
COVID-19 Vaccine Acceptance Rate and Its Factors among Healthcare Students: A Systematic Review with Meta-Analysis

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Assessment of Study Quality
2.5. Data Analysis
3. Results
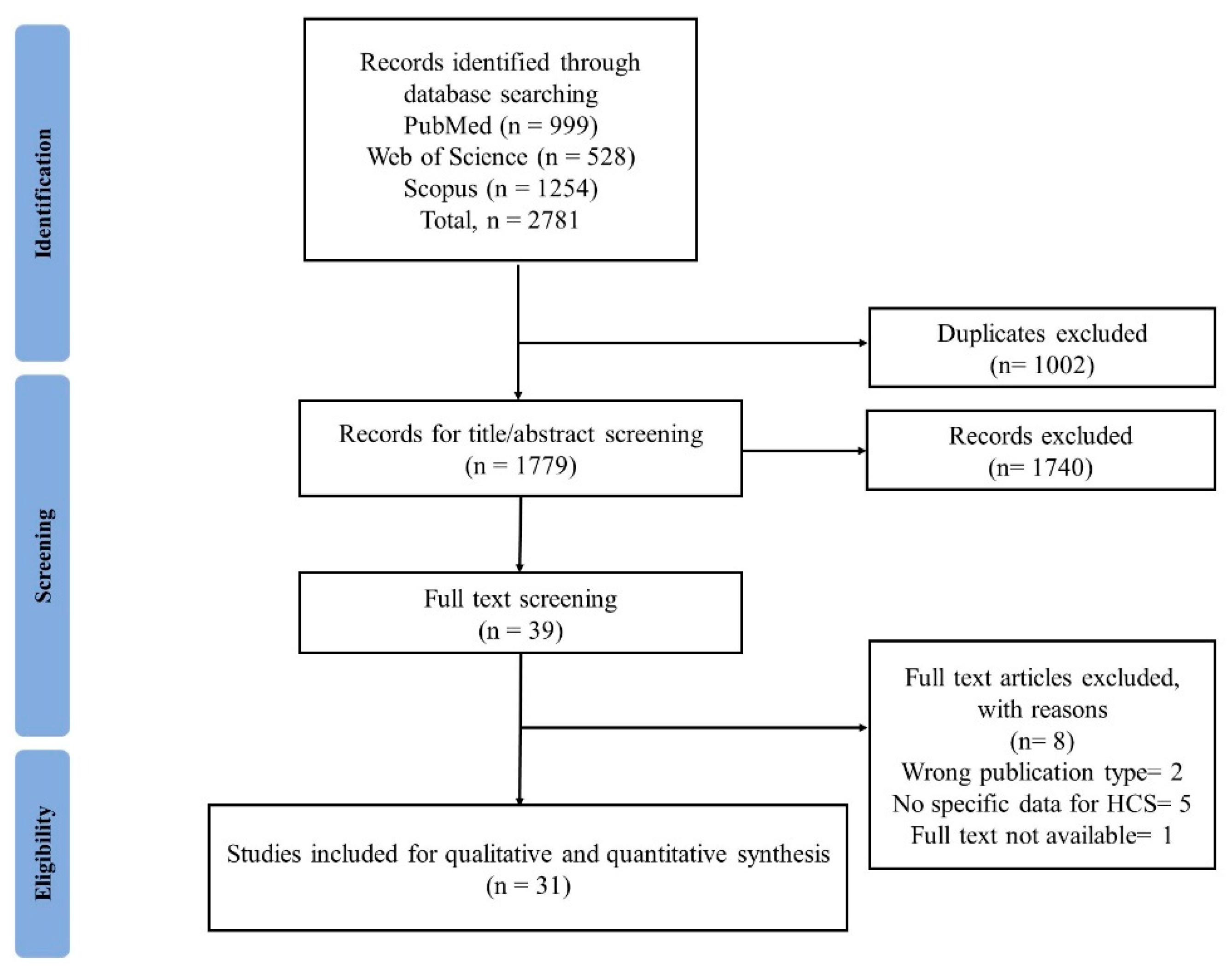
3.1. Search Results
3.2. Characteristics of Included Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SL | Author | Study Country | Type of Healthcare Students | Study Design | Survey Method | Survey Period | Sampling Method | Sample Size, N | Gender, Female (%) | Vaccine Acceptance Rate (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Al Janabi et al. [37] | USA | Osteopathic medical | Cross-sectional | Online | October 2020 | NR | 197 | 57.9 | 45 |
| 2 | Bălan et al. [38] | Romania | General Medicine, Dentistry, Pharmacy and Nursing and Midwifery | Cross-sectional | Online | 12 January until 3 March 2021 | NR | 1581 | 74.5 | 88 |
| 3 | Belingheri et al. [39] | Italy | Nursing | Cross-sectional | Online | 21–27 December 2020 | NR | 422 | 82.9 | 80.9 |
| 4 | Bolatov et al. [40] | Kazakhstan | Medical | Cross-sectional | Online | March 2021 | NR | 888 | 76.5 | 22.4 |
| 5 | De Sousa Chaves et al. [41] | Brazil | Medical | Cross-sectional | Online | 18 December 2020 to 8 January 2021 | Snowball sampling | 250 | 58.5 | 84 |
| 6 | Gao et al. [42] | China | Medical | Cross-sectional | Online | February–March 2021 | Convenience sampling | 612 | 63.2 | NR |
| 7 | Gotlib et al. [43] | Poland | Nursing undergraduate students | Cross-sectional | Online | March–April 2021 | NR | 793 | 90.8 | 38 |
| 8 | Grochowska et al. [44] | Poland | Medical | Cross-sectional | Online/Off line | 4 September–5 November 2020 | NR | 419 | n = 331 | 70.7 |
| 9 | Jain et al. [45] | India | Medical | Cross-sectional | Online | 2 February–7 March 2021 | Respondent-driven sampling strategy | 1068 | 48.6 | 89.4 |
| 10 | Jiang et al. [2] | China | Nursing | Cross-sectional | Online | February–April 2021 | Convenience | 1488 | 84.27 | 1256 |
| 11 | Kanyike et al. [4] | Uganda | Medical | Cross-sectional | Online | 15–21 March 2021 | Convenience | 600 | 37.2 | 224 |
| 12 | Katz et al. [35] | Israel | Medical | Cross-sectional | Online | December 2020 | NR | 104 | 61.5 | 91.35 |
| 13 | Kelekar et al. [17] | USA | Medical | Cross-sectional | Online | November–December 2019 | NR | 167 | NR | 126 |
| Dental | 248 | 135 | ||||||||
| 14 | L. Jain et al. [46] | India | Healthcare student | Cross-sectional | Online | November 2020–January 2021 | Snowball sampling | 655 | 61.98 | 63.82 |
| 15 | Li et al. [47] | China | Medical | Cross-sectional | Online | 15 March–30 March 2021 | NR | 2196 | 81.7 | 1291 |
| 16 | Lindner-Pawłowicz et al. [48] | Poland | Medical | Cross-sectional | Online | 8–31 December 2020 | NR | 350 | NR | 76.9 |
| 17 | Lucia et al. [18] | USA | Medical | Cross-sectional | Online | NR | NR | 167 | 57 | 126 |
| 18 | Lo Moro et al. [49] | Italy | Medical | Cross-sectional | Online | 20 November 2020–2 February 2021 | NR | 838 | 63.5 | 93.3 |
| 19 | Mahdi [50] | Iraq | Medical | Cross-sectional | Online | 2021 | NR | 810 | 60.2 | 33.83 |
| 20 | Manning et al. [21] | USA | Nursing | Cross-sectional | Online | 10 August–14 September 2020 | NR | 1029 | 87.7 | 466 |
| 21 | Mascarenhas et al. [20] | USA | Dental | Cross-sectional | Online | 2020 | NR | 248 | 58 | 136 |
| 22 | Mayan et al. [51] | USA | Medical | Cross-sectional | Online | 9 February–15 March 2021 | NR | 1899 | 64.3 | 93.31 |
| 23 | Mose et al. [52] | Ethiopia | Medical and health science | Cross-sectional | NR | 1–30 March 2021 | Simple random sampling | 420 | 41.7 | 58.8 |
| 24 | Petravic et al. [53] | Slovenia | Medical & Healthcare students | Cross-sectional | Online | December 2020 | NR | 624 | 79.49 | Medical: 82, Healthcare: 51 |
| 25 | Riad et al. [36] | 22 countries | Dental | Cross-sectional | Online | 6–28 February 2021 | NR | 6639 | 70.5 | 63.6 |
| 26 | Rosental and Shmueli [54] | Israel | Medical and nursing | Cross-sectional | Online | 27 August–28 September 2020 | NR | 628 | 66.6 | Medical: 282Nursing: 234 |
| 27 | Saied et al. [6] | Egypt | Medical | Cross-sectional | Online | 8–15 January 2021 | Convenience sampling | 2133 | NR | 34.9 |
| 28 | Szmyd et al. [55] | Poland | Medical | Cross-sectional | Online | 22–25 December 2020 | NR | 687 | 64.77 | 632 |
| 29 | Talarek et al. [56] | Poland | Medical | Cross-sectional | Online | March and April 2020 | NR | 411 | 68.4 | 94.6 |
| 30 | Zhang et al. [57] | China | Healthcare students | Cross-sectional | Online | 16–20 August 2021 | NR | 631 | 79.71 | 77.81 |
| 31 | Zhou et al. [58] | China | Nursing | Cross-sectional | Online | 4–20 January 2021 | NR | 1070 | 82.1 | 51.9 |
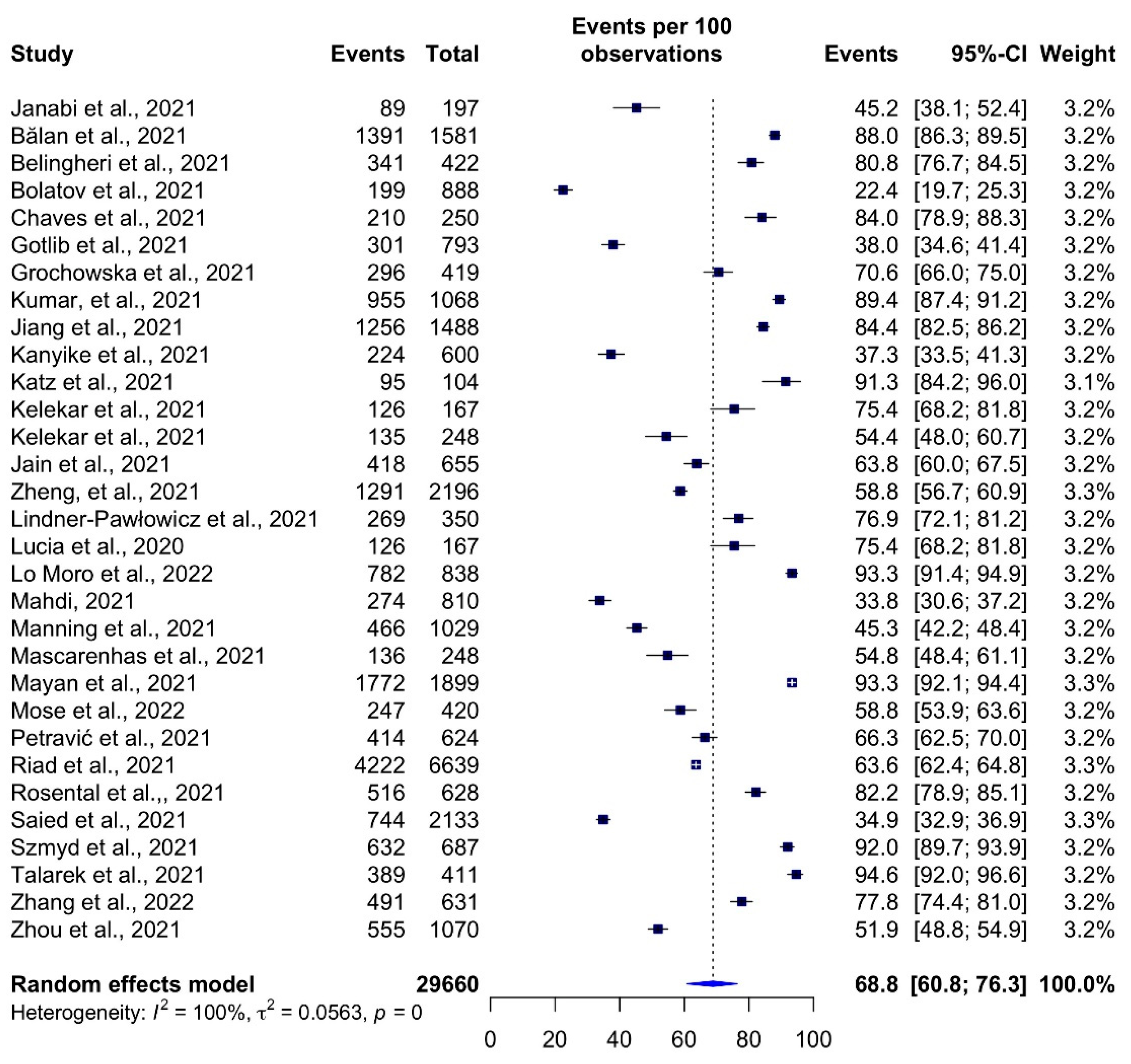
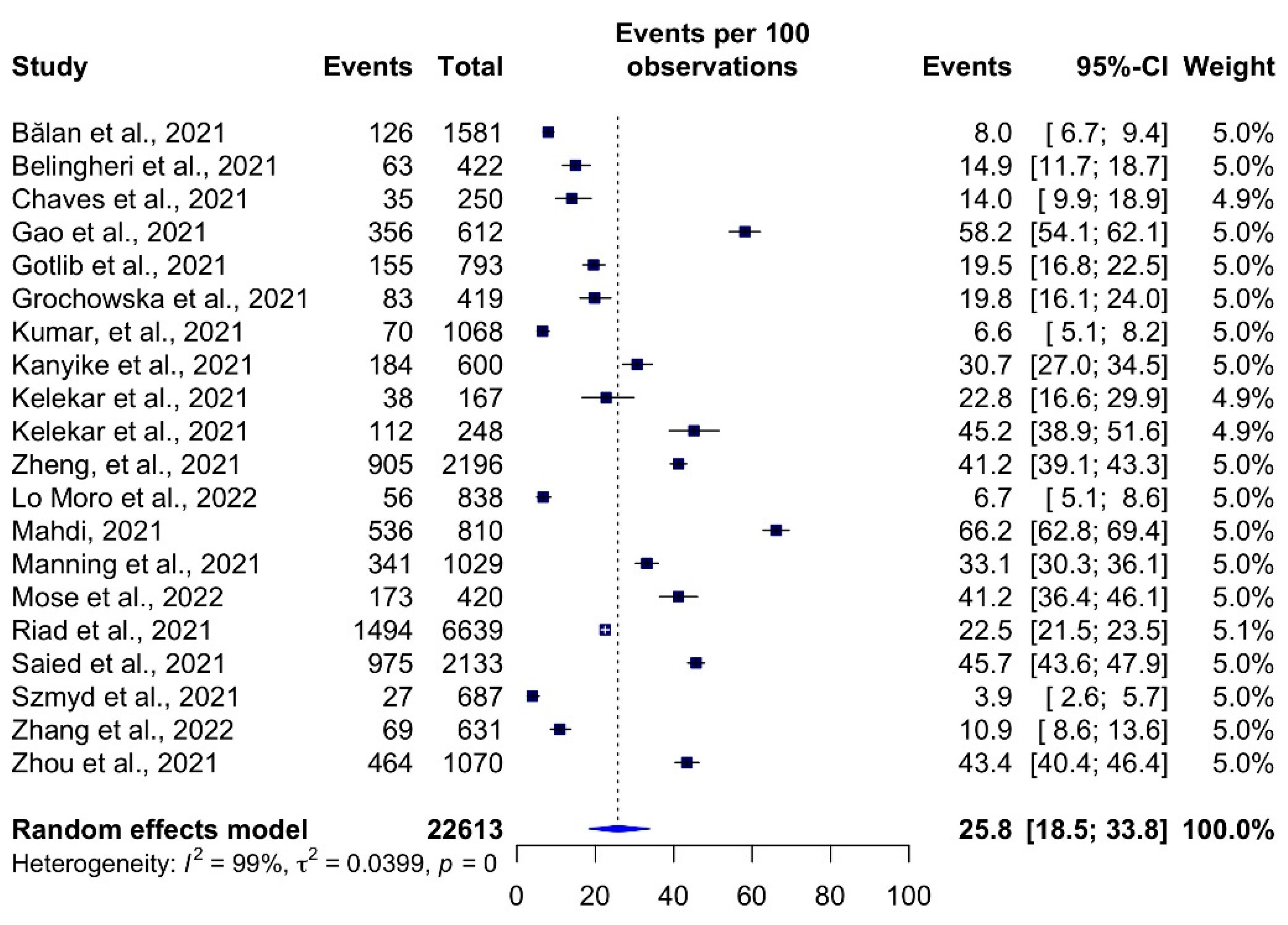
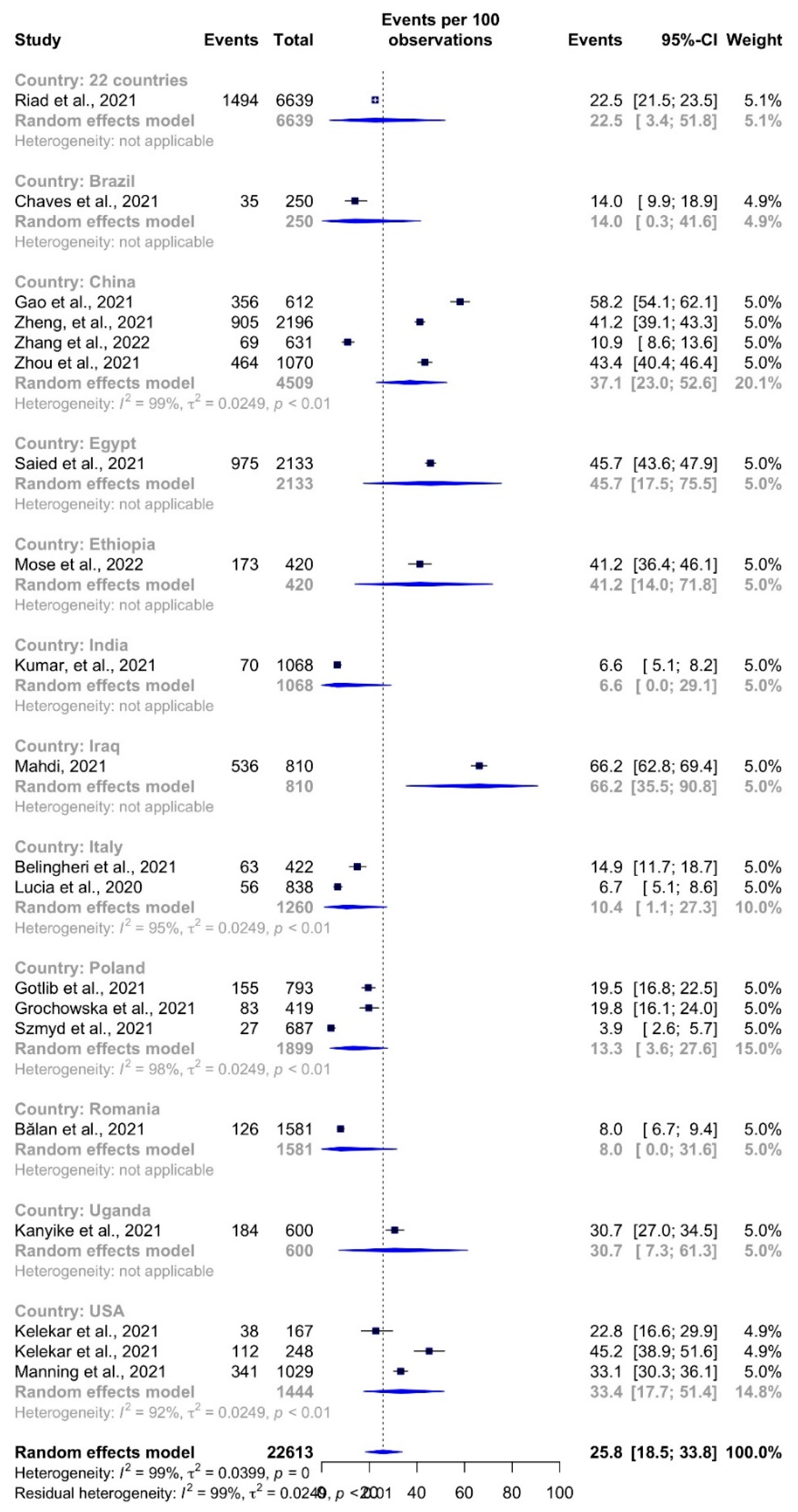
3.3. Prevalence of Vaccine Acceptance and Hesitancy
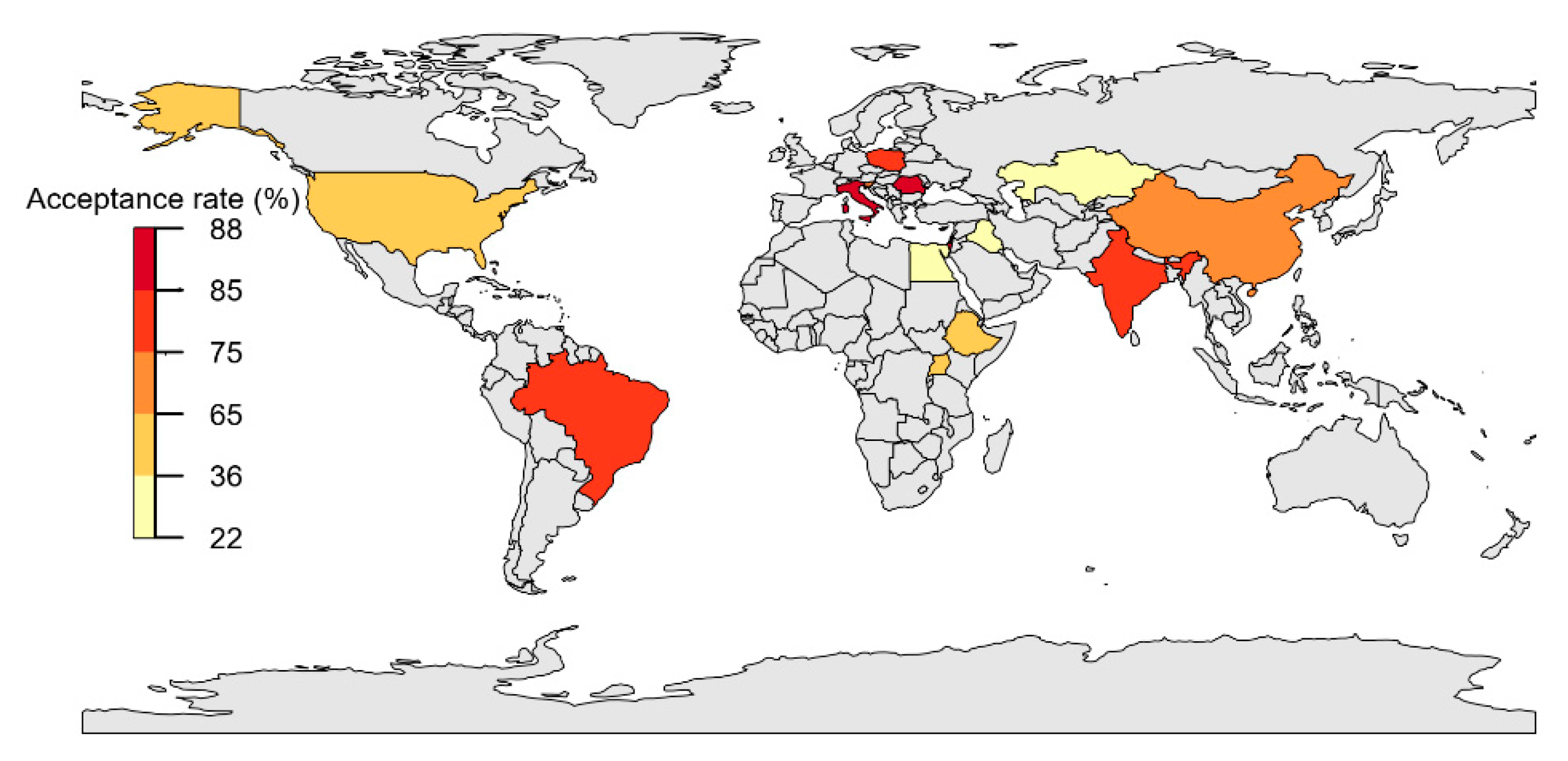
3.4. Sub-Group Analysis
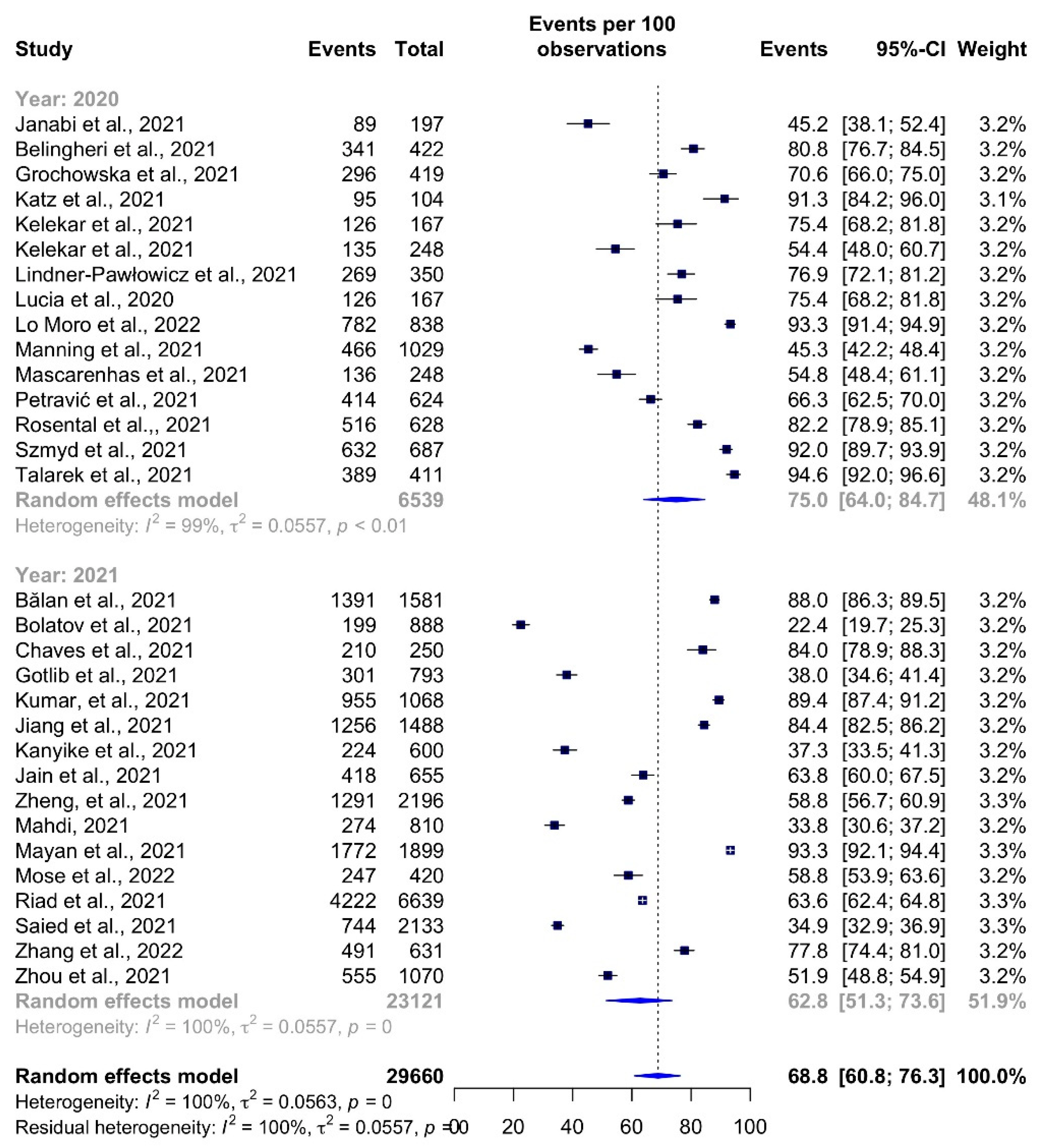
3.5. Time Trends
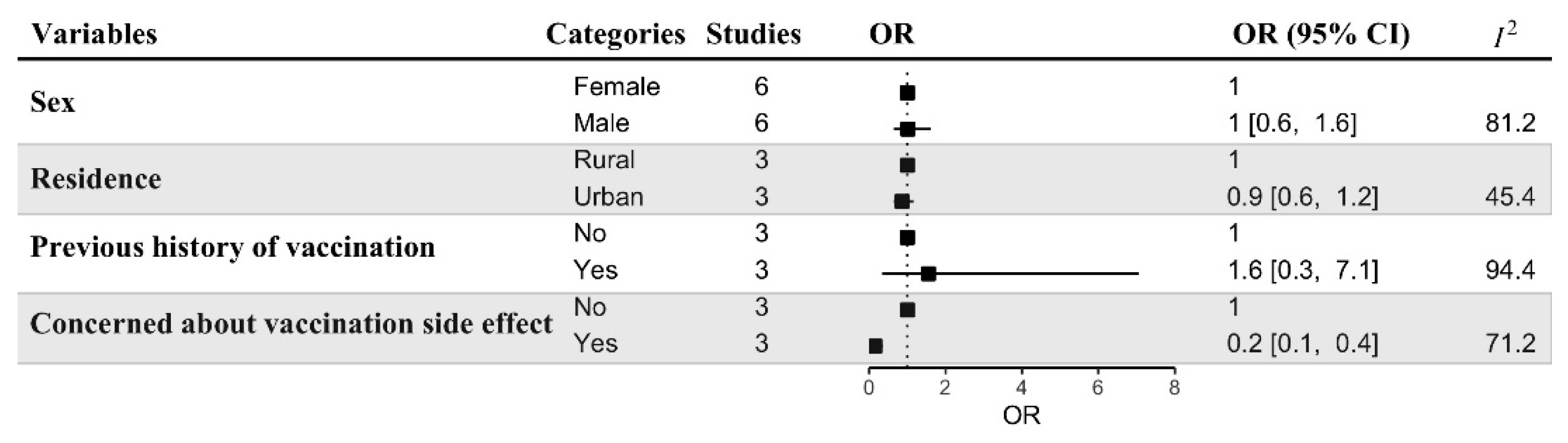
3.6. Predictors of Vaccine Acceptance
3.7. Risk of Bias
4. Discussion
4.1. Summary of the Main Findings
4.2. Implications
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Worldometer COVID Live Update: 223,669,445 Cases and 4,613,672 Deaths from the Coronavirus. Available online: https://www.worldometers.info/coronavirus/ (accessed on 5 September 2021).
- Jiang, N.; Wei, B.; Lin, H.; Wang, Y.; Chai, S.; Liu, W. Nursing students’ attitudes, knowledge and willingness of to receive the coronavirus disease vaccine: A cross-sectional study. Nurse Educ. Pract. 2021, 55, 103148. [Google Scholar] [CrossRef] [PubMed]
- Fontanet, A.; Cauchemez, S. COVID-19 herd immunity: Where are we? Nat. Rev. Immunol. 2020, 20, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Kanyike, A.M.; Olum, R.; Kajjimu, J.; Ojilong, D.; Akech, G.M.; Nassozi, D.R.; Agira, D.; Wamala, N.K.; Asiimwe, A.; Matovu, D.; et al. Acceptance of the coronavirus disease-2019 vaccine among medical students in Uganda. Trop. Med. Health 2021, 49, 37. [Google Scholar] [CrossRef] [PubMed]
- Looi, M.-K. COVID-19: Is a second wave hitting Europe? BMJ 2020, 371, 4113. [Google Scholar] [CrossRef]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A.E.-F. Vaccine hesitancy: Beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef]
- Mullard, A. COVID-19 vaccine development pipeline gears up. Lancet 2020, 395, 1751–1752. [Google Scholar] [CrossRef]
- Forni, G.; Mantovani, A.; Forni, G.; Mantovani, A.; Moretta, L.; Rappuoli, R.; Rezza, G.; Bagnasco, A.; Barsacchi, G.; Bussolati, G.; et al. COVID-19 vaccines: Where we stand and challenges ahead. Cell Death Differ. 2021, 28, 626–639. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Wong, E.L.Y.; Cheung, A.W.L.; Huang, J.; Lai, C.K.C.; Yeoh, E.K.; Chan, P.K.S. COVID-19 vaccine hesitancy in a city with free choice and sufficient doses. Vaccines 2021, 9, 1250. [Google Scholar] [CrossRef]
- Robinson, E.; Jones, A.; Lesser, I.; Daly, M. International estimates of intended uptake and refusal of COVID-19 vaccines: A rapid systematic review and meta-analysis of large nationally representative samples. Vaccine 2021, 39, 2024–2034. [Google Scholar] [CrossRef]
- Gates, A.; Gates, M.; Rahman, S.; Guitard, S.; MacGregor, T.; Pillay, J.; Ismail, S.J.; Tunis, M.C.; Young, K.; Hardy, K.; et al. A systematic review of factors that influence the acceptability of vaccines among Canadians. Vaccine 2021, 39, 222–236. [Google Scholar] [CrossRef]
- Patwary, M.M.; Bardhan, M.; Disha, A.S.; Hasan, M.; Haque, M.Z.; Sultana, R.; Hossain, M.R.; Browning, M.H.E.M.; Alam, M.A.; Sallam, M. Determinants of COVID-19 Vaccine Acceptance among the Adult Population of Bangladesh Using the Health Belief Model and the Theory of Planned Behavior Model. Vaccines 2021, 9, 1393. [Google Scholar] [CrossRef] [PubMed]
- Salomoni, M.G.; di Valerio, Z.; Gabrielli, E.; Montalti, M.; Tedesco, D.; Guaraldi, F.; Gori, D. Hesitant or Not Hesitant? A Systematic Review on Global COVID-19 Vaccine Acceptance in Different Populations. Vaccines 2021, 9, 873. [Google Scholar] [CrossRef]
- Nossier, S.A. Vaccine hesitancy: The greatest threat to COVID-19 vaccination programs. J. Egypt. Public Health Assoc. 2021, 96, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Yang, W. Transmission dynamics of and insights from the 2018-2019 measles outbreak in New York City: A modeling study. Sci. Adv. 2020, 6, 4037–4064. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, L.; Jin, H.; Lin, L. Vaccination against COVID-19: A systematic review and meta-analysis of acceptability and its predictors. Prev. Med. 2021, 150, 106694. [Google Scholar] [CrossRef] [PubMed]
- Kelekar, A.K.; Lucia, V.C.; Afonso, N.M.; Mascarenhas, A.K. COVID-19 vaccine acceptance and hesitancy among dental and medical students. J. Am. Dent. Assoc. 2021, 152, 596–603. [Google Scholar] [CrossRef]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2020, 1–5, 445–449. [Google Scholar] [CrossRef]
- Bazan, D.; Nowicki, M.; Rzymski, P. Medical students as the volunteer workforce during the COVID-19 pandemic: Polish experience. Int. J. Disaster Risk Reduct. 2021, 55, 102109. [Google Scholar] [CrossRef] [PubMed]
- Mascarenhas, A.K.; Lucia, V.C.; Kelekar, A.; Afonso, N.M. Dental students’ attitudes and hesitancy toward COVID-19 vaccine. J. Dent. Educ. 2021, 85, 1504–1510. [Google Scholar] [CrossRef]
- Manning, M.L.; Gerolamo, A.M.; Marino, M.A.; Hanson-Zalot, M.E.; Pogorzelska-Maziarz, M. COVID-19 vaccination readiness among nurse faculty and student nurses. Nurs. Outlook 2021, 69, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.; Cartmill, R.; Johnson-Gordon, B.; Landes, M.; Malik, K.; Sinnott, J.; Wallace, K.; Wallin, R. Preparing for a School-Located COVID-19 Vaccination Clinic. NASN Sch. Nurse 2021, 36, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Jain, J.; Saurabh, S.; Goel, A.D.; Gupta, M.K.; Bhardwaj, P.; Raghav, P.R. COVID-19 vaccine hesitancy among undergraduate medical students. medRxiv 2021, 12. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Wake, A.D. The Willingness to Receive COVID-19 Vaccine and Its Associated Factors: “Vaccination Refusal Could Prolong the War of This Pandemic”—A Systematic Review. Risk Manag. Healthc. Policy 2021, 14, 2609. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Yang, Y.; Liu, Y.; Zheng, D.; Shao, L.; Jin, J.; He, Q. Intention to COVID-19 vaccination and associated factors among health care workers: A systematic review and meta-analysis of cross-sectional studies. Am. J. Infect. Control 2021, 49, 1295–1304. [Google Scholar] [CrossRef]
- Li, M.; Luo, Y.; Watson, R.; Zheng, Y.; Ren, J.; Tang, J.; Chen, Y. Healthcare workers’ (HCWs) attitudes and related factors towards COVID-19 vaccination: A rapid systematic review. Postgrad. Med. J. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Garritty, C.; Gartlehner, G.; Nussbaumer-Streit, B.; King, V.J.; Hamel, C.; Kamel, C.; Affengruber, L.; Stevens, A. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J. Clin. Epidemiol. 2021, 130, 13–22. [Google Scholar] [CrossRef]
- Joanna Briggs Institute. Checklist for Analytical cross Sectional Studies, Critical Appraisal Tools. 2017. Available online: https://jbi.global/critical-appraisal-tools (accessed on 18 May 2022).
- Al-Amer, R.; Maneze, D.; Everett, B.; Montayre, J.; Villarosa, A.R.; Dwekat, E.; Salamonson, Y. COVID-19 vaccination intention in the first year of the pandemic: A systematic review. J. Clin. Nurs. 2021, 1–25. [Google Scholar] [CrossRef]
- Villarosa, A.R.; Maneze, D.; Ramjan, L.M.; Srinivas, R.; Camilleri, M.; George, A. The effectiveness of guideline implementation strategies in the dental setting: A systematic review. Implement. Sci. 2019, 14, 1–16. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Katz, M.; Azrad, M.; Glikman, D.; Peretz, A. COVID-19 Vaccination Compliance and Associated Factors among Medical Students during an Early Phase of Vaccination Rollout—A Survey from Israel. Vaccines 2021, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koščík, M.; Mendes, J.J.; Klugar, M.; Kateeb, E. Global prevalence and drivers of dental students’ covid-19 vaccine hesitancy. Vaccines 2021, 9, 566. [Google Scholar] [CrossRef] [PubMed]
- Al Janabi, T.; Chinsky, R.; Pino, M.A. Perceptions of COVID-19 vaccines among osteopathic medical students (OMS). Int. J. Osteopath. Med. 2021, 42, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Bălan, A.; Bejan, I.; Bonciu, S.; Eni, C.E.; Ruță, S. Romanian medical students’ attitude towards and perceived knowledge on covid-19 vaccination. Vaccines 2021, 9, 854. [Google Scholar] [CrossRef] [PubMed]
- Belingheri, M.; Ausili, D.; Paladino, M.E.; Luciani, M.; Di Mauro, S.; Riva, M.A. Attitudes towards COVID-19 vaccine and reasons for adherence or not among nursing students. J. Prof. Nurs. 2021, 37, 923–927. [Google Scholar] [CrossRef]
- Bolatov, A.K.; Seisembekov, T.Z.; Askarova, A.Z.; Pavalkis, D. Barriers to COVID-19 vaccination among medical students in Kazakhstan: Development, validation, and use of a new COVID-19 Vaccine Hesitancy Scale. Hum. Vaccines Immunother. 2021, 17, 4982–4992. [Google Scholar] [CrossRef]
- De Sousa Chaves, Í.E.; Brito, P.R.P.; de Araújo Rodrigues, J.G.B.; Costa, M.S.; Cândido, E.L.; Moreira, M.R.C. Hesitation regarding the covid-19 vaccine among medical students in brazil. Rev. Assoc. Med. Bras. 2021, 67, 1397–1402. [Google Scholar] [CrossRef]
- Gao, X.; Li, H.; He, W.; Zeng, W. COVID-19 Vaccine Hesitancy among Medical Students: The Next COVID-19 Challenge in Wuhan, China. Disaster Med. Public Health Prep. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gotlib, J.; Sobierajski, T.; Jaworski, M.; Wawrzuta, D.; Borowiak, E.; Dobrowolska, B.; Dyk, D.; Gaworska-Krzemińska, A.; Grochans, E.; Kózka, M.; et al. “Vaccinate, Do Not Hesitate!”. Vaccination Readiness against COVID-19 among Polish Nursing Undergraduate Students: A National Cross-Sectional Survey. Vaccines 2021, 9, 1029. [Google Scholar] [CrossRef] [PubMed]
- Grochowska, M.; Ratajczak, A.; Zdunek, G.; Adamiec, A.; Waszkiewicz, P.; Feleszko, W. A Comparison of the Level of Acceptance and Hesitancy towards the Influenza Vaccine and the Forthcoming COVID-19 Vaccine in the Medical Community. Vaccines 2021, 9, 475. [Google Scholar] [CrossRef] [PubMed]
- Jain, J.; Saurabh, S.; Kumar, P.; Verma, M.K.; Goel, A.D.; Gupta, M.K.; Bhardwaj, P.; Raghav, P.R. COVID-19 vaccine hesitancy among medical students in India. Epidemiol. Infect. 2021, 149, 132. [Google Scholar] [CrossRef] [PubMed]
- Jain, L.; Vij, J.; Satapathy, P.; Chakrapani, V.; Patro, B.; Kar, S.S.; Singh, R.; Pala, S.; Sankhe, L.; Modi, B.; et al. Factors Influencing COVID-19 Vaccination Intentions Among College Students: A Cross-Sectional Study in India. Front. Public Health 2021, 9, 1966. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zheng, Y.; Luo, Y.; Ren, J.; Jiang, L.; Tang, J.; Yu, X.; Luo, D.; Fan, D.; Chen, Y. Hesitancy toward COVID-19 vaccines among medical students in Southwest China: A cross-sectional study. Hum. Vaccin. Immunother. 2021, 17, 4021–4027. [Google Scholar] [PubMed]
- Lindner-Pawłowicz, K.; Mydlikowska-śmigórska, A.; Łampika, K.; Sobieszczańska, M. COVID-19 Vaccination Acceptance among Healthcare Workers and General Population at the Very Beginning of the National Vaccination Program in Poland: A Cross-Sectional, Exploratory Study. Vaccines 2021, 10, 66. [Google Scholar] [CrossRef] [PubMed]
- Lo Moro, G.; Cugudda, E.; Bert, F.; Raco, I.; Siliquini, R. Vaccine Hesitancy and Fear of COVID-19 Among Italian Medical Students: A Cross-Sectional Study. J. Community Health 2022, 1–9. [Google Scholar] [CrossRef]
- Mahdi, B.M. COVID-19 vaccine hesitancy and acceptance among medical students: An online cross-sectional study in Iraq. Open Access Maced. J. Med. Sci. 2021, 9, 955–958. [Google Scholar] [CrossRef]
- Mayan, D.; Nguyen, K.; Keisler, B. National attitudes of medical students towards mandating the COVID-19 vaccine and its association with knowledge of the vaccine. PLoS ONE 2021, 16, e0260898. [Google Scholar] [CrossRef]
- Mose, A.; Haile, K.; Timerga, A. COVID-19 vaccine hesitancy among medical and health science students attending Wolkite University in Ethiopia. PLoS ONE 2022, 17, e0263081. [Google Scholar] [CrossRef]
- Petravić, L.; Arh, R.; Gabrovec, T.; Jazbec, L.; Rupčić, N.; Starešinič, N.; Zorman, L.; Pretnar, A.; Srakar, A.; Zwitter, M.; et al. Factors affecting attitudes towards covid-19 vaccination: An online survey in slovenia. Vaccines 2021, 9, 247. [Google Scholar] [CrossRef] [PubMed]
- Rosental, H.; Shmueli, L. Integrating Health Behavior Theories to Predict COVID-19 Vaccine Acceptance: Differences between Medical Students and Nursing Students. Vaccines 2021, 9, 783. [Google Scholar] [CrossRef] [PubMed]
- Szmyd, B.; Bartoszek, A.; Karuga, F.F.; Staniecka, K.; Błaszczyk, M.; Radek, M. Medical students and sars-cov-2 vaccination: Attitude and behaviors. Vaccines 2021, 9, 128. [Google Scholar] [CrossRef]
- Talarek, E.; Warzecha, J.; Banasiuk, M.; Banaszkiewicz, A. Influenza Vaccination Coverage and Intention to Receive Hypothetical Ebola and COVID-19 Vaccines among Medical Students. Vaccines 2021, 9, 709. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Dean, J.; Yin, Y.; Wang, D.; Sun, Y.; Zhao, Z.; Wang, J. Determinants of COVID-19 Vaccine Acceptance and Hesitancy: A Health Care Student-Based Online Survey in Northwest China. Front. Public Health 2022, 9, 2146. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wang, Y.; Li, Z. Intention to get vaccinated against COVID-19 among nursing students: A cross-sectional survey. Nurse Educ. Today 2021, 107, 105152. [Google Scholar] [CrossRef] [PubMed]
- Patwary, M.M.; Alam, M.A.; Bardhan, M.; Disha, A.S.; Haque, M.Z.; Billah, S.M.; Kabir, M.P.; Browning, M.H.E.M.; Rahman, M.M.; Parsa, A.D.; et al. COVID-19 Vaccine Acceptance among Low- and Lower-Middle-Income Countries: A Rapid Systematic Review and Meta-Analysis. Vaccines 2022, 10, 427. [Google Scholar] [CrossRef]
- Ahmed, M.A.M.; Colebunders, R.; Gele, A.A.; Farah, A.A.; Osman, S.; Guled, I.A.; Abdullahi, A.A.M.; Hussein, A.M.; Ali, A.M.; Siewe Fodjo, J.N. COVID-19 Vaccine Acceptability and Adherence to Preventive Measures in Somalia: Results of an Online Survey. Vaccines 2021, 9, 543. [Google Scholar] [CrossRef]
- Nguyen, K.H.; Srivastav, A.; Razzaghi, H.; Williams, W.; Lindley, M.C.; Jorgensen, C.; Abad, N.; Singleton, J.A. COVID-19 Vaccination Intent, Perceptions, and Reasons for Not Vaccinating Among Groups Prioritized for Early Vaccination—United States, September and December 2020. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 217–222. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Intention of healthcare workers to accept COVID-19 vaccination and related factors: A systematic review and meta-analysis. Asian Pac. J. Trop. Med. 2021, 14, 543. [Google Scholar] [CrossRef]
- Ramachandran, R.; Ross, J.S.; Miller, J.E. Access to COVID-19 Vaccines in High-, Middle-, and Low-Income Countries Hosting Clinical Trials. JAMA Netw. Open 2021, 4, 2134233. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Bono, S.A.; Faria de Moura Villela, E.; Siau, C.S.; Chen, W.S.; Pengpid, S.; Hasan, M.T.; Sessou, P.; Ditekemena, J.D.; Amodan, B.O.; Hosseinipour, M.C.; et al. Factors Affecting COVID-19 Vaccine Acceptance: An International Survey among Low- and Middle-Income Countries. Vaccines 2021, 9, 515. [Google Scholar] [CrossRef] [PubMed]
- Kabamba Nzaji, M.; Kabamba Ngombe, L.; Ngoie Mwamba, G.; Banza Ndala, D.B.; Mbidi Miema, J.; Luhata Lungoyo, C.; Lora Mwimba, B.; Cikomola Mwana Bene, A.; Mukamba Musenga, E. Acceptability of Vaccination Against COVID-19 Among Healthcare Workers in the Democratic Republic of the Congo. Pragmatic Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef]
- Dzinamarira, T.; Nachipo, B.; Phiri, B.; Musuka, G. COVID-19 vaccine roll-out in south africa and zimbabwe: Urgent need to address community preparedness, fears and hesitancy. Vaccines 2021, 9, 250. [Google Scholar] [CrossRef] [PubMed]
- Nehal, K.R.; Steendam, L.M.; Ponce, M.C.; van der Hoeven, M.; Smit, G.S.A. Worldwide vaccination willingness for covid-19: A systematic review and meta-analysis. Vaccines 2021, 9, 1071. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccin. Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Anti-Vaccine Attitudes and Risk Factors for Not Agreeing to Vaccination Against COVID-19 Amongst 32,361 UK Adults: Implications for Public Health Communications. SSRN Electron. J. 2020, 1, 100012. [Google Scholar] [CrossRef]
- Roozenbeek, J.; Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; Van Der Bles, A.M.; Van Der Linden, S. Susceptibility to misinformation about COVID-19 around the world: Susceptibility to COVID misinformation. R. Soc. Open Sci. 2020, 7, 201199. [Google Scholar] [CrossRef]
- Hussein, A.A.M.; Galal, I.; Makhlouf, N.A.; Makhlouf, H.A.; Abd-Elaal, H.K.; Kholief, K.M.; Saad, M.M.; Abdellah, D.A. A national survey of potential acceptance of COVID-19 vaccines in healthcare workers in Egypt. medRxiv 2021. [Google Scholar] [CrossRef]
- Wright, K.B. Researching internet-based populations: Advantages and disadvantages of online survey research, online questionnaire authoring software packages, and web survey services. J. Comput. Commun. 2005, 10, JCMC1034. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patwary, M.M.; Bardhan, M.; Haque, M.Z.; Sultana, R.; Alam, M.A.; Browning, M.H.E.M. COVID-19 Vaccine Acceptance Rate and Its Factors among Healthcare Students: A Systematic Review with Meta-Analysis. Vaccines 2022, 10, 806. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050806
Patwary MM, Bardhan M, Haque MZ, Sultana R, Alam MA, Browning MHEM. COVID-19 Vaccine Acceptance Rate and Its Factors among Healthcare Students: A Systematic Review with Meta-Analysis. Vaccines. 2022; 10(5):806. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050806
Chicago/Turabian StylePatwary, Muhammad Mainuddin, Mondira Bardhan, Md. Zahidul Haque, Rabeya Sultana, Md Ashraful Alam, and Matthew H. E. M. Browning. 2022. "COVID-19 Vaccine Acceptance Rate and Its Factors among Healthcare Students: A Systematic Review with Meta-Analysis" Vaccines 10, no. 5: 806. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050806