
COVID-19 Vaccination Acceptance and Hesitancy among Healthcare Workers in Germany

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
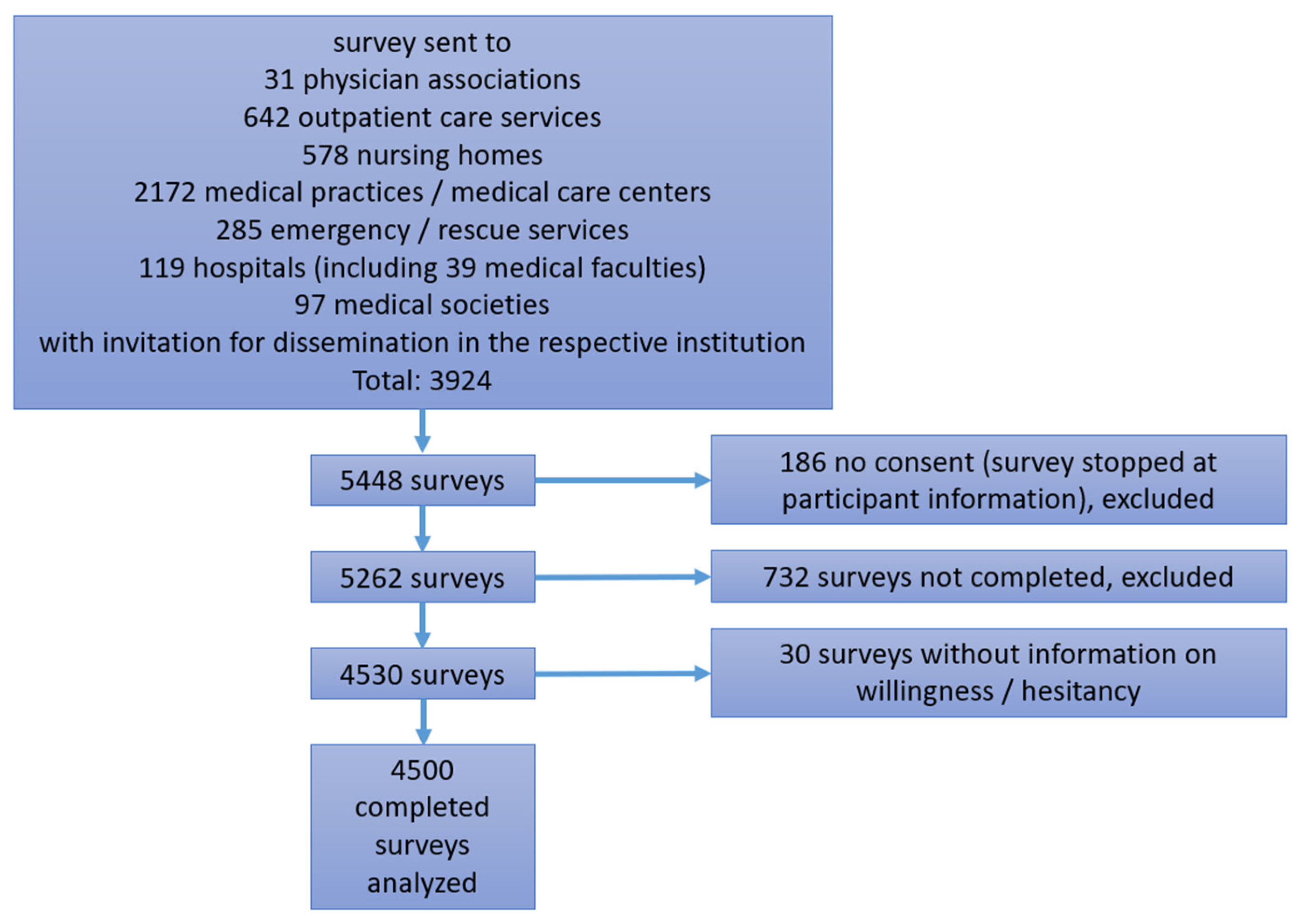
2.1. Study Setting and Participants
2.2. Study Size
2.3. Survey Instrument
2.4. Data Collection
2.5. Statistical Methods
2.6. Ethical Issues
3. Results
3.1. Study Population
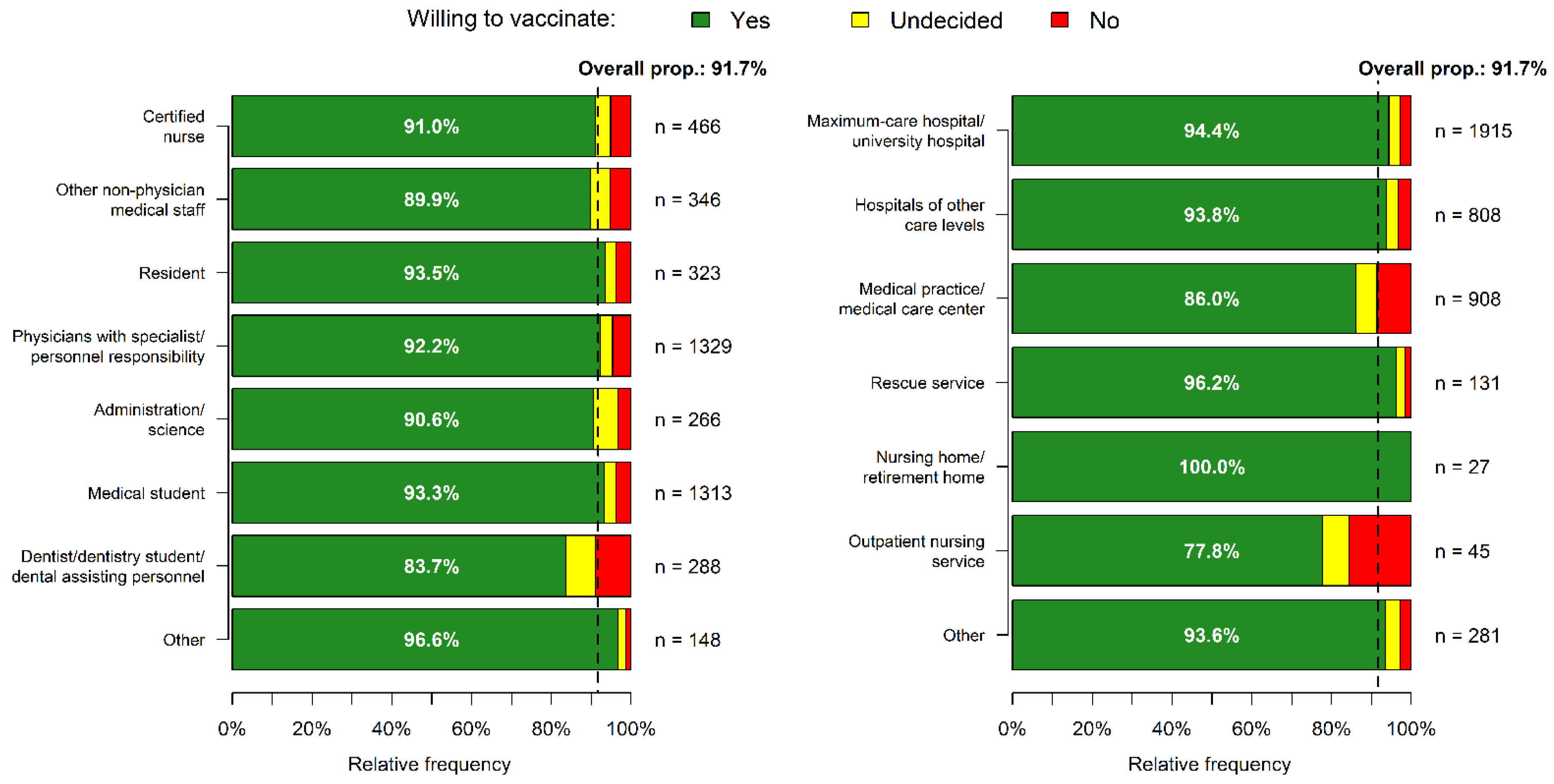
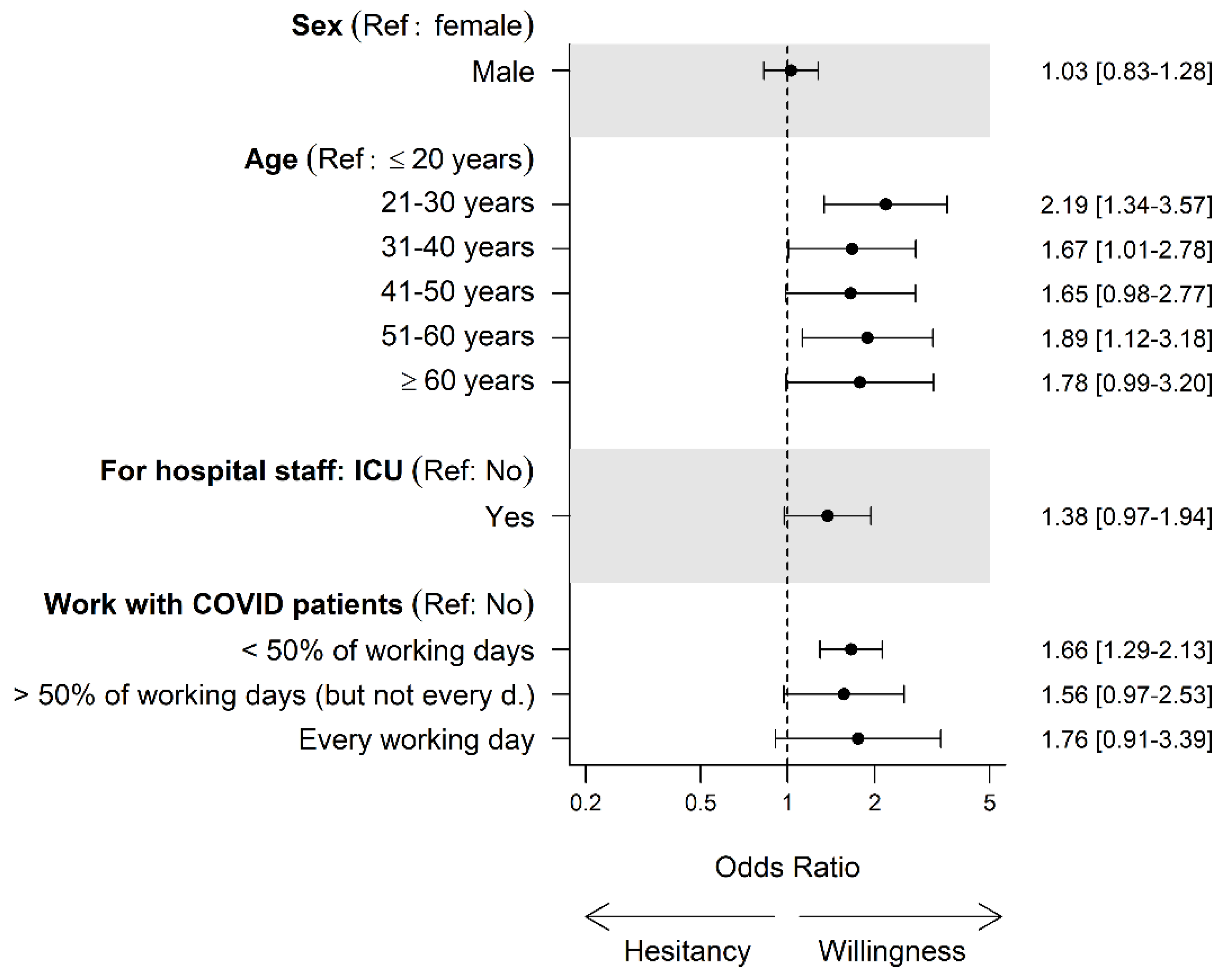
3.2. Vaccination Acceptance in Different Age Groups/Work Settings and Regions
3.3. Personal Attitudes and Vaccination Experience
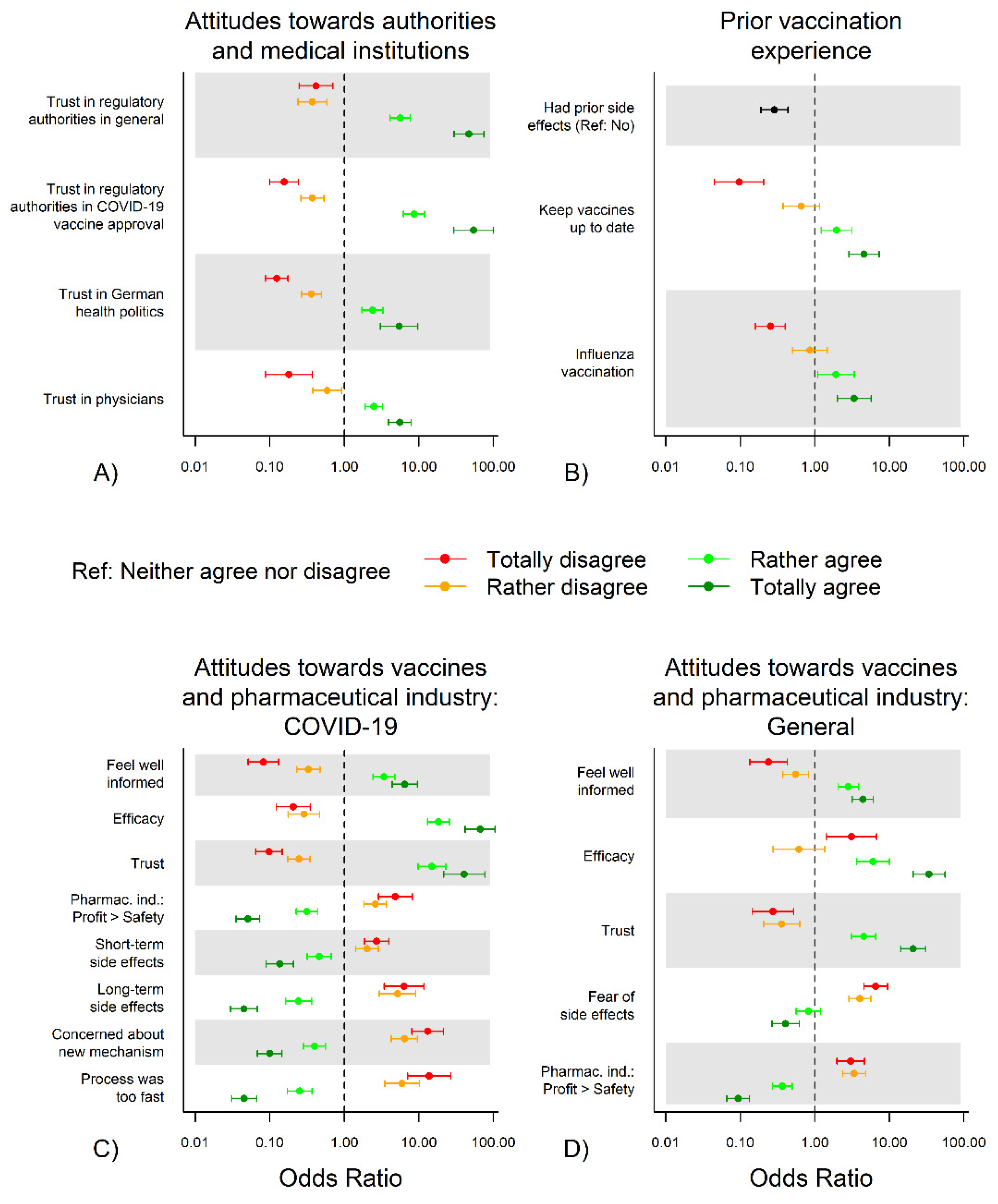
3.3.1. Attitudes towards Authorities and Medical Institutions and COVID-19 Vaccination Hesitancy
3.3.2. Prior Vaccination Experience and COVID-19 Vaccination Hesitancy
3.3.3. Attitudes to (COVID-19) Vaccines and Pharmaceutical Industry and COVID-19 Vaccination Hesitancy
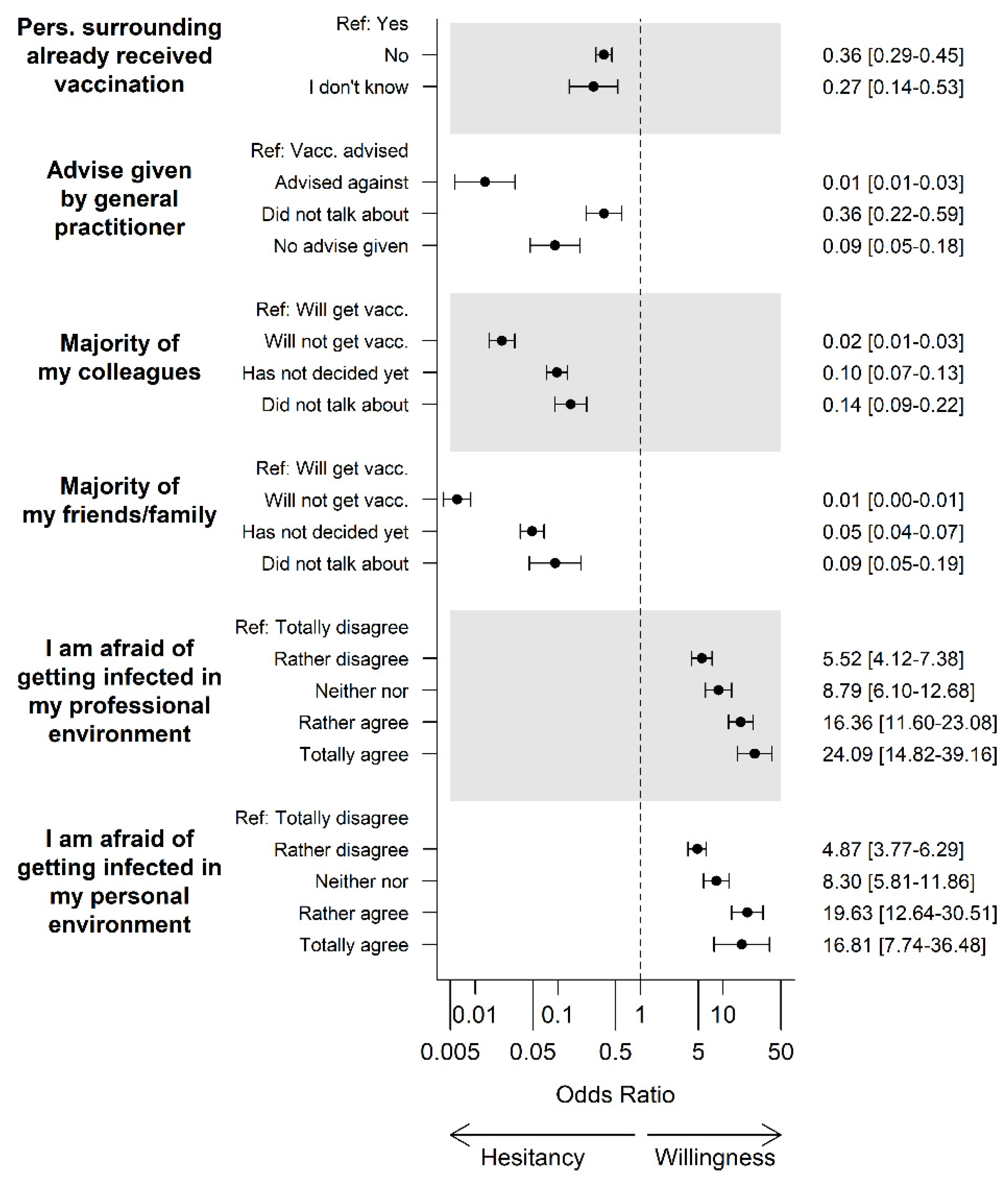
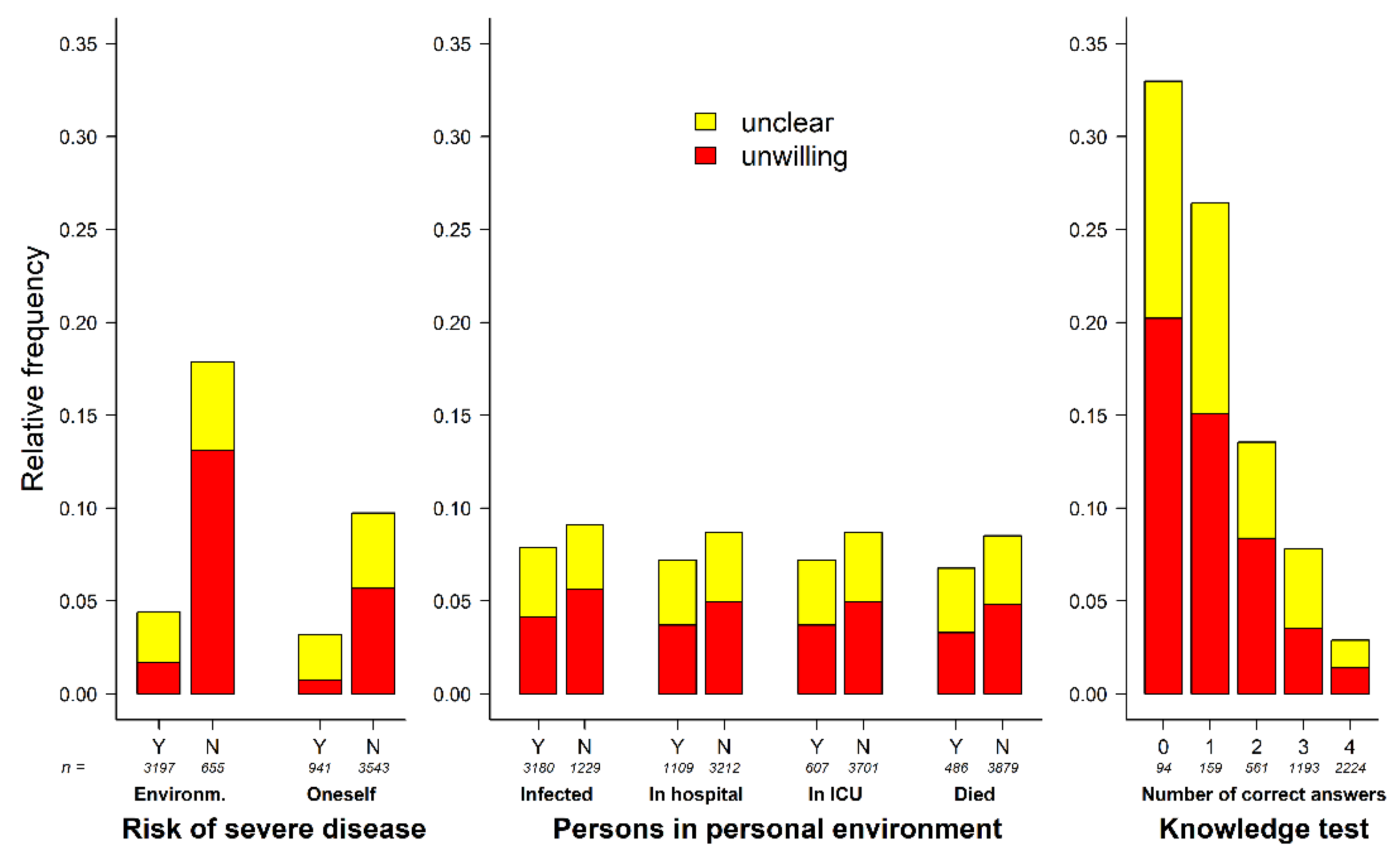
3.4. COVID-19-Specific Attitudes and Experiences in Personal Surroundings
3.5. Main Sources of Information on COVID-19
4. Discussion
4.1. Summary of Findings
4.2. Overall Acceptance
4.3. Comparison of Vaccine Hesitancy in the German Healthcare Workers and the General Population
4.4. Factors Associated with Vaccination Hesitancy
4.5. Possible Implications for COVID-19 Vaccination Campaigns
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Randolph, H.E.; Barreiro, L.B. Herd Immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Sivan, M.; Taylor, S. NICE guideline on long covid. BMJ 2020, 371, m4938. [Google Scholar] [CrossRef]
- Polyakova, M.; Kocks, G.; Udalova, V.; Finkelstein, A. Initial economic damage from the COVID-19 pandemic in the United States is more widespread across ages and geographies than initial mortality impacts. Proc. Natl. Acad. Sci. USA 2020, 117, 27934–27939. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, M.J. WHO’s Top Health Threats for 2019. JAMA 2019, 321, 1041. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J.; the SAGE Working Group on Vaccine Hesitancy. Strategies for addressing vaccine hesitancy—A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [PubMed]
- Wiysonge, C.S.; Ndwandwe, D.; Ryan, J.; Jaca, A.; Batoure, O.; Anya, B.M.; Cooper, S. Vaccine hesitancy in the era of COVID-19: Could lessons from the past help in divining the future? Hum. Vaccines Immunother. 2021, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Squeri, R.; Di Pietro, A.; La Fauci, V.; Genovese, C. Healthcare workers’ vaccination at European and Italian level: A narrative review. Acta Biomed. 2019, 90, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C. COSMO COVID-19 Snapshot Monitoring Zusammenfassung und Empfehlungen Welle 35. 2021. Available online: https://dfncloud.uni-erfurt.de/s/XZ5KJ29pGdPpAYw#pdfviewer (accessed on 26 March 2021).
- Robert-Koch-Institute. Täglicher Lagebericht des RKIzur Coronavirus-Krankheit-2019(COVID-19). Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Feb_2021/2021-02-27-de.pdf?__blob=publicationFile; https://www.rki.de/DE/Home/homepage_node.html (accessed on 28 May 2021).
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- COSMO COVID-19 Snapshot Monitoring. Fokuserhebungen: COVID-19 Impfung-Einstellungen und Impfabsicht. 2021. Available online: https://projekte.uni-erfurt.de/cosmo2020/web/topic/impfung/20-fokuserhebung/#gesundheitspersonal-60-und-chronisch-kranke (accessed on 26 March 2021).
- Karagiannidis, C.; Spies, C.; Kluge, S.; Marx, G.; Janssens, U. Willingness to vaccinate among intensive care personnel: Counteracting fears. Med. Klin. Intensivmed. Notf. 2021, 116, 216–219. [Google Scholar] [CrossRef]
- DIVI-Deutsche Interdisziplinäre Verienigung für Intensiv- und Notfallmedizin. Mehr als 75 Prozent Wollen Sich Gegen SARS-CoV-2 Impfen Lassen: Impfbereitschaft Unter Ärzten und Pflegekräften Gestiegen. 2021. Available online: https://www.divi.de/pressemeldungen-nach-themen/covid-19/mehr-als-75-prozent-wollen-sich-gegen-sars-cov-2-impfen-lassen-impfbereitschaft-unter-aerzten-und-pflegekraeften-gestiegen (accessed on 26 March 2021).
- American Nurses Foundation. December Pulse on the Nation’s Nurses COVID-19 Survey Series: COVID-19 Vaccine. 2020. Available online: https://www.nursingworld.org/practice-policy/work-environment/health-safety/disaster-preparedness/coronavirus/what-you-need-to-know/covid-19-vaccine-survey/ (accessed on 11 April 2021).
- Revive Health. Survey Findings Report: Physicians and Nurses on the COVID-19 Vaccine: Implications for Hospital Communicators. 2020. Available online: https://www.thinkrevivehealth.com/blog/public-trust-vaccine-depends-what-happens-inside-your-hospital (accessed on 11 April 2021).
- Di Gennaro, F.; Murri, R.; Segala, F.V.; Cerruti, L.; Abdulle, A.; Saracino, A.; Bavaro, D.F.; Fantoni, M. Attitudes towards Anti-SARS-CoV2 Vaccination among Healthcare Workers: Results from a National Survey in Italy. Viruses 2021, 13, 371. [Google Scholar] [CrossRef] [PubMed]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of healthcare workers towards COVID-19 vaccination: A survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef]
- Papagiannis, D.; Rachiotis, G.; Malli, F.; Papathanasiou, I.V.; Kotsiou, O.; Fradelos, E.C.; Giannakopoulos, K.; Gourgoulianis, K.I. Acceptability of COVID-19 Vaccination among Greek Health Professionals. Vaccines 2021, 9, 200. [Google Scholar] [CrossRef] [PubMed]
- Meyer, M.N.; Gjorgjieva, T.; Rosica, D. Healthcare worker intentions to receive a COVID-19 vaccine and reasons for hesitancy: A survey of 16,158 health system employees on the eve of vaccine distribution. medRxiv 2020. [Google Scholar] [CrossRef]
- Schrading, W.A.; Trent, S.A.; Paxton, J.H.; Rodriguez, R.M.; Swanson, M.B.; Mohr, N.M.; Talan, D.A. Vaccination Rates and Acceptance of SARS-CoV-2 Vaccination Among US Emergency Department Health Care Personnel. Acad. Emerg. Med. 2021. [Google Scholar] [CrossRef]
- Nohl, A.; Afflerbach, C.; Lurz, C.; Brune, B.; Ohmann, T.; Weichert, V.; Zeiger, S.; Dudda, M. Acceptance of COVID-19 Vaccination among Front-Line Health Care Workers: A Nationwide Survey of Emergency Medical Services Personnel from Germany. Vaccines 2021, 9, 424. [Google Scholar] [CrossRef]
- Dzieciolowska, S.; Hamel, D.; Gadio, S.; Dionne, M.; Gagnon, D.; Robitaille, L.; Cook, E.; Caron, I.; Talib, A.; Parkes, L.; et al. Covid-19 vaccine acceptance, hesitancy, and refusal among Canadian healthcare workers: A multicenter survey. Am. J. Infect. Control 2021. [Google Scholar] [CrossRef]
- Aloweidi, A.; Bsisu, I.; Suleiman, A.; Abu-Halaweh, S.; Almustafa, M.; Aqel, M.; Amro, A.; Radwan, N.; Assaf, D.; Abdullah, M.Z.; et al. Hesitancy towards COVID-19 Vaccines: An Analytical Cross–Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5111. [Google Scholar] [CrossRef]
- Butler, R.; MacDonald, N.E. Diagnosing the determinants of vaccine hesitancy in specific subgroups: The Guide to Tailoring Immunization Programmes (TIP). Vaccine 2015, 33, 4176–4179. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Meerpohl, J.J.; Voigt-Radloff, S.; Rueschemeyer, G.; Balzer, F.; Benstoem, C.; Binder, H.; Boeker, M.; Burns, J.; Dirnagl, U.; Featherstone, R.; et al. CEOsys: Creating an ecosystem for COVID-19 evidence. In Collaborating in Response to COVID-19: Editorial and Methods Initiatives across Cochrane; John Wiley & Sons, Ltd.: New York, NY, USA, 2020; Volume 12, pp. 9–11. [Google Scholar] [CrossRef]
- Stebbins, R.A. Exploratory Research in the Social Sciences; Sage: Southend Oaks, CA, USA, 2001; Volume 48. [Google Scholar]
- Döring, N.; Bortz, J. Forschungsmethoden und Evaluation; Springer: Wiesbaden, Germany, 2016. [Google Scholar]
- Deutsche Gesellschaft für Innere Medizin e.V. Die DGIM-Wer Sind Wir? Available online: https://www.dgim.de/ueber-uns/ (accessed on 28 June 2021).
- AWMF. Gesellschaft für Pädiatrische Gastroenterologie und Ernährung e.V. (GPGE). Available online: https://www.awmf.org/fachgesellschaften/mitgliedsgesellschaften/visitenkarte/fg/gesellschaft-fuer-paediatrische-gastroenterologie-und-ernaehrung-gpge.html (accessed on 28 June 2021).
- Leiner, D.J. SoSci Survey, 3.1.06. 2019. Available online: https://www.soscisurvey.de/de/about (accessed on 11 April 2021).
- Lenzner, T.; Menold, N. Question Wording (Version 2.0); (GESIS Survey Guidelines); GESIS-Leibniz-Institut für Sozialwissenschaften: Mannheim, Germany, 2016. [Google Scholar]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef]
- Larson, H.J.; De Figueiredo, A.; Xiahong, Z.; Schulz, W.S.; Verger, P.; Johnston, I.G.; Cook, A.R.; Jones, N.S. The state of vaccine confidence 2016: Global insights through a 67-country survey. EBioMedicine 2016, 12, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting Form data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef] [PubMed]
- Robert-Koch-Institut. COVID-19 Impfquoten-Monitoring in Deutschland (COVIMO)–2. Report. 2021. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Projekte_RKI/COVIMO_Reports/covimo_studie_bericht_2.pdf?__blob=publicationFile (accessed on 26 March 2021).
- Bundesamt, S. Bevölkerung-Anzahl der Einwohner in Den Bundesländern in Deutschland Am 31 Dezember. 2019. Available online: https://de.statista.com/statistik/daten/studie/71085/umfrage/verteilung-der-einwohnerzahl-nach-bundeslaendern/#professional (accessed on 27 May 2021).
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef]
- Robert-Koch-Institute. Epidemiologisches Bulletin Beschluss der STIKO zur 2. Aktualisierung der COVID-19-Impfempfehlung. 2021. Available online: https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2021/05/Art_01.html (accessed on 15 June 2021).
- Bouder, F.; Way, D.; Löfstedt, R.; Evensen, D. Transparency in Europe: A quantitative study. Risk Anal. 2015, 35, 1210–1229. [Google Scholar] [CrossRef]
- Betsch, C.; Wieler, L.H.; Habersaat, K. Monitoring behavioural insights related to COVID-19. Lancet 2020, 395, 1255–1256. [Google Scholar] [CrossRef]
- The Lancet, H. COVID-19 vaccines: Building and maintaining confidence. Lancet Haematol. 2021, 8, e305. [Google Scholar] [CrossRef]
- Neufeind, J.; Wenchel, R.; Boedeker, B.; Wicker, S.; Wichmann, O. Monitoring influenza vaccination coverage and acceptance among health-care workers in German hospitals—Results from three seasons. Hum. Vaccines Immunother. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- To, K.W.; Lai, A.; Lee, K.C.; Koh, D.; Lee, S.S. Increasing the coverage of influenza vaccination in healthcare workers: Review of challenges and solutions. J. Hosp. Infect. 2016, 94, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Sanci, L.; Webb, M.; Hocking, J. Risk-taking behaviour in adolescents. Aust. J. Gen. Pract. 2018, 47, 829–834. [Google Scholar] [CrossRef]
- Erber, J.; Kappler, V.; Haller, B.; Mijočević, H.; Galhoz, A.; da Costa, C.P.; Gebhardt, F.; Graf, N.; Hoffmann, D.; Thaler, M.; et al. Strategies for infection control and prevalence of anti-SARS-CoV-2 IgG in 4,554 employees of a university hospital in Munich, Germany. medRxiv 2020. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.; Ho, K.F.; Cheung, A.W.; Yau, P.S.; Dong, D.; Wong, S.Y.; Yeoh, E.K. Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys. Vaccines 2021, 9, 62. [Google Scholar] [CrossRef]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suk, J.; Celentano, L.P.; Kramarz, P.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef]
- Edwards, K.M.; Hackell, J.M. Countering Vaccine Hesitancy. Pediatrics 2016, 138. [Google Scholar] [CrossRef]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Hlatshwako, T.G.; Shah, S.J.; Kosana, P.; Adebayo, E.; Hendriks, J.; Larsson, E.C.; Hensel, D.J.; Erausquin, J.T.; Marks, M.; Michielsen, K.; et al. Online health survey research during COVID-19. Lancet Digit. Health 2021, 3, e76–e77. [Google Scholar] [CrossRef]
- Bethlehem, J. Selection bias in web surveys. Int. Stat. Rev. 2010, 78, 161–188. [Google Scholar] [CrossRef]
- European Commission. Europäische Kommission erteilt Dritte Zulassung für Sicheren und Wirksamen Impfstoff Gegen COVID-19. Available online: https://ec.europa.eu/commission/presscorner/detail/de/ip_21_306 (accessed on 15 June 2021).
- World Health Organization. COVAX Statement on WHO Emergency Use Listing for AstraZeneca/Oxford COVID-19 Vaccine. Available online: https://www.who.int/news/item/16-02-2021-covax-statement-on-who-emergency-use-listing-for-astrazeneca-oxford-covid-19-vaccine (accessed on 15 June 2021).
- U.S. Food & Drug Administration. Pfizer-BioNTech COVID-19 Vaccine. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/pfizer-biontech-covid-19-vaccine (accessed on 15 June 2021).
- European Commission. Union Register of Medicinal Products for Human Use. Available online: https://ec.europa.eu/health/documents/community-register/html/h1528.htm (accessed on 15 June 2021).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Total (n = 4500) | Undecided/Dismissive (n = 375) | Willing (n = 4125) | p |
|---|---|---|---|---|
| Sex | ||||
| Female | 2610 (58.0) | 218 (8.4) | 2392 (91.6) | 0.801 |
| Male | 1879 (41.8) | 153 (8.1) | 1726 (91.9) | |
| No answer | 11 (0.2) | |||
| Age | ||||
| ≤20 years | 156 (3.5) | 22 (14.1) | 134 (85.9) | 0.039 |
| 21–30 years | 1603 (35.6) | 112 (7.0) | 1491 (93.0) | |
| 31–40 years | 872 (19.4) | 78 (8.9) | 794 (91.1) | |
| 41–50 years | 730 (16.2) | 66 (9.0) | 664 (91.0) | |
| 51–60 years | 776 (17.2) | 62 (8.0) | 714 (92.0) | |
| ≥61 years | 355 (7.9) | 30 (8.5) | 325 (91.5) | |
| No answer | 8 (0.2) | |||
| Professional groups | ||||
| Certified nurse | 466 (10.4) | 42 (9.0) | 424 (91.0) | <0.001 |
| Other non-physician medical staff | 346 (7.7) | 35 (10.1) | 311 (89.9) | |
| Resident | 323 (7.2) | 21 (6.5) | 302 (93.5) | |
| Physicians with specialist/personnel responsibility | 1329 (29.5) | 104 (7.8) | 1225 (92.2) | |
| Administration/science | 266 (5.9) | 25 (9.4) | 241 (90.6) | |
| Medical student | 1313 (29.2) | 88 (6.7) | 1225 (93.3) | |
| Dentist/dentistry student/dental assisting personnel | 288 (6.4) | 47 (16.3) | 241 (83.7) | |
| Other | 148 (3.3) | 5 (3.4) | 143 (96.6) | |
| No answer | 21 (0.5) | |||
| Work setting | ||||
| Maximum-care hospital/university hospital | 1838 (40.8) | 102 (5.5) | 1736 (94.5) | <0.001 |
| Hospitals of other care levels | 792 (17.6) | 47 (5.9) | 745 (94.1) | |
| Medical practice/medical care center | 771 (17.1) | 107 (13.9) | 664 (86.1) | |
| Rescue service | 128 (2.8) | 5 (3.9) | 123 (96.1) | |
| Nursing home/retirement home | 26 (0.6) | 0 (0.0) | 26 (100.0) | |
| Outpatient nursing service | 34 (0.8) | 10 (29.4) | 24 (70.6) | |
| Other | 526 (11.7) | 47 (8.9) | 479 (91.1) | |
| No answer | 385 (8.6) | |||
| Hospital, intensive care unit yes | 1105 (24.6) | 52 (4.7) | 1053 (95.3) | 0.070 |
| Hospital, intensive care unit no | 1525 (33.9) | 97 (6.4) | 1428 (93.6) | |
| Region | ||||
| Northern Germany | 1266 (28.1) | 134 (10.6) | 1132 (89.4) | 0.001 |
| Southern Germany | 1582 (35.2) | 107 (6.8) | 1475 (93.2) | |
| Eastern Germany | 380 (8.2) | 36 (9.5) | 344 (90.5) | |
| Western Germany | 1168 (26.0) | 85 (7.3) | 1083 (92.7) | |
| No answer | 104 (2.3) | |||
| COVID-19 patient care | ||||
| Never | 1729 (38.4) | 170 (9.8) | 1559 (90.2) | <0.001 |
| <50% of working days | 1815 (40.3) | 112 (6.2) | 1703 (93.8) | |
| >50% of working days (but not every working day) | 307 (6.8) | 20 (6.5) | 287 (93.5) | |
| On each working day | 171 (3.8) | 10 (5.8) | 161 (94.2) | |
| No answer | 478 (10.6) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holzmann-Littig, C.; Braunisch, M.C.; Kranke, P.; Popp, M.; Seeber, C.; Fichtner, F.; Littig, B.; Carbajo-Lozoya, J.; Allwang, C.; Frank, T.; et al. COVID-19 Vaccination Acceptance and Hesitancy among Healthcare Workers in Germany. Vaccines 2021, 9, 777. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070777
Holzmann-Littig C, Braunisch MC, Kranke P, Popp M, Seeber C, Fichtner F, Littig B, Carbajo-Lozoya J, Allwang C, Frank T, et al. COVID-19 Vaccination Acceptance and Hesitancy among Healthcare Workers in Germany. Vaccines. 2021; 9(7):777. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070777
Chicago/Turabian StyleHolzmann-Littig, Christopher, Matthias Christoph Braunisch, Peter Kranke, Maria Popp, Christian Seeber, Falk Fichtner, Bianca Littig, Javier Carbajo-Lozoya, Christine Allwang, Tamara Frank, and et al. 2021. "COVID-19 Vaccination Acceptance and Hesitancy among Healthcare Workers in Germany" Vaccines 9, no. 7: 777. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070777