
Congenital Zika Infection and the Risk of Neurodevelopmental, Neurological, and Urinary Track Disorders in Early Childhood. A Systematic Review

 ,
,  ,
, 
 ,
, 
Abstract
:1. Introduction
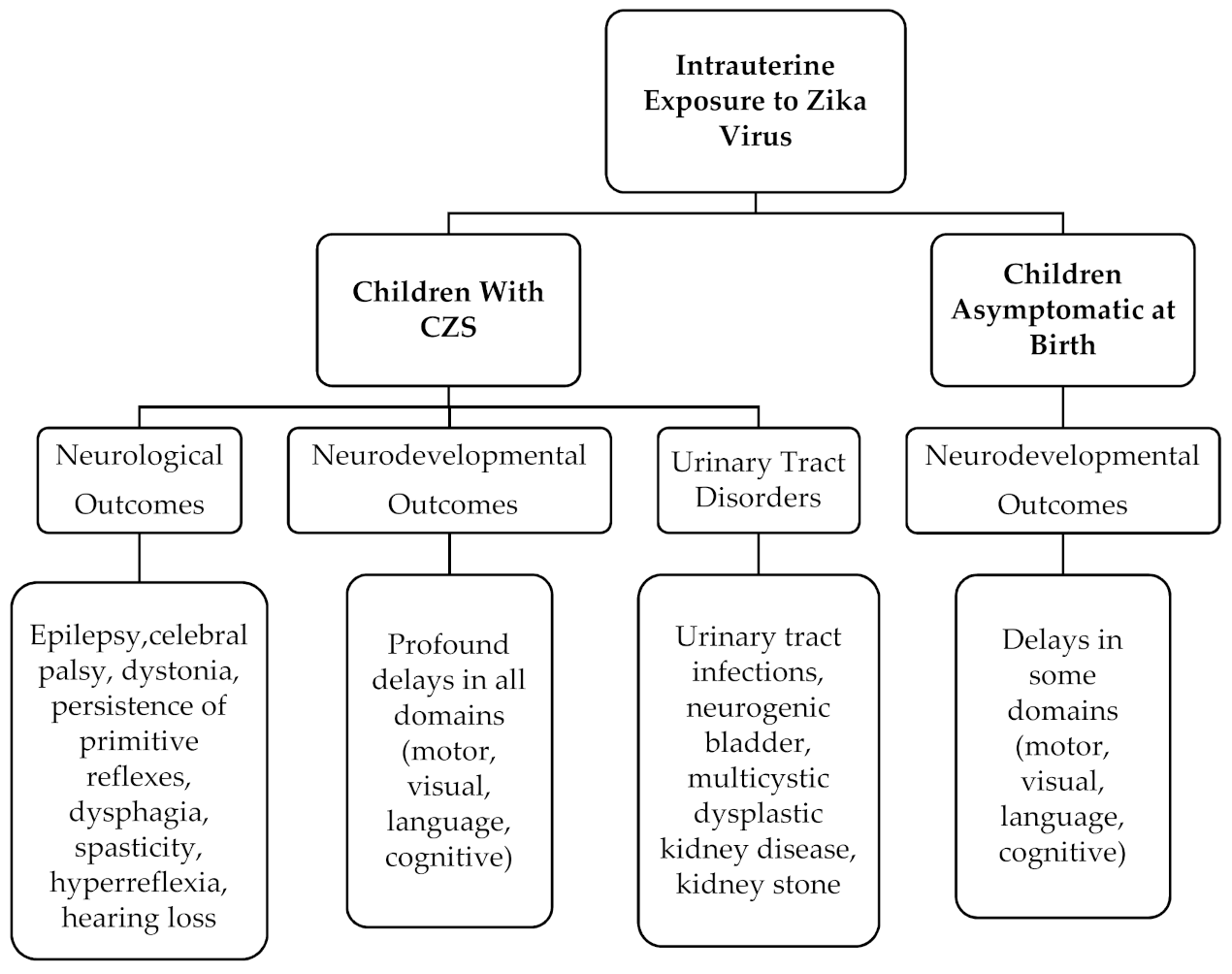
1.1. Congenital Zika Syndrome and Neurodevelopmental Outcomes
1.2. Congenital Zika Syndrome and Urinary Track Outcomes
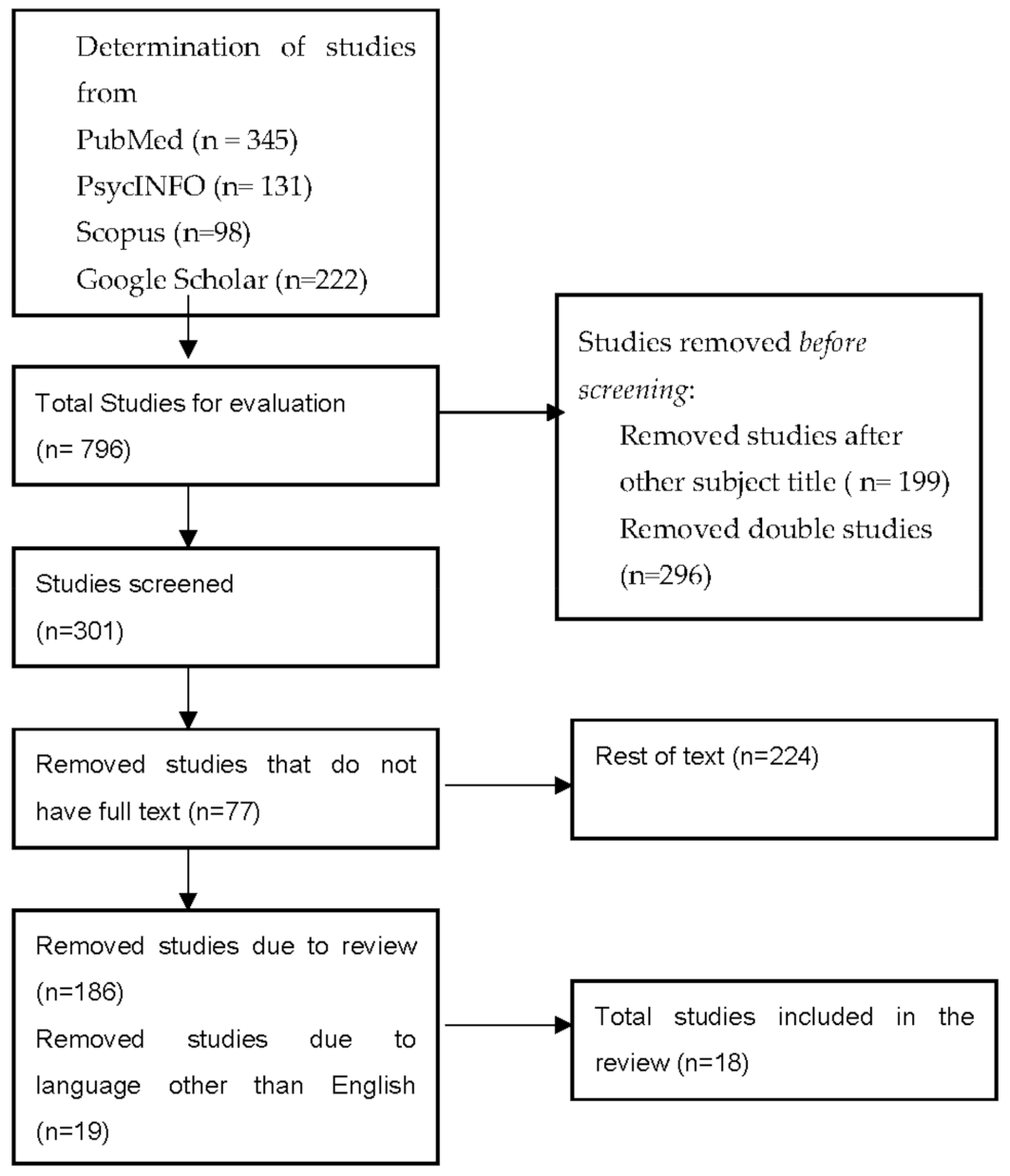
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agumadu, V.C.; Ramphul, K. Zika Virus: A Review of Literature. Cureus 2018, 10, e3025. [Google Scholar] [CrossRef] [Green Version]
- WHO. Director-General Summarizes the Outcome of the Emergency Committee Regarding Clusters of Microcephaly and Guillain-Barré Syndrome. Available online: https://www.who.int/news/item/01-02-2016-who-director-general-summarizes-the-outcome-of-the-emergency-committee-regarding-clusters-of-microcephaly-and-guillain-barré-syndrome (accessed on 25 October 2020).
- Yan, M.; Luan, R. Research Progress of the Causal Link between Zika Virus and Microcephaly. Glob. Health J. 2018, 2, 11–18. [Google Scholar] [CrossRef]
- Santa Rita, T.H.; Barra, R.B.; Peixoto, G.P.; Mesquita, P.G.; Barra, G.B. Association between Suspected Zika Virus Disease during Pregnancy and Giving Birth to a Newborn with Congenital Microcephaly: A Matched Case–Control Study. BMC Res. Notes 2017, 10, 457. [Google Scholar] [CrossRef]
- de Araújo, T.V.B.; Rodrigues, L.C.; de Alencar Ximenes, R.A.; de Barros Miranda-Filho, D.; Montarroyos, U.R.; de Melo, A.P.L.; Valongueiro, S.; de Albuquerque, M.d.F.P.M.; Souza, W.V.; Braga, C.; et al. Association between Zika Virus Infection and Microcephaly in Brazil, January to May, 2016: Preliminary Report of a Case-Control Study. Lancet Infect. Dis. 2016, 16, 1356–1363. [Google Scholar] [CrossRef] [Green Version]
- Melo, A.S.O.; Malinger, G.; Ximenes, R.; Szejnfeld, P.O.; Sampaio, S.A.; de Filippis, A.M.B. Zika Virus Intrauterine Infection Causes Fetal Brain Abnormality and Microcephaly: Tip of the Iceberg? Ultrasound Obstet. Gynecol. 2016, 47, 6–7. [Google Scholar] [CrossRef] [PubMed]
- Sarno, M.; Aquino, M.; Pimentel, K.; Cabral, R.; Costa, G.; Bastos, F.; Brites, C. Progressive Lesions of Central Nervous System in Microcephalic Fetuses with Suspected Congenital Zika Virus Syndrome. Ultrasound Obstet. Gynecol. 2017, 50, 717–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Driggers, R.W.; Ho, C.-Y.; Korhonen, E.M.; Kuivanen, S.; Jääskeläinen, A.J.; Smura, T.; Rosenberg, A.; Hill, D.A.; DeBiasi, R.L.; Vezina, G.; et al. Zika Virus Infection with Prolonged Maternal Viremia and Fetal Brain Abnormalities. N. Engl. J. Med. 2016, 374, 2142–2151. [Google Scholar] [CrossRef] [PubMed]
- Calvet, G.; Aguiar, R.S.; Melo, A.S.O.; Sampaio, S.A.; de Filippis, I.; Fabri, A.; Araujo, E.S.M.; de Sequeira, P.C.; de Mendonça, M.C.L.; de Oliveira, L.; et al. Detection and Sequencing of Zika Virus from Amniotic Fluid of Fetuses with Microcephaly in Brazil: A Case Study. Lancet Infect. Dis. 2016, 16, 653–660. [Google Scholar] [CrossRef] [Green Version]
- Hoen, B.; Schaub, B.; Funk, A.L.; Ardillon, V.; Boullard, M.; Cabié, A.; Callier, C.; Carles, G.; Cassadou, S.; Césaire, R.; et al. Pregnancy Outcomes after ZIKV Infection in French Territories in the Americas. N. Engl. J. Med. 2018, 378, 985–994. [Google Scholar] [CrossRef]
- Rice, M.E.; Galang, R.R.; Roth, N.M.; Ellington, S.R.; Moore, C.A.; Valencia-Prado, M.; Ellis, E.M.; Tufa, A.J.; Taulung, L.A.; Alfred, J.M.; et al. Vital Signs: Zika-Associated Birth Defects and Neurodevelopmental Abnormalities Possibly Associated with Congenital Zika Virus Infection—U.S. Territories and Freely Associated States, 2018. Morb. Mortal. Wkly. Rep. 2018, 67, 858–867. [Google Scholar] [CrossRef] [Green Version]
- Antoniou, E.; Orovou, E.; Sarella, A.; Iliadou, M.; Rigas, N.; Palaska, E.; Iatrakis, G.; Dagla, M. Zika Virus and the Risk of Developing Microcephaly in Infants: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3806. [Google Scholar] [CrossRef]
- Vargas, J.E.; Allred, E.N.; Leviton, A.; Holmes, L.B. Congenital Microcephaly: Phenotypic Features in a Consecutive Sample of Newborn Infants. J. Pediatr. 2001, 139, 210–214. [Google Scholar] [CrossRef] [PubMed]
- CDC. Facts About Microcephaly|Birth Defects|NCBDDD|CDC. Available online: https://www.cdc.gov/ncbddd/birthdefects/microcephaly.html (accessed on 31 March 2020).
- CDC. Congenital Zika Syndrome & Other Birth Defects|CDC. Available online: https://www.cdc.gov/pregnancy/zika/testing-follow-up/zika-syndrome-birth-defects.html (accessed on 29 October 2020).
- WHO. Defining the Syndrome Associated with Congenital Zika Virus Infection. Available online: http://www.who.int/bulletin/volumes/94/6/16-176990/en/ (accessed on 29 October 2020). [CrossRef]
- Lemos de Carvalho, A.; Brites, C.; Taguchi, T.B.; Pinho, S.F.; Campos, G.; Lucena, R. Congenital Zika Virus Infection with Normal Neurodevelopmental Outcome, Brazil. Emerg. Infect. Dis. 2018, 24, 2128–2130. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, V. Description of 13 Infants Born During October 2015–January 2016 With Congenital Zika Virus Infection Without Microcephaly at Birth—Brazil. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.; Brites, C.; Mochida, G.; Ventura, P.; Fernandes, A.; Lage, M.L.; Taguchi, T.; Brandi, I.; Silva, A.; Franceschi, G.; et al. Clinical and Neurodevelopmental Features in Children with Cerebral Palsy and Probable Congenital Zika. Brain Dev. 2019, 41, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Peçanha, P.M.; Gomes, S.C., Jr.; Pone, S.M.; Pone, M.V.d.S.; Vasconcelos, Z.; Zin, A.; Vilibor, R.H.H.; Costa, R.P.; Meio, M.D.B.B.; Nielsen-Saines, K.; et al. Neurodevelopment of Children Exposed Intra-Uterus by Zika Virus: A Case Series. PLoS ONE 2020, 15. [Google Scholar] [CrossRef] [Green Version]
- Glazier, D.B.; Cummings, K.B.; Barone, J.G. Urodynamic Evaluation of Profound Microcephaly in Children. Br. J. Urol. 1997, 80, 825–826. [Google Scholar] [CrossRef] [Green Version]
- Costa Monteiro, L.M.; Cruz, G.N.d.O.; Fontes, J.M.; Saad Salles, T.R.D.; Boechat, M.C.B.; Monteiro, A.C.; Moreira, M.E.L. Neurogenic Bladder Findings in Patients with Congenital Zika Syndrome: A Novel Condition. PLoS ONE 2018, 13. [Google Scholar] [CrossRef]
- Monteiro, L.M.C.; Cruz, G.N.d.O.; Fontes, J.M.; de Araujo, G.F.; Ventura, T.; Monteiro, A.C.; Moreira, M.E.L. Neurogenic Bladder in the Settings of Congenital Zika Syndrome: A Confirmed and Unknown Condition for Urologists. J. Pediatr. Urol. 2019, 15, 450.e1–450.e7. [Google Scholar] [CrossRef]
- de Medeiros Francilaide Campos, Â.; Azevedo de Souza, L.; Mattos, A.; Oliveira Filho, J.; Barroso, U. Urological Profile of Children with Microcephaly and Congenital Zika Syndrome. J. Pediatr. Urol. 2021, 17, 255.e1–255.e5. [Google Scholar] [CrossRef]
- Wheeler, A.C.; Toth, D.; Ridenour, T.; Lima Nóbrega, L.; Borba Firmino, R.; Marques da Silva, C.; Carvalho, P.; Marques, D.; Okoniewski, K.; Ventura, L.O.; et al. Developmental Outcomes Among Young Children with Congenital Zika Syndrome in Brazil. JAMA Netw. Open 2020, 3. [Google Scholar] [CrossRef] [PubMed]
- Pereira, H.V.F.S.; dos Santos, S.P.; Amâncio, A.P.R.L.; de Oliveira-Szejnfeld, P.S.; Flor, E.O.; Tavares, J.d.S.; Ferreira, R.V.B.; Tovar-Moll, F.; de Amorim, M.M.R.; Melo, A. Neurological Outcomes of Congenital Zika Syndrome in Toddlers and Preschoolers: A Case Series. Lancet Child Adolesc. Health 2020, 4, 378–387. [Google Scholar] [CrossRef]
- Mulkey, S.B.; Arroyave-Wessel, M.; Peyton, C.; Bulas, D.I.; Fourzali, Y.; Jiang, J.; Russo, S.; McCarter, R.; Msall, M.E.; du Plessis, A.J.; et al. Neurodevelopmental Abnormalities in Children with In Utero Zika Virus Exposure without Congenital Zika Syndrome. JAMA Pediatr. 2020, 174, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, H.N.C.; Schiariti, V.; Regalado, I.C.R.; Sousa, K.G.; Pereira, S.A.; Fechine, C.P.N.D.S.; Longo, E. Functioning and Disability Profile of Children with Microcephaly Associated with Congenital Zika Virus Infection. Int. J. Environ. Res. Public Health 2018, 15, 1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Carvalho, A.L.; Ventura, P.; Taguchi, T.; Brandi, I.; Brites, C.; Lucena, R. Cerebral Palsy in Children with Congenital Zika Syndrome: A 2-Year Neurodevelopmental Follow-Up. J. Child Neurol. 2020, 35, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Bertolli, J.; Attell, J.E.; Rose, C.; Moore, C.A.; Melo, F.; Staples, J.E.; Kotzky, K.; Krishna, N.; Satterfield-Nash, A.; Pereira, I.O.; et al. Functional Outcomes among a Cohort of Children in Northeastern Brazil Meeting Criteria for Follow-Up of Congenital Zika Virus Infection. Am. J. Trop. Med. Hyg. 2020, 102, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Sobral da Silva, P.F.; Eickmann, S.H.; Arraes de Alencar Ximenes, R.; Ramos Montarroyos, U.; de Carvalho Lima, M.; Turchi Martelli, C.M.; Velho Barreto de Araújo, T.; Brickley, E.B.; Cunha Rodrigues, L.; Lima da Silva Pastich Gonçalves, F.C.; et al. Pediatric Neurodevelopment by Prenatal Zika Virus Exposure: A Cross-Sectional Study of the Microcephaly Epidemic Research Group Cohort. BMC Pediatr. 2020, 20, 472. [Google Scholar] [CrossRef] [PubMed]
- Cranston, J.S.; Tiene, S.F.; Nielsen-Saines, K.; Vasconcelos, Z.; Pone, M.V.; Pone, S.; Zin, A.; Salles, T.S.; Pereira, J.P.; Orofino, D.; et al. Association Between Antenatal Exposure to Zika Virus and Anatomical and Neurodevelopmental Abnormalities in Children. JAMA Netw. Open 2020, 3. [Google Scholar] [CrossRef] [PubMed]
- García-Boyano, M.; García-Segovia, R.; Fernández-Menéndez, A.; Pérez, Y.; Bustamante-Amador, J.; Layana-Coronel, M.; Caballero-Caballero, J.M.; Rodríguez-Izquierdo, C.; Chávez-Solórzano, N.; Solís-Montiel, D.; et al. Long-Term Outcomes of Infants with Congenital Zika Virus Infection in Ecuador: A Retrospective Longitudinal Study. J. Trop. Pediatr. 2020, fmaa066. [Google Scholar] [CrossRef] [PubMed]
- Quilião, M.E.; Venancio, F.A.; Mareto, L.K.; Metzker, S.d.A.; do Nascimento, A.I.; Vitorelli-Venancio, D.C.; Santos-Pinto, C.D.B.; de Oliveira, E.F. Neurological Development, Epilepsy, and the Pharmacotherapy Approach in Children with Congenital Zika Syndrome: Results from a Two-Year Follow-up Study. Viruses 2020, 12, 1083. [Google Scholar] [CrossRef] [PubMed]
- Ticona, J.P.A.; Nery, N., Jr.; Ladines-Lim, J.B.; Gambrah, C.; Sacramento, G.; Freitas, B.d.P.; Bouzon, J.; Oliveira-Filho, J.; Borja, A.; Adhikarla, H.; et al. Developmental Outcomes in Children Exposed to Zika Virus in Utero from a Brazilian Urban Slum Cohort Study. PLoS Negl. Trop. Dis. 2021, 15, e0009162. [Google Scholar] [CrossRef]
- Hcini, N.; Kugbe, Y.; Rafalimanana, Z.H.L.; Lambert, V.; Mathieu, M.; Carles, G.; Baud, D.; Panchaud, A.; Pomar, L. Association between Confirmed Congenital Zika Infection at Birth and Outcomes up to 3 Years of Life. Nat. Commun. 2021, 12, 3270. [Google Scholar] [CrossRef] [PubMed]
- Abtibol-Bernardino, M.R.; de Almeida Peixoto, L.d.F.A.; de Oliveira, G.A.; de Almeida, T.F.; Rodrigues, G.R.I.; Otani, R.H.; Soares Chaves, B.C.; de Souza Rodrigues, C.; de Andrade, A.B.C.A.; de Fatima Redivo, E.; et al. Neurological Findings in Children without Congenital Microcephaly Exposed to Zika Virus in Utero: A Case Series Study. Viruses 2020, 12, 1335. [Google Scholar] [CrossRef] [PubMed]
- Cruz, G.N.; Monteiro, A.C.; Gomes, S.C., Jr.; Fontes, J.M.; Saad, T.; Costa Monteiro, L.M. Virus-Related Neurological Lower Urinary Tract Dysfunction: Lessons Learned during 4-Year Follow-up of Patients with Congenital Zika Syndrome. J. Pediatr. Urol. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Villamil-Gómez, W.E.; Padilla-Ruiz, D.; Mendoza, A.; Álvarez, Á.; Baldrich-Gomez, O.; Posso, H.; Campo-Urbina, M.; Parra-Saad, E.A.; Rodríguez-Morales, A.J. Urinary Bladder Agenesis and Renal Hypoplasia Potentially Related to in Utero Zika Virus Infection. Int. J. Infect. Dis. 2019, 85, 54–56. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Tang, L.; Tang, H.; Pu, J.; Gong, S.; Fang, D.; Zhang, H.; Li, Y.-P.; Zhu, X.; Wang, W.; et al. Zika Virus Infection Induces Acute Kidney Injury Through Activating NLRP3 Inflammasome Via Suppressing Bcl-2. Front. Immunol. 2019, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zika Cumulative Cases—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/tag/zika-cumulative-cases (accessed on 22 June 2021).
- de Carvalho-Sauer, R.d.C.O.; Costa, M.d.C.N.; Paixão, E.S.; de Jesus Silva, N.; Barreto, F.R.; Teixeira, M.G. Cross-Sectional Study of the Anthropometric Characteristics of Children with Congenital Zika Syndrome up to 12 Months of Life. BMC Pediatr. 2020, 20, 479. [Google Scholar] [CrossRef]
- Ashwal, S.; Michelson, D.; Plawner, L.; Dobyns, W.B. Practice Parameter: Evaluation of the Child with Microcephaly (an Evidence-Based Review). Neurology 2009, 73, 887–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Almeida, V.A.; Gonçalves, R.P.; Morya, E.; Simas, L.E.C.; Arrais, N.M.R.; Lisboa, L.L.; Monteiro, L.M.C.; de Oliveira Freitas, R.A., Jr. Evaluation of Bladder and Bowel Functions in Children with Microcephaly and Congenital Zika Syndrome. J. Pediatr. Urol. 2021. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author/Year | Selection 1 2 3 4 | Comparability 5 6 | Result 7 8 9 | Total |
|---|---|---|---|---|
| 1.Wheather (2020) [25] | * - * * | * * | * * * | 8 |
| 2. Pereira (2020) [26] | * - * * | * * | * * * | 8 |
| 3. Pecanha (2020) [20] | * - * * | * * | * * * | 8 |
| 4. Mulkey (2020) [27] | * - * * | - * | * * * | 7 |
| 5. Ferreira (2018) [28] | * - * * | * * | * * * | 8 |
| 6. Carvalho (2019) [29] | * - * * | - * | * * * | 7 |
| 7. Bertolli (2020) [30] | * - * * | * * | * * * | 8 |
| 8. Silva (2020) [31] | * - * * | - * | * * * | 7 |
| 9. Cranston (2020) [32] | * - * * | - * | * * * | 7 |
| 10. Garcia-Boyano (2020) [33] | * - * * | * * | * * * | 8 |
| 11. Quilião (2020) [34] | * - * * | - * | * * * | 7 |
| 12. Ticona (2021) [35] | * - * * | * * | * * * | 8 |
| 13. Hcini (2021) [36] | * - * * | - * | * * * | 8 |
| 14. Abtibol-Bernardino (2020) [37] | * - * * | * * | * * * | 8 |
| 15. Costa Monteiro (2018) [22] | * - * * | - * | * * * | 7 |
| 16. Costa Monteiro (2019) [23] | * - * * | - * | * * * | 7 |
| 17. de Medeiros (2021) [24] | * - * * | * * | * * * | 8 |
| 18. Villamil-Gómez (2019) [38] | - - * - | - * | * * * | 5 |
| 19. Liu (2019) [39] | - - ** | - * | * * * | 6 |
| Author/ Year | Design | Start– Expiry | N | Population Characteristics | Data/ Country | Outcome |
|---|---|---|---|---|---|---|
| 1.Wheather (2020) [25] | longitudinal study | January 2018–Still on going | 121 | 2.5–3 years old CZS | Rehabilitation center Brazil | Profound delays in all neurodevelopmental domains |
| 2. Pereira (2020) [26] | Cohort study | November 2015–2017 | 75 | 26–40 months of age Exposed to Zika virus | Instituto de Pesquisa Brazil | Neurological outcomes Urinary tract disorders |
| 3. Pecanha (2020) [20] | Cohort study | May 2016 and January 2018 | 84 | 2 years old Asymptomatic at birth | Instituto Fernandes Figueira Brazil | Neurodevelopmental outcomes |
| 4. Mulkey (2020) [27] | Cohort study | 1August, 2016– 30 November 2017 | 70 | 18 months of age Asymptomatic at birth | National Medical Center Columbia | Neurodevelopmental outcomes |
| 5. Ferreira (2018) [28] | Cross- sectional study | September 2017– January 2018 | 34 | 21 months average age CZS | Four rehabilitation facilities Brazil | Neurodevelopmental outcomes |
| 6. Carvalho (2019) [29] | Cohort study | July 2015– 2017 | 69 | 23–32 months of age CZS | Neurorehabilitation Hospital Brazil | Neurological outcomes Neurodevelopmental outcomes |
| 7. Bertolli (2020) [30] | Cohort study | July 2017– October 2017 | 120 | 19–26 months of age Exposed to Zika virus | The Brazilian Ministry of Health The CDC | Neurological outcomes Neurodevelopmental outcomes |
| 8. Silva (2020) [31] | Cross- sectional study | February 2017– August 2019 | 219 | 10–45 months of age Exposed to Zika virus | Two Tertiary Hospitals Brazil | Neurological outcomes Neurodevelopmental outcomes |
| 9. Cranston (2020) [32] | Retrospective cohort study | May 2019– July 2019 | 219 | 6–42 months of age Exposed to Zika virus | Instituto Fernandes Figueira Brazil | Neurological outcomes Neurodevelopmental outcomes |
| 10. Garcia-Boyano (2020) [33] | Cohort study | March 2016– September 2019 | 21 | 23.6 months of age Exposed to Zika virus | Pediatric Hospital Ecuador | Neurological outcomes Neurodevelopmental outcomes |
| 11. Quilião (2020) [34] | Cohort study | October 2018– February 2020 | 11 | 36 months median age CZS | University of Mato Grosso do Sul Brazil | Neurological outcomes Neurodevelopmental outcomes |
| 12. Ticona (2021) [35] | Cohort study | January 2015– December 2016 | 46 | 11–32 months of age Exposed to Zika virus | Hospital Brazil | Neurodevelopmental outcomes |
| 13. Hcini (2021) [36] | Cohort study | January 2016– September 2016 | 129 | 3 years of age Exposed to Zika virus | Pediatric clinic French Guiana | Neurodevelopmental outcomes Neurological outcomes |
| 14. Abtibol-Bernardino (2020) [37] | Cohort study | 2006–2008 | 26 | 25–42 months of age Exposed to Zika virus | Tropical Medicine Foundation Brazil | Neurodevelopmental outcomes Neurological outcomes |
| 15. Costa Monteiro (2018) [22] | Cohort study | June 2016– May 2017 | 22 | 9.8 months mean age CZS | CZS clinics Brazil | Urinary track Disorders |
| 16. Costa Monteiro (2019) [23] | Cohort study | June 2016–May 2018 | 69 | 13.6 months of age CZS | Referral center Brazil | Urinary track Disorders |
| 17. de Medeiros Francilai de Campos (2021) [24] | Cross- sectional study | January 2019– December 2019 | 33 | 35–47 months of age CZS | Center for urinary disorders Brazil | Urinary track Disorders |
| 18. Villamil-Gómez (2019) [39] | Case report | February 2017 | 1 | 16 weeks of gestation infected fetus | University Hospital Colombia | Urinary track Disorders |
| 19. Liu (2019) [40] | Clinical study | February 2016 | - | Newborn and adult mice | Sun Yat-sen University China | Urinary track Disorders |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antoniou, E.; Orovou, E.; Andronikidi, P.E.; Orovas, C.; Rigas, N.; Palaska, E.; Sarella, A.; Iatrakis, G.; Voyiatzaki, C. Congenital Zika Infection and the Risk of Neurodevelopmental, Neurological, and Urinary Track Disorders in Early Childhood. A Systematic Review. Viruses 2021, 13, 1671. https://0-doi-org.brum.beds.ac.uk/10.3390/v13081671
Antoniou E, Orovou E, Andronikidi PE, Orovas C, Rigas N, Palaska E, Sarella A, Iatrakis G, Voyiatzaki C. Congenital Zika Infection and the Risk of Neurodevelopmental, Neurological, and Urinary Track Disorders in Early Childhood. A Systematic Review. Viruses. 2021; 13(8):1671. https://0-doi-org.brum.beds.ac.uk/10.3390/v13081671
Chicago/Turabian StyleAntoniou, Evangelia, Eirini Orovou, Paraskevi Eva Andronikidi, Christos Orovas, Nikolaos Rigas, Ermioni Palaska, Angeliki Sarella, Georgios Iatrakis, and Chrysa Voyiatzaki. 2021. "Congenital Zika Infection and the Risk of Neurodevelopmental, Neurological, and Urinary Track Disorders in Early Childhood. A Systematic Review" Viruses 13, no. 8: 1671. https://0-doi-org.brum.beds.ac.uk/10.3390/v13081671