
Prevalence and Clinical Impact of Human Pegivirus-1 Infection in HIV-1-Infected Individuals in Yunnan, China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statements
2.2. Study Population and Sample Collection
2.3. RNA Extraction, HPgV-1 Gene Amplification and Sequencing
2.4. Sequence Analyses
2.5. Statistical Analysis
3. Results
3.1. Epidemiologic and Demographic Characteristics
3.2. HPgV-1 Infection Status
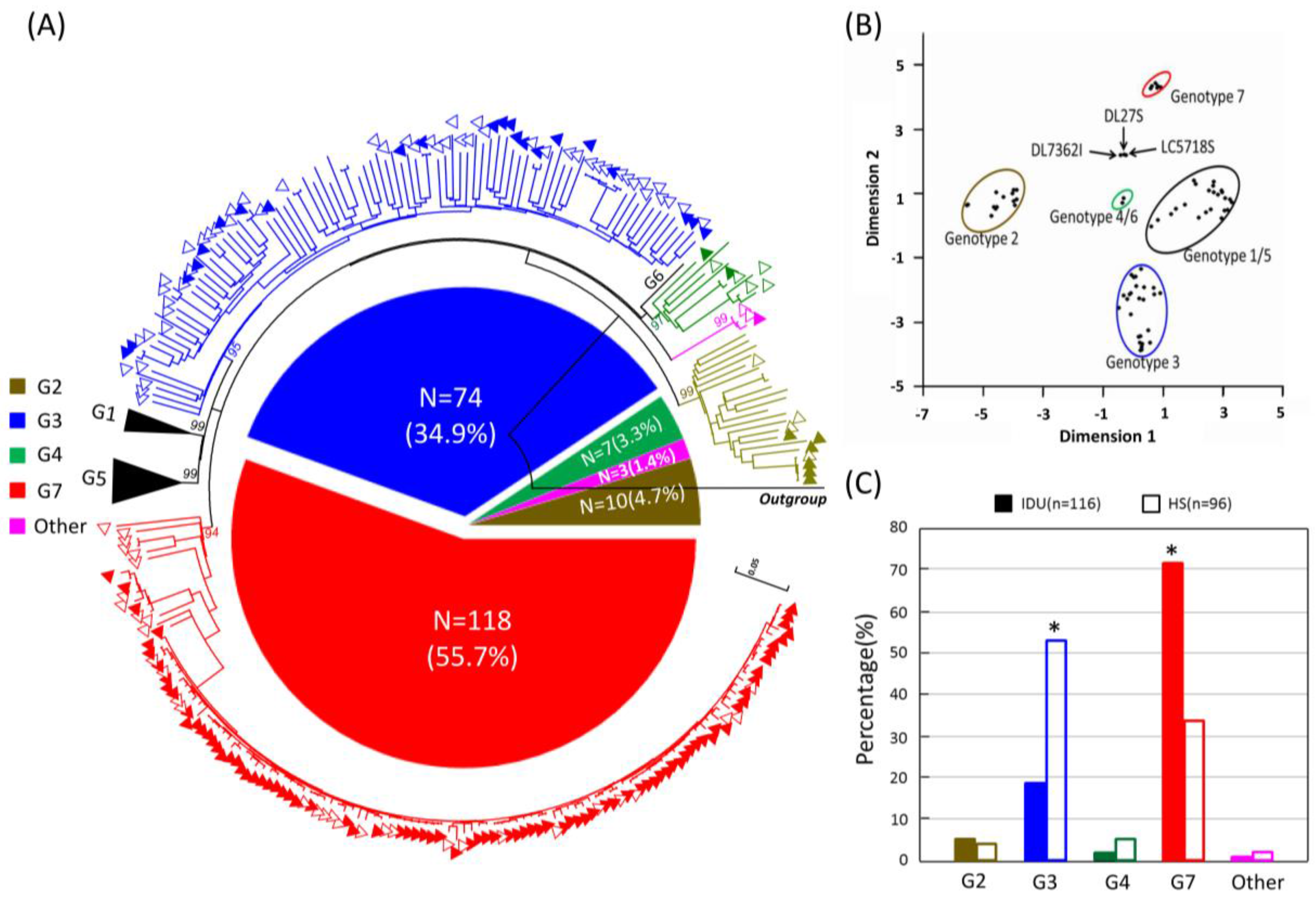
3.3. HPgV-1 Genotypes Distribution
3.4. Co-infection of HPgV-1 with HIV/HCV and Its Clinical Effect
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Berg, M.G.; Lee, D.; Coller, K.; Frankel, M.; Aronsohn, A.; Cheng, K.; Forberg, K.; Marcinkus, M.; Naccache, S.N.; Dawson, G.; et al. Discovery of a novel human pegivirus in blood associated with hepatitis C virus co-infection. PLoS Pathog. 2015, 11, e1005325. [Google Scholar] [CrossRef] [PubMed]
- Chivero, E.T.; Bhattarai, N.; Rydze, R.T.; Winters, M.A.; Holodniy, M.; Stapleton, J.T. Human pegivirus RNA is found in multiple blood mononuclear cells in vivo and serum-derived viral RNA-containing particles are infectious in vitro. J. Gen. Virol. 2014, 95, 1307–1319. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.J.; Lefkowitz, E.J.; King, A.M.; Carstens, E.B. Ratification vote on taxonomic proposals to the international committee on taxonomy of viruses (2014). Arch. Virol. 2014, 159, 2831–2841. [Google Scholar] [CrossRef] [PubMed]
- Chivero, E.T.; Stapleton, J.T. Tropism of human pegivirus (formerly known as GB virus C/hepatitis G virus) and host immunomodulation: Insights into a highly successful viral infection. J. Gen. Virol. 2015, 96, 1521–1532. [Google Scholar] [CrossRef] [PubMed]
- AbuOdeh, R.O.; Al-Absi, E.; Ali, N.H.; Khalili, M.; Al-Mawlawi, N.; Hadwan, T.A.; Althani, A.A.; Nasrallah, G.K. Detection and phylogenetic analysis of human pegivirus (GBV-C) among blood donors and patients infected with hepatitis B virus (HBV) in Qatar. J. Med. Virol. 2015, 87, 2074–2081. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Padhi, A.; Xu, J.; Gong, X.; Tien, P. Evidence for within-host genetic recombination among the human pegiviral strains in HIV infected subjects. PLoS ONE 2016, 11, e0161880. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Zhao, W.; Feng, Y.; Dai, J.; Li, Z.; Zhang, X.; Liu, L.; Bai, J.; Zhang, H.; Lu, L.; et al. A novel genotype of GB virus C: Its identification and predominance among injecting drug users in Yunnan, China. PLoS ONE 2011, 6, e21151. [Google Scholar] [CrossRef] [PubMed]
- Bhattarai, N.; Stapleton, J.T. GB virus C: The good boy virus? Trends Microbiol. 2012, 20, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Giret, M.T.; Kallas, E.G. GBV-C: State of the art and future prospects. Curr. HIV/AIDS Rep. 2012, 9, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Rendina, D.; Vigorita, E.; Bonavolta, R.; D’Onofrio, M.; Iura, A.; Pietronigro, M.T.; Laccetti, R.; Bonadies, G.; Liuzzi, G.; Borgia, G.; et al. HCV and GBV-C/HGV infection in HIV positive patients in southern Italy. Eur. J. Epidemiol. 2001, 17, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Tenckhoff, S.; Kaiser, T.; Bredeek, F.; Donfield, S.; Menius, E.; Lail, A.; Mossner, J.; Daar, E.S.; Tillmann, H.L. Role of GB virus C in HIV-1-infected and hepatitis C virus-infected hemophiliac children and adolescents. J. Acquir. Immune Defic. Syndr. 2012, 61, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Mohr, E.L.; Stapleton, J.T. GB virus type C interactions with HIV: The role of envelope glycoproteins. J. Viral Hepat. 2009, 16, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Berzsenyi, M.D.; Woollard, D.J.; McLean, C.A.; Preiss, S.; Perreau, V.M.; Beard, M.R.; Scott Bowden, D.; Cowie, B.C.; Li, S.; Mijch, A.M.; et al. Down-regulation of intra-hepatic T-cell signaling associated with GB virus C in a HCV/HIV co-infected group with reduced liver disease. J. Hepatol. 2011, 55, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Liu, L.; Feng, Y.M.; Zhao, W.; Li, Z.; Zhang, A.M.; Song, Y.; Xia, X. GB Virus C infection in patients with HIV/hepatitis C virus coinfection: Improvement of the liver function in chronic hepatitis C. Hepat. Mon. 2014, 14, e14169. [Google Scholar] [CrossRef] [PubMed]
- Berzsenyi, M.D.; Bowden, D.S.; Kelly, H.A.; Watson, K.M.; Mijch, A.M.; Hammond, R.A.; Crowe, S.M.; Roberts, S.K. Reduction in hepatitis C-related liver disease associated with GB virus C in human immunodeficiency virus coinfection. Gastroenterology 2007, 133, 1821–1830. [Google Scholar] [CrossRef] [PubMed]
- Blackard, J.T.; Ma, G.; Welge, J.A.; King, C.C.; Taylor, L.E.; Mayer, K.H.; Klein, R.S.; Celentano, D.D.; Sobel, J.D.; Jamieson, D.J.; et al. GB virus C (GBV-C) infection in hepatitis C virus (HCV) seropositive women with or at risk for HIV infection. PLoS ONE 2014, 9, e114467. [Google Scholar] [CrossRef] [PubMed]
- Berzsenyi, M.D.; Bowden, D.S.; Roberts, S.K.; Revill, P.A. GB virus C genotype 2 predominance in a hepatitis C virus/HIV infected population associated with reduced liver disease. J. Gastroenterol. Hepatol. 2009, 24, 1407–1410. [Google Scholar] [CrossRef] [PubMed]
- Muerhoff, A.S.; Tillmann, H.L.; Manns, M.P.; Dawson, G.J.; Desai, S.M. GB virus C genotype determination in GB virus-C/HIV co-infected individuals. J. Med. Virol. 2003, 70, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Alcalde, R.; Nishiya, A.; Casseb, J.; Inocencio, L.; Fonseca, L.A.; Duarte, A.J. Prevalence and distribution of the GBV-C/HGV among HIV-1-infected patients under anti-retroviral therapy. Virus Res. 2010, 151, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Wang, M.; Xia, W.J.; Tian, L.W.; Xu, R.; Li, C.H.; Wang, J.X.; Rong, X.; Xiong, H.P.; Huang, K.; et al. Migration patterns of hepatitis C virus in China characterized for five major subtypes based on samples from 411 volunteer blood donors from 17 provinces and municipalities. J. Virol. 2014, 88, 7120–7129. [Google Scholar] [CrossRef] [PubMed]
- China outline map. Available online: http://www.zonu.com/fullsize-en/2011-07-28-14186/China-outline-map.html (accessed on 12 October 2016).
- Tamura, K.; Stecher, G.; Peterson, D.; Filipski, A.; Kumar, S. MEGA6: Molecular Evolutionary Genetics Analysis version 6.0. Mol Biol Evol. 2013, 30, 2725–2729. [Google Scholar] [CrossRef] [PubMed]
- Sievers, F.; Wilm, A.; Dineen, D. Fast, scalable generation of high-quality protein multiple sequence alignments using Clustal Omega. Mol. Syst. 2011, 7, 539. [Google Scholar] [CrossRef] [PubMed]
- Standard Nucleotide BLAST. Available online: https://blast.ncbi.nlm.nih.gov/Blast.cgi?PROGRAM=blastn&PAGE_TYPE=BlastSearch&LINK_LOC=blasthome (accessed on 12 October 2016).
- BioEdit v7.2.5. Available online: http://www.mbio.ncsu.edu/BioEdit/page2.html (accessed on 12 October 2016).
- The reference sequences of GBV-C E2 gene. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/nuccore/?term=GB+Virus+C+E2 (accessed on 12 October 2016).
- Vickerman, P.; Hickman, M.; May, M.; Kretzschmar, M.; Wiessing, L. Can hepatitis C virus prevalence be used as a measure of injection-related human immunodeficiency virus risk in populations of injecting drug users? An ecological analysis. Addiction 2010, 105, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Nelson, P.K.; Mathers, B.M.; Cowie, B.; Hagan, H.; Des Jarlais, D.; Horyniak, D.; Degenhardt, L. Global epidemiology of hepatitis B and hepatitis C in people who inject drugs: Results of systematic reviews. Lancet 2011, 378, 571–583. [Google Scholar] [CrossRef]
- Zhu, T.F.; Wang, C.H.; Lin, P.; He, N. High risk populations and HIV-1 infection in China. Cell Res. 2005, 15, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Schwarze-Zander, C.; Blackard, J.T.; Zheng, H.; Addo, M.M.; Lin, W.; Robbins, G.K.; Sherman, K.E.; Zdunek, D.; Hess, G.; Chung, R.T. GB virus C (GBV-C) infection in hepatitis C virus (HCV)/HIV-coinfected patients receiving HCV treatment: Importance of the GBV-C genotype. J. Infect. Dis. 2006, 194, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Da Mota, L.D.; Nishiya, A.S.; Finger-Jardim, F.; Barral, M.F.; Silva, C.M.; Nader, M.M.; Goncalves, C.V.; Da Hora, V.P.; Silveira, J.; Basso, R.P.; et al. Prevalence of human pegivirus (HPgV) infection in patients carrying HIV-1C or non-C in southern Brazil. J. Med. Virol. 2016, 88, 2106–2114. [Google Scholar] [CrossRef] [PubMed]
- Bien, C.H.; Cai, Y.; Emch, M.E.; Parish, W.; Tucker, J.D. High adult sex ratios and risky sexual behaviors: A systematic review. PLoS ONE 2013, 8, e71580. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.M.; Guo, S.J.; Sun, Y.Y. Sexual behaviours and associated risks in chinese young people: A meta-analysis. Sex. Health 2013, 10, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.T.; Takebe, Y.; Chook, J.B.; Chow, W.Z.; Chan, K.G.; Abed Al-Darraji, H.A.; Kamarulzaman, A.; Tee, K.K. Co-infections and transmission networks of HCV, HIV-1 and HPgV among people who inject drugs. Sci. Rep. 2015, 5, 15198. [Google Scholar] [PubMed]
- Liu, Z.; Li, L.; Chen, Z.; Xu, M.; Zhang, T.; Jiao, Y.; Sheng, B.; Chen, D.; Wu, H. Prevalence of GB virus type C viraemia in MSM with or without HIV-1 infection in Beijing, China. Epidemiol. Infect. 2012, 140, 2199–2209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.K.; Tang, J.W.; Chiu, L.; Loh, T.P.; Olszyna, D.; Chew, N.; Archuleta, S.; Koay, E.S. Epidemiology of GB virus type C among patients infected with HIV in Singapore. J. Med. Virol. 2014, 86, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Anggorowati, N.; Yano, Y.; Subronto, Y.W.; Utsumi, T.; Heriyanto, D.S.; Mulya, D.P.; Rinonce, H.T.; Widasari, D.I.; Lusida, M.I.; Soetjipto, Y.H.; et al. GB virus C infection in indonesian HIV-positive patients. Microbiol. Immunol. 2013, 57, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Takebe, Y.; Wei, H.; He, X.; Hsi, J.H.; Li, Z.; Xing, H.; Ruan, Y.; Yang, Y.; Li, F.; et al. Geographic origin and evolutionary history of China’s two predominant HIV-1 circulating recombinant forms, CRF07_BC, CRF08_BC. Sci. Rep. 2016, 6, 19279. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Ma, Y.; Chen, H.; Luo, H.; Dai, J.; Song, L.; Yang, C.; Mei, J.; Yang, L.; Dong, L.; et al. Multiple introduction and naturally occuring drug resistance of HCV among HIV-infected intravenous drug users in Yunnan: An origin of China’s HIV/HCV epidemics. PLoS ONE 2015, 10, e0142543. [Google Scholar] [CrossRef] [PubMed]
- Pont, J.; Neuwald, C.; Salzner, G. Antibody prevalence of parenterally transmitted viruses (HIV-1, HTLV-i, HBV, HCV) in austrian intravenous drug users. Infection 1991, 19, 427–430. [Google Scholar] [CrossRef] [PubMed]
- Xia, X.; Lu, L.; Tee, K.K.; Zhao, W.; Wu, J.; Yu, J.; Li, X.; Lin, Y.; Mukhtar, M.M.; Hagedorn, C.H.; et al. The unique HCV genotype distribution and the discovery of a novel subtype 6u among IDUs co-infected with HIV-1 in Yunnan, China. J. Med. Virol. 2008, 80, 1142–1152. [Google Scholar] [CrossRef] [PubMed]
- Reilly, K.H.; Wang, J.J.; Zhu, Z.B.; Li, S.H.; Yang, T.H.; Ding, G.W.; Qian, H.Z.; Kissinger, P.; Wang, N. HIV and associated risk factors among male clients of female sex workers in a chinese border region. Sex. Transm. Dis. 2012, 39, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.M.; Xing, H.; Hsi, J.H.; Jia, M.H.; Feng, Y.; Duan, S.; He, C.; Yao, S.T.; Ruan, Y.H.; He, X.; et al. The sexually driven epidemic in youths in China’s southwestern border region was caused by dynamic emerging multiple recombinant HIV-1 strains. Sci. Rep. 2015, 5, 11323. [Google Scholar] [CrossRef] [PubMed]
- Jia, M.; Luo, H.; Ma, Y.; Wang, N.; Smith, K.; Mei, J.; Lu, R.; Lu, J.; Fu, L.; Zhang, Q.; et al. The HIV epidemic in Yunnan province, China, 1989–2007. J. Acquir. Immune Defic. Syndr. 2010, 53 (Suppl. 1), S34–S40. [Google Scholar] [CrossRef] [PubMed]
- Xiang, J.; McLinden, J.H.; Chang, Q.; Kaufman, T.M.; Stapleton, J.T. An 85-aa segment of the GB virus type C NS5A phosphoprotein inhibits HIV-1 replication in CD4+ Jurkat T cells. Proc. Natl. Acad. Sci. USA 2006, 103, 15570–15575. [Google Scholar] [CrossRef] [PubMed]
- Herrera, E.; Tenckhoff, S.; Gomara, M.J.; Galatola, R.; Bleda, M.J.; Gil, C.; Ercilla, G.; Gatell, J.M.; Tillmann, H.L.; Haro, I. Effect of synthetic peptides belonging to E2 envelope protein of GB virus C on human immunodeficiency virus type 1 infection. J. Med. Chem. 2010, 53, 6054–6063. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Eichenmuller, M.; Donhauser, N.; Neipel, F.; Engel, A.M.; Hess, G.; Fleckenstein, B.; Reil, H. HIV entry inhibition by the envelope 2 glycoprotein of GB virus C. Aids 2007, 21, 645–647. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Group 1: HIV-1/HCV (n = 287) | Group 2: HIV-1 (n = 775) | ||||
|---|---|---|---|---|---|---|
| HPgV-1-Infected | HPgV-1-Uninfected | p | HPgV-1-Infected | HPgV-1-Uninfected | p | |
| Patients, n (%) | 94 (32.75) | 193 (62.25) | N/A | 154 (19.87) | 621 (80.13) | N/A |
| Gender, male:female 2 | 79:15 | 150:43 | 0.273 | 86:71 | 386:240 | 0.145 |
| Mean (SD) age, y 1 | 37.99 (5.80) | 38.33 (6.05) | 0.639 | 36.90 (11.5) | 39.14 (11.34) | 0.029 |
| Mean (SD) ALT, IU/L 1 | 51.45 (37.42) | 55.48 (43.29) | 0.227 | 31.15 (26.71) | 33.03 (29.94) | 0.834 |
| Mean (SD) AST, IU/L 1 | 55.26 (36.20) | 56.22 (40.03) | 0.843 | 34.46 (23.33) | 35.06 (26.24) | 0.237 |
| Mean (SD) CD4+ count, cells/Ul 1 | 322 (193) | 280 (148) | 0.046 | 322 (184) | 288.5 (154) | 0.048 |
| Mean (SD) HIV-1 RNA log copies/mL 1 | 3.88 (0.47) | 4.02 (0.61) | 0.040 | 3.93 (0.52) | 4.04 (0.69) | 0.048 |
| HIV-1 transmission route no. (%) 2 | 0.530 | 0.278 | ||||
| Injection drug users | 78 (82.98) | 154 (79.79) | 51 (33.12) | 181 (28.91) | N/A | |
| Heterosexual | 16 (17.02) | 39 (20.21) | 103 (66.88) | 445 (71.09) | N/A | |
| Mean (SD) HCV RNA logcopies/mL 1 | 4.98 (0.21) | 5.12 (0.31) | 0.378 | N/A | N/A | N/A |
| HCV genotype no. (%) 2 | 0.563 | N/A | ||||
| 1 | 17 (18.09) | 40 (20.73) | N/A | N/A | ||
| 2 | 0 (0.00) | 2 (1.04) | N/A | N/A | ||
| 3 | 61 (64.89) | 112 (58.03) | N/A | N/A | ||
| 6 | 16 (17.02) | 39 (20.20) | N/A | N/A | ||
| Variable | HPgV-1-Uninfected | HPgV-1-Infected | ||||
|---|---|---|---|---|---|---|
| G3 | P1 | G7 | P2 | P3 | ||
| Group 1: HCV+, n (%) | 193 (62.25) | 11 (3.83) | N/A | 66 (23.00) | N/A | N/A |
| Gender, male:female 2 | 150:43 | 8:3 | 0.714 | 57:9 | 0.156 | 0.363 |
| Mean (SD) age, y1 | 38.33 (6.05) | 37.91 (7.35) | 0.822 | 38.11 (5.33) | 0.783 | 0.915 |
| Mean (SD) ALT, IU/L 1 | 55.48 (43.29) | 55.48 (43.29) | 0.703 | 50.93 (38.8) | 0.463 | 0.968 |
| Mean (SD) AST, IU/L 1 | 56.22 (40.03) | 50.62 (22.56) | 0.647 | 54.61 (36.25) | 0.781 | 0.726 |
| Mean (SD) CD4+ count, cells/uL 1 | 280 (148) | 352 (199) | 0.144 | 332 (204) | 0.037 | 0.503 |
| Mean (SD) HIV-1 RNA log10 copies/mL 1 | 4.02 (0.61) | 3.97 (0.37) | 0.827 | 3.85 (0.49) | 0.042 | 0.481 |
| HIV-1 transmission route IDUs:HS 2 | 154:39 | 10:1 | 0.696 | 56:10 | 0.467 | 0.999 |
| HCV genotype no. (%) 2 | 0.757 | 0.535 | 0.753 | |||
| 1 | 40 (20.73) | 2 (18.18) | 10 (15.15) | |||
| 2 | 2 (1.04) | 0 (0.00) | 0(0.00) | |||
| 3 | 112 (58.03) | 8 (72.73) | 44 (66.67) | |||
| 6 | 39 (20.20) | 1 (9.09) | 12 (18.18) | |||
| Group 2: HCV-, n (%) | 621 (84.37) | 63 (8.56) | N/A | 52 (7.07) | N/A | N/A |
| Gender, male:female 2 | 386:240 | 33:30 | 0.999 | 31:21 | 0.769 | 0.457 |
| Mean (SD) age, yrs 1 | 39.14 (11.34) | 34.73 (12.04) | 0.004 | 38.27 (11.60) | 0.596 | 0.113 |
| Mean (SD) ALT 1 | 33.03 (29.94) | 34.5 (4.04) | 0.248 | 33.71 (28.37) | 0.879 | 0.324 |
| Mean (SD) AST 1 | 35.06 (26.24) | 34.42 (25.90) | 0.855 | 34.57 (19.62) | 0.899 | 0.896 |
| Mean (SD) CD4+ count, cells/uL 1 | 288.5 (154) | 310 (195) | 0.366 | 341 (164) | 0.015 | 0.387 |
| Mean (SD) HIV-1 RNA log10 copies/mL 1 | 4.04 (0.69) | 3.97 (0.57) | 0.258 | 3.83 (0.64) | 0.038 | 0.349 |
| HIV-1 transmission route IDUs:HS 2 | 181:445 | 16:47 | 0.661 | 24:28 | 0.012 | 0.030 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miao, Z.; Gao, L.; Song, Y.; Yang, M.; Zhang, M.; Lou, J.; Zhao, Y.; Wang, X.; Feng, Y.; Dong, X.; et al. Prevalence and Clinical Impact of Human Pegivirus-1 Infection in HIV-1-Infected Individuals in Yunnan, China. Viruses 2017, 9, 28. https://0-doi-org.brum.beds.ac.uk/10.3390/v9020028
Miao Z, Gao L, Song Y, Yang M, Zhang M, Lou J, Zhao Y, Wang X, Feng Y, Dong X, et al. Prevalence and Clinical Impact of Human Pegivirus-1 Infection in HIV-1-Infected Individuals in Yunnan, China. Viruses. 2017; 9(2):28. https://0-doi-org.brum.beds.ac.uk/10.3390/v9020028
Chicago/Turabian StyleMiao, Zhijiang, Li Gao, Yindi Song, Ming Yang, Mi Zhang, Jincheng Lou, Yue Zhao, Xicheng Wang, Yue Feng, Xingqi Dong, and et al. 2017. "Prevalence and Clinical Impact of Human Pegivirus-1 Infection in HIV-1-Infected Individuals in Yunnan, China" Viruses 9, no. 2: 28. https://0-doi-org.brum.beds.ac.uk/10.3390/v9020028