
Timely Birth Dose Vaccine to Prevent Vertical Transmission of Hepatitis B: A Single Center Experience on the Road to the WHO Elimination Goals in Italy

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
- -
- Mothers’ age, country of origin, parity, and mode of birth;
- -
- maternal HBsAg status at birth (assessed by biochemical luminescence microparticle immunoassay, CMIA);
- -
- the laboratory data included HBV DNA level during pregnancy and other serologic markers of HBV maternal infection (e.g., HBcAb total, HBcIgM, HBeAg, HBeAb), when available;
- -
- the maternal HIV and HCV co-infection status;
- -
- the newborns’ gender, birth weight, gestational age at birth, and feeding method.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Weinbaum, C.M.; Williams, I.; Mast, E.E.; Wang, S.A.; Finelli, L.; Wasley, A.; Neitzel, S.M.; Ward, J.W. Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm. Rep. 2008, 57, 1–20. [Google Scholar] [CrossRef]
- Schillie, S.; Vellozzi, C.; Reingold, A.; Harris, A.; Haber, P.; Ward, J.W.; Nelson, N.P. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm. Rep. 2018, 67, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S.; Bzowej, N.H.; Wong, J.B. Update on Prevention, Diagnosis, and Treatment of Chronic Hepatitis B: AASLD 2018 Hepatitis B Guidance. Clin. Liver Dis. 2018, 12, 33–34. [Google Scholar] [CrossRef] [PubMed]
- LEGGE 27 maggio 1991, n. 165 Obbligatorieta’ della Vaccinazione Contro L’epatite Virale B. (GU Serie Generale n.127 del 01-06-1991). Available online: https://www.gazzettaufficiale.it/eli/id/1991/06/01/091G0201/sg#:~:text=note%3A%20Entrata%20in%20vigore%20della%20legge%3A%2016%2F6%2F1991&text=1.-,1.,nel%20primo%20anno%20di%20vita (accessed on 24 January 2021).
- Linea Guida Gravidanza Fisiologica. Sistema Nazionale per le linee Guida Istituto Superiore di Sanità (SNLG-ISS), Aggiornamento. 2011. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_1436_allegato.pdf (accessed on 24 January 2021).
- Piano Nazionale Prevenzione Vaccinale PNPV 2017-2019. G.U. Serie Generale, n. 41 del 18 Febbraio 2017. Available online: https://www.gazzettaufficiale.it/eli/gu/2017/02/18/41/sg/pdf (accessed on 24 January 2021).
- Campagna, M.; Siddu, A.; Meloni, A.; Murru, C.; Masia, G.; Coppola, R.C. Epidemiological impact of mandatory vaccination against hepatitis B in Italian young adults. Hepat. Mon. 2011, 11, 750–752. [Google Scholar] [CrossRef]
- Sistema Epidemiologico Integrato dell’Epatite Virale Acuta (SEIEVA). Istituto Superiore di Sanità. Bollettino Annuale 2019. Available online: http://www.iss.it/seieva (accessed on 24 March 2020).
- 2015 Assessment Report of the Global Vaccine Action Plan; World Health Organization: Geneva, Switzerland, 2015. Available online: https://www.who.int/immunization/sage/meetings/2015/october/2_ARORA__GVAP_Assessment_recommendations_SAGE_Oct_2015_Final.pdf (accessed on 24 January 2021).
- Boccalini, S.; Taddei, C.; Ceccherini, V.; Bechini, A.; Levi, M.; Bartolozzi, D.; Bonanni, P. Economic analysis of the first 20 years of universal hepatitis B vaccination program in Italy: An a posteriori evaluation and forecast of future benefits. Hum. Vaccines Immunother. 2013, 9, 1119–1128. [Google Scholar] [CrossRef] [Green Version]
- Lai, A.; Sagnelli, C.; Presti, A.L.; Cella, E.; Angeletti, S.; Spoto, S.; Costantino, S.; Sagnelli, E.; Ciccozzi, M. What is changed in HBV molecular epidemiology in Italy? J. Med. Virol. 2018, 90, 786–795. [Google Scholar] [CrossRef] [Green Version]
- Prevention of Mother-to-Child Transmission of Hepatitis B Virus: Guidelines on Antiviral Prophylaxis in Pregnancy; World Health Organization: Geneva, Switzerland, 2020. Available online: https://www.who.int/publications/i/item/978-92-4-000270-8 (accessed on 9 January 2021).
- Cornberg, M. Annex C: Hepatitis B Birth dose Investment Case. GAVI. 2018. Available online: https://www.gavi.org/sites/default/files/document/ppc-meeting-18-19-october-2018---vis-06a---annex-c--hepatitis-b-birth-dose-investment-casepdf.pdf (accessed on 9 January 2021).
- Goldstein, S.T.; Zhou, F.; Hadler, S.C.; Bell, B.P.; Mast, E.E.; Margolis, H.S. A mathematical model to estimate global hepatitis B disease burden and vaccination impact. Int. J. Epidemiol. 2005, 34, 1329–1339. [Google Scholar] [CrossRef] [Green Version]
- de Villiers, M.J.; Gamkrelidze, I.; Hallett, T.B.; Nayagam, S.; Razavi, H.; Razavi-Shearer, D. Modelling hepatitis B virus infection and impact of timely birth dose vaccine: A comparison of two simulation models. PLoS ONE 2020, 15, e0237525. [Google Scholar] [CrossRef] [PubMed]
- Global Hepatitis Report; World Health Organization: Geneva, Switzerland, 2017. Available online: http://apps.who.int/iris/bitstream/10665/255016/1/9789241565455-eng.pdf?ua=1 (accessed on 5 January 2021).
- Wong, V.C.; Ip, H.M.; Reesink, H.W.; Lelie, P.N.; Reerink-Brongers, E.E.; Yeung, C.Y.; Ma, H.K. Prevention of the HBsAg carrier state in newborn infants of mothers who are chronic carriers of HBsAg and HBeAg by administration of hepatitis-B vaccine and hepatitis-B immunoglobulin. Double-blind randomised placebo-controlled study. Lancet 1984, 1, 921–926. [Google Scholar] [CrossRef]
- Lo, K.J.; Tsai, Y.T.; Lee, S.D.; Wu, T.C.; Wang, J.Y.; Chen, G.H.; Yeh, C.L.; Chiang, B.N.; Yeh, S.H.; Goudeau, A. Immunoprophylaxis of infection with hepatitis B virus in infants born to hepatitis B surface antigen-positive carrier mothers. J. Infect. Dis. 1985, 152, 817–822. [Google Scholar] [CrossRef]
- Beasley, R.P. Rocks along the road to the control of HBV and HCC. Ann. Epidemiol. 2009, 19, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Indolfi, G.; Easterbrook, P.; Dusheiko, G.; Siberry, G.; Chang, M.H.; Thorne, C.; Bulterys, M.; Chan, P.L.; El-Sayed, M.H.; Giaquinto, C.; et al. Hepatitis B virus infection in children and adolescents. Lancet Gastroenterol. Hepatol. 2019, 4, 466–476. [Google Scholar] [CrossRef]
- Guidelines for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection; World Health Organization: Geneva, Switzerland, 2015. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK305553/ (accessed on 23 January 2021).
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrault, N.A.; Bzowej, N.H.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Murad, M.H.; Diseases, A.A. AASLD guidelines for treatment of chronic hepatitis B. Hepatology 2016, 63, 261–283. [Google Scholar] [CrossRef]
- Jourdain, G.; Ngo-Giang-Huong, N.; Harrison, L.; Decker, L.; Khamduang, W.; Tierney, C.; Salvadori, N.; Cressey, T.R.; Sirirungsi, W.; Achalapong, J.; et al. Tenofovir versus Placebo to Prevent Perinatal Transmission of Hepatitis B. N. Engl. J. Med. 2018, 378, 911–923. [Google Scholar] [CrossRef] [PubMed]
- Willis, B.C.; Wortley, P.; Wang, S.A.; Jacques-Carroll, L.; Zhang, F. Gaps in hospital policies and practices to prevent perinatal transmission of hepatitis B virus. Pediatrics 2010, 125, 704–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harder, K.M.; Cowan, S.; Eriksen, M.B.; Krarup, H.B.; Christensen, P.B. Universal screening for hepatitis B among pregnant women led to 96% vaccination coverage among newborns of HBsAg positive mothers in Denmark. Vaccine 2011, 29, 9303–9307. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Jia, Z.F.; Wu, X.; Wen, S.M.; Kong, F.; Hu, K.Q.; Li, J.; Jiang, J.; Niu, J.Q. Protective effect of an improved immunization practice of mother-to-infant transmission of hepatitis B virus and risk factors associated with immunoprophylaxis failure. Medicine 2016, 95, e4390. [Google Scholar] [CrossRef]
- Kang, W.; Ding, Z.; Shen, L.; Zhao, Z.; Huang, G.; Zhang, J.; Xiong, Q.; Zhang, S.; Wang, F. Risk factors associated with immunoprophylaxis failure against mother to child transmission of hepatitis B virus and hepatitis B vaccination status in Yunnan province, China. Vaccine 2014, 32, 3362–3366. [Google Scholar] [CrossRef]
- Komatsu, H. Hepatitis B virus: Where do we stand and what is the next step for eradication? World J. Gastroenterol. 2014, 20, 8998–9016. [Google Scholar]
- Soeung, S.C.; Thiep, C.; Duncan, R.; Patel, M.; Hennessey, K. Using data to guide policy: Next steps for preventing perinatal hepatitis B virus transmission in Cambodia. Vaccine 2012, 31, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Luman, E.T.; Barker, L.E.; McCauley, M.M.; Drews-Botsch, C. Timeliness of childhood immunizations: A state-specific analysis. Am. J. Public Health 2005, 95, 1367–1374. [Google Scholar] [CrossRef] [PubMed]
- Kushner, T.; Kaplowitz, E.; Mei, R.; Xu, C.; Acker, A.; Rosenbluth, E.; Oredein, I.; Sarkar, M.; Terrault, N.; Bansa, M.; et al. Adherence to pregnancy hepatitis B care guidelines in women and infants in the U.S. and evaluation of two interventions to improve care: A multi-center hospital-based study. J. Viral Hepat. 2021, 28, 582–591. [Google Scholar] [CrossRef]
- Fasano, M.; Saracino, A.; Carosi, G.; Mazzotta, F.; Marino, N.; Sagnelli, E.; Gaeta, G.B.; Angarano, G.; Verucchi, G.; Bellissima, P.; et al. Hepatitis B and immigrants: A SIMIT multicenter cross-sectional study. Infection 2013, 41, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Sagnelli, E.; Sagnelli, C.; Pisaturo, M.; Macera, M.; Coppola, N. Epidemiology of acute and chronic hepatitis B and delta over the last 5 decades in Italy. World J. Gastroenterol. 2014, 20, 7635–7643. [Google Scholar] [CrossRef]
- Coppola, N.; Alessio, L.; Gualdieri, L.; Pisaturo, M.; Sagnelli, C.; Minichini, C.; Di Caprio, G.; Starace, M.; Onorato, L.; Signoriello, G.; et al. Hepatitis B virus infection in undocumented immigrants and refugees in Southern Italy: Demographic, virological, and clinical features. Infect. Dis. Poverty 2017, 6, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Alert and Response. Hepatitis B. Prevention and Treatment; World Health Organization: Geneva, Switzerland, 2002. Available online: http://www.who.int/csr/disease/hepatitis/whocdscsrlyo20022/en/index5.html (accessed on 24 January 2021).
- Mele, A.; Tancredi, F.; Romanò, L.; Giuseppone, A.; Colucci, M.; Sangiuolo, A.; Lecce, R.; Adamo, B.; Tosti, M.E.; Taliani, G.; et al. Effectiveness of hepatitis B vaccination in babies born to hepatitis B surface antigen-positive mothers in Italy. J. Infect. Dis. 2001, 184, 905–908. [Google Scholar] [CrossRef]
- Calvo, P.L.; Pinon, M.; Dell’Olio, D.; Carpino, A.; Biasin, E.; Pizzol, A.; Catalano, S.; Peruzzi, L.; Rigazio, C.; Cisarò, F.; et al. Management of Hepatitis-B Virus Infection in Immunocompromised Children. A Single Center Experience. J. Pediatr. Gastroenterol. Nutr. 2020, 72, 597–602. [Google Scholar] [CrossRef]
- Indolfi, G.; Abdel-Hady, M.; Bansal, S.; Debray, D.; Smets, F.; Czubkowski, P.; van der Woerd, W.; Samyn, M.; Jahnel, J.; Gupte, G.; et al. Management of Hepatitis B Virus Infection and Prevention of Hepatitis B Virus Reactivation in Children With Acquired Immunodeficiencies or Undergoing Immune Suppressive, Cytotoxic, or Biological Modifier Therapies. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Ghany, M.G.; Morgan, T.R. Hepatitis C Guidance 2019 Update: American Association for the study of the Liver Diseases-Infectious Disease Society of American recommendations for Testing, Managing and Treating Hepatitis C Virus Infection. AASLD/IDSA Hepat. C Guid. Panel Hepatol. 2020, 71, 10–1002. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | Italian Origin N (%) | Foreign Origin N (%) | Total N (%) |
|---|---|---|---|
| Mothers’ Age | |||
| <25 years | 0 | 15 (7) | 15 (6) |
| 25–35 years | 13 (42) | 138 (68) | 151 (64) |
| >35 years | 18 (58) | 51 (25) | 69 (30) |
| Parity | |||
| Primiparous | 13 (42) | 74 (36) | 87 (37) |
| Multiparous | 18 (58) | 130 (64) | 148 (63) |
| Mode of Birth | |||
| Natural birth | 24 (77) | 134 (66) | 158 (67) |
| Scheduled Cesarean | 3 (10) | 38 (18) | 41 (18) |
| Urgent Cesarean | 4 (13) | 32 (16) | 36 (15) |
| Gestational Age at Birth | |||
| <37 weeks | 4 (13) | 15 (7) | 19 (8) |
| ≥37 weeks | 27 (87) | 189 (93) | 216 (92) |
| Markers of Active Viral Replication (HBV DNAand/or HBeAg) | |||
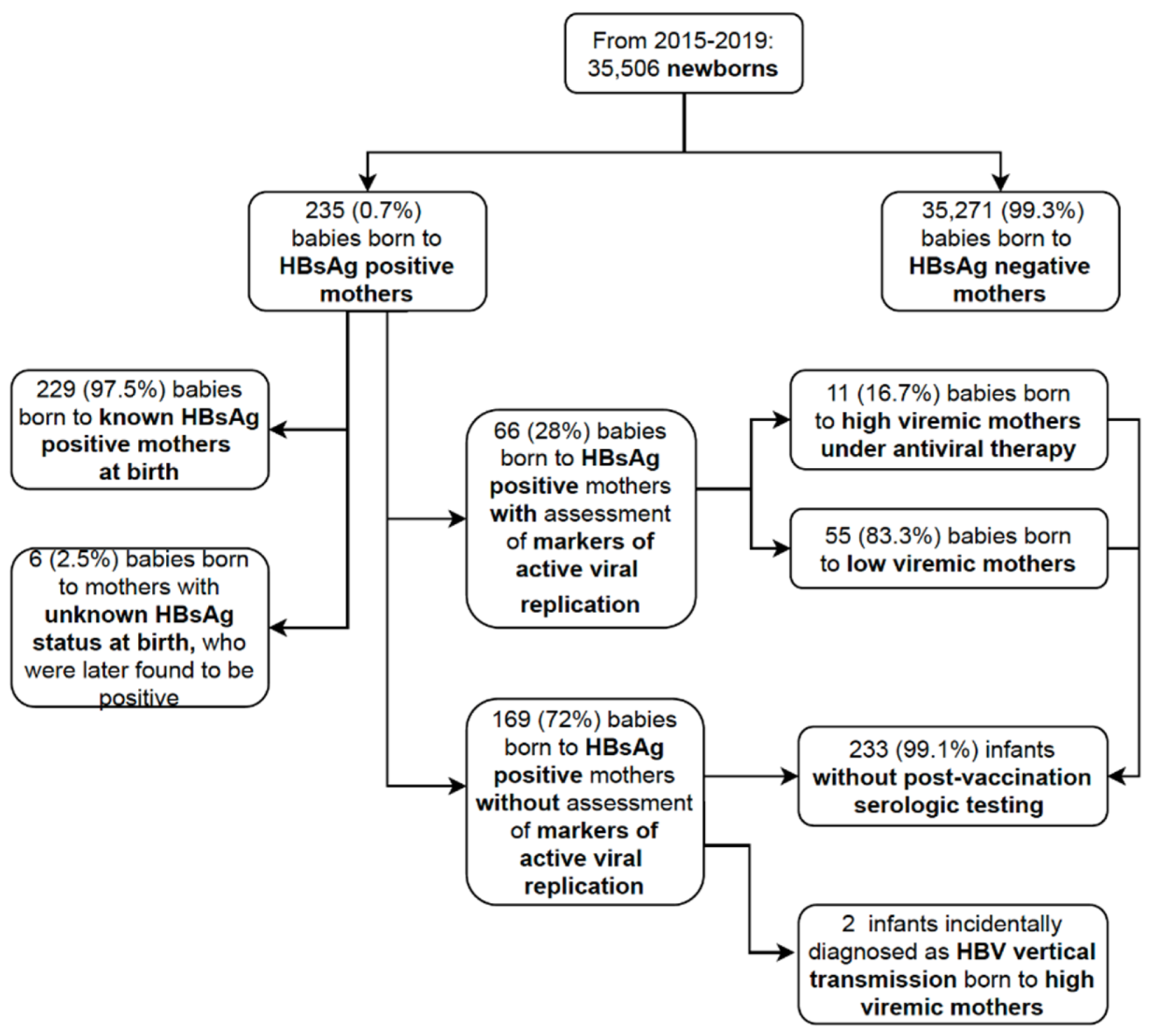
| Reported in medical records | 12 (39) | 54 (26) | 66 (28) |
| Not reported in medical records | 19 (61) | 150 (74) | 169 (72) |
| High viremic women | 3 (25) | 8 (15) | 11 (17) |
| Low viremic women | 9 (75) | 46 (85) | 55 (83) |
| HBV DNA levels (IU/mL) in high viremic women; median (range) | 200,001 (200,001–143,000,000) | 785,000 (350,000–170,000.000) | 460,573 (200,001–170,000,000) |
| Median HBV DNA levels (IU/mL) in low viremic women; median (range) | 28 (<20–6000) | 22 (<20–22,228) | 22 (<20–22,228) |
| Newborns’ Gender | |||
| Male | 15 (48) | 109 (53) | 124 (53) |
| Female | 16 (52) | 95 (47) | 111 (47) |
| Birth Weight | |||
| <2.5 Kg | 4 (13) | 16 (8) | 20 (9) |
| ≥2.5 Kg | 27 (87) | 188 (92) | 215 (91) |
| Feeding Method | |||
| Breastfeeding | 20 (65) | 107 (52) | 127 (54) |
| Bottle feeding | 1 (3) | 48 (24) | 49 (21) |
| Mixed feeding | 10 (32) | 49 (24) | 59 (25) |
| Day of the Week for Birth | |||
| On a weekday | 21 (68) | 156 (76) | 177 (75) |
| At weekends | 10 (32) | 48 (24) | 58 (25) |
| Birth Time | |||
| Day-time | 11 (35) | 83 (41) | 94 (40) |
| Night-time | 20 (65) | 121 (59) | 141 (60) |
| Late Immunoprophylaxis Proportion (%) | OR (95% CI) | p-Value | |
|---|---|---|---|
| Mothers’ Age | |||
| <25 years | 1/15 (7) | 1 (ref) | - |
| 25–35 years | 35/151 (23) | 4.34 (0.55–34.17) | 0.16 |
| >35 years | 10/69 (14) | 2.99 (0.35–25.04) | 0.31 |
| Country of Origin | |||
| Italy | 7/31 (23) | 1 (ref) | |
| Foreign country | 42/204 (21) | 0.89 (0.36–2.20) | 0.80 |
| Parity | |||
| Primiparous | 29/87 (33) | 1 (ref) | |
| Multiparous | 20/148 (14) | 0.43 (0.27–0.83) | 0.01 * |
| Gestational Age at Birth | |||
| <37 weeks | 4/19 (21) | 1 (ref) | |
| >37 weeks | 45/216 (21) | 0.99 (0.31–3.12) | 0.98 |
| Markers of Active Viral Replication (HBV DNAand/or HBeAg) | |||
| Not reported in medical records | 41/169 (24) | 1 (ref) | |
| Reported in medical records | 16/66 (24) | 0.93 (0.46–1.89) | 0.84 |
| Mode of Birth | |||
| Scheduled Cesarean | 9/41 (22) | 1 (ref) | |
| Natural birth | 31/158 (20) | 0.87 (0.38–2.00) | 0.74 |
| Urgent Cesarean | 9/36 (25) | 1.18 (0.41–3.41) | 0.75 |
| Newborns’ Gender | |||
| Female | 18/111 (16) | 1 (ref) | |
| Male | 31/124 (25) | 1.72 (0.9–3.29) | 0.10 |
| Birth Weight | |||
| <2500 g | 6/20 (30) | 1 (ref) | |
| >2500 g | 43/215 (20) | 0.72 (0.24–2.1) | 0.54 |
| Feeding Method | |||
| Bottle feeding | 6/49 (12) | 1 (ref) | |
| Breastfeeding | 28/127 (22) | 1.73 (0.70–4.28) | 0.46 |
| Mixed feeding | 15/59 (25) | 1.95 (0.72–5.31) | 0.51 |
| Day of the Week for Birth | |||
| On a weekday | 36/177 (20) | 1 (ref) | |
| At weekends | 13/58 (22) | 1.13 (0.55–2.32) | 0.37 |
| Birth Time | |||
| Day-time | 13/94 (14) | 1 (ref) | |
| Night-time | 36/141 (26) | 2.13 (1.06–4.29) | 0.03 * |
| Case 1 | Case 2 | |
|---|---|---|
| Post-partum maternal viral load | >170,000,000 UI/mL | >170,000,000 UI/mL |
| Maternal antiviral prophylaxis | no | no |
| Immunoprophylaxis (HBV vaccine + HIBG) at birth | <6 h from birth | <6 h from birth |
| Scheduled vaccination | regular | regular |
| Age at diagnosis | 12 months | 18 months |
| Child HBV DNA (IU/mL) | >170,000,000 | >170,000,000 |
| Child HBsAg (s/co) | + | + |
| Child HBeAg (s/co) | + | + |
| Child HBsAb (UI/mL) | <10 | <10 |
| Child HBcAb (s/co) | + | + |
| Child AST/ALT (UI/mL) | 140/158 | 65/80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinon, M.; Giugliano, L.; Nicastro, E.; Kakaa, O.; Coscia, A.; Carbonara, C.; D’Antiga, L.; Calvo, P.L. Timely Birth Dose Vaccine to Prevent Vertical Transmission of Hepatitis B: A Single Center Experience on the Road to the WHO Elimination Goals in Italy. Vaccines 2021, 9, 801. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070801
Pinon M, Giugliano L, Nicastro E, Kakaa O, Coscia A, Carbonara C, D’Antiga L, Calvo PL. Timely Birth Dose Vaccine to Prevent Vertical Transmission of Hepatitis B: A Single Center Experience on the Road to the WHO Elimination Goals in Italy. Vaccines. 2021; 9(7):801. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070801
Chicago/Turabian StylePinon, Michele, Laura Giugliano, Emanuele Nicastro, Omar Kakaa, Alessandra Coscia, Caterina Carbonara, Lorenzo D’Antiga, and Pier Luigi Calvo. 2021. "Timely Birth Dose Vaccine to Prevent Vertical Transmission of Hepatitis B: A Single Center Experience on the Road to the WHO Elimination Goals in Italy" Vaccines 9, no. 7: 801. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070801