

A Descriptive Study of the Carpal Joint of Healthy Donkeys Using Ultrasonography, Computed Tomography, and Magnetic Resonance Imaging
 ,
,  and
and 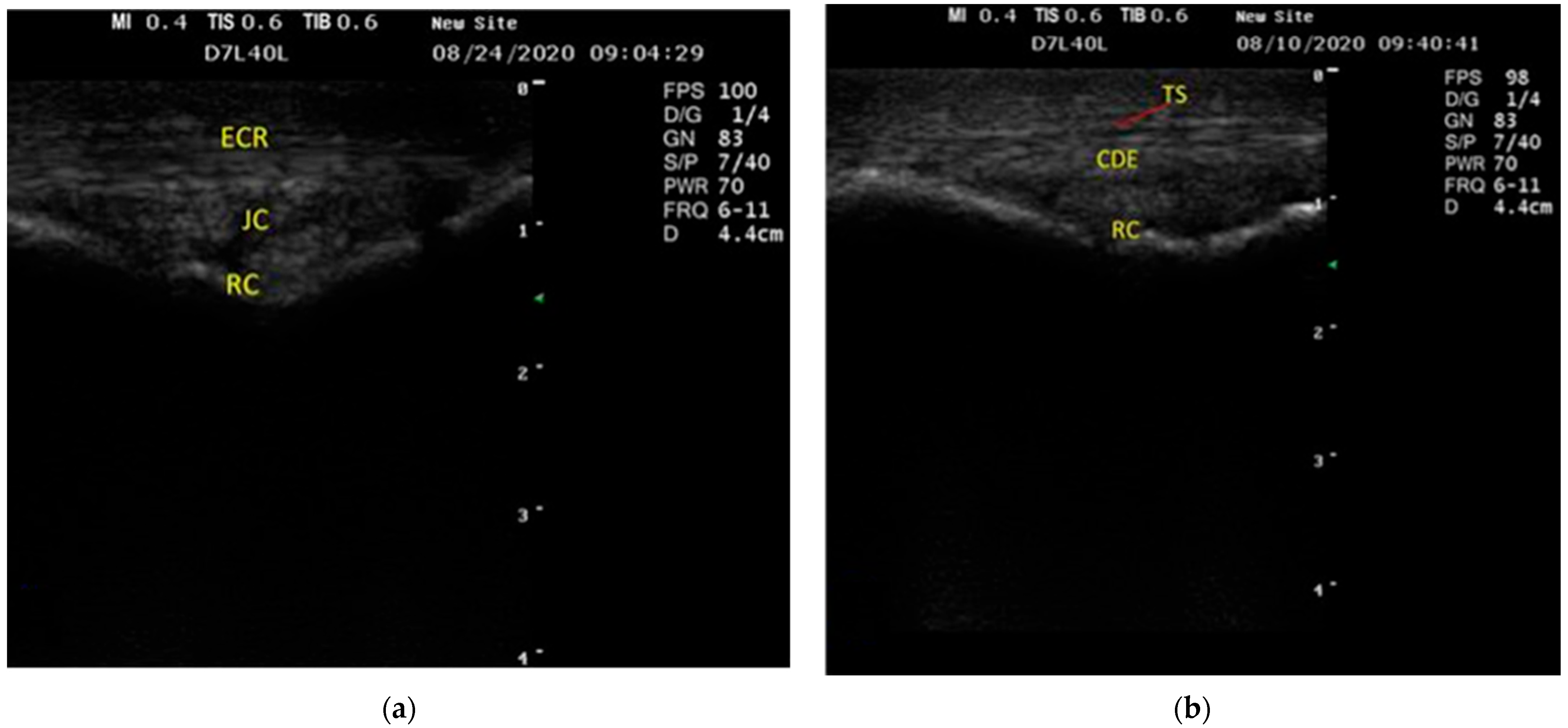{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. US Examination
2.3. CT Examination
2.4. MRI Examination
3. Results
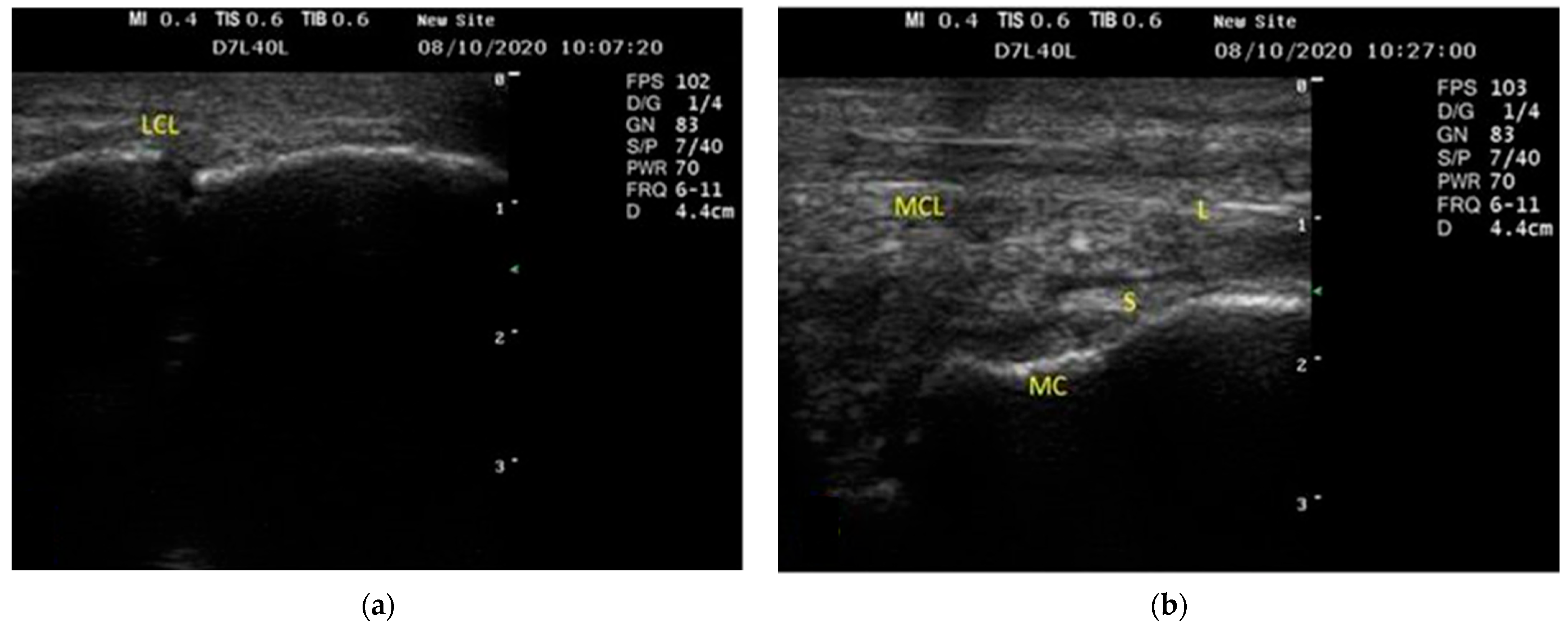
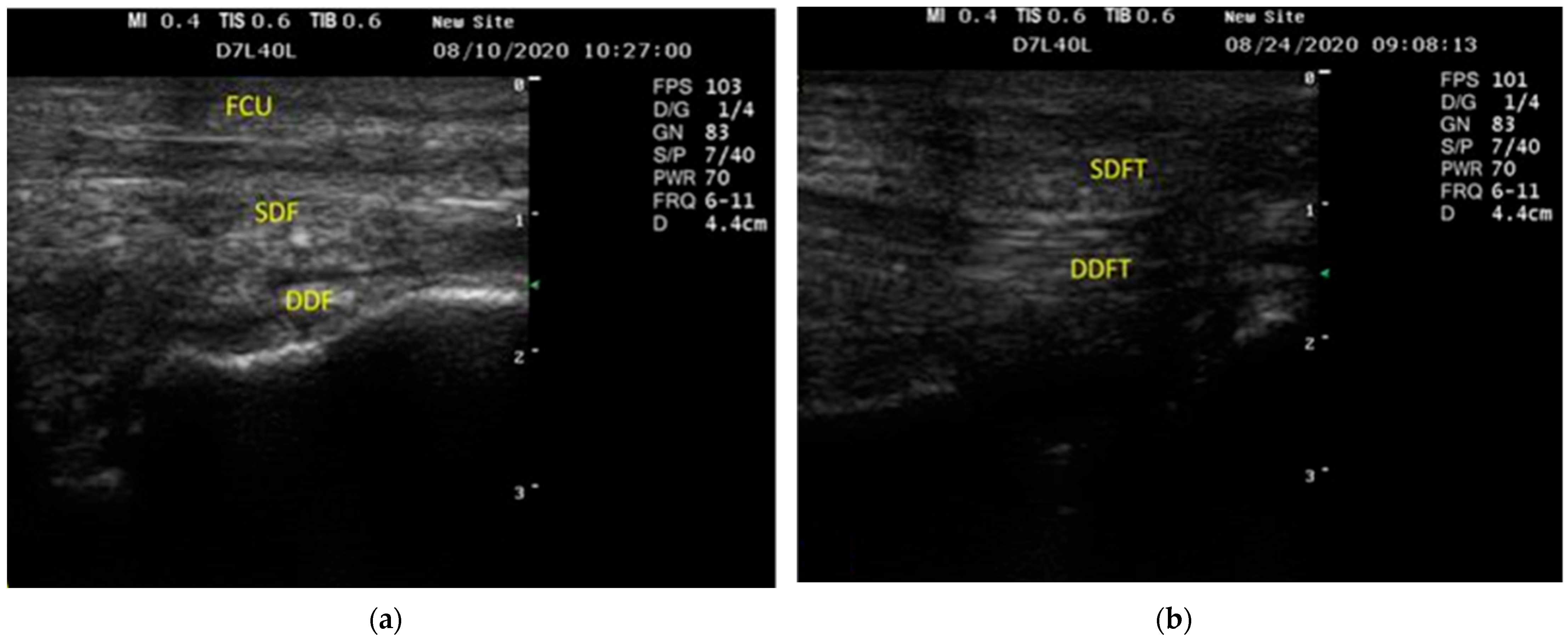
3.1. US Findings
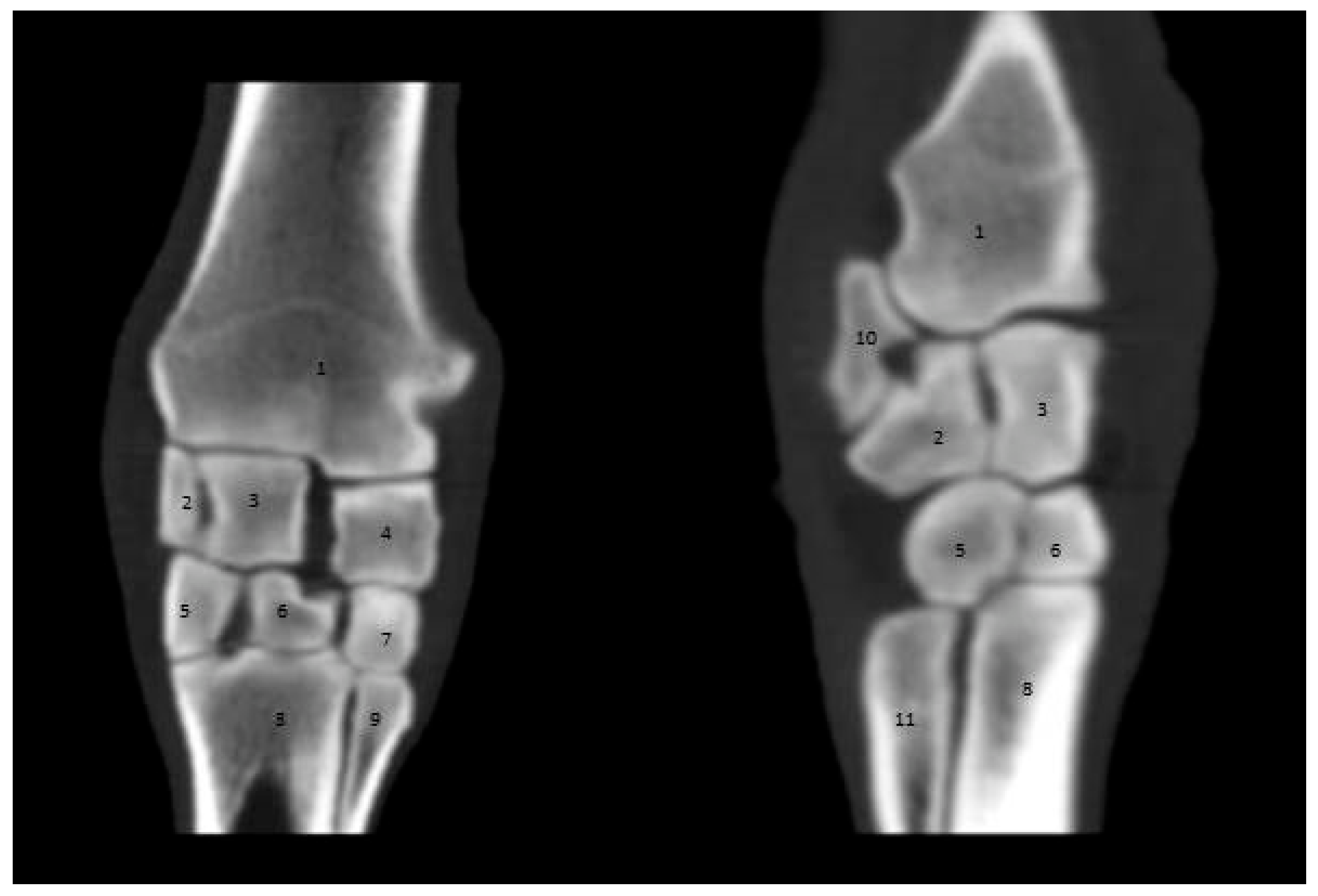
3.2. CT Findings
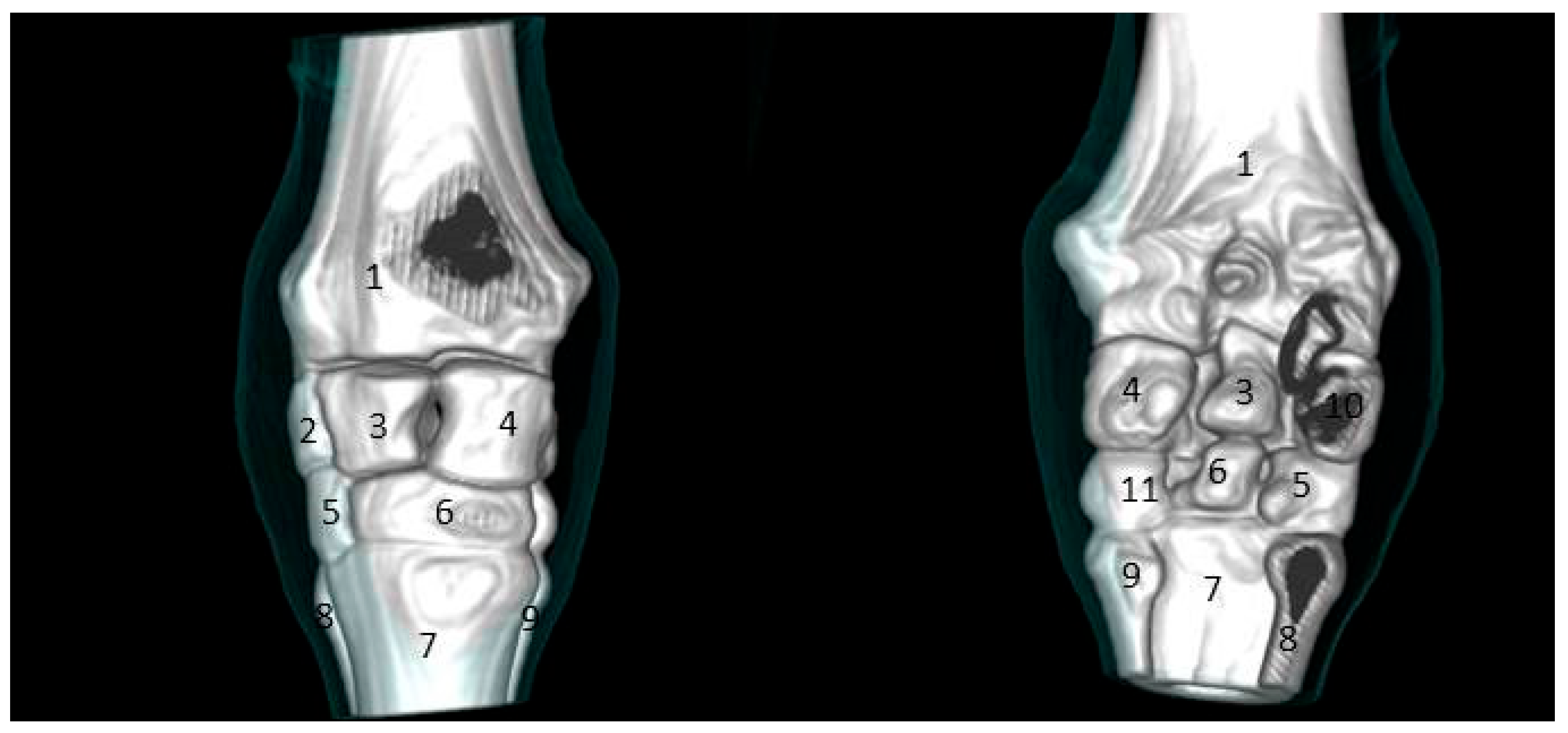
3.2.1. Sagittal and 3D Scan
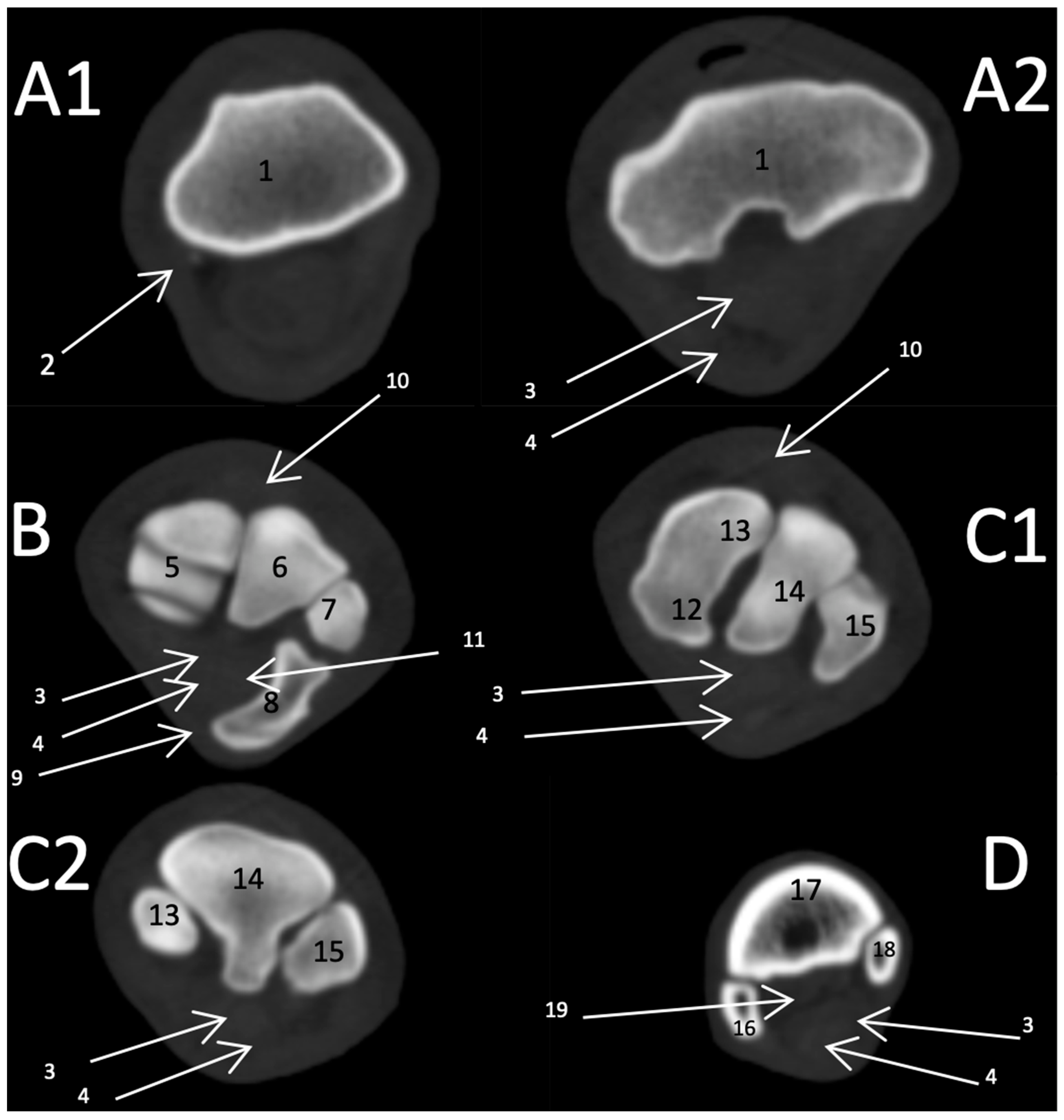
3.2.2. Transverse Scan
3.3. MRI Findings
3.3.1. First Zone
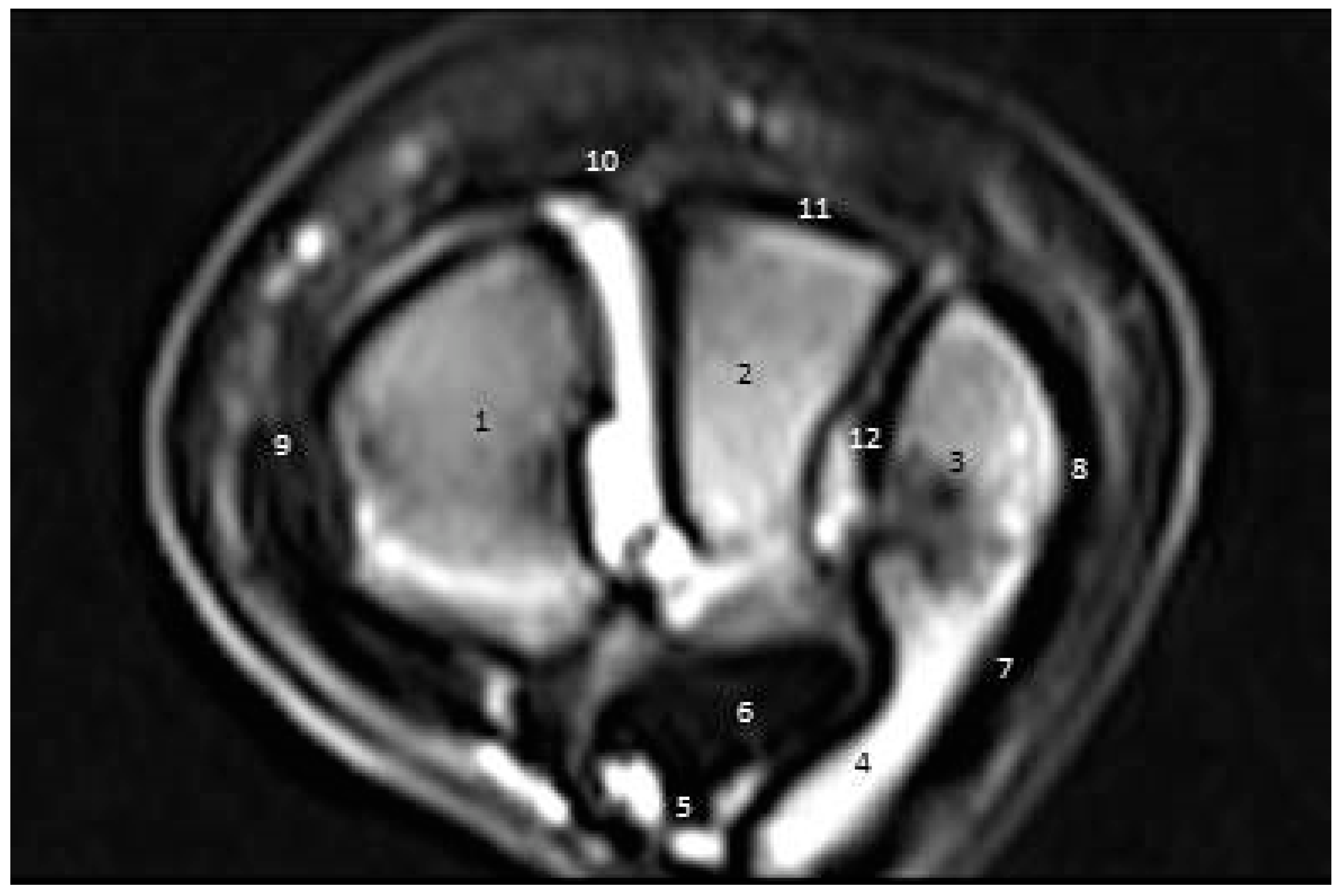
3.3.2. Second Zone
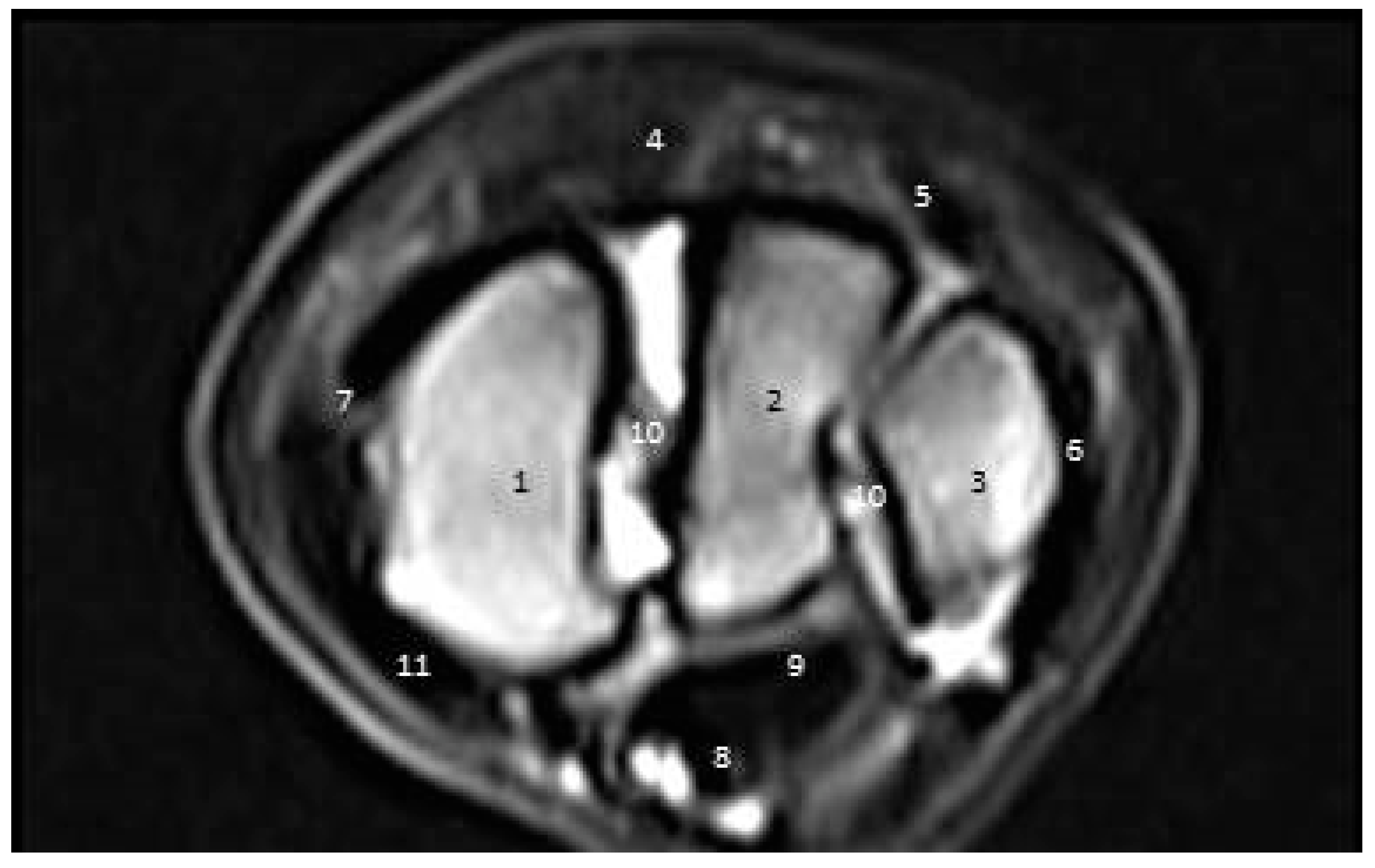
3.3.3. Third Zone
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alrtib, A.; Philip, C.; Abdunnabi, A.; Davies, H. Morphometrical Study of Bony Elements of the Forelimb Fetlock Joints in Horses. Anat. Histol. Embryol. 2013, 42, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Denoix, J.M. Functional anatomy of tendons and ligaments in the distal limbs (manus and pes). Vet. Clin. N. Am. Equine Pract. 1994, 10, 273–322. [Google Scholar] [CrossRef]
- McDuffee, L.A.; Stover, S.M.; Coleman, K. Limb Loading Activity of Adult Horses Confined to Box Stalls in an Equine Hospital Barn. Am. J. Vet. Res. 2000, 61, 234–237. [Google Scholar] [CrossRef] [PubMed]
- Dik, K.; Weller, R.; Saunders, J.; Van den Belt, A.J.; Bergman, H.-J.; Sadeleer, C.D.; Peremans, K. Diagnostic Imaging of Equine Sport Injuries. In Nuclear Medicine and Radiologic Imaging in Sports Injuries; Springer: Berlin/Heidelberg, Germany, 2015; pp. 1007–1034. [Google Scholar] [CrossRef]
- Vaughan, B.; Whitcomb, M.B.; Galuppo, L.; Shields, G. Spontaneous Rupture of the Proximal Superficial Digital Flexor Tendon: A Clinical Syndrome in Aged Equids; American Association of Equine Practitioners (AAEP): Lexington, KY, USA, 2014. [Google Scholar]
- Shields, G.E.; Barrett, M.F.; Johnson, S. How to Ultrasound the Carpal Canal and Caudal Antebrachium. How- to Session: Field Imaging. In Proceedings of the AAEP Proceedings 2015, Las Vegas, NV, USA, 5 December 2015; Available online: https://www.ivis.org/library/aaep/aaep-annual-convention-las-vegas-2015/how-to-ultrasound-carpal-canal-and-caudal-antebrachium (accessed on 1 April 2022).
- Jorgensen, J.S.; Genovese, R.L.; Döpfer, D.; Stewart, M.C. Musculoskeletal Lesions and Lameness in 121 Horses with Carpal Sheath Effusion (1999–2010). Vet. Radiol. Ultrasound 2015, 56, 307–316. [Google Scholar] [CrossRef]
- Redding, W. Use of Ultrasonography in the Evaluation of Joint Disease in Horses. Part 1: Indications, Technique and Examination of the Soft Tissues. Equine Vet. Educ. 2001, 13, 198–204. [Google Scholar] [CrossRef]
- Swidan, D.; Nouh, S.; El Kammar, M.; Abu, A.-H.M. Radiographic and Computed Tomographic Evaluation of the Carpal and Tarsal Joints in Apparently Healthy Donkeys. Alex. J. Vet. Sci. 2016, 51, 58–73. [Google Scholar] [CrossRef]
- D’Anjou, M.; Thrall, D. Textbook of Veterinary Diagnostic Radiology; Elsevier: Amsterdam, The Netherlands, 2013. [Google Scholar] [CrossRef]
- Nagy, A.; Dyson, S. Magnetic Resonance Imaging Findings in the Carpus and Proximal Metacarpal Region of 50 Lame Horses. Equine Vet. J. 2012, 44, 163–168. [Google Scholar] [CrossRef]
- Zanetti, M.; Bräm, J.; Hodler, J. Triangular Fibrocartilage and Intercarpal Ligaments of the Wrist: Does MR Arthrography Improve Standard MRI? J. Magn. Reson. Imaging 1997, 7, 590–594. [Google Scholar] [CrossRef]
- Kaser-Hotz, B.; Sartoretti-Schefer, S.; Weiss, R. Computed Tomography and Magnetic Resonance Imaging of the Normal Equine Carpus. Vet. Radiol. Ultrasound 1994, 35, 457–461. [Google Scholar] [CrossRef]
- Bienert, A.; Stadler, P. Computertomographische Untersuchungen Am Bewegungsapparat Des Pferdes–Eine Übersicht. Pferdeheilkunde 2006, 22, 218–226. [Google Scholar] [CrossRef] [Green Version]
- Groth, A.; May, S.; Weaver, M.; Weller, R. Intra-and Interobserver Agreement in the Interpretation of Navicular Bones on Radiographs and Computed Tomography Scans. Equine Vet. J. 2009, 41, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Raes, E.; Bergman, H.; Van Ryssen, B.; Vanderperren, K.; Stock, E.; Saunders, J. Computed Tomographic Features of Lesions Detected in Horses with Tarsal Lameness. Equine Vet. J. 2014, 46, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Tucker, R.L.; Sande, R.D. Computed Tomography and Magnetic Resonance Imaging in Equine Musculoskeletal Conditions. Vet. Clin. N. Am. Equine Pract. 2001, 17, 145–157. [Google Scholar] [CrossRef]
- Alsafy, M.A.; El-Gendy, S.A.; Abou-Ahmed, H.M. Articulación Del Carpo Del Asno (Equus Asinus): Investigación Morfológica. Int. J. Morphol. 2015, 33, 948–954. [Google Scholar] [CrossRef] [Green Version]
- Biggi, M.; Dyson, S.J. Use of High-Field and Low-Field Magnetic Resonance Imaging to Describe the Anatomy of the Proximal Portion of the Tarsal Region of Nonlame Horses. Am. J. Vet. Res. 2018, 79, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Kraft, S.L.; Gavin, P. Physical Principles and Technical Considerations for Equine Computed Tomography and Magnetic Resonance Imaging. Vet. Clin. N. Am. Equine Pract. 2001, 17, 115–130. [Google Scholar] [CrossRef]
- Nasvall, K.; Dyson, S.; Murray, R. The Appearance of the Proximal Part of the Metacarpal/Metatarsal Interosseous Ligaments in MRI of Horses with No History of Lameness. In Proceedings of the 47th Congress of the British Equine Veterinary Association, Liverpool, UK, 10–13 September 2008; p. 142. [Google Scholar]
- Zubrod, C.J.; Schneider, R.K.; Tucker, R.L. Use of Magnetic Resonance Imaging Identify Suspensory Desmitis and Adhesions between Exostoses of the Second Metacarpal Bone and the Suspensory Ligament in Four Horses. J. Am. Vet. Med. Assoc. 2004, 224, 1815–1820. [Google Scholar] [CrossRef]
- Bischofberger, A.S.; Konar, M.; Ohlerth, S.; Geyer, H.; Lang, J.; Ueltschi, G.; Lischer, C.J. Magnetic Resonance Imaging, Ultrasonography and Histology of the Suspensory Ligament Origin: A Comparative Study of Normal Anatomy of Warmblood Horses. Equine Vet. J. 2006, 38, 508–516. [Google Scholar] [CrossRef]
- Anastasiou, A.; Skioldebrand, E.; Ekman, S.; Hall, L. Ex Vivo Magnetic Resonance Imaging of the Distal Row of Equine Carpal Bones: Assessment of Bone Sclerosis and Cartilage Damage. Vet. Radiol. Ultrasound 2003, 44, 501–512. [Google Scholar] [CrossRef]
- Murray, R.C.; Branch, M.V.; Tranquille, C.; Woods, S. Validation of Magnetic Resonance Imaging for Measurement of Equine Articular Cartilage and Subchondral Bone Thickness. Am. J. Vet. Res. 2005, 66, 1999–2005. [Google Scholar] [CrossRef]
- Dyson, S.; Murray, R. Magnetic Resonance Imaging of the Equine Foot. Clin. Tech. Equine Pract. 2007, 6, 46–61. [Google Scholar] [CrossRef]
- Ross, M.W. Carpus. In Diagnosis and Management of Lameness in the Horse; Elsevier: Amsterdam, The Netherlands, 2003; pp. 376–394. [Google Scholar] [CrossRef]
- Alsafy, M.A.; El-Kammar, M.H.; Nouh, S.R.; Abou-Ahmed, H.M.; Perez, W.; Vazquez, N.; Swidan, D. Radiographic and Computed Tomographic Anatomy of the Donkey Carpus. J. Morphol. Sci. 2019, 36, 145–155. [Google Scholar] [CrossRef] [Green Version]
- Nagy, A.; Dyson, S. Magnetic Resonance Anatomy of the Carpus of the Horse Described from Images Acquired from Low-field and High-field Magnets. Vet. Radiol. Ultrasound 2011, 52, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Baxter, G.M.; Stashak, T.S.; Keegan, K.G. Examination for Lameness: History, Visual Exam, and Conformation. In Adams Stashak’s Lameness Horses, 7th ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2020; pp. 67–188. [Google Scholar] [CrossRef]
- Salem, M.; El-Shafaey, E.-S.; Mosbah, E.; Zaghloul, A. Ultrasonographic, Computed Tomographic, and Magnetic Resonance Imaging of the Normal Donkeys (Equus Asinus) Digit. J. Equine Vet. Sci. 2019, 74, 68–83. [Google Scholar] [CrossRef]
- Dyson, S.; Murray, R.; Schramme, M.; Branch, M. Magnetic Resonance Imaging of the Equine Foot: 15 Horses. Equine Vet. J. 2003, 35, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Hage, M.C.F.N.S.; Invernizzi, M.S.; Bellegard, G.M.C.; Dória, R.G.S.; Schwarzbach, S.V.; Miada, V.J.Y. Didatic Approach of Ultrasonographic Examination for Evaluation of the Carpal Joint in Horses. Ciência Rural. 2017, 47, 1–6. [Google Scholar] [CrossRef]
- El-Bably, S.; Abdelgalil, A. Ultrasonographic Anatomy of the Equine Carpal Region (Equus Caballus). Int. J. Vet. Sci. 2018, 7, 44–49. [Google Scholar] [CrossRef]
- Reef, V.B.; Whittier, M.; Allam, L.G. Muscle and Bone Ultrasonography. Clin. Tech. Equine Pract. 2004, 3, 268–273. [Google Scholar] [CrossRef]
- Reef, V.B. Muscloskeletal ultrasonography. In Equine Diagnostic Ultrasound, 1st ed.; W.B. saunders Co.: Philadilphia, PA, USA, 1998; Volume 3, pp. 39–186. [Google Scholar]
- Smith, R.K.W. Pathophysiology of tendon injury. In Diagnosis and Management of Lameness in the Horse; Elsevier: Amsterdam, The Netherlands, 2003; pp. 616–628. [Google Scholar] [CrossRef]
- Tnibar, M.; Kaser-Hotz, B.; Auer, J.A. Ultrasonography of the Dorsal and Lateral Aspects of the Equine Carpus: Technique and Normal Appearance. Vet. Radiol. Ultrasound 1993, 34, 413–425. [Google Scholar] [CrossRef]
- Kofler, J. Ultrasonographic Examination of the Carpal Region in Cattle—Normal Appearance. Vet. J. 2000, 159, 85–96. [Google Scholar] [CrossRef]
- Kassab, A. The Normal Anatomical, Radiographical and Ultrasonographic Appearance of the Carpal Region of One-humped Camel (Camelus Dromedarius). Anat. Histol. Embryol. 2008, 37, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Denoix, J.-M. Ultrasonographic Examination of Joints, a Revolution in Equine Locomotor Pathology. Bull. De L’académie Vétérinaire De Fr. 2009, 162, 313–325. [Google Scholar] [CrossRef] [Green Version]
- McIlwraith, C.W.; Frisbie, D.D.; Kawcak, C.; Van Weeren, R. Joint Disease in the Horse; Elsevier Health Sciences: Amsterdam, The Netherlands, 2015; ISBN 0-323-35289-8. [Google Scholar]
- Dyce, K.M.; Sack, W.O.; Wensing, C.J.G. Textbook of Veterinary Anatomy-E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2009; ISBN 1-4377-0875-7. [Google Scholar]
- Schwarz, T.; Saunders, J. Veterinary Computed Tomography; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar] [CrossRef]
- Bergman, H.; Saunders, J. Equine Upper Limbs (Carpus, Tarsus, Stifle). In Veterinary Computed Tomography; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2011; pp. 483–501. [Google Scholar] [CrossRef]
- Thrall, D.E. Textbook of Veterinary Diagnostic Radiology-E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013; ISBN 0-323-26638-X. [Google Scholar]
- Bowen, A.J.; Burd, M.A.; Craig, J.J.; Craig, M. Radiographic calibration for analysis of bone mineral density of the equine third metacarpal bone. J. Equine Vet. Sci. 2013, 33, 1131–1135. [Google Scholar] [CrossRef]
- Mair, T.; Kinns, J.; Jones, R.; Bolas, N. Magnetic Resonance Imaging of the Distal Limb of the Standing Horse. Equine Vet. Educ. 2005, 17, 74–78. [Google Scholar] [CrossRef]
- Whitton, R.; Buckley, C.; Donovan, T.; Wales, A.D.; Dennis, R. The Diagnosis of Lameness Associated with Distal Limbpathology in a Horse: A Comparison of Radiography, Computed Tomography and Magnetic Resonance Imaging. Vet. J. 1998, 155, 223–229. [Google Scholar] [CrossRef]
- Tietje, S.; Nowak, M.; Petzoldt, S.; Weiler, H. Die Computertomographische Darstellung Des Distalen Abschnitts Der Tiefen Beugesehne (TBS) Des Pferdes. Pferdeheilk 2001, 17, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Nazem, M.; Sajjadian, S. Anatomical Transverse Magnetic Resonance Imaging Study of Ligaments in Palmar Surface of Metacarpus in Miniature Donkey: Identification of a New Ligament. Folia Morphol. 2017, 76, 110–116. [Google Scholar] [CrossRef] [Green Version]
- Nagy, A.; Dyson, S.J. Magnetic Resonance Findings in the Carpus and Proximal Metacarpal Region of Non-Lame Horses. In Proceedings of the American Association of Equine Practitioners Annual Convention, Las Vegas, NV, USA, 9 December 2009; Volume 55, pp. 408–4017. [Google Scholar]
- Whitton, R.C.; Kannegieter, N.J.; Rose, R.J. The Intercarpal Ligaments of the Equine Midcarpal Joint, Part 3: Clinical Observations in 32 Racing Horses with Midcarpal Joint Disease. Vet. Surg. 1997, 26, 374–381. [Google Scholar] [CrossRef]
- Budras, K.D.; Sack, W.O.; Rock, S.; Horowitz, A.; Berg, R. Anatomy of the Horse, 6th ed.; Schluetersche: London, UK, 2012; ISBN 978-3-8426-8368-6. [Google Scholar]
- Murray, R.C. Equine MRI; John Wiley & Sons: Hoboken, NJ, USA, 2010; ISBN 1-4443-2920-0. [Google Scholar]
- Erickson, S.J.; Prost, R.; Timins, M. The Magic Angle Effect: Background Physics and Clinical Relevance. Radiology 1993, 188, 23–25. [Google Scholar] [CrossRef] [Green Version]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salem, M.; El-Shafaey, E.-S.; Farag, A.M.M.; El-khodery, S.; Al Mohamad, Z.; Abass, M. A Descriptive Study of the Carpal Joint of Healthy Donkeys Using Ultrasonography, Computed Tomography, and Magnetic Resonance Imaging. Vet. Sci. 2022, 9, 249. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci9050249
Salem M, El-Shafaey E-S, Farag AMM, El-khodery S, Al Mohamad Z, Abass M. A Descriptive Study of the Carpal Joint of Healthy Donkeys Using Ultrasonography, Computed Tomography, and Magnetic Resonance Imaging. Veterinary Sciences. 2022; 9(5):249. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci9050249
Chicago/Turabian StyleSalem, Mohamed, El-Sayed El-Shafaey, Alshimaa M. M. Farag, Sabry El-khodery, Zakriya Al Mohamad, and Marwa Abass. 2022. "A Descriptive Study of the Carpal Joint of Healthy Donkeys Using Ultrasonography, Computed Tomography, and Magnetic Resonance Imaging" Veterinary Sciences 9, no. 5: 249. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci9050249