack, D.; Feld, J.J.; Gomes, T.; Tadrous, M. Impact of COVID-19 on prescribing trends of direct-acting antivirals for the treatment of Hepatitis, C. in Ontario, Canada. Am. J. Gastroenterol. 2021. [Google Scholar] [CrossRef]
- Blach, S.; Kondili, L.A.; Aghemo, A.; Cai, Z.; Dugan, E.; Estes, C.; Gamkrelidze, I.; Ma, S.; Pawlotsky, J.M.; Razavi-Shearer, D.; et al. Impact of COVID-19 on global HCV elimination efforts. J. Hepatol. 2021, 74, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Razavi, H.; Sanchez Gonzalez, Y.; Yuen, C.; Cornberg, M. Global timing of hepatitis C virus elimination in high-income countries. Liver Int. 2020, 40, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Li, H.C.; Lo, S.Y. Hepatitis C virus: Virology, diagnosis and treatment. World J. Hepatol. 2015, 7, 1377–1389. [Google Scholar] [CrossRef] [PubMed]
- Boucher, L.M.; Bayoumi, A.M.; Mark, A.E.; Cooper, C.; Martin, A.; Marshall, Z.; Boyd, R.; Oickle, P.; Diliso, N.; Pineau, D.; et al. Hepatitis C Testing, Status and Treatment among Marginalized People Who Use Drugs in an Inner City Setting: An Observational Cohort Study. Subst. Use Misuse 2019, 54, 18–30. [Google Scholar] [CrossRef]
- Graham, C.S.; Swan, T. A path to eradication of hepatitis C in low- and middle-income countries. Antivir. Res. 2015, 119, 89–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tordrup, D.; Hutin, Y.; Stenberg, K.; Lauer, J.A.; Hutton, D.W.; Toy, M.; Scott, N.; Bulterys, M.; Ball, A.; Hirnschall, G. Additional resource needs for viral hepatitis elimination through universal health coverage: Projections in 67 low-income and middle-income countries, 2016–2030. Lancet Glob. Health 2019, 7, e1180–e1188. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
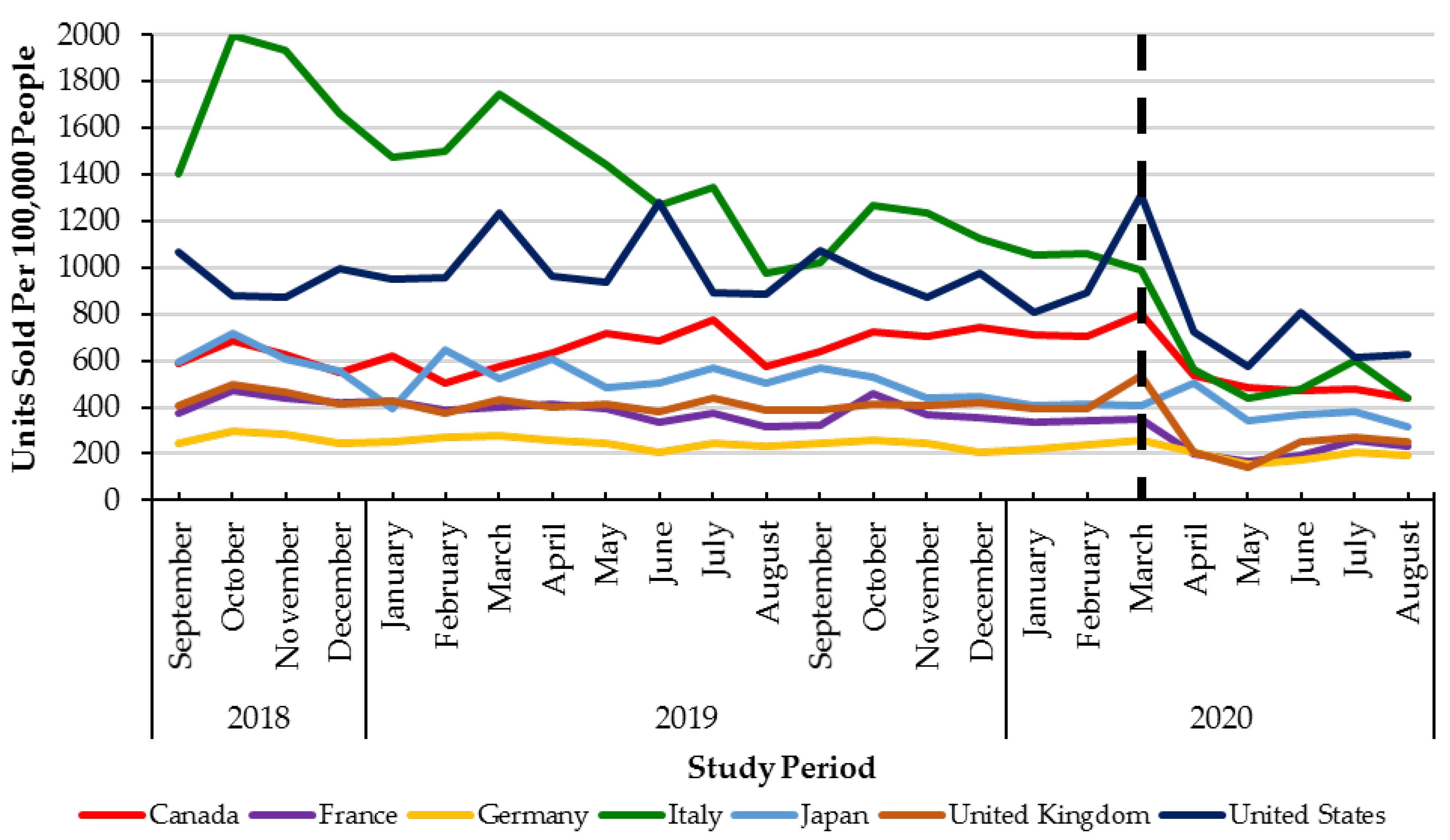
| G7 Countries | Percent Change 1 (%) | Change in Trend of Monthly Direct Acting Antiviral Utilization 2 |
|---|---|---|
| Canada | −18 | p = 0.0299 |
| France | −37 | p = 0.3399 |
| Germany | −19 | p = 0.0150 |
| Italy | −58 | p = 0.2008 |
| Japan | −28 | p = 0.7015 |
| United Kingdom | −32 | p = 0.0004 |
| United States of America | −24 | p = 0.0003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shakeri, A.; Konstantelos, N.; Chu, C.; Antoniou, T.; Feld, J.; Suda, K.J.; Tadrous, M. Global Utilization Trends of Direct Acting Antivirals (DAAs) during the COVID-19 Pandemic: A Time Series Analysis. Viruses 2021, 13, 1314. https://0-doi-org.brum.beds.ac.uk/10.3390/v13071314
Shakeri A, Konstantelos N, Chu C, Antoniou T, Feld J, Suda KJ, Tadrous M. Global Utilization Trends of Direct Acting Antivirals (DAAs) during the COVID-19 Pandemic: A Time Series Analysis. Viruses. 2021; 13(7):1314. https://0-doi-org.brum.beds.ac.uk/10.3390/v13071314
Chicago/Turabian StyleShakeri, Ahmad, Natalia Konstantelos, Cherry Chu, Tony Antoniou, Jordan Feld, Katie J. Suda, and Mina Tadrous. 2021. "Global Utilization Trends of Direct Acting Antivirals (DAAs) during the COVID-19 Pandemic: A Time Series Analysis" Viruses 13, no. 7: 1314. https://0-doi-org.brum.beds.ac.uk/10.3390/v13071314