
COVID-19 Vaccination Scenarios: A Cost-Effectiveness Analysis for Turkey

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
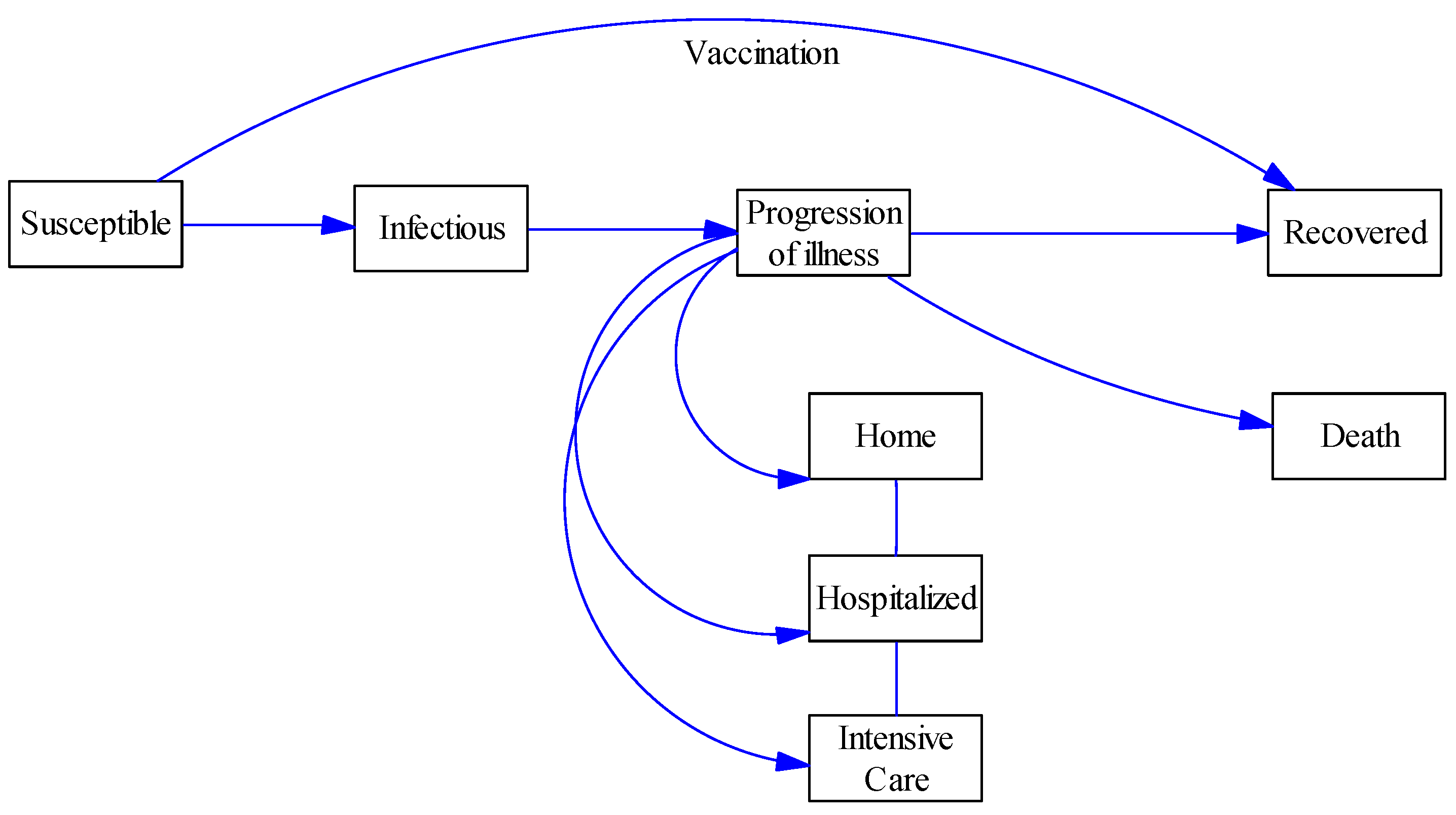
2.2. Dynamic Transmission Model
2.3. Scenarios
2.4. Costs
2.5. Sensitivity Analysis
3. Results
3.1. Initial Situation
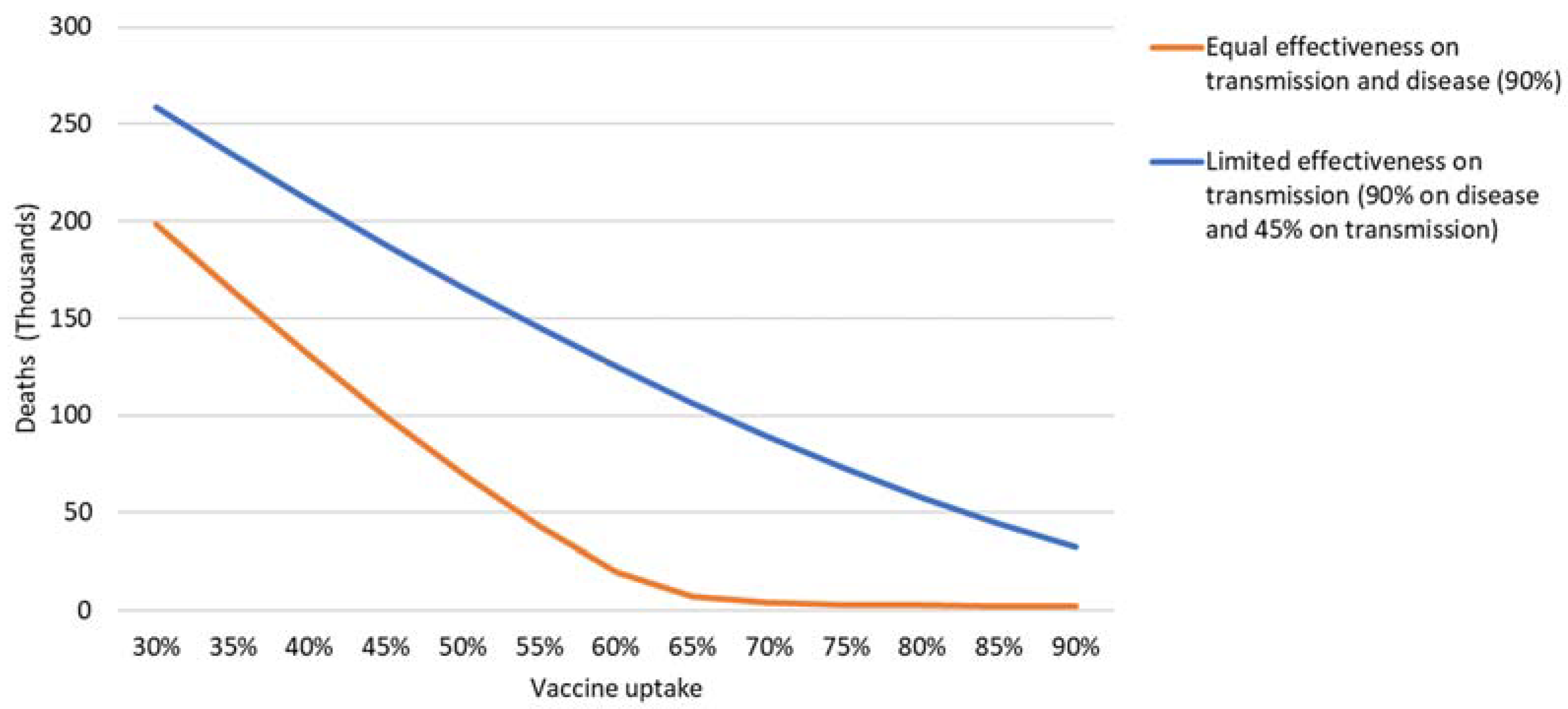
3.2. Equal Effectiveness on Transmission and Disease
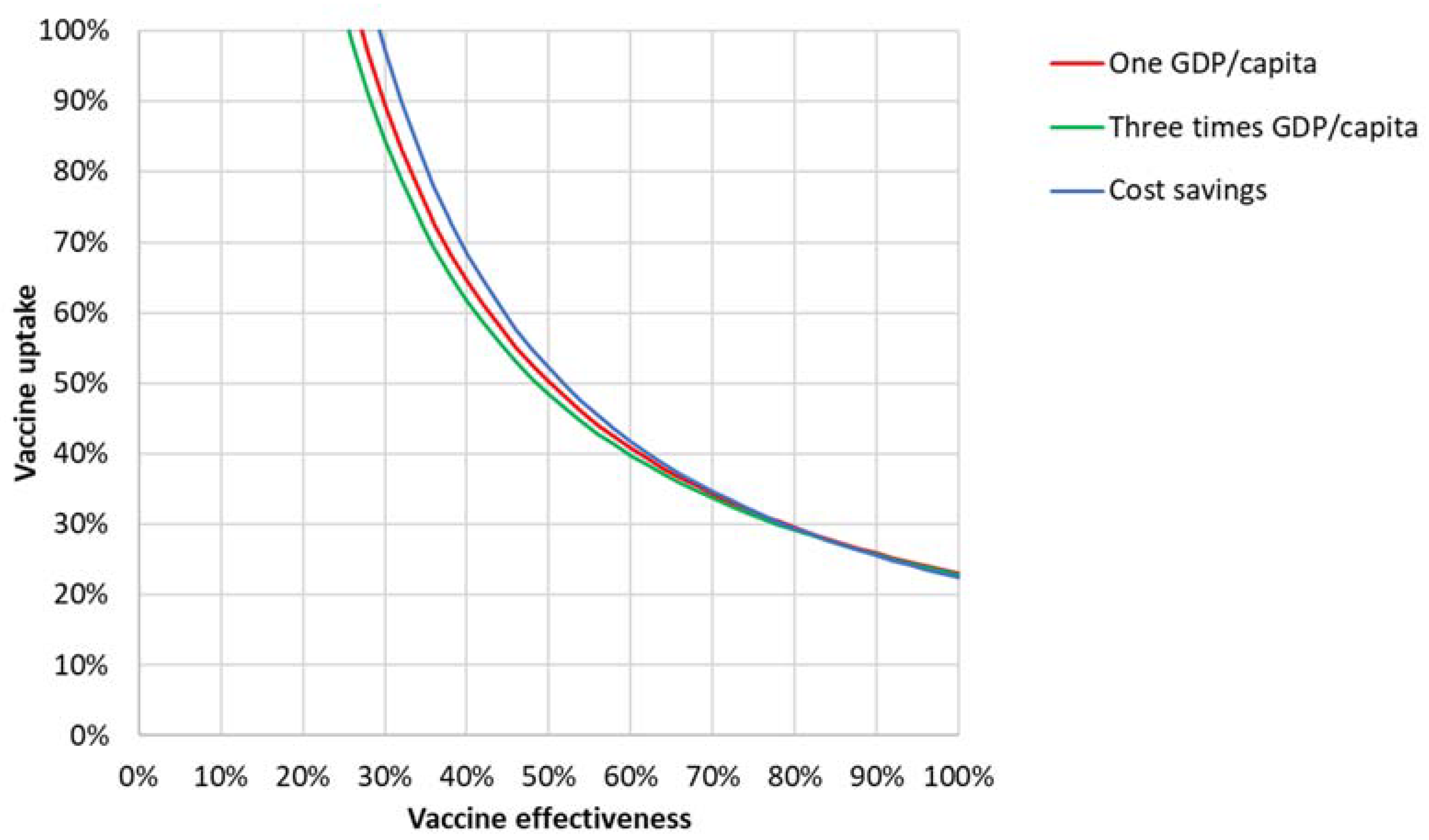
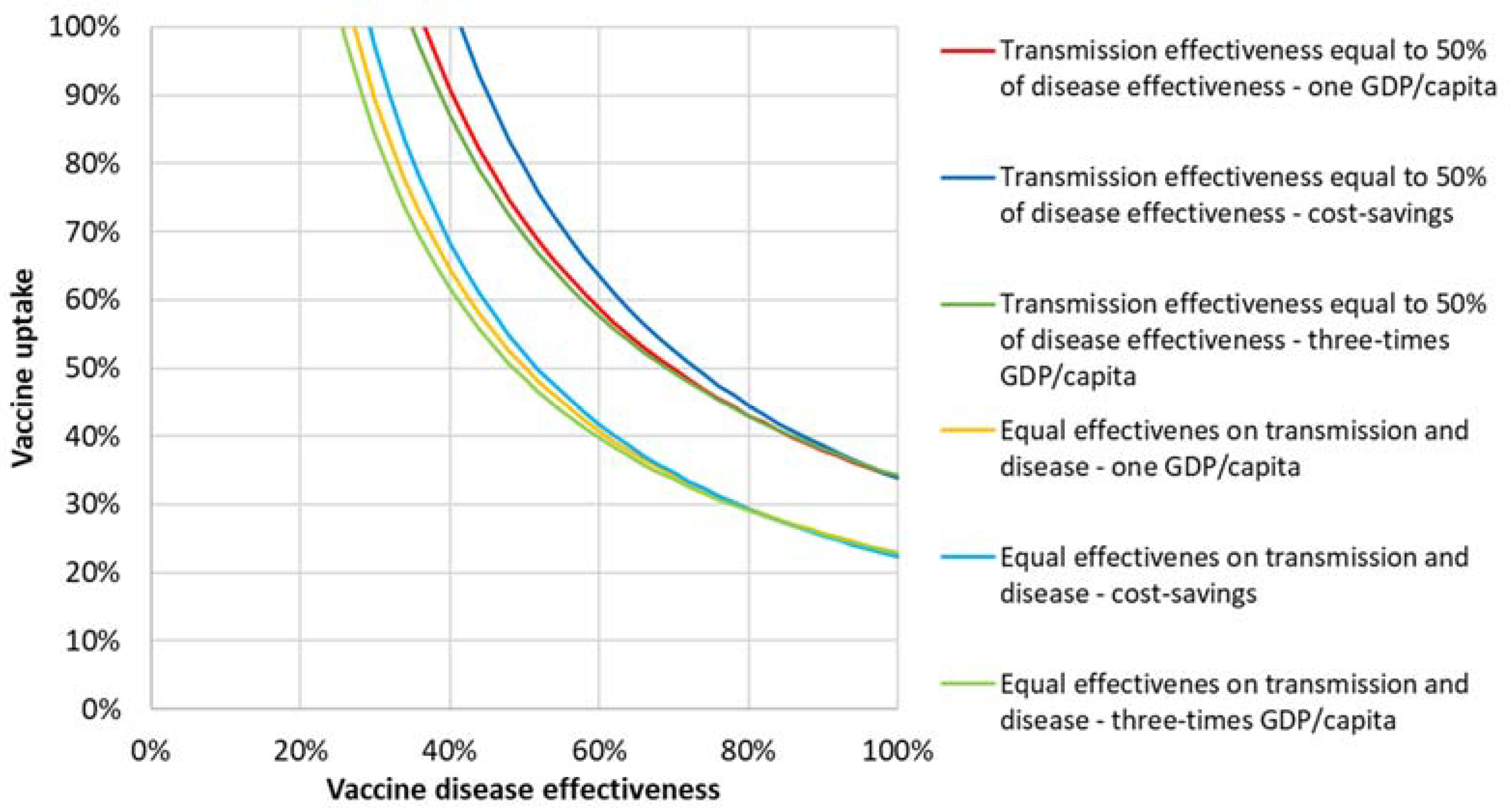
3.2.1. Cost-Effectiveness Analysis
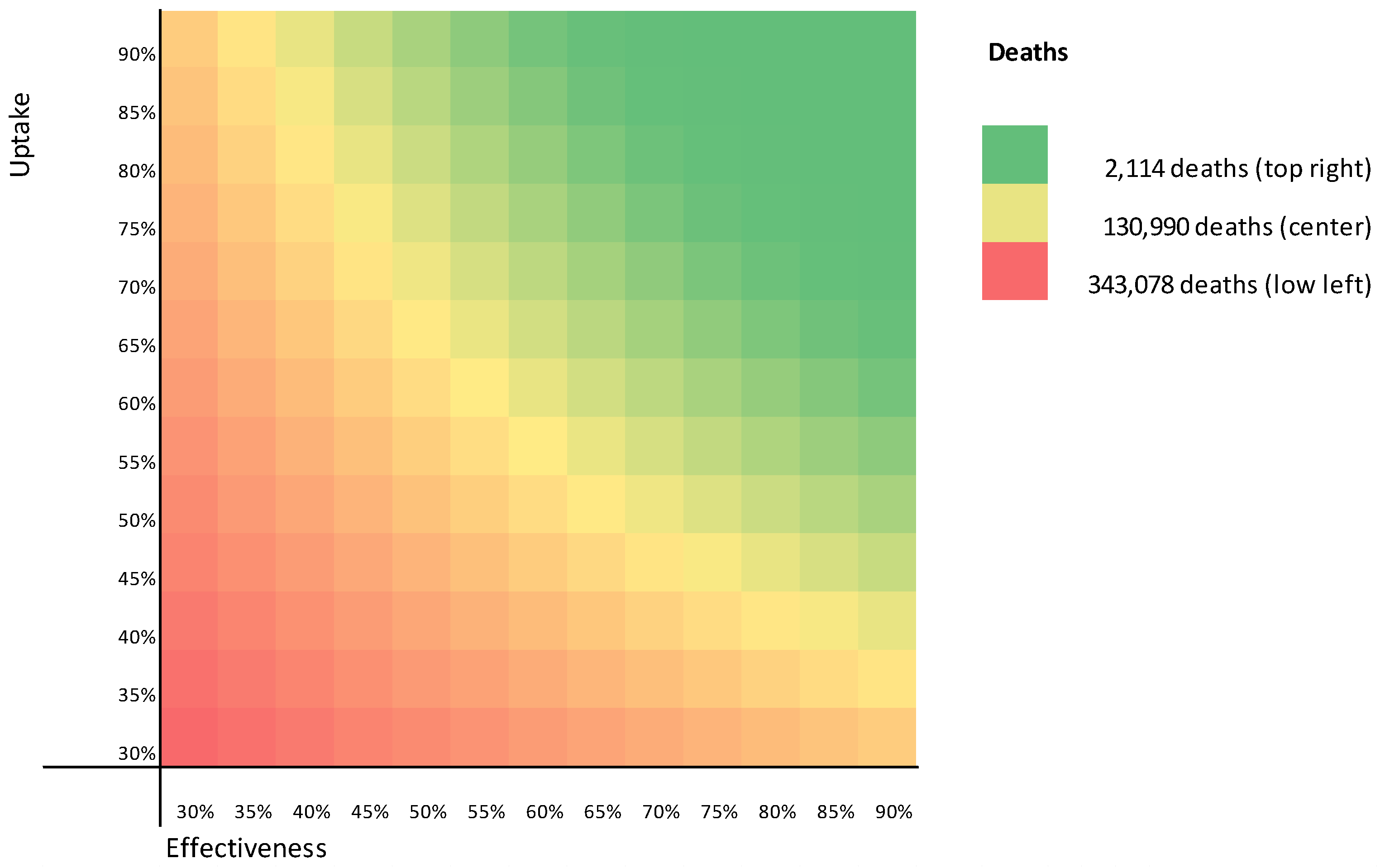
3.2.2. Sensitivity Analysis
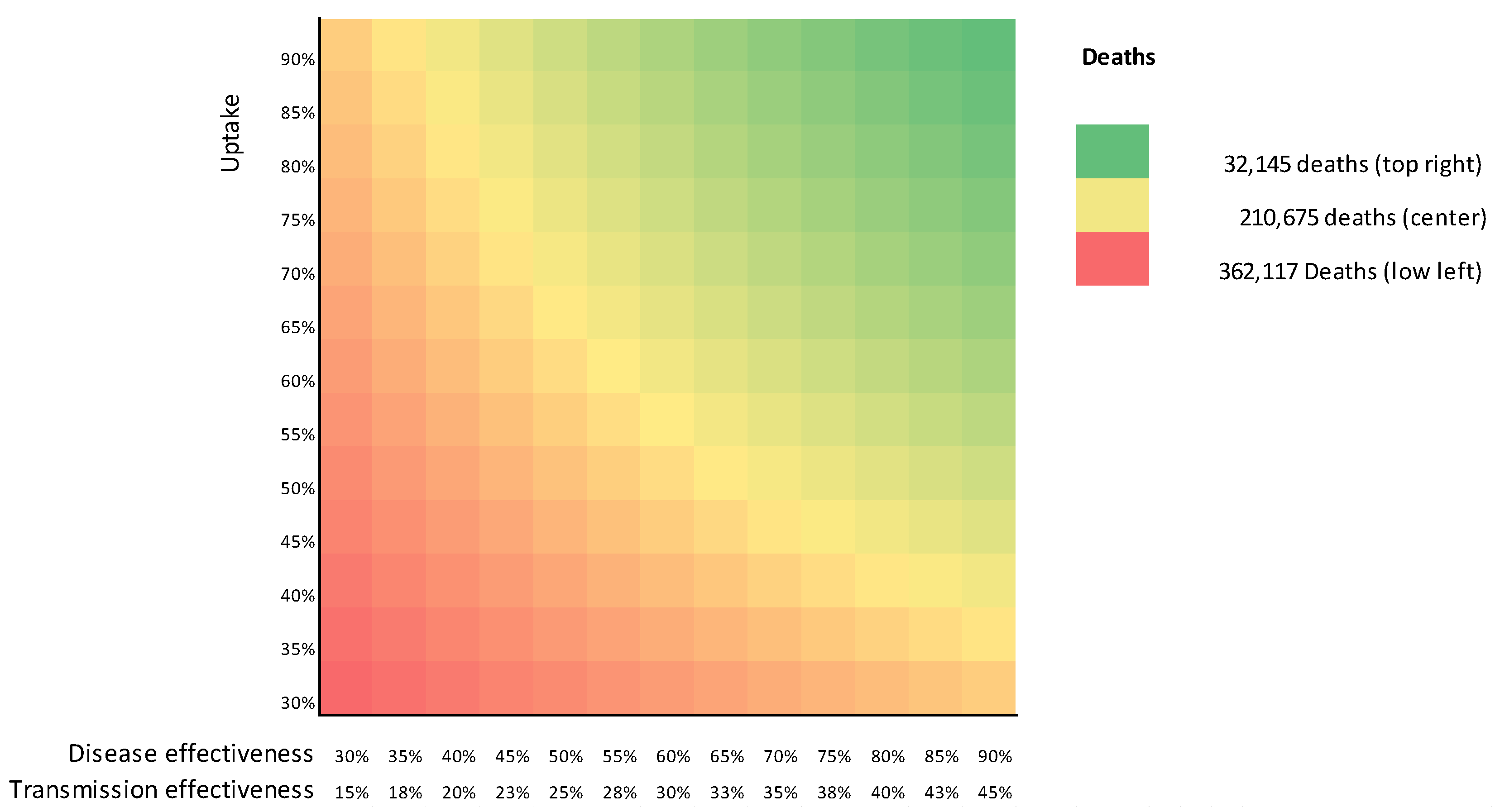
3.3. Limited Effectiveness on Transmission
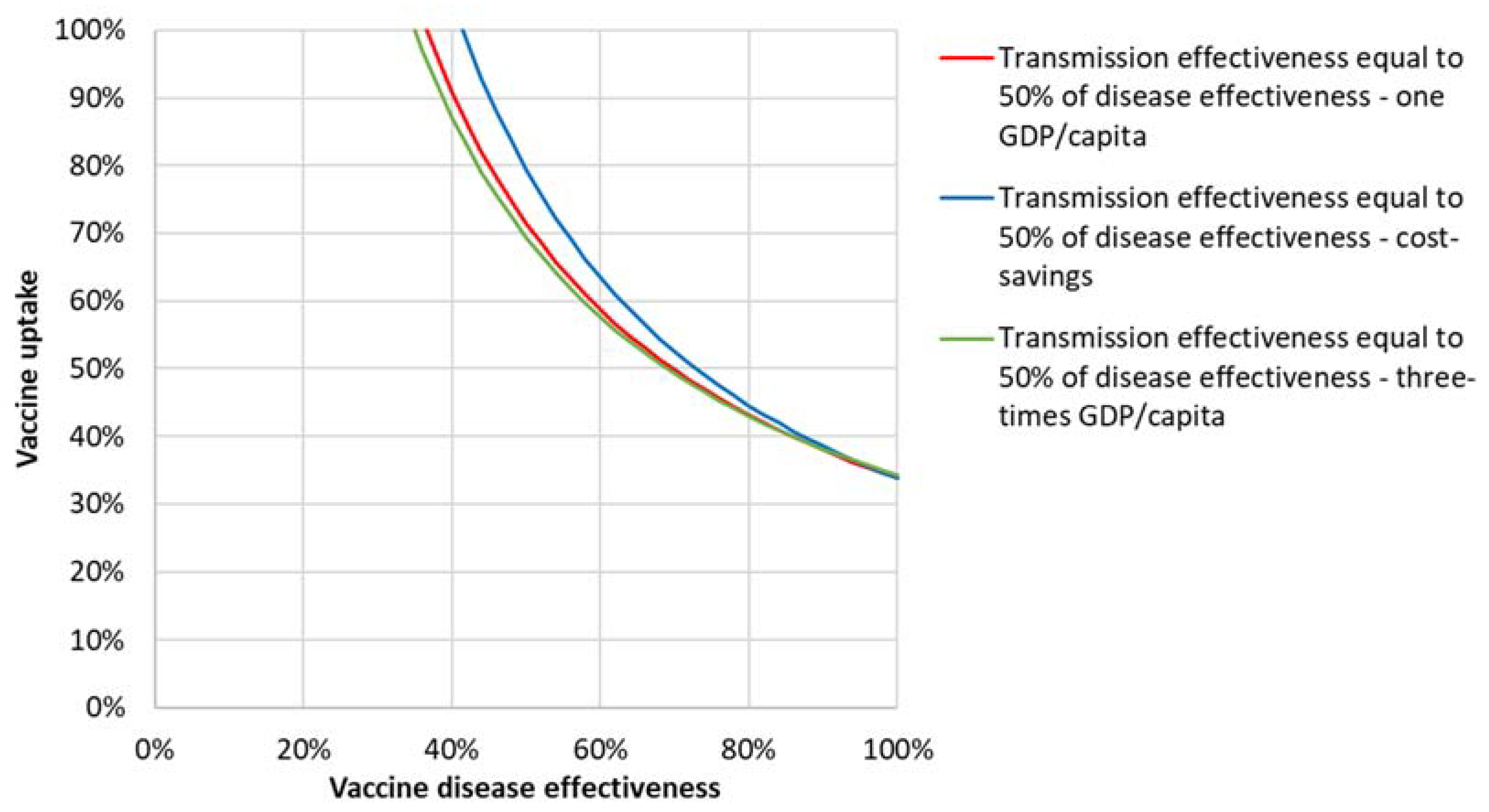
3.3.1. Cost-Effectiveness Analysis
3.3.2. Sensitivity Analysis
3.4. Comparison of Scenarios
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Model Parameters

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Age Classes | General | References | ||||
|---|---|---|---|---|---|---|---|
| 0–19 | 20–39 | 40–59 | ≥60 | ||||
| 1. General | |||||||
| 1.1 Total Population | 83,429,615 | [51] | |||||
| 1.2 Share of total population (fraction) | 0.325 | 0.310 | 0.238 | 0.127 | [52] | ||
| 1.3 Case-fatality rate (deaths/case) | 0.000030 | 0.000282 | 0.004858 | 0.087421 | Estimated | ||
| Recovery rate | 0.999970 | 0.999718 | 0.995142 | 0.912579 | |||
| 1.4 Years of expected life left | 64.34 | 44.92 | 26.71 | 8.75 | [28] | ||
| 1.5 Quality-adjusted years of life left 3% DR | 26.54 | 21.94 | 14.88 | 5.40 | [27] | ||
| 1.6 Quality-adjusted years of life left 0% DR | 57.33 | 38.62 | 21.02 | 6.09 | [27] | ||
| 1.7 Quality-adjusted years of life left 5% DR | 18.47 | 16.34 | 12.22 | 5.00 | [27] | ||
| 2. Recovery location fractions after infection | |||||||
| 2.1 At home | 0.999356 | 0.998336 | 0.992295 | 0.875283 | [38,39,53] + model | ||
| 2.2 Normal hospitalization | 0.000628 | 0.001453 | 0.005931 | 0.101664 | [38,39,53] + model | ||
| 2.3 Intensive care | 0.000016 | 0.000211 | 0.001774 | 0.023053 | [38,39,53] + model | ||
| 3. Duration of recovery (days) | |||||||
| 3.1 At home | 1 | [38,39] | |||||
| 3.2 Normal hospitalization | 7.4 | [38,39] | |||||
| 3.3 Intensive care | 17.7 | [38,39] | |||||
| 4. Health care costs per day (USD) | |||||||
| 4.1 At home | 1 | Assumption | |||||
| 4.2 Normal hospitalization | 110 | [42] | |||||
| 4.3 Intensive care | 171 | [42] | |||||
| 5. Productivity costs (USD) | |||||||
| 5.1 Productivity loss due to premature death | 239.30 | 3711.20 | 4510.65 | 1525.29 | Calculated | ||
| 5.2 Productivity loss due to sickness per day | 2.43 | 37.66 | 45.77 | 15.48 | Calculated | ||
| 5.3 Nonproductive days | |||||||
| 5.3.1 Home | 10 | Assumption | |||||
| 5.3.2 Normal Hospitalization | 12.35 | Assumption | |||||
| 5.3.3 Intensive care | 28 | Assumption | |||||
| 5.4 Home working share | 0.25 | Assumption | |||||
| 5.5 Friction period (year) | 0.27 | [41] | |||||
| 5.6 GDP per year per capita | 886 | 13,745 | 16,706 | 5649 | Appendix B | ||
| 6. Infectious period | 8 | [54,55,56,57] | |||||
| 7. Basic reproduction number (R0) | 2.8 | [29] | |||||
| 7.1 R0 in natural measures mode | 1.8 | Assumption | |||||
| 7.2 R0 in enforced long measures mode | 1.08 | Assumption | |||||
| 8. Contact matrix—fixed | |||||||
| 0–19 | 3.02155 | 0.91557 | 0.55907 | 0.13828 | [22] | ||
| 20–39 | 0.95991 | 1.93832 | 0.69595 | 0.12841 | [22] | ||
| 40–59 | 0.76151 | 0.90416 | 0.72299 | 0.14798 | [22] | ||
| ≥60 | 0.35273 | 0.31242 | 0.27712 | 0.22518 | [22] | ||
Appendix B. GDP per Capita by Age Group
| Age Group | # Persons in Group [52] | # of People Working (2018) [58] | Average Annual Wage (TRY 2018) [58] | Total Wage (TRY) | Share | GDP per Age Group (USD) | GDP/Capita (USD) |
|---|---|---|---|---|---|---|---|
| 0–19 | 27,087,441 | 1,580,000 | 28,117.33 | 44,425,373,634.55 | 3% | 24,007,496,131 | 886 |
| 20–39 | 25,836,161 | 14,066,000 | 46,718.91 | 657,148,242,209.70 | 46% | 355,123,268,339 | 13,745 |
| 40–59 | 19,886,588 | 11,041,000 | 55,681.63 | 614,780,864,598.12 | 43% | 332,227,914,381 | 16,706 |
| ≥60 | 10,619,425 | 1,830,000 | 60,662.68 | 111,012,695,467.37 | 8% | 59,991,321,150 | 5649 |
| Total | 83,429,615 | 28,517,000 | 1,427,367,175,909.73 | 771,350,000,000 | 9246 |
Appendix C. Differential Equations
References
- World Health Organization WHO Coronavirus Disease (COVID-19) Dashboard | WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 2 March 2021).
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Boulware, D.R.; Pullen, M.F.; Bangdiwala, A.S.; Pastick, K.A.; Lofgren, S.M.; Okafor, E.C.; Skipper, C.P.; Nascene, A.A.; Nicol, M.R.; Abassi, M.; et al. A randomized trial of hydroxychloroquine as postexposure prophylaxis for Covid-19. N. Engl. J. Med. 2020, 383, 517–525. [Google Scholar] [CrossRef]
- Deb, P.; Molla, M.M.A.; Saif-Ur-Rahman, K.M. An update to monoclonal antibody as therapeutic option against COVID-19. Biosaf. Heal. 2021. [Google Scholar] [CrossRef]
- Schaffer DeRoo, S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 vaccination program. JAMA 2020, 323, 2458. [Google Scholar] [CrossRef]
- Shah, A.; Marks, P.W.; Hahn, S.M. Unwavering Regulatory Safeguards for COVID-19 Vaccines. J. Am. Med. Assoc. 2020, 324, 931–932. [Google Scholar] [CrossRef] [PubMed]
- Thanh Le, T.; Andreadakis, Z.; Kumar, A.; Gómez Román, R.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA vaccine against SARS-CoV-2—Preliminary report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Xia, S.; Duan, K.; Zhang, Y.; Zhao, D.; Zhang, H.; Xie, Z.; Li, X.; Peng, C.; Zhang, Y.; Zhang, W.; et al. Effect of an inactivated vaccine against SARS-CoV-2 on safety and immunogenicity outcomes: Interim analysis of 2 randomized clinical trials. J. Am. Med. Assoc. 2020, 324, 951–960. [Google Scholar] [CrossRef] [PubMed]
- JCVI JCVI Interim Statement on Phase 2 of the COVID-19 Vaccination Programme-GOV.UK. Available online: https://www.gov.uk/government/publications/priority-groups-for-phase-2-of-the-coronavirus-covid-19-vaccination-programme-advice-from-the-jcvi/jcvi-interim-statement-on-phase-2-of-the-covid-19-vaccination-programme (accessed on 2 March 2021).
- Our World in Data Coronavirus (COVID-19) Vaccinations-Statistics and Research-Our World in Data. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 18 March 2021).
- Turkish Ministry of Health COVID-19 Information platform. Available online: https://covid19asi.saglik.gov.tr/ (accessed on 24 February 2021).
- Avorn, J.; Kesselheim, A. Regulatory decision-making on COVID-19 vaccines during a public health emergency. J. Am. Med. Assoc. 2020, 324, 1284–1285. [Google Scholar] [CrossRef]
- Trogen, B.; Oshinsky, D.; Caplan, A. Adverse consequences of rushing a SARS-CoV-2 vaccine: Implications for public trust. J. Am. Med. Assoc. 2020, 323, 2460–2461. [Google Scholar] [CrossRef]
- JCVI Joint Committee on Vaccination and Immunisation: Advice on Priority Groups for COVID-19 Vaccination, 30 December 2020-GOV.UK. Available online: https://www.gov.uk/government/publications/priority-groups-for-coronavirus-covid-19-vaccination-advice-from-the-jcvi-30-december-2020/joint-committee-on-vaccination-and-immunisation-advice-on-priority-groups-for-covid-19-vaccination-30-december-2020 (accessed on 2 March 2021).
- Portnoy, A.; Vaughan, K.; Clarke-Deelder, E.; Suharlim, C.; Resch, S.C.; Brenzel, L.; Menzies, N.A. Producing standardized country-level immunization delivery unit cost estimates. Pharmacoeconomics 2020, 38, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- Bollyky, T.J.; Gostin, L.O.; Hamburg, M.A. The equitable distribution of COVID-19 therapeutics and vaccines. J. Am. Med. Assoc. 2020, 323, 2462–2463. [Google Scholar] [CrossRef] [PubMed]
- Makhoul, M.; Ayoub, H.H.; Chemaitelly, H.; Seedat, S.; Mumtaz, G.R.; Al-Omari, S.; Abu-Raddad, L.J. Epidemiological impact of SARS-CoV-2 vaccination: Mathematical modeling analyses. Vaccines 2020, 8, 668. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Background Paper on Covid-19 Disease and Vaccines: Prepared by the Strategic Advisory Group of Experts (SAGE) on Immunization Working Group on COVID-19 Vaccines; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. Making Choices in Health: Who Guide to Cost-Effectiveness Analysis; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- World Bank Group GDP Per Capita (Current US$)-Turkey|Data. Available online: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?locations=TR (accessed on 24 February 2021).
- Prem, K.; Cook, A.R.; Jit, M. Projecting social contact matrices in 152 countries using contact surveys and demographic data. PLoS Comput. Biol. 2017, 13, e1005697. [Google Scholar] [CrossRef] [PubMed]
- Turkish Ministry of Health Sağlık Bilgi Sistemleri Genel Müdürlüğü. Available online: https://sbsgm.saglik.gov.tr/Eklenti/ (accessed on 1 September 2020).
- The Economist Covid-19 Data-Tracking Covid-19 Excess Deaths across Countries|Graphic Detail|The Economist. Available online: https://www.economist.com/graphic-detail/coronavirus-excess-deaths-tracker (accessed on 26 February 2021).
- Turkstat Death and Cause of Death Statistics. Available online: https://data.tuik.gov.tr/Bulten/Index?p=Olum-ve-Olum-Nedeni-Istatistikleri-2019-33710 (accessed on 12 April 2021).
- Levin, A.T.; Hanage, W.P.; Owusu-Boaitey, N.; Cochran, K.B.; Walsh, S.P.; Meyerowitz-Katz, G. Assessing the age specificity of infection fatality rates for COVID-19: Systematic review, meta-analysis, and public policy implications. Eur. J. Epidemiol. 2020, 35, 1123–1138. [Google Scholar] [CrossRef]
- Yetim, B.; Celik, Y. What predicts the quality of life in Turkey: The results of a country representative study. Health Soc. Care Community 2020, 28, 431–438. [Google Scholar] [CrossRef]
- Hacettepe Üniversitesi Aktüerya Bilimleri Bölümü Turkey Life Tables. Available online: http://www.aktuerya.hacettepe.edu.tr/TurkiyeHayatTablolari.php (accessed on 4 February 2021).
- Liu, Y.; Gayle, A.A.; Wilder-Smith, A.; Rocklöv, J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J. Travel Med. 2020, 27, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. Effectiveness of BNT162b2 mRNA Vaccine Against Infection and COVID-19 Vaccine Coverage in Healthcare Workers in England, Multicentre Prospective Cohort Study (the SIREN Study). SSRN Electron. J. 2021. [Google Scholar] [CrossRef]
- Raddad, L.J.A.; Chemaitelly, H.; Malek, J.A.; Ahmed Bsc, A.A.; Mohamoud, Y.A.; Younuskunju, S.; Ayoub, H.H.; Al Kanaani, Z.; Al Khal, A.; Al Kuwari, E.; et al. Assessment of the risk of SARS-CoV-2 reinfection in an intense re-exposure setting. MedRxiv 2020. [Google Scholar] [CrossRef]
- Bloomberg Turkey Finds Chinese Vaccine Efficacy Rate of 91.25% in Trial-Bloomberg. Available online: https://www.bloomberg.com/news/articles/2020-12-24/turkey-finds-chinese-vaccine-efficacy-rate-of-91-25-in-trial (accessed on 25 February 2021).
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Tukhvatulin, A.I.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2020, 384, 403–416. [Google Scholar] [CrossRef]
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020. [Google Scholar] [CrossRef]
- NICE COVID-19 Infecties op de Verpleegafdeling. Available online: https://www.stichting-nice.nl/covid-19-op-de-zkh.jsp (accessed on 12 October 2020).
- NICE Covid-19 op de IC. Available online: https://www.stichting-nice.nl/covid-19-op-de-ic.jsp (accessed on 12 October 2020).
- Koopmanschap, M.A.; Rutten, F.F.H. A practical guide for calculating indirect costs of disease. Pharmacoeconomics 1996, 10, 460–466. [Google Scholar] [CrossRef]
- Pike, J.; Grosse, S.D. Friction Cost estimates of productivity costs in cost-of-Illness studies in comparison with human capital estimates: A review. Appl. Health Econ. Health Policy 2018, 16, 765–778. [Google Scholar] [CrossRef] [PubMed]
- Turkish Official Gazette. Available online: https://www.resmigazete.gov.tr/eskiler/2020/04/20200404-18.pdf (accessed on 25 February 2021).
- Bosely, S. Belgian minister tweets EU’s Covid vaccine price list to anger of manufacturers. Guardian 2020. Available online: https://cde.news/belgian-minister-tweets-eus-covid-vaccine-price-list-to-anger-of-manufacturers/ (accessed on 19 December 2020).
- Terry, M. UPDATED Comparing COVID-19 Vaccines: Timelines, Types and Prices|BioSpace. Available online: https://www.biospace.com/article/comparing-covid-19-vaccines-pfizer-biontech-moderna-astrazeneca-oxford-j-and-j-russia-s-sputnik-v/ (accessed on 26 February 2021).
- Vynnycky, E.; White, R.G. An Introduction to Infectious Disease Modelling; Oxford University Press: New York, NY, USA, 2010. [Google Scholar]
- Kohli, M.; Maschio, M.; Becker, D.; Weinstein, M.C. The potential public health and economic value of a hypothetical COVID-19 vaccine in the United States: Use of cost-effectiveness modeling to inform vaccination prioritization. Vaccine 2021, 39, 1157–1164. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.; Jamieson, L.; Edoka, I.; Long, L.; Silal, S.; Pulliam, J.R.C.; Moultrie, H.; Sanne, I.; Meyer-Rath, G.; Nichols, B.E. Cost-effectiveness of remdesivir and dexamethasone for COVID-19 treatment in South Africa. Open Forum Infect. Dis. 2021, 8, ofab040. [Google Scholar] [CrossRef] [PubMed]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C.; et al. Antibody Persistence through 6 Months after the Second Dose of mRNA-1273 Vaccine for Covid-19. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- The Economist GitHub-TheEconomist/Covid-19-Excess-Deaths-Tracker: Source Code and Data for The Economist’s Covid-19 Excess Deaths Tracker. Available online: https://github.com/TheEconomist/covid-19-excess-deaths-tracker (accessed on 10 April 2021).
- Demiralp, S. The Economic Impact of COVID-19 on Turkey|Middle East Institute. Available online: https://www.mei.edu/publications/economic-impact-covid-19-turkey (accessed on 4 March 2021).
- World Bank Group Turkey|Data. Available online: http://data.worldbank.org/country/turkey (accessed on 31 January 2021).
- PopulationPyramid.net Population of Turkey 2019-PopulationPyramid.net. Available online: https://www.populationpyramid.net/turkey/2019/ (accessed on 30 January 2021).
- RIVM RIVM Data Catalogus. Available online: https://data.rivm.nl/geonetwork/srv/dut/catalog.search#/metadata/2c4357c8-76e4-4662-9574-1deb8a73f724 (accessed on 31 January 2021).
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Flasche, S.; Clifford, S.; Pearson, C.A.B.; Munday, J.D.; et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- Peirlinck, M.; Linka, K.; Sahli Costabal, F.; Kuhl, E. Outbreak dynamics of COVID-19 in China and the United States. Biomech. Model. Mechanobiol. 2020, 19, 2179–2193. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, M.B.; Karim, F.; Muscioni, G.; Augustine, A.S. Are we there yet? An adaptive SIR model for continuous estimation of COVID-19 infection rate and reproduction number in the United States. J. Med. Internet Res. 2020. [Google Scholar] [CrossRef]
- ECDC Questions and Answers on COVID-19: Basic Facts. Available online: https://www.ecdc.europa.eu/en/covid-19/facts/questions-answers-basic-facts (accessed on 31 January 2021).
- Turkey Statistical Institute (TURKSTAT). Available online: https://www.tuik.gov.tr/ (accessed on 30 January 2021).










| Compartment | Persons (n) | % |
|---|---|---|
| Susceptibles | 72,410,075 | 86.8% |
| Infectious and ill | 98,217 | 0.1% |
| Recovered (Immune) | 10,874,915 | 13.0% |
| Deaths | 46,409 | 0.1% |
| Total population | 83,429,615 | 100.0% |
| Main Scenario | Health Outcomes | Direct Costs | Indirect Costs | |||
|---|---|---|---|---|---|---|
| Deaths | QALYs Lost | Health Care | Vaccination | Sickness Leave | Premature Death | |
| Baseline without vaccination or imposed measures | 211,415 | 1,538,105 | 407,011,036 | - | 6,417,051,139 | 433,671,346 |
| Equal effectiveness on disease and transmission (90% effectiveness) | 3994 | 31,604 | 9,302,328 | 1,168,014,610 | 183,562,183 | 8,806,634 |
| Limited effectiveness on transmission (90% disease and 45% transmission effectiveness) | 88,865 | 645,570 | 171,275,569 | 1,168,014,610 | 2,676,371,116 | 182,019,930 |
| Incremental Health Outcomes | Incremental Direct Costs | Incremental Indirect Cost Savings | Total Incremental Cost Savings | ICERs | |||
|---|---|---|---|---|---|---|---|
| Scenario | Lives Saved | QALYs Gained | Health Perspective | Societal Perspective | |||
| Equal effectiveness on transmission and disease (90%) | 207,421 | 1,506,501 | 770,305,902 | 6,658,353,668 | 5,888,047,767 | 511 | Cost saving |
| Limited effectiveness on transmission (90% on disease and 45% on transmission) | 122,550 | 892,536 | 932,279,143 | 3,992,331,439 | 3,060,052,296 | 1045 | Cost saving |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hagens, A.; İnkaya, A.Ç.; Yildirak, K.; Sancar, M.; van der Schans, J.; Acar Sancar, A.; Ünal, S.; Postma, M.; Yeğenoğlu, S. COVID-19 Vaccination Scenarios: A Cost-Effectiveness Analysis for Turkey. Vaccines 2021, 9, 399. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9040399
Hagens A, İnkaya AÇ, Yildirak K, Sancar M, van der Schans J, Acar Sancar A, Ünal S, Postma M, Yeğenoğlu S. COVID-19 Vaccination Scenarios: A Cost-Effectiveness Analysis for Turkey. Vaccines. 2021; 9(4):399. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9040399
Chicago/Turabian StyleHagens, Arnold, Ahmet Çağkan İnkaya, Kasirga Yildirak, Mesut Sancar, Jurjen van der Schans, Aylin Acar Sancar, Serhat Ünal, Maarten Postma, and Selen Yeğenoğlu. 2021. "COVID-19 Vaccination Scenarios: A Cost-Effectiveness Analysis for Turkey" Vaccines 9, no. 4: 399. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9040399