
One-Year Outcomes after Ledipasvir/Sofosbuvir Treatment of Chronic Hepatitis C in Teenagers with and without Significant Liver Fibrosis—A Case Series Report



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Transient Elastography (TE)
2.3. Biomarker Evaluation
2.4. Ethical Statement
3. Results
3.1. Participants
3.2. Treatment Outcomes
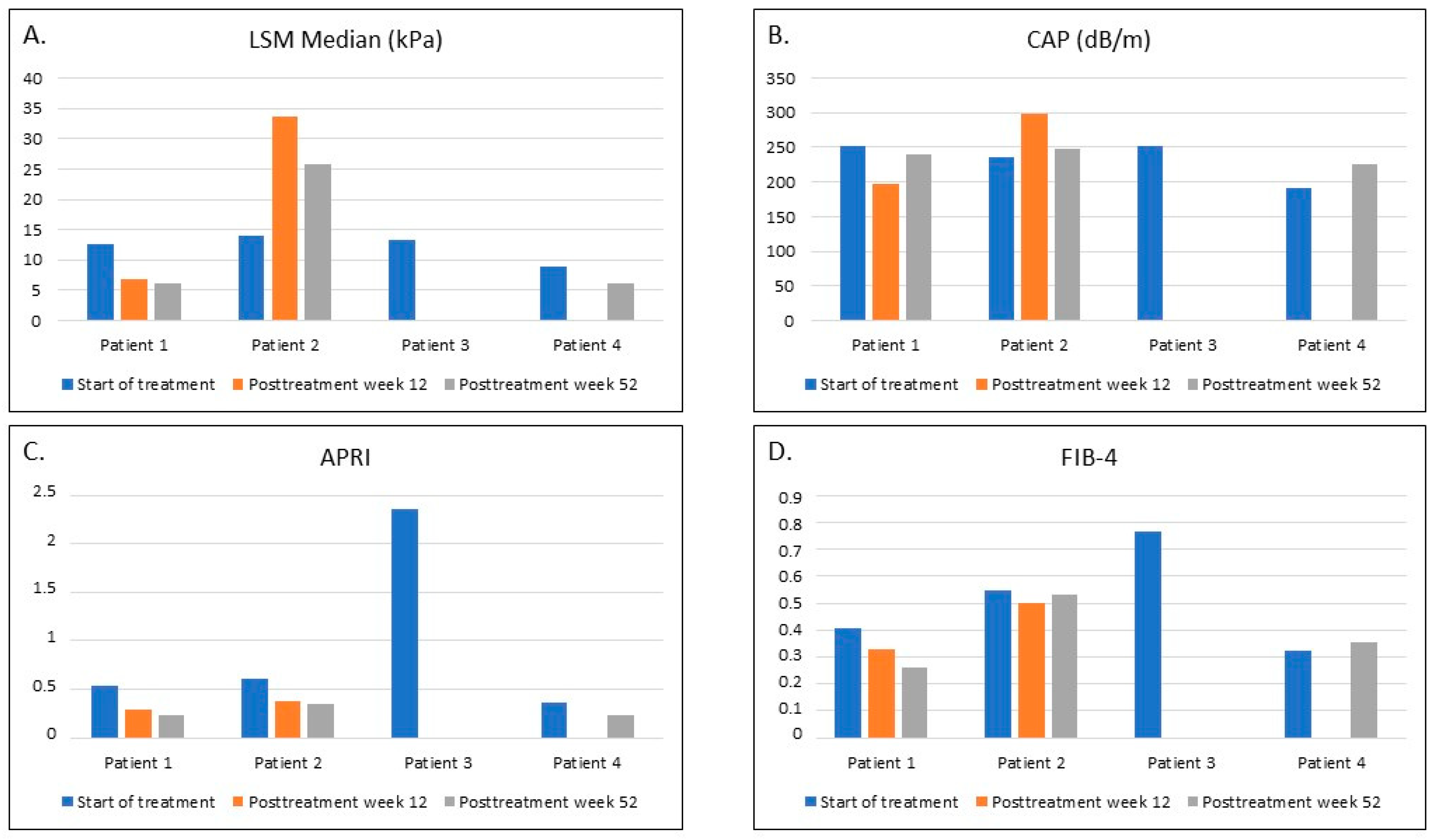
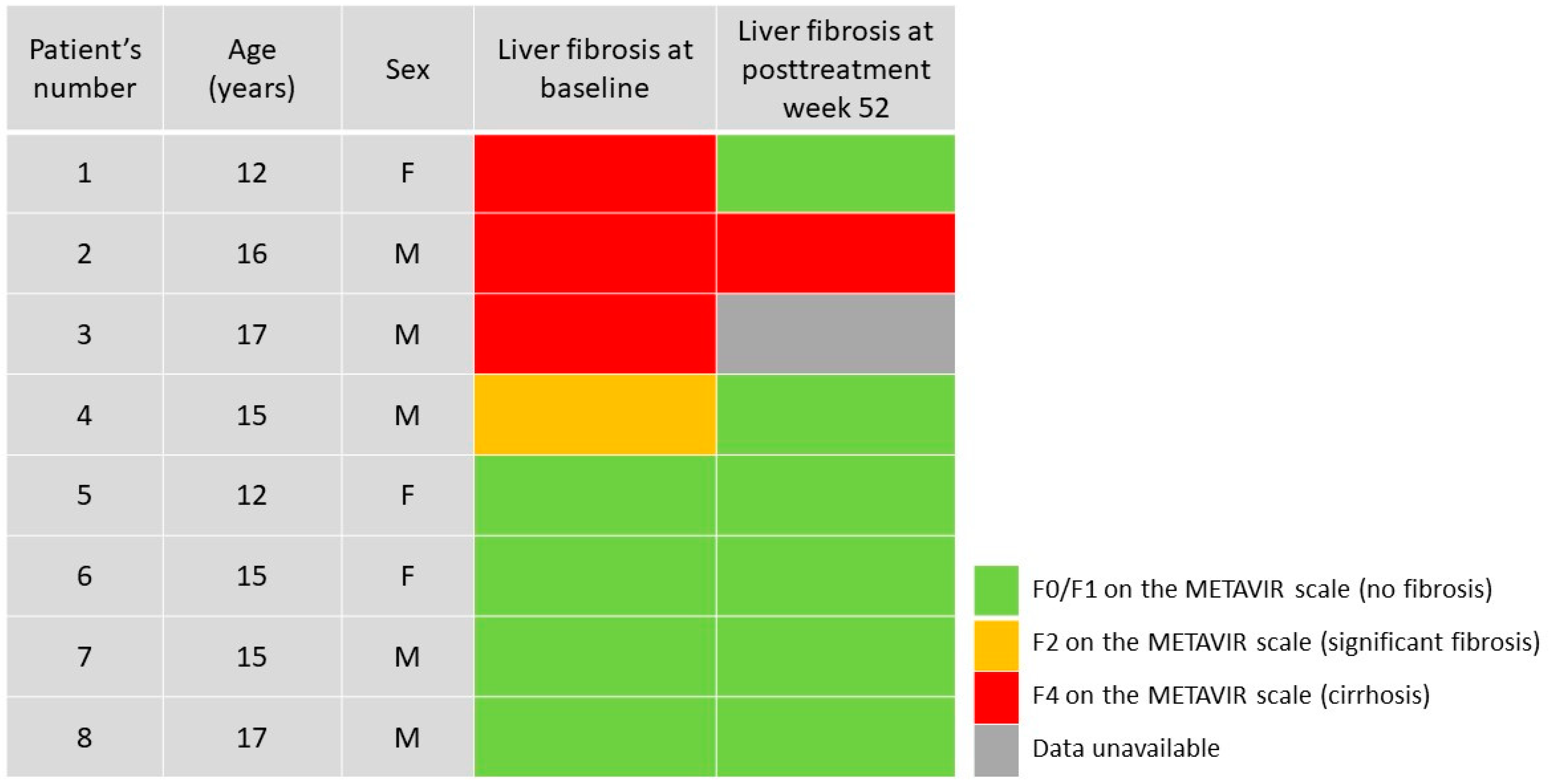
3.3. Liver Fibrosis and Steatosis after the Treatment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bortolotti, F.; Verucchi, G.; Camma, C.; Cabibbo, G.; Zancan, L.; Indolfi, G.; Giacchino, R.; Marcellini, M.; Marazzi, M.G.; Barbera, C.; et al. Long-term course of chronic hepatitis C in children: From viral clearance to end-stage liver disease. Gastroenterology 2008, 134, 1900–1907. [Google Scholar] [CrossRef]
- The European Paediatric Hepatitis C Virus Network. Three broad modalities in the natural history of vertically acquired hepatitis C virus infection. Clin. Infect. Dis. 2005, 41, 45–51. [Google Scholar] [CrossRef]
- Jara, P.; Resti, M.; Hierro, L.; Giacchino, R.; Barbera, C.; Zancan, L.; Crivellaro, C.; Sokal, E.; Azzari, C.; Guido, M.; et al. Chronic Hepatitis C Virus Infection in Childhood: Clinical Patterns and Evolution in 224 White Children. Clin. Infect. Dis. 2003, 36, 275–280. [Google Scholar] [CrossRef] [Green Version]
- Pokorska-Śpiewak, M.; Kowalik-Mikołajewska, B.; Aniszewska, M.; Pluta, M.; Walewska-Zielecka, B.; Marczyńska, M. Determinants of liver disease progression in children with chronic hepatitis C virus infection. Pol. J. Pathol. 2015, 4, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Guido, M.; Bortolotti, F.; Leandro, G.; Jara, P.; Hierro, L.; Larrauri, J.; Barbera, C.; Giacchino, R.; Zancan, L.; Balli, F.; et al. Fibrosis in Chronic Hepatitis C Acquired in Infancy: Is It Only a Matter of Time? Am. J. Gastroenterol. 2003, 98, 660–663. [Google Scholar] [CrossRef] [PubMed]
- Pokorska-Śpiewak, M.; Dobrzeniecka, A.; Lipińska, M.; Tomasik, A.; Aniszewska, M.; Marczyńska, M. Liver Fibrosis Evaluated With Transient Elastography in 35 Children with Chronic Hepatitis C Virus Infection. Pediatr. Infect. Dis. J. 2021, 40, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Turkova, A.; Volynets, G.V.; Crichton, S.; Skvortsova, T.A.; Panfilova, V.N.; Rogozina, N.V.; Khavkin, A.I.; Tumanova, E.L.; Indolfi, G.; Thorne, C. Advanced liver disease in Russian children and adolescents with chronic hepatitis C. J. Viral Hepat. 2019, 26, 881–892. [Google Scholar] [CrossRef] [Green Version]
- Modin, L.; Arshad, A.; Wilkes, B.; Benselin, J.; Lloyd, C.; Irving, W.L.; Kelly, D.A. Epidemiology and natural history of hepatitis C virus infection among children and young people. J. Hepatol. 2019, 70, 371–378. [Google Scholar] [CrossRef]
- Indolfi, G.; Giometto, S.; Serranti, D.; Bettiol, A.; Bigagli, E.; De Masi, S.; Lucenteforte, E. Systematic review with meta-analysis: The efficacy and safety of direct-acting antivirals in children and adolescents with chronic hepatitis C virus infection. Aliment. Pharmacol. Ther. 2020, 52, 1125–1133. [Google Scholar] [CrossRef]
- Mogahed, E.A.; El-Karaksy, H.; Abdullatif, H.; Yasin, N.A.; Nagy, A.; Alem, S.A.; Eldeen, H.G.; El-Raziky, M.S. Improvement in Liver Stiffness in Pediatric Patients with Hepatitis C Virus after Treatment with Direct Acting Antivirals. J. Pediatr. 2021, 233, 126–131. [Google Scholar] [CrossRef]
- Indolfi, G.; Hierro, L.; Dezsofi, A.; Jahnel, J.; Debray, D.; Hadzic, N.; Czubkowski, P.; Gupte, G.; Mozer-Glassberg, Y.; van der Woerd, W.; et al. Treatment of Chronic Hepatitis C Virus Infection in Children: A Position Paper by the Hepatology Committee of European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Zeng, J.; Zhang, X.; Sun, C.; Pan, Q.; Lu, W.-Y.; Chen, Q.; Huang, L.-S.; Fan, J.-G. Feasibility study and reference values of FibroScan 502 with M probe in healthy preschool children aged 5 years. BMC Pediatr. 2019, 19, 129. [Google Scholar] [CrossRef] [PubMed]
- Castéra, L.; Vergniol, J.; Foucher, J.; Le Bail, B.; Chanteloup, E.; Haaser, M.; Darriet, M.; Couzigou, P.; de Lédinghen, V. Prospective comparison of transient elastography, Fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis C. Gastroenterology 2005, 128, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Sasso, M.; Miette, V.; Sandrin, L.; Beaugrand, M. The controlled attenuation parameter (CAP): A novel tool for the non-invasive evaluation of steatosis using Fibroscan®. Clin. Res. Hepatol. Gastroenterol. 2012, 36, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Wai, C.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [Green Version]
- Lin, Z.-H.; Xin, Y.-N.; Dong, Q.-J.; Wang, Q.; Jiang, X.-J.; Zhan, S.-H.; Sun, Y.; Xuan, S.-Y. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: An updated meta-analysis. Hepatology 2010, 53, 726–736. [Google Scholar] [CrossRef]
- Balistreri, W.F.; Murray, K.F.; Rosenthal, P.; Bansal, S.; Lin, C.-H.; Kersey, K.; Massetto, B.; Zhu, Y.; Kanwar, B.; German, P.; et al. The safety and effectiveness of ledipasvir-sofosbuvir in adolescents 12–17 years old with hepatitis C virus genotype 1 infection. Hepatology 2017, 66, 371–378. [Google Scholar] [CrossRef]
- Schwarz, K.B.; Rosenthal, P.; Murray, K.F.; Honegger, J.R.; Hardikar, W.; Hague, R.; Mittal, N.; Massetto, B.; Brainard, D.M.; Hsueh, C.; et al. Ledipasvir-Sofosbuvir for 12 Weeks in Children 3 to <6 Years Old with Chronic Hepatitis C. Hepatology 2020, 71, 422–430. [Google Scholar] [CrossRef]
- Murray, K.F.; Balistreri, W.F.; Bansal, S.; Whitworth, S.; Evans, H.; Gonzalez-Peralta, R.P.; Wen, J.; Massetto, B.; Kersey, K.; Shao, J.; et al. Safety and Efficacy of Ledipasvir-Sofosbuvir With or Without Ribavirin for Chronic Hepatitis C in Children Ages 6-11. Hepatology 2018, 68, 2158–2166. [Google Scholar] [CrossRef] [Green Version]
- Rogers, M.E.; Balistreri, W.F. Cascade of care for children and adolescents with chronic hepatitis C. World J. Gastroenterol. 2021, 27, 1117–1131. [Google Scholar] [CrossRef]
- Chen, S.-H.; Lai, H.-C.; Chen, S.-H.; Chiang, W.-P.; Su, S.-H.; Lin, C.-H.; Kao, J.-T.; Chuang, P.-H.; Hsu, W.-F.; Wang, H.-W.; et al. Changes in liver stiffness measurement using acoustic radiation force impulse elastography after antiviral therapy in patients with chronic hepatitis C. PLoS ONE 2018, 13, e0190455. [Google Scholar] [CrossRef]
- Rockey, D.C. Fibrosis reversal after hepatitis C virus elimination. Curr. Opin. Gastroenterol. 2019, 35, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Knop, V.; Hoppe, D.; Welzel, T.; Vermehren, J.; Herrmann, E.; Friedrich-Rust, M.; Sarrazin, C.; Zeuzem, S.; Welker, M.-W. Regression of fibrosis and portal hypertension in HCV-associated cirrhosis and sustained virologic response after interferon-free antiviral therapy. J. Viral Hepat. 2016, 23, 994–1002. [Google Scholar] [CrossRef]
- Bachofner, J.A.; Valli, P.V.; Kröger, A.; Bergamin, I.; Künzler, P.; Baserga, A.; Braun, D.; Seifert, B.; Moncsek, A.; Fehr, J.; et al. Direct antiviral agent treatment of chronic hepatitis C results in rapid regression of transient elastography and fibrosis markers fibrosis-4 score and aspartate aminotransferase-platelet ratio index. Liver Int. 2017, 37, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.P.Y.; Levy, M.T.; Shackel, N.; Davison, A.S.; Prakoso, E. Hepatocellular carcinoma incidence post direct-acting antivirals in hepatitis C-related advanced fibrosis/cirrhosis patients in Australia. Hepatobiliary Pancreat. Dis. Int. 2020, 19, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Makhlouf, A.N.; Abdelmalek, O.M.; Ibrahim, M.E.; Abu-Faddan, N.H.; Kheila, E.A.; Mahmoud, A.A. Ledipasvir/Sofosbuvir in Adolescents With Chronic Hepatitis C Genotype 4 With and Without Hematological Disorders: Virological Efficacy and Impact on Liver Stiffness. J. Pediatr. Infect. Dis. Soc. 2021, 10, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Lledó, G.M.; Carrasco, I.; Benítez-Gutiérrez, L.M.; Arias, A.; Royuela, A.; Requena, S.; Cuervas-Mons, V.; De Mendoza, C. Regression of liver fibrosis after curing chronic hepatitis C with oral antivirals in patients with and without HIV coinfection. AIDS 2018, 32, 2347–2352. [Google Scholar] [CrossRef] [PubMed]
- Pokorska-Śpiewak, M.; Śpiewak, M. Management of hepatitis C in children and adolescents during COVID-19 pandemic. World J. Hepatol. 2020, 12, 485–492. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Feature | Patients with Significant Fibrosis (F ≥ 2 on METAVIR Scale) n = 4 | Patients without Fibrosis (F0/F1 on METAVIR Scale) n = 4 | |
|---|---|---|---|
| Sex | Male | 3 | 2 |
| Female | 1 | 2 | |
| Age at start of the treatment (years) | 12; 16; 17; 15 | 12; 15; 15; 17 | |
| HCV genotype | 1 | 3 | 3 |
| 4 | 1 | 1 | |
| Mode of HCV infection | Vertical | 4 | 3 |
| Unknown | 0 | 1 | |
| Previous ineffective anti-HCV treatment (interferon plus ribavirin) | 3 | 2 | |
| Duration of LDV/SOF treatment | 12 weeks | 2 | 4 |
| 24 weeks | 2 | 0 | |
| BMI (kg/m2)/BMI z-score at start of LDV/SOF | 25.4/2.07; 25.7/1.55; 37.0/3.28; 20.4/0.23 | 18.0/0.01; 20.9/0.23; 18.4/−0.64; 23.5/0.77 | |
| ALT (IU/mL) at start of LDV/SOF | 40; 52; 438; 46 | 32; 41; 18; 67 | |
| HCV/HIV coinfection | 1 | 1 | |
| HCV viral load (IU/mL) at start of LDV/SOF | 2.23 × 106; 4.89 × 105; 7.0 ×104; 6.28 × 105 | 4.49 × 105; 1.37 × 104; 7.06 × 105; 2.24 × 106 | |
| Undetectable HCV viral load ≥ 12 weeks posttreatment (SVR) | 3 (one patient lost to follow-up after week 4) | 4 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pokorska-Śpiewak, M.; Dobrzeniecka, A.; Marczyńska, M. One-Year Outcomes after Ledipasvir/Sofosbuvir Treatment of Chronic Hepatitis C in Teenagers with and without Significant Liver Fibrosis—A Case Series Report. Viruses 2021, 13, 1518. https://0-doi-org.brum.beds.ac.uk/10.3390/v13081518
Pokorska-Śpiewak M, Dobrzeniecka A, Marczyńska M. One-Year Outcomes after Ledipasvir/Sofosbuvir Treatment of Chronic Hepatitis C in Teenagers with and without Significant Liver Fibrosis—A Case Series Report. Viruses. 2021; 13(8):1518. https://0-doi-org.brum.beds.ac.uk/10.3390/v13081518
Chicago/Turabian StylePokorska-Śpiewak, Maria, Anna Dobrzeniecka, and Magdalena Marczyńska. 2021. "One-Year Outcomes after Ledipasvir/Sofosbuvir Treatment of Chronic Hepatitis C in Teenagers with and without Significant Liver Fibrosis—A Case Series Report" Viruses 13, no. 8: 1518. https://0-doi-org.brum.beds.ac.uk/10.3390/v13081518