
A Review of the Implementation Status of and National Plans on HPV Vaccination in 17 Middle-Income Countries of the WHO Western Pacific Region


Abstract
:1. Introduction
2. Materials and Methods
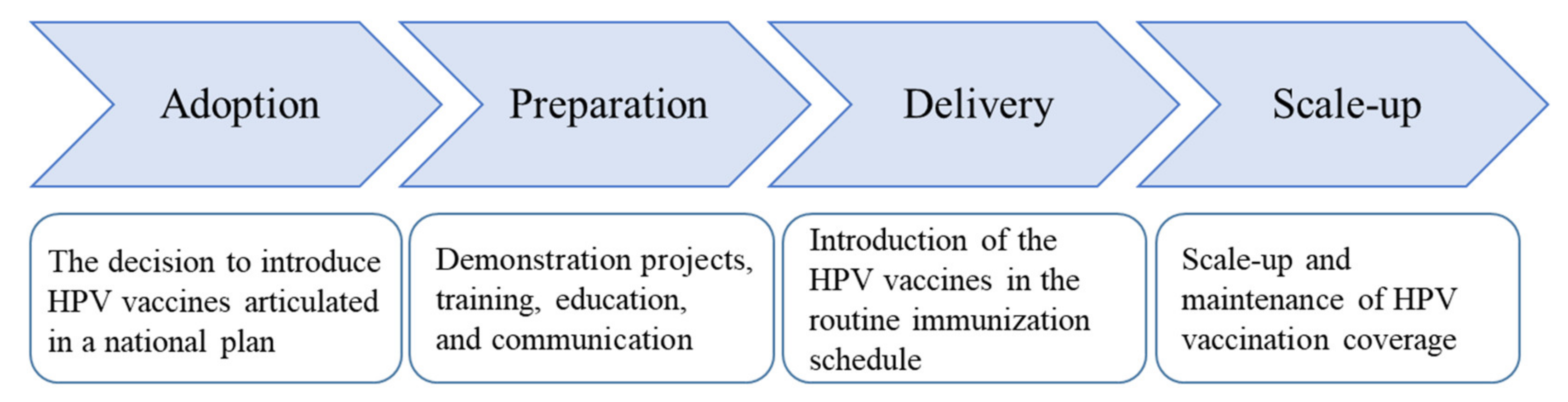
2.1. Conceptual Framework
2.2. Data Sources
2.2.1. Cervical Cancer Burden
2.2.2. Cervical Cancer Screening Practice
2.2.3. HPV Vaccination Demonstration Projects and National Programs
2.2.4. National Plans
2.3. Review of the National Plans
2.4. Data Synthesis
3. Results
3.1. Cervical Cancer Burden
3.2. Cervical Cancer Screening Practice
3.3. Implementation Status of HPV Vaccination
3.4. National Plans on HPV Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects 2019. Available online: https://population.un.org/wpp/Download/Standard/Population/ (accessed on 31 August 2021).
- World Health Organization. Countries. Available online: https://www.who.int/countries (accessed on 31 August 2021).
- World Bank. New Country Classifications by Income Level: 2021–2022. Available online: https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2021-2022 (accessed on 31 August 2021).
- Ferlay, J.E.M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F.; Global Cancer Observatory: Cancer Today. International Agency for Research on Cancer: Lyon, France. Available online: https://gco.iarc.fr/today (accessed on 31 August 2021).
- World Health Organization. Global Health Estimates 2019: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2019. 2020. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death (accessed on 31 August 2021).
- Schiffman, M.; Castle, P.E.; Jeronimo, J.; Rodriguez, A.C.; Wacholder, S. Human papillomavirus and cervical cancer. Lancet 2007, 370, 890–907. [Google Scholar] [CrossRef]
- World Health Organization. Global Strategy to Accelerate the Eliminate Cervical Cancer as a Public Health Problem. 2020. Available online: https://www.who.int/publications/i/ (accessed on 31 August 2021).
- Brisson, M.; Kim, J.J.; Canfell, K.; Drolet, M.; Gingras, G.; Burger, E.A.; Martin, D.; Simms, K.T.; Bénard, É.; Boily, M.-C.; et al. Impact of HPV vaccination and cervical screening on cervical cancer elimination: A comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet 2020, 395, 575–590. [Google Scholar] [CrossRef] [Green Version]
- Simms, K.T.; Steinberg, J.; Caruana, M.; Smith, M.A.; Lew, J.-B.; Soerjomataram, I.; Castle, P.E.; Bray, F.; Canfell, K. Impact of scaled up human papillomavirus vaccination and cervical screening and the potential for global elimination of cervical cancer in 181 countries, 2020–99: A modelling study. Lancet Oncol. 2019, 20, 394–407. [Google Scholar] [CrossRef]
- Bruni, L.; Saura-Lázaro, A.; Montoliu, A.; Brotons, M.; Alemany, L.; Diallo, M.S.; Afsar, O.Z.; LaMontagne, D.S.; Mosina, L.; Contreras, M.; et al. HPV vaccination introduction worldwide and WHO and UNICEF estimates of national HPV immunization coverage 2010–2019. Prev. Med. 2021, 144, 106399. [Google Scholar] [CrossRef]
- World Health Organization. The Global Health Observatory. Available online: https://www.who.int/data/gho (accessed on 31 August 2021).
- UNAIDS. HIV Estimates with Uncertainty Bounds 1990–2020. 2021. Available online: https://www.unaids.org/en/resources/documents/2021/HIV_estimates_with_uncertainty_bounds_1990-present (accessed on 31 August 2021).
- World Health Organization. WHO Vaccine-Preventable Diseases: Monitoring System. 2020 Global Summary. Available online: https://apps.who.int/immunization_monitoring/globalsummary/ (accessed on 31 August 2021).
- Sodha, S.V.; Dietz, V. Strengthening routine immunization systems to improve global vaccination coverage. Br. Med. Bull. 2015, 113, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Murillo, R.; Robles, C. Research Needs for Implementing Cancer Prevention and Early Detection in Developing Countries: From Scientists’ to Implementers’ Perspectives. BioMed Res. Int. 2019, 2019, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Aarons, G.A.; Hurlburt, M.; Horwitz, S.M. Advancing a Conceptual Model of Evidence-Based Practice Implementation in Public Service Sectors. Adm. Policy Ment. Health Ment. Health Serv. Res. 2010, 38, 4–23. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Report on Cancer: Setting Priorities, Investing Wisely and Providing Care for All. 2020. Available online: https://apps.who.int/iris/handle/10665/330745 (accessed on 31 August 2021).
- Hanson, C.M.; Eckert, L.; Bloem, P.; Cernuschi, T. Gavi HPV Programs: Application to Implementation. Vaccines 2015, 3, 408–419. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, K.E.; Howard, N.; Kabakama, S.; Mounier-Jack, S.; Griffiths, U.K.; Feletto, M.; Burchett, H.; Lamontagne, D.S.; Watson-Jones, D. Lessons learnt from human papillomavirus (HPV) vaccination in 45 low- and middle-income countries. PLoS ONE 2017, 12, e0177773. [Google Scholar] [CrossRef] [Green Version]
- Ferlay, J.L.M.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F.; Global Cancer Observatory: Cancer Tomorrow. International Agency for Research on Cancer: Lyon, France, 2020. Available online: https://gco.iarc.fr/tomorrow (accessed on 31 August 2021).
- United Nations Children’s Fund. WHO/UNICEF Human Papillomavirus (HPV) Immunization Coverage Estimates. 2021. Available online: https://data.unicef.org/resources/dataset/immunization/ (accessed on 31 August 2021).
- Romero, Y.; Trapani, D.; Johnson, S.; Tittenbrun, Z.; Given, L.; Hohman, K.; Stevens, L.; Torode, J.S.; Boniol, M.; Ilbawi, A.M. National cancer control plans: A global analysis. Lancet Oncol. 2018, 19, e546–e555. [Google Scholar] [CrossRef]
- World Health Organization. WHO-UNICEF Guidelines for Comprehensive Multi-Year Planning for Immunization. 2014. Available online: https://apps.who.int/iris/bitstream/handle/10665/100618/WHO_IVB_14.01_eng.pdf?sequence=1 (accessed on 31 August 2021).
- World Health Organization. Noncommunicable Disease Document Repository. Available online: https://extranet.who.int/ncdccs/documents/Db (accessed on 31 August 2021).
- International Cancer Control Partnership. ICCP Portal—the One-Stopshop Online Resource for Cancer Planners. Available online: https://www.iccp-portal.org (accessed on 31 August 2021).
- Gavi, the Vaccine Alliance. County hub. Available online: https://www.gavi.org/programmes-impact/country-hub (accessed on 31 August 2021).
- Tervonen, H.; Foliaki, S.; Bray, F.; Roder, D. Cancer epidemiology in the small nations of Pacific Islands. Cancer Epidemiol. 2017, 50, 184–192. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Control Program, Department of Health and Social Affairs. Comprehensive Cancer Control Plan 2019–2024; National Comprehensive Cancer Control Program, Department of Health and Social Affairs: Palikir, Micronesia, 2019. [Google Scholar]
- Ministry of Health and Human Services. National Comprehensive Cancer Control Plan 2017–2022; Ministry of Health and Human Services: Majuro, Micronesia, 2017.
- Ministry of Health. National Strategic Plan for Cancer Control Programme 2016–2020; Ministry of Health: Putrajaya, Malaysia, 2016.
- Ministry of Health and Medical Services. Cervical Cancer Screening Policy; Ministry of Health and Medical Services: Suva, Fiji, 2015.
- La Vincente, S.F.; Mielnik, D.; Jenkins, K.; Bingwor, F.; Volavola, L.; Marshall, H.; Druavesi, P.; Russell, F.M.; Lokuge, K.; Mulholland, E.K. Implementation of a national school-based Human Papillomavirus (HPV) vaccine campaign in Fiji: Knowledge, vaccine acceptability and information needs of parents. BMC Public Health 2015, 15, 1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philippines Department of Health. Guidelines in the Implementation of HPV Vaccination (DM 2015-0316). 2015. Available online: https://doh.gov.ph/philippine-cancer-control-program (accessed on 31 August 2021).
- Philippines, Department of Health. National Immunization Program. Manual of Operations. Booklet 1. 2016. Available online: https://doh.gov.ph/sites/default/files/publications/NIP-MOP-Booklet%201.pdf (accessed on 31 August 2021).
- Jhpiego. Igniting Change in the Landscape of Health Care for Women and Families. 2016. Available online: https://www.jhpiego.org/wp-content/uploads/2017/03/Jhpiego-40-Greatest-Hits.pdf (accessed on 31 August 2021).
- Solomon Islands. Comprehensive Multi-Year Plan for Immunization, 2016–2020. Available online: https://www.gavi.org/sites/default/files/document/2021/cMYP%20Solomon%20Islands%202016-2020.pdf (accessed on 29 September 2021).
- United States Agency for International Development. National Immunization Programme Updated Comprehensive Multi-year Plan 2019–2023; United States Agency for International Development: Washington, DC, USA, 2018. [Google Scholar]
- Xiamen Municipal Health Commission. Notice on the Implementation Plan of Domestic Bivalent HPV Vaccination in Xiamen; Xiamen Municipal Health Commission: Xiamen, China, 2020. (In Chinese) [Google Scholar]
- Office of the People’s Government of Ordos City, China. Notice of the Office of the People’s Government of Ordos City on Issuing the Implementation Plan of the Two-Cancer Prevention and Control Project. 2020. Available online: http://www.ordos.gov.cn/ordosml/ordoszf/202012/t20201228_2827928.html (accessed on 31 August 2021). (In Chinese)
- Lamontagne, D.S.; Barge, S.; Le, N.T.; Mugisha, E.; Penny, M.E.; Gandhi, S.; Janmohamed, A.; Kumakech, E.; Mosqueira, N.R.; Nguyen, N.Q.; et al. Human papillomavirus vaccine delivery strategies that achieved high coverage in low- and middle-income countries. Bull. World Health Organ. 2011, 89, 821–830. [Google Scholar] [CrossRef]
- Garon, J.; Wuddhika, I.V.; Sreenivasan, N.; Wannemuehler, K.; Vutthikol, Y.; Chhorvann, C.; Loharikar, A. Community-based household assessment of human papillomavirus (HPV) vaccination coverage and acceptability—HPV vaccine demonstration program, Cambodia—2017. Vaccine 2019, 37, 1202–1208. [Google Scholar] [CrossRef]
- Ladner, J.; Besson, M.-H.; Hampshire, R.; Tapert, L.; Chirenje, M.; Saba, J. Assessment of eight HPV vaccination programs implemented in lowest income countries. BMC Public Health 2012, 12, 370. [Google Scholar] [CrossRef] [Green Version]
- Ladner, J.; Besson, M.-H.; Rodrigues, M.; Audureau, E.; Saba, J. Performance of 21 HPV vaccination programs implemented in low and middle-income countries, 2009–2013. BMC Public Health 2014, 14, 670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batmunkh, T.; von Mollendorf, C.; Tulgaa, K.; Surenjav, U.; Dalmau, M.T.; Namjil, N.; Tsedevdamba, B.; Tsegmed, S.; Enkhmaa, J.; Garland, S.M.; et al. HPV genoprevalence and HPV knowledge in young women in Mongolia, five years following a pilot 4vHPV vaccination campaign. Papillomavirus Res. 2019, 8, 100175. [Google Scholar] [CrossRef]
- Waramin, E.N.P.; Toka, D.; Mola, G.; Amos, L.; Stinshoff, J.V.; Bagita, M. HPV Vaccination Pilot Program in Papua New Guinea. 2017. Available online: https://psrh.org.nz/wp-content/uploads/2017/09/HPV-Vaccination-pilot-in-PNG-Mary-Bagita-.pdf (accessed on 31 August 2021).
- Harry, T.J. Cervical Cancer Care & HPV Vaccination and Screening in Vanuatu. 2017. Available online: https://psrh.org.nz/wp-content/uploads/2017/09/Cervical-Cancer-Care-HPV-Vaccinaon-and-screening-In-Vanuatu-Margaret-McAdam-and-Tony-Harry.pdf (accessed on 31 August 2021).
- Muhamad, N.A.; Buang, S.N.; Jaafar, S.; Jais, R.; Tan, P.S.; Mustapha, N.; Lodz, N.A.; Aris, T.; Sulaiman, L.H.; Murad, S. Achieving high uptake of human papillomavirus vaccination in Malaysia through school-based vaccination programme. BMC Public Health 2018, 18, 1402. [Google Scholar] [CrossRef]
- Ministry of Health. National Immunisation Policy and Procedure Manual 2013–2016; Ministry of Health: Suvo, Fiji, 2013.
- Heffelfinger, J. HPV Vaccination in the Western Pacific and South-East Asia Regions: Overview, Challenges and Opportunities. 2018. Available online: https://www.sabin.org/sites/sabin.org/files/james_heffelfinger.pdf (accessed on 31 August 2021).
- Zhao, F.; Qiao, Y. Cervical cancer prevention in China: A key to cancer control. Lancet 2019, 393, 969–970. [Google Scholar] [CrossRef]
- Government of Federated States of Micronesia. National Strategic Plan of Action for the Prevention and Control of Non-Communicable Diseases in the Federated States of Micronesia 2019–2024; Government of Federated States of Micronesia: Palikir, Micronesia, 2019.
- Ministry of Health. NCD Emergency Response Towards a Healthy RMI Action Plan 2013–2018; Ministry of Health: Majuro, Micronesia, 2013.
- Ministry of Health. Medium Term Strategic Plan to Further Strengthen the NCD Prevention and Control Program in Malaysia (2016–2025); Ministry of Health: Putrajaya, Malaysia, 2016.
- Ministry of Health and Medical Services. Non-Communicable Diseases Strategic Plan 2015–2019; Ministry of Health and Medical Services: Suva, Fiji, 2015.
- Department of Health. Philippine Strategic Plan for the Prevention and Control Of Noncommunicable Diseases 2017–2025; Department of Health: Manila, Philiphines, 2017.
- Philippines Department of Health. National Cancer Prevention and Control Action Plan 2015–2020. Available online: https://doh.gov.ph/philippine-cancer-control-program (accessed on 31 August 2021).
- Ministry of Health and Medical Services. Multi-Sectoral National Non-communicable Disease Strategic Plan 2019–2023; Ministry of Health and Medical Services: Honiara, Solomon Islands, 2019.
- Ministry of Health. National Multisectoral Action Plan for the Prevention and Control of Noncommunicable Diseases 2014–2020; Ministry of Health: Vientiane, Laos, 2014.
- National Health Commission. Healthy China Action Cancer Control Implementation Plan 2019–2022; National Health Commision: Beijing, China, 2019. (In Chinese) [Google Scholar]
- Office of the State Council. Long-Term Plan for the Prevention and Treatment of Chronic Diseases (2017–2025); Office of the State Council: Beijing, China, 2017. (In Chinese) [Google Scholar]
- Ministry of Health. National Strategy on Prevention and Control of Cancer, Cardiovascular Diseases, Diabetes, Chronic Obstructive Pulmonary Diseases, Asthma and Other NCDs Period 2015–2025; Ministry of Health: Hanoi, Vietnam, 2015.
- Ministry of Health. National Action Plan for Prevention and Control of Cervical Cancer 2016–2025; Ministry of Health: Hanoi, Vietnam, 2016. (In Vietnamese)
- Ministry of Health. Comprehensive Multi-Year Plan for Extended Program on Immunization 2016–2020; Ministry of Health: Hanoi, Vietnam, 2016.
- Ministry of Health. National Immunization Program Strategic Plan 2016–2020; Ministry of Health: Phnom Penh, Cambodia, 2016.
- Ministry of Health. National Multisectoral Action Plan for the Prevention and Control of Noncommunicable Diseases 2018–2027; Ministry of Health: Phnom Penh, Cambodia, 2018.
- Ministry of Health. National Action Plan for Cervical Cancer Prevention and Control 2019–2023; Ministry of Health: Phnom Penh, Cambodia, 2019.
- Ministry of Health. Sub-Program on Cancer Prevention and Control 2015–2020; Ministry of Health: Ulaanbaatar, Mongolia, 2015.
- Ministry of Health. National Program on NCD Control; Ministry of Health: Ulaanbaatar, Mongolia, 2017.
- Ministry of Health. United Nations Joint Global Program to Reduce Cervical Cancer Morbidity and Mortality in Mongolia in 2018–2021; Ministry of Health: Ulaanbaatar, Mongolia, 2018. (In Mongolian)
- Ministry of Health. National Infectious Disease Prevention and Control Program 2017–2021; Ministry of Health: Ulaanbaatar, Mongolia, 2017. (In Mongolian)
- National Department of Health. National Multisetoral Strategic Plan for the Prevention and Control of NonCommunicable Diseases 2015–2020; National Department of Health: Port Moresby, Papua New Guinea, 2015.
- National Department of Health. Comprehensive Epi Multi-Year Plan For National Immunization Programme 2016–2020; National Department of Health: Port Moresby, Papua New Guinea, 2016.
- National Department of Health. Cancer Action Priorities for 2017–2021; National Department of Health: Port Moresby, Papua New Guinea, 2017.
- Ministry of Health. Non-communicable Disease Policy and Strategic Plan 2016–2020; Ministry of Health: Port Vila, Vanuatu, 2016.
- Ministry of Health & Medical Services. Comprehensive Multi-Year Plan for Immunization & Nutrition 2019–2023; Ministry of Health & Medical Services: Tarawa, Kiribati, 2019.
- Ministry of Health. National Noncommunicable Disease Control Policy 2018–2023; Ministry of Health: Apia, Samoa, 2018.
- Ministry of Health. National Strategy for Prevention and Control of Non-Communicable Diseases 2015–2020; Ministry of Health: Nuku’alofa, Tonga, 2015.
- Ministry of Health. National Noncommunicable Diseases Strategic Plan 2017–2021; Ministry of Health: Funafuti, Tuvalu, 2017.
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjosé, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, K.; LaMontagne, D.; Watson-Jones, D. Status of HPV vaccine introduction and barriers to country uptake. Vaccine 2018, 36, 4761–4767. [Google Scholar] [CrossRef]
- Tsu, V.D.; LaMontagne, D.S.; Atuhebwe, P.; Bloem, P.N.; Ndiaye, C. National implementation of HPV vaccination programs in low-resource countries: Lessons, challenges, and future prospects. Prev. Med. 2021, 144, 106335. [Google Scholar] [CrossRef]
- Kumar, S.; Khanduri, A.; Sidibe, A.; Morgan, C.; Torode, J.; Basu, P.; Bhatla, N.; Schocken, C.; Bloem, P. Acting on the call: A framework for action for rapid acceleration of access to the HPV vaccination in low-and lower-middle-income countries. Int. J. Gynecol. Obstet. 2021, 152, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Toh, Z.Q.; Russell, F.M.; Garland, S.M.; Mulholland, E.K.; Patton, G.; Licciardi, P.V. Human Papillomavirus Vaccination After COVID-19. JNCI Cancer Spectr. 2021, 5, pkab011. [Google Scholar] [CrossRef]
- World Health Organization. Guide to Introducing HPV Vaccine into National Immunization Programmes. 2016. Available online: https://apps.who.int/iris/bitstream/handle/10665/253123/9789241549769-eng.pdf?sequence=1&isAllowed=y (accessed on 31 August 2021).
- Hindin, M.J.; Bloem, P.; Ferguson, J. Effective Nonvaccine Interventions to Be Considered Alongside Human Papilloma Virus Vaccine Delivery. J. Adolesc. Health 2015, 56, 10–18. [Google Scholar] [CrossRef]
- Broutet, N.; Lehnertz, N.; Mehl, G.; Camacho, A.V.; Bloem, P.; Chandra-Mouli, V.; Ferguson, J.; Dick, B. Effective Health Interventions for Adolescents That Could Be Integrated with Human Papillomavirus Vaccination Programs. J. Adolesc. Health 2013, 53, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Buang, S.N.; Ja’Afar, S.; Pathmanathan, I.; Saint, V. Human papillomavirus immunisation of adolescent girls: Improving coverage through multisectoral collaboration in Malaysia. BMJ 2018, 363, k4602. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Market Study: HPV Vaccines. 2020. Available online: https://www.who.int/immunization/programmes_systems/procurement/mi4a/platform/module2/HPV_Global_Market_Study_Public_Summary-Nov2020.pdf?ua=1 (accessed on 31 August 2021).
- World Health Organization. Vaccine Pricing: Gavi Fully Self-financing & Accelerated Transition Countries. 2018. Available online: https://www.who.int/immunization/programmes_systems/procurement/mi4a/platform/module2/Factsheet_vacc_pricing_Gavi_transitioning.pdf (accessed on 31 August 2021).
- Van Minh, H.; My, N.T.T.; Jit, M. Cervical cancer treatment costs and cost-effectiveness analysis of human papillomavirus vaccination in Vietnam: A PRIME modeling study. BMC Health Serv. Res. 2017, 17, 353. [Google Scholar] [CrossRef] [Green Version]
- UNICEF Supply Division. Vaccines Pricing Data. 2021. Available online: https://www.unicef.org/supply/vaccines-pricing-data (accessed on 31 August 2021).
- World Health Organization. Prequalification of Medical Products (IVDs, Medicines, Vaccines and Immunization Devices, Vector Control). Cecolin®. Available online: https://extranet.who.int/pqweb/content/cecolin%C2%AE (accessed on 6 November 2021).
- Vänskä, S.; Luostarinen, T.; Baussano, I.; Apter, D.; Eriksson, T.; Natunen, K.; Nieminen, P.; Paavonen, J.; Pimenoff, V.N.; Pukkala, E.; et al. Vaccination with Moderate Coverage Eradicates Oncogenic Human Papillomaviruses If a Gender-Neutral Strategy Is Applied. J. Infect. Dis. 2020, 222, 948–956. [Google Scholar] [CrossRef] [Green Version]
- Obel, J.; McKenzie, J.; Buenconsejo-Lum, L.; Durand, A.; Ekeroma, A.; Souares, Y.; Hoy, D.; Baravilala, W.; Garland, S.; Kjaer, S.; et al. Mapping HPV Vaccination and Cervical Cancer Screening Practice in the Pacific Region-Strengthening National and Regional Cervical Cancer Prevention. Asian Pac. J. Cancer Prev. 2015, 16, 3435–3442. [Google Scholar] [CrossRef] [Green Version]
- Sankaranarayanan, R.; Basu, P.; Kaur, P.; Bhaskar, R.; Singh, G.B.; Denzongpa, P.; Grover, R.K.; Sebastian, P.; Saikia, T.; Oswal, K.; et al. Current status of human papillomavirus vaccination in India’s cervical cancer prevention efforts. Lancet Oncol. 2019, 20, e637–e644. [Google Scholar] [CrossRef]
- Black, E.; Richmond, R. Prevention of Cervical Cancer in Sub-Saharan Africa: The Advantages and Challenges of HPV Vaccination. Vaccines 2018, 6, 61. [Google Scholar] [CrossRef] [Green Version]
- Piñeros, M.; Saraiya, M.; Baussano, I.; Bonjour, M.; Chao, A.; Bray, F. The role and utility of population-based cancer registries in cervical cancer surveillance and control. Prev. Med. 2021, 144, 106237. [Google Scholar] [CrossRef]


{kind=link}
| Socioeconomic Indicators | Health Indicators | Immunization Indicators [13] | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Income Classification (2021) [3] | Total Female Population (2020) [1] | Total Number of Girls Aged 9–14 Years (2020) [1] | Female Life Expectancy at Birth (Years, 2019) [11] | Total Fertility Rate (Births per Women, 2015–2020) [1] | Prevalence of Current Tobacco Use in Women (%, 2018) [11] | Prevalence of HIV in Women Aged 15–49 Years (%, 2020) [12] | Estimated DTP3 Coverage (%, 2019) | Availability of a National System to Monitor AEFI (2019) | % of Immunization Expenditure Financed Using Government Funds (%, 2016–2019) | ||
| Asian countries | China | UM | 701,076,000 | 46,907,000 | 80.5 | 1.7 | 2.1 | - | 99 | Yes | 100 |
| Philippines | LM | 54,552,000 | 6,366,000 | 73.6 | 2.6 | 6.5 | <0.1 | 77 | Yes | 100 | |
| Vietnam | LM | 48,740,000 | 4,064,000 | 78.1 | 2.1 | - | <0.1 | 89 | Yes | 81 | |
| Malaysia | UM | 15,735,000 | 1,426,000 | 77.1 | 2.0 | 1.0 | <0.1 | 98 | Yes | - | |
| Cambodia | LM | 8,557,000 | 969,000 | 72.8 | 2.5 | 5.7 | 0.2 | 92 | Yes | 28 | |
| Lao PDR | LM | 3,624,000 | 448,000 | 71.0 | 2.7 | 14.4 | 0.1 | 68 | Yes | 32 | |
| Mongolia | LM | 1,663,000 | 172,000 | 72.8 | 2.9 | 6.1 | <0.1 | 98 | Yes | 93 | |
| Pacific Island Countries | Papua New Guinea | LM | 4,379,000 | 580,000 | 67.4 | 3.6 | - | 0.4 | 35 | No | 11 |
| Fiji | UM | 442,000 | 49,000 | 70.3 | 2.8 | 11.1 | <0.1 | 99 | Yes | 89 | |
| Solomon Islands | LM | 338,000 | 47,000 | 67.9 | 4.4 | 20.1 | - | 94 | Yes | 44 | |
| Vanuatu | LM | 151,000 | 22,000 | 68.3 | 3.8 | 3.3 | - | 90 | No | 48 | |
| Samoa | UM | 96,000 | 13,000 | 71.9 | 3.9 | 16.7 | - | 58 | Yes | - | |
| Kiribati | LM | 61,000 | 8000 | 62.8 | 3.6 | 34.8 | - | 97 | No | 59 | |
| Federated States of Micronesia | LM | 57,000 | 7000 | 66.1 | 3.1 | - | - | 78 | Yes | - | |
| Tonga | UM | 53,000 | 7000 | 76 | 3.6 | 12.1 | - | 99 | Yes | 90 | |
| Marshall Islands | UM | - | - | - | - | - | - | 79 | Yes | 2 | |
| Tuvalu | UM | - | - | - | - | 31.4 | - | 92 | Yes | - | |
| Population-Based Cancer Registry [4,27] | Incidence (2020) [4] | Mortality (2020) [4] | Projection (2040) [20] | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimation Method a | No. | ASR (per 100,000 Women) | % among All Female Cancers | Ranking among Female Cancers | Estimation Method b | Total (No.) | ASR (per 100,000 Women) | % among all Female Cancers | Ranking among Female Cancers | Incidence No. | Mortality No. | |||
| Asian Countries | China | Regional | 2b | 109,741 | 10.7 | 5.2 | 6 | 2b | 59,060 | 5.3 | 5.0 | 7 | 116,000 | 74,600 |
| Philippines | Regional | 2b | 7897 | 15.2 | 9.1 | 2 | 3 | 4052 | 7.9 | 8.9 | 3 | 12,900 | 7360 | |
| Vietnam | Regional | 2b | 4132 | 6.6 | 4.9 | 8 | 3 | 2223 | 3.4 | 4.6 | 7 | 5930 | 3720 | |
| Malaysia | Regional | 2b | 1740 | 10.2 | 6.8 | 4 | 3 | 991 | 5.8 | 7.1 | 5 | 2860 | 1850 | |
| Cambodia | No | 9 | 1135 | 14.0 | 11.4 | 2 | 3 | 643 | 8.3 | 10.4 | 3 | 1790 | 1090 | |
| Lao PDR | No | 9 | 371 | 12.0 | 8.1 | 4 | 3 | 191 | 6.7 | 7.1 | 3 | 629 | 354 | |
| Mongolia | National | 2a | 334 | 19.7 | 12.4 | 2 | 2a | 182 | 11.6 | 9.3 | 3 | 514 | 333 | |
| Pacific Island Countries | Papua New Guinea | No | 9 | 1077 | 29.2 | 15.9 | 2 | 3 | 650 | 19.1 | 17.0 | 2 | 1750 | 1100 |
| Fiji | No | 3b | 136 | 29.8 | 15.2 | 2 | 2a | 92 | 20.7 | 17.9 | 2 | |||
| Solomon Islands | No | 9 | 65 | 25.4 | 18.1 | 2 | 3 | 40 | 16.4 | 25.2 | 2 | |||
| Vanuatu | National | 2a | 22 | 17.1 | 17.9 | 2 | 3 | 19 | 14.9 | 27.9 | 1 | |||
| Samoa | No | 9 | 10 | 12.4 | 9.9 | 7 | 9 | 6 | 7.5 | 5.6 | 6 | |||
| Kiribati | No | - | - | - | - | - | - | - | - | - | - | |||
| Federated States of Micronesia | National | - | - | - | - | - | - | - | - | - | ||||
| Tonga | No | - | - | - | - | - | - | - | - | - | ||||
| Marshall Islands | National | - | - | - | - | - | - | - | - | - | ||||
| Tuvalu | No | - | - | - | - | - | - | - | - | - | - | |||
| Total (27 countries in WPR) | 145,747 | 10.7 | 74,864 | 5.0 | 159,000 | 97,600 | ||||||||
| Total (China, Philippines, Viet Nam, Malaysia, Cambodia, Lao PDR, Mongolia, Papua New Guinea) (% among 27 countries in WPR) | 126,427 (87%) | 67,992 (91%) | 142,373 (90%) | 90,407 (93%) | ||||||||||
| Cervical Cancer Screening Program [11] | ||||
|---|---|---|---|---|
| National Program | Main Testing Method | Screening Coverage (%) * | ||
| Asian Countries | China | Yes | Cytology | 10–50 |
| Philippines | Yes | VIA | - | |
| Vietnam | Yes | Cytology | 10–50 | |
| Malaysia | Yes | Cytology | 10–50 | |
| Cambodia | Yes | VIA | 10–50 | |
| Lao PDR | Yes | Cytology | - | |
| Mongolia | Yes | Cytology | 10–50 | |
| Pacific Island Countries | Papua New Guinea | No | - | - |
| Fiji | Yes | Cytology | 10–50 | |
| Solomon Islands | Yes | VIA | 10–50 | |
| Vanuatu | Yes | Cytology | 10–50 | |
| Samoa | No | - | - | |
| Kiribati | Yes | Cytology | 10–50 | |
| Federated States of Micronesia | Yes | VIA | 10–50 | |
| Tonga | Yes | Cytology | <10 | |
| Marshall Islands | Yes | Cytology | 10–50 | |
| Tuvalu | Yes | VIA | 10–50 | |
| Demonstration Project | National Program | Vaccination Coverage of National Program * | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Project Year | Introduction Year | Target Population | Vaccine Type; Dosing Schedule | Primary Place of Delivery | ’08 | ’09 | ’10 | ’11 | ’12 | ’13 | ’14 | ’15 | ’16 | ’17 | ’18 | ’19 | ’20 | ||
| Scale-up group | Federated States of Micronesia [28] | - | 2009 | 11–12 yo, girls | 9v; 0, 6 m | school | NA NA | NA NA | NA NA | NA NA | NA NA | NA NA | NA NA | 71 NA | 77 66 | 70 57 | 70 57 | 99 37 | |
| Marshall Islands [29] | - | 2009 | 11–12 yo, girls | 9v; 0, 6 m | school | NA NA | 30 46 | NA NA | 20 3 | 11 10 | 46 14 | 31 23 | 88 31 | 21 21 | NA 28 | 67 24 | NA NA | ||
| Malaysia [30] | - | 2010 | 13 yo, girls | 2v; 0, 6 m | school | NA NA | 83 80 | 85 84 | 91 90 | 85 85 | 85 84 | 83 83 | 96 96 | 84 83 | 86 85 | 88 84 | |||
| Fiji [31,32] | 2008–09 | 2013 | 12–13 yo, girls | 2v; 0, 6 m | school | D | D | 98 59 | 92 89 | 91 67 | 93 53 | 90 56 | 86 48 | 93 56 | NA NA | ||||
| Delivery group | Philippines [33,34,35] | 2011–12; 2014 | 2015 | 9–10 yo, girls | 4v; 0, 6 m | school | D | D | D | 28 24 | 34 24 | 27 4 | 14 1 | 23 2 | 23 5 | ||||
| Solomon Islands [36] | 2015–17 | 2019 | 9 yo, girls | 4v; 0, 12 m | school | D | D | D | 67 NA | NA 22 | |||||||||
| Lao PDR [37] | 2013–16 | 2020 | 10 yo, girls | 4v; 0, 12 m | school | D | D | D | D | 76 NA | |||||||||
| Preparation group | China [38,39] | 2020–22; 2021– | - | - | - | - | D | ||||||||||||
| Vietnam [40] | 2008–10 | - | - | - | - | D | D | D | |||||||||||
| Cambodia [41,42,43] | 2009–10; 2010–11; 2016–17 | - | - | - | - | D | D | D | D | D | |||||||||
| Mongolia [19,44] | 2012; 2014 | - | - | - | - | D | D | ||||||||||||
| Papua New Guinea [19,45] | 2012; 2017–18 | - | - | - | - | D | D | D | |||||||||||
| Vanuatu [46] | 2008; 2015–16 | - | - | - | - | D | D | D | |||||||||||
| Kiribati [19] | 2011–13 | - | - | - | - | D | D | D | |||||||||||
| Others | Samoa | - | - | - | - | - | |||||||||||||
| Tonga | - | - | - | - | - | ||||||||||||||
| Tuvalu | - | - | - | - | - | ||||||||||||||
| Cancer-Related Plan | Immunization Plan | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| NCD Plan | Cancer Control Plan | Cervical Cancer Control Plan | |||||||
| Availablity (Year Covered) | Description of HPV Vaccination * | Availablity (Year Covered) | Description of HPV Vaccination* | Availablity (Year Covered) | Description of HPV Vaccination * | Availablity (Year Covered) | Description of HPV Vaccination* | ||
| Scale-up group | Federated States of Micronesia [28,51] | Yes (2019–24) | 1 | Yes (2019–24) | 2 | NA | - | NA | - |
| Marshall Islands [29,52] | Yes (2013–18) | 0 | Yes (2017–22) | 2 | NA | - | NA | - | |
| Malaysia [30,53] | Yes (2016–25) | 0 | Yes (2016–20) | 2 | NA | - | NA | - | |
| Fiji [48,54] | Yes (2015–19) | 1 | NA | - | NA | - | Yes (2013–16) | 2 | |
| Delivery group | Philippines [34,55,56] | Yes (2017–25) | 1 | Yes (2015–20) | 1 | NA | - | Yes (2016–21) | 1 |
| Solomon Islands [36,57] | Yes (2019–23) | 0 | NA | - | NA | - | Yes (2016–20) | 2 | |
| Lao PDR [37,58] | Yes (2014–20) | 1 | NA | - | NA | - | Yes (2019–23) | 2 | |
| Preparation group | China [59,60] | Yes (2017–25) | 0 | Yes (2019–22) | 1 | NA | - | NA | - |
| Vietnam [61,62,63] | Yes (2015–25) | 1 | NA | - | Yes (2016–25) | 2 | Yes (2016–20) | 1 | |
| Cambodia [64,65,66] | Yes (2018–27) | 0 | NA | - | Yes (2019–23) | 2 | Yes (2016–20) | 1 | |
| Mongolia [67,68,69,70] | Yes (2017–21) | 1 | Yes (2015–20) | 1 | Yes (2018–21) | 2 | Yes (2017–21) | 0 | |
| Papua New Guinea [71,72,73] | Yes (2015–20) | 2 | Yes (2017–21) | 1 | NA | - | Yes (2016–20) | 2 | |
| Vanuatu [74] | Yes (2016–20) | 1 | NA | - | NA | - | NA | - | |
| Kiribati [75] | NA | - | NA | - | NA | - | Yes (2019–23) | 1 | |
| Others | Samoa [76] | Yes (2018–23) | 0 | NA | - | NA | - | NA | - |
| Tonga [77] | Yes (2015–20) | 0 | NA | - | NA | - | NA | - | |
| Tuvalu [78] | Yes (2017–21) | 0 | NA | - | NA | - | NA | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haruyama, R.; Okawa, S.; Akaba, H.; Obara, H.; Fujita, N. A Review of the Implementation Status of and National Plans on HPV Vaccination in 17 Middle-Income Countries of the WHO Western Pacific Region. Vaccines 2021, 9, 1355. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111355
Haruyama R, Okawa S, Akaba H, Obara H, Fujita N. A Review of the Implementation Status of and National Plans on HPV Vaccination in 17 Middle-Income Countries of the WHO Western Pacific Region. Vaccines. 2021; 9(11):1355. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111355
Chicago/Turabian StyleHaruyama, Rei, Sumiyo Okawa, Hiroki Akaba, Hiromi Obara, and Noriko Fujita. 2021. "A Review of the Implementation Status of and National Plans on HPV Vaccination in 17 Middle-Income Countries of the WHO Western Pacific Region" Vaccines 9, no. 11: 1355. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111355