
The Impact of Resistance Training on Body Composition, Muscle Strength, and Functional Fitness in Older Women (45–80 Years): A Systematic Review (2010–2020)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Questions
2.2. Literature Search
2.2.1. Search Strategy
2.3.2. Inclusion and Exclusion Criteria
2.3.3. Quality Assessment
3. Results
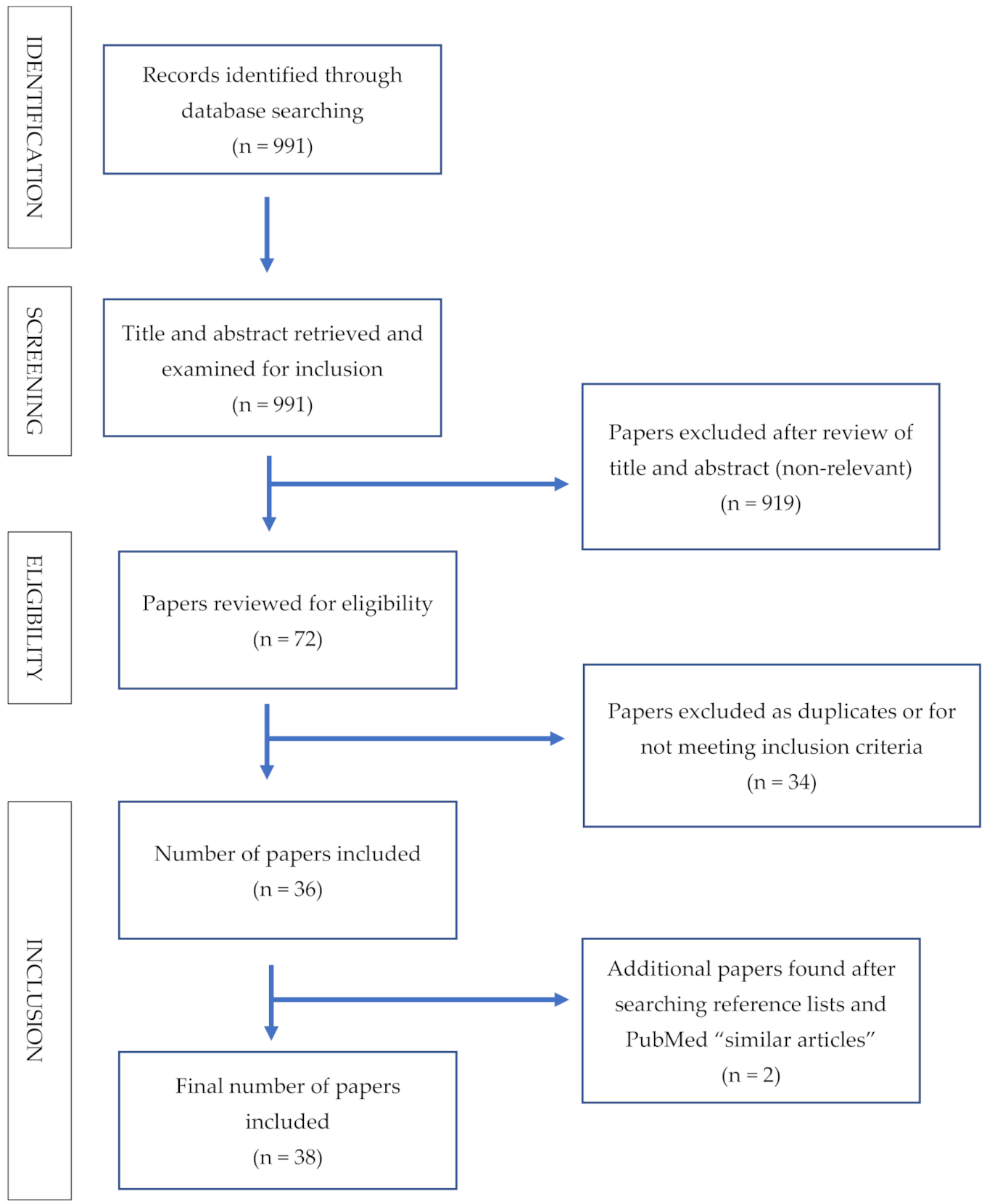
3.1. Summary of Search Results
3.2. Characteristics of Included Studies
3.2.1. Participant Characteristics
3.2.2. Summary of Intervention Characteristics
3.2.3. Study Quality
3.2.4. Effects on Body Composition
3.2.5. Effects on Muscle Strength
3.2.6. Effects on Functional Fitness

{kind=link}
| Study and Duration | # Sets | # Reps (Midpoint of Range) | # Exercises | Participant Exposure Score (Reps × Sets × Exercises) | Total Sessions (Times/Wk × Total # Weeks) | Total Minutes (# Sessions × Minutes/Session) | Adherence | >Muscle Mass, FFM or LBM | <%BF | Other Body Comp Measure |
|---|---|---|---|---|---|---|---|---|---|---|
| Short-length study (<12 wks) | ||||||||||
| dos Santos [33] | 3 | 10 | 8 | 240 | 24 | ? | ≥85% | x | ||
| dos Santos [34] | 3 | 10 | 8 | 240 | 24 | ? | ≥85% | x (mostly android) | ||
| Nabuco [43] | 3 | 10 | 8 | 240 | 24 | ? | ? | High PRO | ||
| Medium-length studies (≥12 to <24 wks) | ||||||||||
| Aguiar [21] | 2 | 12.5 | 8 | 200 | 36 | 2160 | ? | x | NC by measurement | |
| Barbalho [22] | 3.75 | 10 | 8 | 240 | 24 | ? | 95% | |||
| Bocalini [23] | 1 | Timed reps | 12 | ? | 36 | 1800 | >90% | x | not measured | |
| Carrasco-Poyatos [25] | 1 | 8 | 8 | 60 | 36 | 2160 | ? | >both Pilates and RT | ||
| Cavalcante [26] | 1 | 12.5 | 8 | 250 | 40 | 1200 | ≥85% | Both 2x/wk and 3x/wk< | ||
| Coelho-Junior [27] | 2 | 13.5 | 9 | 364.5 | 44 | ? | 89% | NC | NC by measure | |
| Cunha [29] | 2 | 12.5 | 8 | 100 LV or 300 HV | 36 | 540 LV or 1620 HV | ≥85% | >both low and high volume | ||
| Daly [30] | 3 | 9 | 7 | 189 | 48 | 2880 | 89% | >in LBM, FFM in fortified milk group | %BF < in both grps but more in Milk Grp | <Fat mass |
| Francis [35] | 3.5 | 12 | 9 | 378 | 36 | 1908 | 82–86% | >leg lean tissue in both PRO + PRO + RT | ||
| Gadelha [36] | 3 | 10 | 8 | 240 | 72 | ? | ≥75% | >FFM in RT vs. CTL | NC | Sarcopenic obesity index > in RT vs. CTL |
| Gualano [37] | 2 | 10 | 7 | 175 | 60 | ? | ≥84% | RT + CR ≥ appendicular LBM vs. PL, CR and PL + RT | Fat mass (kg) did not change between grps | |
| Kim [38] | 1 | 8 | varying | ? | 24 | ? | 70–80% | Leg LBM > EX + AA and EX | ||
| Liao [40] | 3 | 10 | 8 | 240 | 36 | 1980 | ? | Ex bands > LBM | %BF < in EG vs. CG | Ex bands > muscle quality |
| Mori [41] | 2.5 | 10 | 7 | 175 | 48 | ? | 87–90% | >LBM in EX + PRO vs. EX or PRO | ||
| Nabuco [42] | 3 | 10 | 8 | 240 | 36 | ? | ? | Exercise + whey PRO > LBM vs. placebo | ||
| Nabuco [44] | 3 | 8 | 8 | 192 | 36 | ? | ? | RT+ PRO > LBM vs. RT+PLA | <%BF in RT + PRO vs. RT + PLA | |
| Nascimento [45] | 1 | 12.5 | 8 | 100 | 48 (2x) or 72 (3x) | ? | 92–93% adherence | 2 or 3x/wk > LBM | ||
| Rabelo [46] | 3 | 10 | 10 | 300 | 72 | 4320 | ≥85% | RT > LBM | ||
| Radaelli [47] | 2 | 14.5 | 10 | L: 145 H: 435 | 26 | L: 585 H: 1430 | Muscle thickness and neuromuscular adaptations > similarly in both groups | |||
| Ribeiro [51] | 3 | 11.5 | 8 | 300 | 96 | ? | ≥85% | Both pyramid and constant training > LBM | Neither grp changed | |
| Ribeiro [52] | 3 | 10 | 8 | 240 | 48 | ? | ≥85% | Both pyramid and trad > LBM | ||
| Strandberg [54] | 3 | 13.5 | 7 | 283.5 | 48 | ? | ? | Lean leg mass > only in RT + healthy diet | ||
| Strandberg [55] | 3 | 13.5 | 7 | 283.5 | 48 | ? | ? | Sig hypertrophy of T2 muscle fibers only in RT + PUFA-not RT only or CTL | ||
| Sugihara [56] | 3 | 10 | 8 | 240 | 36 | 1800 | ? | Both RT+PRO and RT + PLA > LBM (but RT + PRO >) | Both RT+PRO and RT + PLA > muscle quality | |
| Study and Duration | PS | # Sets | # Reps (Midpoint of Range) | # Exercises | Participant Exposure Score (Reps × Sets × Exercises) | Total Sessions (Times/Wk × Total # Weeks) | Total Minutes (# Sessions × Minutes/Session) | Adherence | 1RM Bench or Chest Press | 1RM Bicep Curl (or > Timed Curl) | >1RM Knee Extension | >1RM Leg Press | Other Strength Measure |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Short-length studies (<12 wks) | |||||||||||||
| dos Santos [33] | 5 | 3 | 10 | 8 | 240 | 24 | ? | ≥85% | x | x | x | x | |
| Nabuco [43] | 2 | 3 | 10 | 8 | 240 | 24 | ? | ? | High PRO | Total strength > high PRO | |||
| Medium-length studies (≥12 to <24 wks) | |||||||||||||
| Aguiar [21] | 7 | 2 | 12.5 | 8 | 200 | 36 | 2160 | ? | x | x | x | ||
| Barbalho [22] | 4 | 3.75 | 10 | 8 | 240 | 24 | ? | 95% | x | x | x | ||
| Correa [28] | 5 | 3 | ? | 3 lower body | ? | 36 | ? | x | >muscle activation | ||||
| Cunha [29] | 4 | 2 | 12.5 | 8 | 100 LV or 300 HV | 36 | 540 LV or 1620 HV | ≥85% | x | x | |||
| Daly [30] | 4 | 3 | 9 | 7 | 189 | 48 | 2880 | 89% | NS diff in muscle strength. Why? Adherence was good | ||||
| de Resende-Netro [31] | 5 | 2 | 9 | 8 | 144 | 36 | 1620 | ? | Functional and trad RT > strength | ||||
| Francis [35] | 4 | 3.5 | 12 | 9 | 378 | 36 | 1908 | 82–86% | >in PRO + RT | ||||
| Gualano [37] | 6 | 2 | 10 | 7 | 175 | 60 | ? | ≥84% | >1RM bench press in RT + CR | >1RM Leg Press in RT + CR | |||
| Kim [38] | 4 | 1 | 8 | varying | ? | 24 | ? | 70–80% | >only in EX + AA | ||||
| Letieri [39] | 6 | 4 | ? | High or low blood flow occlusion | H: 112 or L: 240 | 48 | 2160 | ? | Isokinetic torque of KE (R/L) and LC higher in both groups | ||||
| Nabuco [42] | 5 | 3 | 10 | 8 | 240 | 36 | ? | ? | >WP vs. PLA | >WP vs. PLA | >total strength in WP vs. PLA | ||
| Nabuco [44] | 6 | 3 | 8 | 8 | 192 | 36 | ? | ? | Both> | Both> | Both> | Both > total strength | |
| Rabelo [46] | 4 | 3 | 10 | 10 | 300 | 72 | 4320 | ≥85% | RT > KE peak torque | ||||
| Radaelli [47] | 3 | 2 | 14.5 | 10 | L: 145 H: 435 | 26 | L: 585 H: 1430 | 1RM KE > both grps | Muscle activation > both grps | ||||
| Ramirez-Campillo [49] | 4 | 3 | 8 | 8 | 192 | 36 | ? | ? | High and low spd > strength | ||||
| Ramirez-Campillo [50] | 4 | 3 | 8 | 8 | 2x = 192 3x = 128 | 2x = 24 3x = 36 | 2x = 1440 3x = 2160 | ? | > isometric hand grip strength | ||||
| Ribeiro [51] | 4 | 3 | 11.5 | 8 | 300 | 96 | ? | ≥85% | Both pyramid and constant training > | ||||
| Ribeiro [52] | 5 | 3 | 10 | 8 | 240 | 48 | ? | ≥85% | Both pyramid and trad > | Both pyramid and trad > | Both pyramid and trad > | ||
| Strandberg [54] | 4 | 3 | 13.5 | 7 | 283.5 | 48 | ? | ? | RT+HD and RT > vs. CTL | ||||
| Sugihara [56] | 5 | 3 | 10 | 8 | 240 | 36 | 1800 | ? | Both > WP > PLA | Both > WP > PLA | Both > WP > PLA | ||
| Tiggeman [57] | 4 | 2 | 12 | 6 | 144 | 24 | ? | ? | Both > KE | Both > LP | |||
| Study and Duration | PS | # Sets | # Reps (Midpoint of Range) | # Exercises | Participant Exposure Score (Reps × Sets × Exercises) | Total Sessions (Times/Wk × Total # Weeks) | Total Minutes (# Sessions × Minutes/Session) | Adherence | <TUG Time | >30 s Chair Stands | >Walking or Gait Speed | Other FF Measure |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medium-length studies (≥12 to <24 wks) | ||||||||||||
| Aguiar [21] | 7 | 2 | 12.5 | 8 | 200 | 36 | 2160 | ? | x | <floor get up time | ||
| Barbalho [22] | 4 | 3.75 | 10 | 8 | 240 | 24 | ? | 95% | x | |||
| Carrasco-Poyatos [25] | 3 | 1 | 8 | 8 | 60 | 36 | 2160 | ? | Pilates > RT and CTL | RT > static balance | ||
| Coelho-Junior [27] | 6 | 2 | 13.5 | 9 | 364.5 | 44 | ? | 89% | x | >CM jump; balance | ||
| Correa [28] | 5 | 3 | ? | 3 lower body | ? | 36 | ? | >in rapid strength only | <CM jump in rapid strength only | |||
| Daly [30] | 4 | 3 | 9 | 7 | 189 | 48 | 2880 | 89% | Both grps > stair ascent | |||
| de Resende-Netro [31] | 5 | 2 | 9 | 8 | 144 | 36 | 1620 | ? | >Only in functional training | |||
| Francis [35] | 4 | 3.5 | 12 | 9 | 378 | 36 | 1908 | 82–86% | >Gait speed in PRO + RT | |||
| Kim [38] | 4 | 1 | 8 | varying | ? | 24 | ? | 70–80% | >in all int grps | |||
| Liao [40] | 4 | 3 | 10 | 8 | 240 | 36 | 1980 | ? | <TUG score | >chair rise | >gait speed | |
| Mori [41] | 4 | 2.5 | 10 | 7 | 175 | 48 | ? | 87–90% | >gait speed in EX + PRO vs. PRO alone | |||
| Nabuco [42] | 5 | 3 | 10 | 8 | 240 | 36 | ? | ? | <10 m walk test time | |||
| Radaelli [47] | 3 | 2 | 14.5 | 10 | L: 145 H: 435 | 26 | L: 585 H: 1430 | |||||
| Radaelli [48] | 5 | 2 | 10 | 7 | L: 70 H: 210 | 24 | L: 720 H: 1200 | ≥85% | Both grps > VJ | |||
| Ramirez-Campillo [49] | 4 | 3 | 8 | 8 | 192 | 36 | ? | ? | High spd < TUG vs. lo spd | High spd > gait speed and ball throw vs. low spd | ||
| Ramirez-Campillo [50] | 4 | 3 | 8 | 8 | 2x = 192 3x = 128 | 2x = 24 3x = 36 | 2x = 1440 3x = 2160 | ? | Both < TUG score | Both > chair rise score | Both > 10 m walk | |
| Souza [53] | 4 | 2 | 12 | varied | 72 | 28 | 462 | >80% | Trad RT > walk speed vs. elastic band | |||
| Tiggeman [57] | 4 | 2 | 12 | 6 | 144 | 24 | ? | ? | <TUG score | >chair rise score | >distance on 6 min walk test; >stair climb | |
4. Discussion
4.1. Limitations
4.2. Future Research Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Volpi, E.; Nazemi, R.; Fujita, S. Muscle tissue changes with aging. Curr. Opin. Clin. Nutr. Metab. Care 2004, 7, 405–410. [Google Scholar] [CrossRef] [Green Version]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.M.E.E.; Mahanani, W.R.; et al. The world report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [Green Version]
- Utian, W.H. Biosynthesis and physiologic effects of estrogen and pathophysiologic effects of estrogen deficiency: A review. Am. J. Obstet. Gynecol. 1989, 161, 1828–1831. [Google Scholar] [CrossRef]
- Li, C.Y.; Jee, W.S.S.; Chen, J.L.; Mo, A.; Setterberg, R.B.; Su, M.; Tian, X.Y.; Ling, Y.F.; Yao, W. Estrogen and “Exercise” Have a Synergistic Effect in Preventing Bone Loss in the Lumbar Vertebra and Femoral Neck of the Ovariectomized Rat. Calcif. Tissue Int. 2003, 72, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Bamman, M.M.; Hill, V.J.; Adams, G.R.; Haddad, F.; Wetzstein, C.G.; Gower, G.A.; Ahmed, A.; Hunter, G.R. Gender differences in resistance training induced myofiber hypertrophy among older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 108–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, S.K.; Rook, K.M.; Siddle, N.C.; Bruce, S.A.; Woledge, R.C. Muscle weakness in women occurs at an earlier age than in men, but strength is preserved by hormone replacement therapy. Clin. Sci. 1993, 84, 95–98. [Google Scholar] [CrossRef] [Green Version]
- Dam, T.V.; Dalgaard, L.B.; Ringgaard, S.; Johansen, F.T.; Bengtsen, M.B.; Mose, M.; Lauritsen, K.M.; Ortenblad, N.; Gravholt, C.H.; Hansen, M. Transdermal estrogen therapy improves gains in skeletal muscle mass after 12 weeks of resistance training in early postmenopausal women. Front. Physiol. 2021, 11, 596130. [Google Scholar] [CrossRef] [PubMed]
- Chambers, M.A.; Moylan, J.S.; Reid, M.B. Physical inactivity and muscle weakness in the critically ill. Crit. Care Med. 2009, 37, S337–S346. [Google Scholar] [CrossRef]
- Jerome, G.J.; Glass, T.A.; Mielke, M.; Xue, Q.-L.; Andersen, R.E.; Fried, L.P. Physical activity participation by presence and type of functional deficits in older women: The Women’s Health and Aging Studies. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1171–1176. [Google Scholar] [CrossRef] [Green Version]
- Becker, L.; Semmlinger, L.; Rohleder, N. Resistance training as an acute stressor in healthy young men: Associations with heart rate variability, alpha-amylase, and cortisol levels. Stress 2020, 24, 318–330. [Google Scholar] [CrossRef]
- Benito, P.J.; Cuperio, R.; Ramos-Campo, D.J.; Alcaraz, P.E.; Rubio-Arias, J.Á. Systematic Review with Meta-Analysis of the Effect of Resistance Training on Whole-Body Muscle Growth in Healthy Adult Males. Int. J. Environ. Res. Public Health 2020, 17, 1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marín-Cascales, E.; Alcaraz, P.E.; Ramos-Campo, D.J.; Rubio-Arias, J.A. Effects of multicomponent training on lean and bone mass in postmenopausal and older women: A systematic review. Menopause 2018, 25, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Marín-Cascales, E.; Alcaraz, P.E.; Ramos-Campo, D.J.; Martinez-Rodriguez, A.; Chung, L.H.; Rubio-Arias, J.Á. Whole-body vibration training and bone health in postmenopausla women: A systematic review and meta-analysis. Medicine 2018, 97, e11918. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, G.; Iancu, H.D. Comparison of performance and health indicators between perimenopausal and postmenopausal obese women: The effect of high-intensity interval training (HIIT). Menopause 2020, 28, 50–57. [Google Scholar] [CrossRef]
- Devries, M.C.; Phillips, S.M. Creatine supplementation during resistance training in older adults—A meta-analysis. Med. Sci. Sports Exerc. 2014, 46, 1194–1203. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.K.; Quinn, M.A.; Saunders, D.H.; Greig, C.A. Protein Supplementation Does Not Significantly Augment the Effects of Resistance Exercise Training in Older Adults: A Systematic Review. J. Am. Med. Dir. Assoc. 2016, 17, 959-e1–959-e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, C.-D.; Tsauo, J.-Y.; Wu, Y.-T.; Cheng, C.-P.; Chen, H.-C.; Huang, Y.-C.; Chen, H.-C.; Liou, T.-H. Effects of protein supplementation combined with resistance exercise on body composition and physical function in older adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2017, 106, 1078–1091. [Google Scholar] [CrossRef] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 354, i4086. [Google Scholar] [CrossRef] [Green Version]
- PEDro Scale. Available online: https://pedro.org.au/wp-content/uploads/PEDro_scale.pdf (accessed on 1 May 2021).
- Evidence Based Medicine-PICO. Available online: https://researchguides.uic.edu/c.php?g=252338&p=3954402 (accessed on 19 May 2021).
- Aguiar, A.F.; Januário, R.S.; Junior, R.P.; Gerage, A.M.; Pina, F.L.; do Nascimento, M.A.; Padovani, C.R.; Cyrino, E.S. Long-term creatine supplementation improves muscular performance during resistance training in older women. Eur. J. Appl. Physiol. 2013, 113, 987–996. [Google Scholar] [CrossRef]
- Barbalho, M.S.M.; Gentil, P.; Izquierdo, M.; Fisher, J.; Steele, J.; Raiol, R.A. There are no no-responders to low or high resistance training volumes among older women. Exp. Gerontol. 2017, 99, 18–26. [Google Scholar] [CrossRef]
- Bocalini, D.S.; Lima, L.S.; de Andrade, S.; Madureira, A.; Rica, R.L.; Santos, R.N.D.; Serra, A.J.; Silva, J.A., Jr.; Rodriguez, D.; Figueira, A., Jr.; et al. Effects of circuit-based exercise programs on the body composition of elderly obese women. Clin. Interv. Aging 2012, 7, 551–556. [Google Scholar] [CrossRef] [Green Version]
- Carneiro, N.H.; Ribeiro, A.S.; Nascimento, M.A.; Gobbo, L.A.; Schoenfeld, B.J.; Júnior, A.A.; Gobbi, S.; Oliveira, A.R.; Cyrino, E.S. Effects of different resistance training frequencies on flexibility in older women. Clin. Interv. Aging 2015, 10, 531–538. [Google Scholar] [CrossRef] [Green Version]
- Carrasco-Poyatos, M.; Rubio-Arias, J.A.; Ballesta-García, I.; Ramos-Campo, D.J. Pilates vs. muscular training in older women. Effects in functional factors and the cognitive interaction: A randomized controlled trial. Physiol. Behav. 2019, 201, 157–164. [Google Scholar] [CrossRef]
- Cavalcante, E.F.; Ribeiro, A.S.; do Nascimento, M.A.; Silva, A.M.; Tomeleri, C.M.; Nabuco, H.C.G.; Pina, F.L.C.; Mayhew, J.L.; Da Silva-Grigoletto, M.E.; da Silva, D.R.P.; et al. Effects of Different Resistance Training Frequencies on Fat in Overweight/Obese Older Women. Int. J. Sports Med. 2018, 39, 527–534. [Google Scholar] [CrossRef]
- Coelho-Júnior, H.J.; de Oliveira Gonçalvez, I.; Sampaio, R.A.C.; Sampaio, P.Y.S.; Cadore, E.L.; Izquierdo, M.; Marzetti, E.; Uchida, M.C. Periodized and non-periodized resistance training programs on body composition and physical function of older women. Exp. Gerontol. 2019, 121, 10–18. [Google Scholar] [CrossRef]
- Correa, C.S.; LaRoche, D.P.; Cadore, E.L.; Reischak-Oliveira, A.; Bottaro, M.; Kruel, L.F.; Tartaruga, M.P.; Radaelli, R.; Wilhelm, E.N.; Lacerda, F.C.; et al. 3 Different types of strength training in older women. Int. J. Sports Med. 2012, 33, 962–969. [Google Scholar] [CrossRef] [PubMed]
- Cunha, P.M.; Nunes, J.P.; Tomeleri, C.M.; Nascimento, M.A.; Schoenfeld, B.J.; Antunes, M.; Gobbo, L.A.; Teixeira, D.; Cyrino, E.S. Resistance Training Performed with Single and Multiple Sets Induces Similar Improvements in Muscular Strength, Muscle Mass, Muscle Quality, and IGF-1 in Older Women: A Randomized Controlled Trial. J. Strength Cond. Res. 2020, 34, 1008–1016. [Google Scholar] [CrossRef]
- Daly, R.M.; Gianoudis, J.; De Ross, B.; O’Connell, S.L.; Kruger, M.; Schollum, L.; Gunn, C. Effects of a multinutrient-fortified milk drink combined with exercise on functional performance, muscle strength, body composition, inflammation, and oxidative stress in middle-aged women: A 4-month, double-blind, placebo-controlled, randomized trial. Am. J. Clin. Nutr. 2020, 112, 427–446. [Google Scholar] [CrossRef] [PubMed]
- de Resende-Neto, A.G.; do Nascimento, M.A.; de Sá, C.A.; Ribeiro, A.S.; Desantana, J.M.; da Silva-Grigoletto, M.E. Comparison between functional and traditional training exercises on joint mobility, determinants of walking and muscle strength in older women. J. Sports Med. Phys. Fit. 2019, 59, 1659–1668. [Google Scholar] [CrossRef]
- de Resende-Neto, A.G.; Andrade, B.C.O.; Cyrino, E.S.; Behm, D.G.; De-Santana, J.M.; Da Silva-Grigoletto, M.E. Effects of functional and traditional training in body composition and muscle strength components in older women: A randomized controlled trial. Arch. Gerontol. Geriatr. 2019, 84, 103902. [Google Scholar] [CrossRef] [PubMed]
- Santos, L.D.; Ribeiro, A.S.; Cavalcante, E.F.; Nabuco, H.C.; Antunes, M.; Schoenfeld, B.J.; Cyrino, E.S. Effects of Modified Pyramid System on Muscular Strength and Hypertrophy in Older Women. Int. J. Sports Med. 2018, 39, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Santos, L.D.; Ribeiro, A.S.; Nunes, J.P.; Tomeleri, C.M.; Nabuco, H.C.G.; Nascimento, M.A.; Junior, P.S.; Fernandes, R.R.; Campa, F.; Toselli, S.; et al. Effects of Pyramid Resistance-Training System with Different Repetition Zones on Cardiovascular Risk Factors in Older Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 6115. [Google Scholar] [CrossRef] [PubMed]
- Francis, P.; Mc Cormack, W.; Toomey, C.; Norton, C.; Saunders, J.; Kerin, E.; Lyons, M.; Jakeman, P. Twelve weeks’ progressive resistance training combined with protein supplementation beyond habitual intakes increases upper leg lean tissue mass, muscle strength and extended gait speed in healthy older women. Biogerontology 2017, 18, 881–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadelha, A.B.; Paiva, F.M.; Gauche, R.; de Oliveira, R.J.; Lima, R.M. Effects of resistance training on sarcopenic obesity index in older women: A randomized controlled trial. Arch. Gerontol. Geriatr. 2016, 65, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Gualano, B.; Macedo, A.R.; Alves, C.R.; Roschel, H.; Benatti, F.B.; Takayama, L.; de Sá Pinto, A.L.; Lima, F.R.; Pereira, R.M. Creatine supplementation and resistance training in vulnerable older women: A randomized double-blind placebo-controlled clinical trial. Exp. Gerontol. 2014, 53, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; Suzuki, T.; Saito, K.; Yoshida, H.; Kobayashi, H.; Kato, H.; Katayama, M. Effects of Exercise and Amino Acid Supplementation on Body Composition and Physical Function in Community-Dwelling Elderly Japanese Sarcopenic Women: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2012, 60, 16–23. [Google Scholar] [CrossRef]
- Letieri, R.V.; Teixeira, A.M.; Furtado, G.E.; Lamboglia, C.G.; Rees, J.L.; Gomes, B.B. Effect of 16 weeks of resistance exercise and detraining comparing two methods of blood flow restriction in muscle strength of healthy older women: A randomized controlled trial. Exp. Gerontol. 2018, 114, 78–86. [Google Scholar] [CrossRef]
- Liao, C.D.; Tsauo, J.Y.; Huang, S.W.; Ku, J.W.; Hsiao, D.J.; Liou, T.H. Effects of elastic band exercise on lean mass and physical capacity in older women with sarcopenic obesity: A randomized controlled trial. Sci. Rep. 2018, 8, 2317. [Google Scholar] [CrossRef] [Green Version]
- Mori, H.; Tokuda, Y. Effect of whey protein supplementation after resistance exercise on the muscle mass and physical function of healthy older women: A randomized controlled trial. Geriatr. Gerontol. Int. 2018, 18, 1398–1404. [Google Scholar] [CrossRef] [Green Version]
- Nabuco, H.C.G.; Tomeleri, C.M.; Junior, P.S.; Fernandes, R.R.; Cavalcante, E.F.; Antunes, M.; Ribeiro, A.S.; Teixeira, D.C.; Silva, A.M.; Sardinha, L.B.; et al. Effects of Whey Protein Supplementation Pre- or Post-Resistance Training on Muscle Mass, Muscular Strength, and Functional Capacity in Pre-Conditioned Older Women: A Randomized Clinical Trial. Nutrients 2018, 10, 563. [Google Scholar] [CrossRef] [Green Version]
- Nabuco, H.C.; Tomeleri, C.M.; Junior, P.S.; Fernandes, R.R.; Cavalcante, E.F.; Nunes, J.P.; Cunha, P.F.; Dos Santos, L.; Cyrino, E.S. Effects of higher habitual protein intake on resistance-training-induced changes in body composition and muscular strength in untrained older women: A clinical trial study. Nutr. Health 2019, 25, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Nabuco, H.C.G.; Tomeleri, C.M.; Fernandes, R.R.; Junior, P.S.; Cavalcante, E.F.; Cunha, P.M.; Antunes, M.; Nunes, J.P.; Venturini, D.; Barbosa, D.S.; et al. Effect of whey protein supplementation combined with resistance training on body composition, muscular strength, functional capacity, and plasma-metabolism biomarkers in older women with sarcopenic obesity: A randomized, double-blind, placebo-controlled trial. Clin. Nutr. ESPEN 2019, 32, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.A.D.; Gerage, A.M.; Silva, D.; Ribeiro, A.S.; Machado, D.; Pina, F.L.C.; Tomeleri, C.M.; Venturini, D.; Barbosa, D.S.; Mayhew, J.L.; et al. Effect of resistance training with different frequencies and subsequent detraining on muscle mass and appendicular lean soft tissue, IGF-1, and testosterone in older women. Eur. J. Sport Sci. 2019, 19, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Rabelo, H.T.; Bezerra, L.A.; Terra, D.F.; Lima, R.M.; Silva, M.A.; Leite, T.K.; de Oliveira, R.J. Effects of 24 weeks of progressive resistance training on knee extensors peak torque and fat-free mass in older women. J. Strength Cond. Res. 2011, 25, 2298–2303. [Google Scholar] [CrossRef] [PubMed]
- Radaelli, R.; Botton, C.E.; Wilhelm, E.N.; Bottaro, M.; Lacerda, F.; Gaya, A.; Moraes, K.; Peruzzolo, A.; Brown, L.E.; Pinto, R.S. Low- and high-volume strength training induces similar neuromuscular improvements in muscle quality in elderly women. Exp. Gerontol. 2013, 48, 710–716. [Google Scholar] [CrossRef]
- Radaelli, R.; Brusco, C.M.; Lopez, P.; Rech, A.; Machado, C.L.F.; Grazioli, R.; Müller, D.C.; Tufano, J.J.; Cadore, E.L.; Pinto, R.S. Muscle quality and functionality in older women improve similarly with muscle power training using one or three sets. Exp. Gerontol. 2019, 128, 110745. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Campillo, R.; Castillo, A.; de la Fuente, C.I.; Campos-Jara, C.; Andrade, D.C.; Álvarez, C.; Martínez, C.; Castro-Sepúlveda, M.; Pereira, A.; Marques, M.C.; et al. High-speed resistance training is more effective than low-speed resistance training to increase functional capacity and muscle performance in older women. Exp. Gerontol. 2014, 58, 51–57. [Google Scholar] [CrossRef]
- Ramirez-Campillo, R.; Diaz, D.; Martinez-Salazar, C.; Valdés-Badilla, P.; Delgado-Floody, P.; Méndez-Rebolledo, G.; Cañas-Jamet, R.; Cristi-Montero, C.; García-Hermoso, A.; Celis-Morales, C.; et al. Effects of different doses of high-speed resistance training on physical performance and quality of life in older women: A randomized controlled trial. Clin. Interv. Aging 2016, 11, 1797–1804. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, A.S.; Aguiar, A.F.; Schoenfeld, B.J.; Nunes, J.P.; Cavalcante, E.F.; Cadore, E.L.; Cyrino, E.S. Effects of Different Resistance Training Systems on Muscular Strength and Hypertrophy in Resistance-Trained Older Women. J. Strength Cond. Res. 2018, 32, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.S.; Schoenfeld, B.J.; Fleck, S.J.; Pina, F.L.C.; Nascimento, M.A.; Cyrino, E.S. Effects of Traditional and Pyramidal Resistance Training Systems on Muscular Strength, Muscle Mass, and Hormonal Responses in Older Women: A Randomized Crossover Trial. J. Strength Cond. Res. 2017, 31, 1888–1896. [Google Scholar] [CrossRef] [PubMed]
- Souza, D.; Barbalho, M.; Vieira, C.A.; Martins, W.R.; Cadore, E.L.; Gentil, P. Minimal dose resistance training with elastic tubes promotes functional and cardiovascular benefits to older women. Exp. Gerontol. 2019, 115, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Strandberg, E.; Edholm, P.; Ponsot, E.; Wåhlin-Larsson, B.; Hellmén, E.; Nilsson, A.; Engfeldt, P.; Cederholm, T.; Risérus, U.; Kadi, F. Influence of combined resistance training and healthy diet on muscle mass in healthy elderly women: A randomized controlled trial. J. Appl. Physiol. 2015, 119, 918–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strandberg, E.; Ponsot, E.; Piehl-Aulin, K.; Falk, G.; Kadi, F. Resistance Training Alone or Combined With N-3 PUFA-Rich Diet in Older Women: Effects on Muscle Fiber Hypertrophy. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 489–494. [Google Scholar] [CrossRef]
- Junior, P.S.; Ribeiro, A.S.; Nabuco, H.C.G.; Fernandes, R.R.; Tomeleri, C.M.; Cunha, P.M.; Venturini, D.; Barbosa, D.S.; Schoenfeld, B.J.; Cyrino, E.S. Effects of Whey Protein Supplementation Associated With Resistance Training on Muscular Strength, Hypertrophy, and Muscle Quality in Preconditioned Older Women. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 528–535. [Google Scholar] [CrossRef]
- Tiggemann, C.L.; Dias, C.P.; Radaelli, R.; Massa, J.C.; Bortoluzzi, R.; Schoenell, M.C.; Noll, M.; Alberton, C.L.; Kruel, L.F. Effect of traditional resistance and power training using rated perceived exertion for enhancement of muscle strength, power, and functional performance. Age 2016, 38, 42. [Google Scholar] [CrossRef] [Green Version]
- Tucci, H.T.; Figueiredo, D.S.; de Paula Carvalho, R.; Souza, A.C.F.; Vassão, P.G.; Renno, A.C.M.; Ciol, M.A. Quadriceps femoris performance after resistance training with and without photobiomodulation in elderly women: A randomized clinical trial. Lasers Med. Sci. 2019, 34, 1583–1594. [Google Scholar] [CrossRef]
- Liguori, G.; Feito, Y.; Fountaine, C.; Roy, B.A. (Eds.) ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2019; p. 157. [Google Scholar]
- de Lange, C. Brazil’s Billion-Dollar Gym Experiment. Available online: https://mosaicscience.com/story/brazils-billion-dollar-gym-experiment/ (accessed on 19 May 2021).
- Spiering, B.A.; Mujika, I.; Sharp, M.A.; Foulis, S.A. Maintaining Physical Performance: The Minimal Dose of Exercise Needed to Preserve Endurance and Strength Over Time. J. Strength Cond. Res. 2021, 35, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Cañete, S.; Juan, A.F.S.; Pérez, M.; Gómez-Gallego, F. Does creatine supplementation improve functional capacity in elderly women? J. Strength Cond. Res. 2006, 20, 22. [Google Scholar] [PubMed]
- Gotshalk, L.A.; Kraemer, W.J.; Mendonca, M.A.; Vingren, J.L.; Kenny, A.M.; Spiering, B.A.; Volek, J.S. Creatine supplementation improves muscular performance in older women. Eur. J. Appl. Physiol. 2008, 102, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Sestili, P.; Martinelli, C.; Colombo, E.; Barbieri, E.; Potenza, L.; Sartini, S.; Fimognari, C. Creatine as an antioxidant. Amino Acids. 2011, 40, 1385–1396. [Google Scholar] [CrossRef] [PubMed]
- Da Boit, M.; Sibson, R.; Sivasubramaniam, S.; Meakin, J.R.; Greig, C.A.; Aspden, R.M.; Thies, F.; Jeromson, S.; Hamilton, D.L.; Speakman, J.R.; et al. Sex differences in the effect of fish-oil supplementation on the adaptive response to resistance exercise training in older people: A randomized controlled trial. Am. J. Clin. Nutr. 2017, 105, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Devries, M.C.; McGlory, C.; Bolster, D.R.; Kamil, A.; Rahn, M.; Harkness, L.; Baker, S.K.; Phillips, S.M. Leucine, not Total Protein, Content of a Supplement Is the Primary Determinant of Muscle Protein Anabolic Responses in Healthy Older Women. J. Nutr. 2018, 148, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Hanson, E.D.; Srivatsan, S.R.; Agrawal, S.; Menon, K.S.; Delmonico, M.J.; Wang, M.Q.; Hurley, B.F. Effects of strength training on physical function: Influence of power, strength, and body composition. J. Strength Cond. Res. 2009, 23, 2627–2637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smee, D.J.; Berry, H.L.; Anson, J.M.; Waddington, G.S. The relationship between subjective falls-risk assessment tools and functional, health-related, and body composition characteristics. J. Appl. Gerontol. 2017, 36, 156–172. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.C.; Marra, C.A.; Robertson, M.C.; Khan, K.M.; Najafzadeh, M.; Ashe, M.C.; Liu-Ambrose, T. Economic evaluation of dose-response resistance training in older women: A cost-effectiveness and cost-utility analysis. Osteoporos. Int. 2011, 22, 1355–1366. [Google Scholar] [CrossRef] [Green Version]

| Databases (Hits) | Key Words Used |
|---|---|
| PUBMED, SPORT DISCUS, CINAHL | (1) strength training; (2) weight training; (3) body weight training; (4) intervention; (5) older women; (6) postmenopausal women; (7) middle-aged women (8) 1 or 2 or 3 or 4 or 5 or 6 or 7 (9) randomized controlled trial; (10) controlled trial; (11) 9 and 10; (12) 9 and 11 (13) Limit 11 and 12 to women (50–70 yearss old) and 2010–2021 and English and humans |
| PICOS Criteria | Inclusion and Exclusion Criteria |
|---|---|
| Participants |
|
| Interventions |
|
| Comparisons |
|
| Outcomes |
|
| Study Design |
|
| [Reference Number] Author(s) (Year) | PS | Study Purpose | Participants (Study Origin, Ethnicity, Age) | Methods | Results |
|---|---|---|---|---|---|
| Aguiar et al. [21] | 7 | Examine the effects of long-term creatine supplementation combined with resistance training on body composition, 1RM, and functional fitness | 18 Brazilian women (64.9 ± 5.0 years) | Double-blind, randomly assigned to creatine (CR; 5 g/d) or placebo (PL) Grp + RT intervention | CR > increased training volume + 1RM bench press, knee ext, biceps curl; CR > efficiency in 30 s chair stand, arm curl, and getting up from floor; CR > FFM and muscle mass; NC in body mass or %BF in either grp |
| Barbalho et al. [22] | 4 | Compare effects of different RT volumes on body comp, muscle strength, and functional fitness of older women | 376 Brazilian women (71.29 ± 5.77 years) | Randomly assigned to 12 wks of low- or high-volume (LV or HV) resistance training | Both groups > in all strength and functional tests and reduced body weight and waist circumference (non-responsiveness not an issue); Compared to LV group, HV group had > gains in 1RM leg press, 30 s arm curls |
| Bocalini et al. [23] | 4 | Investigate the impact of circuit-based exercise on body composition in obese older women | 70 Brazilian women (64 ± 3.67 years) | Randomized into six groups by BMI (appropriate wt (AW), control AWC), trained AWT, overweight (OW), OWC, OWT, obese (OB), OBC, OBT | Changes > in OB in %BF, lean mass and fat mass vs. AWT and OWT; no diffs in C groups; Circuit training is effective for promoting < in anthropometric parameters, especially > in LBM |
| Carneiro et al. [24] | 4 | Analyze the effect of resistance training (RT) performed at different weekly frequencies on body comp and flexibility in older women | 53 Brazilian women (67.3 ± 5.45 years) | Randomly assigned to perform RT either 2x/wk (G2) or 3x/wk (G3) | Compared to G2, G3 had > increase in frontal hip flexion; Both grps > cervical extension, right hip flexion and left hip flexion (NS diffs); NS diff in muscle mass |
| Carrasco-Poyatos et al. [25] | 3 | Compare effect of two different training interventions on body comp and functional fitness in older women | 60 Spanish women (68.92 ± 4.42 years) | Block randomization used to assign participants to Pilates group (PG), RT group (RT) and control group (CG) | PG > functional fitness more than RT and CG; LBM > in PG and RT; RT > static balance |
| Cavalcante et al. [26] | 5 | Compare the effect of different RT frequencies on total, android, gynoid and trunk body fat in overweight/obese older women | 57 OW/OB Brazilian women (66.9 ± 5.3 years) | Randomly assigned to 2x/wk RT (2X), 3x/wk RT (3X) or control non-exercise (CG) | Both 2X and 3X had significant < in adiposity compared to CG (total %BF, android fat, gynoid fat and trunk fat with greatest < in android region); NS diffs in adiposity between training groups; flexible approach to training may > adherence |
| Coelho-Junior et al. [27] | 6 | Compare a daily undulating periodization (DUP) intervention, combining resistance training (RT) + power training (PT) with non-periodized RT (NP) and control (CG) for improvements in body composition and physical function in older women | 42 women from Brazil, Italy and Spain (66.8 ± 5.4 years) | Randomized into NP, DUP or control group (CG) | NS changes in body comp in any group; Compared to baseline, NP group improved countermovement jump, timed up and go, walking speed and one-leg stand; DUP only improved timed up-and-go test |
| Correa et al. [28] | 5 | Evaluate and compare adaptations of older women who participated in three types of strength training | 58 women from Brazil and the USA (67 ± 5 years) | Randomized to experimental (n = 41) and control (CG n = 17) First 6 wks = traditional strength training for lower extremities; next EG divided into three grps: traditional group (TG), power group (PG) (concentric phase of contraction at high speed) and rapid strength group (RG) (lateral box jump exercise) | After 1st 6 wks, compared to CG, EG had > 1RM knee extension, knee extensor muscle thickness, and maximal muscle activation; next 6 weeks, 1RM > similarly and sig, as did muscle thickness of vastus lateralis (VL) and activation of VL and vastus medialis; reaction time, 20 s chair stand and CMJ > only in RG |
| Cunha et al. [29] | 4 | Compare single set vs. multiple sets of resistance training (RT) in untrained healthy older women | 62 Brazilian women: control (69.03 ± 4.92 years) | Randomized to single set RT (SS, 1 set), multiple set RT (MS, 3 sets), or non- training control (NC) | Compared to NC, SS and MS > 1RM in upper and lower body; also > muscle quality, muscle mass; Gains similar for SS and MS groups; SS may be sufficient for short-term gains but longer-duration trials needed |
| Daly et al. [30] | 4 | Evaluate whether a multi-nutrient-fortified milk drink (MFMD) could enhance effects of exercise on body comp and functional muscle power | 244 Australian women (55.5 ± 5 years) | Double-blind, placebo-controlled randomized trial: Ex + MFMD or Ex + PL; supplemental dry powder: 30 g twice daily + 150 mL of cold water in a plastic shaker | Compared to EX + PL, EX + MFMD had > improvement in LBM, FM, muscle CSA and CMJ; NS diff in muscle strength; both groups improved 5 and 10 step stair ascent power |
| de Resende-Netro et al. [31] | 5 | Compare the effects of 12 week functional and traditional training on joint mobility, gait, and muscle strength, and verify the maintenance of effects after 8 wks detraining in older women | 52 Brazilian women (64.7 ± 4.33 years) | Randomized into three groups functional training (FT), traditional training (TT) and stretching control (SC); 12 weeks training followed by 8 weeks de-training w/post measurement | Compared to SC, FT and TT improved muscle strength and power after 12 wks; only FT showed improvement in walking ability and gait; Muscle power gains partially sustained after 8 wk de-training period for both FT and TT |
| de Resende-Netro et al. [32] | 5 | Investigate whether functional training has similar effects to traditional training on body comp, muscle strength and power in older women | 47 Brazilian women (64.84 ± 4.32 years) | Randomized and crossover clinical trial with block randomization into 3threegroups: functional training (FT), traditional training (TT) or stretching control (SC) | FT < %BF; trad > LM, but no statistically significant difference in body composition; Both FT and TT > muscle strength and power whereas stretching saw < muscle strength. |
| dos Santos et al. [33] | 5 | Analyze the effects of a pyramid system performed with two repetition zones (narrow and wide) on body comp and muscular strength in older women | 39 physically independent older women from Spain (67.8 ± 5.4 years) | Randomly assigned to RT intervention which completed 3 sets—one with 12/10/8 (narrow reps (NR)) and one with 15/10/5 (wide reps (WR)) | Both NR and WR groups > skeletal muscle mass and strength; but NS diff between two interventions. |
| dos Santos et al. [34] | 5 | Analyze the effects of the pyramidal resistance training system with two repetition zones on body comp and cardiovascular risk factors in older women | 59 Spanish women (67.3 ± 4.4 years) | Randomly assigned to three groups: non-exercise control (CON), narrow pyramid reps (NP: 12/10/8) and wide pyramid reps (WP: 15/10/5) | Compared to CON, NPR and WPR reduced %BF (mostly android) and improved glucose, HDL-C, LDL-C and C-reactive protein. |
| Francis et al. [35] | 4 | Compare the effects of RT and protein supplementation (RT + PRO) to PRO on upper-leg lean tissue mass, muscle quality and functional capacity | 57 Irish women (61.1 ± 5.1 years) | Single-blinded, randomized, controlled design; All women consumed 0.33 g/kg milk-based protein for 12 weeks; 29 of 57 also engaged in progressive resistance training (PRT) | Compared to PRO alone, PRO + RT > upper-leg lean tissue mass, knee extensor torque, extended gait speed |
| Gadelha et al. [36] | 3 | Examine the effects of RT on sarcopenic obesity in older women | 243 women from Brazil (67.27 ± 5.04 years) | Random assignment to control group (CG) or RT group | RT > FFM but did not decrease fat mass; sarcopenic obesity index was improved in RT group, but < in CG |
| Gualano et al. [37] | 6 | Examine the efficacy of creatine supplementation, associated or not with resistance training, in older women | 60 women from Brazil (65.78 ± 5 years) | Double-blind, randomized, placebo-controlled trial with 4 comparison groups: placebo (PL), creatine only (CR only), placebo with resistance training (PL+RT) or creatine with resistance training (CR+RT) | CR+RT group had greater appendicular LM accrual vs. PL, CR or PL+RT groups; CR and PL+RT groups had comparable gains in appendicular lean mass, which were superior to PL; Changes in FM did not differ between groups; 1RM leg press > in CR+RT vs. PL- and CR-only groups, but not vs. PL+RT group; CR+RT group > 1RM bench press vs. other groups |
| Kim et al. [38] | 4 | Evaluate the effectiveness of RT + amino acid supplementation in enhancing muscle mass and strength in older sarcopenic women | 155 Japanese women > 75 y | RCT with four groups: exercise + amino acid (EX + AA), exercise only (EO), amino acid only (AAO) or health education (CTRL); AA = 3 g of leucine-rich AA 2 x a day for 12 wks | LBM > only in EX + AA and EO; 1RM Knee Ext > only in EX + AA; walk speed > in 3 intervention groups |
| Letieri et al. [39] | 6 | Compare the effect of RT using different occlusion pressures, followed by 6 wks detraining on the muscular strength levels of older women | 56 recreationally active women from Brazil (68.8 ± 5.09 years) | Randomized controlled trial of 16 wks RT + 6 wks detraining; randomized into 5 groups: low-intensity w/ high blood flow restriction (LI+BFR_H); low-intensity with low blood flow restriction (LI+BFR_L), high-intensity (HI); low-intensity (LI); and control group (CG) | Maximal isokinetic torque of right- and left-knee extension and flexion was higher in LI+BFR_H, LI+BFR_L and HI groups; following 6 wks detraining, LI+BFR_H and LI+BFR_L saw a decrease in strength, but values did not decrease below baseline levels |
| Liao et al. [40] | 4 | Investigate the effect of elastic band resistance training (ERT) on muscle mass and physical function in older women | 56 women from Taiwan with sarcopenia or obesity (67.3 ± 5.1 years) | RCT with assignment to ERT or control (CTL) | Compared to CTL, ERT > increased LBM, muscle quality, physical capacity and physical outcomes |
| Mori et al. [41] | 4 | Evaluate the effectiveness of whey PRO, ingested after resistance exercise, in increasing muscle mass and physical function among older women | 81 Japanese women (70.6 ± 4.3 years) | RCT with three groups: Exercise + PRO (1.2 g/kg body mass+) (EX+PRO), exercise-only group (EX), protein-only group (PRO) | Gains in Muscle mass, grip strength, and gait speed were higher in EX+PRO than in EX or PRO and muscle mass gains were higher in EX vs. PRO |
| Nabuco et al. [42] | 5 | Investigate the effects of whey protein (WP) supplementation (35 g) consumed either immediately pre or post RT on muscle mass, muscular strength and functional capacity in pre-conditioned older women | 70 older women from Brazil | Randomly assigned to: whey protein pre-RT and placebo post-RT (WP-PL), placebo pre-RT and WP post-RT (PL-WP), or placebo pre and post (PL) | Compared to PL, WP-PL and PL-WP had greater increases in strength and muscle mass; supplement timing not important |
| Nabuco et al. [43] | 2 | Evaluate the effects of higher PRO intake on RT induced changes in body composition and strength in untrained postmenopausal women | 70 Brazilian women (68.46 ± 4.87 years) | RT intervention with women separated into tertiles of pre-existing PRO intake [low PI (≤0.77 g/kg/day), medium PI (>0.77–≤1.0 g/kg/day) and high PI (>1.0 g/kg/day)] | Compared to low PRO, high PRO intake > muscle mass, preacher curl weight and total strength improvement; compared to mod PRO intake, high PRO > muscle mass |
| Nabuco et al. [44] | 6 | Analyze the effects of whey protein (WP) supplementation and RT on body composition, muscular strength, functional capacity in older women with sarcopenic obesity (SO) | 26 sarcopenic (appendicular lean soft tissue (ALST) < 15.02) obese (Fat Mass > 35%) Brazilian women (69 ± 4 years) | Randomly assigned to receive daily, either 35 g WP (WP group) or placebo (PL), combined with supervised 12-wk RT | Compared to PL, WP had > ALST and < total and trunk fat mass; both groups improved muscular strength and functional capacity |
| Nascimento et al. [45] | 4 | Analyze the effect of RT frequency on muscle mass and changes with detraining in older women | 45 physically independent older women from Brazil (68.5 ± 5.15 years) | Randomly assigned to perform 12 wks of RT either two (G2X) or three (G3X) times per week | Muscle mass and appendicular lean soft tissue significantly increased post-training in both G2X and G3X with no differences between groups; gains were retained after detraining |
| Rabelo et al. [46] | 4 | Examine the effects of resistance training on knee extensors peak torque and fat-free mass in older women | 154 Brazilian women (67.1 ± 5.9 years) | RT grp vs. control | RT grp > knee extensor peak torque and FFM vs. CTL; RT > appendicular (sum of both arms and legs FFM) FFM > compared to CG |
| Radaelli et al. [47] | 3 | Compare the effects of low- and high-volume strength training on strength, muscle activation and muscle thickness of the lower and upper body and on muscle quality of the lower body in older women | 20 Brazilian women (range 60–74 years; mean age not provided) | Randomly assigned to low- (LV = 1 set) and high-volume (HV = 3 sets) groups | Both groups > 1RM knee extension and isometric max strength of the lower body and upper body; Both groups > max electromyographic activation in the vastus medialis and biceps brachii; all muscle thickness measurements of the lower and upper body increased similarly in both groups |
| Radaelli et al. [48] | 5 | Compare the effects of 1 or 3 sets of muscle power training on muscle quality, power and functional capacity | 26 Brazilian women (60–77 years; mean age not provided) | Randomly assigned into two groups: 1SET and 3SETS | Both groups had significant and similar increases in muscle power, vertical jump height, and functionality |
| Ramirez-Campillo et al. [49] | 4 | Examine the effects of 12 weeks of high-speed resistance training (HS RT) versus low-speed RT (LS RT) on muscle strength, muscle power, functional performance | 45 Hispanic women (67.23 ± 5 years) | Randomly assigned into HS RT, LS RT and control groups | Both HS RT and LS RT > strength, with NS differences; Both RT groups > power, but HS RT had greater changes in ball throwing and 10 m walking sprint; HS RT > 8 ft up and go and sit to stand vs. LS RT. |
| Ramirez-Campillo et al. [50] | 4 | Compare the effects of two frequencies (2 vs. 3 sessions per week), equated for volume and intensity) of high-speed resistant training (HS RT) on physical performance in older women | 24 women (70.27 ± 6.9 years) | Randomized into HS RT intervention composed of either 2 (RT2) or 3 (RT3) sessions per week (equated for volume and intensity) or into a control group | Compared with control group, both training groups > muscle strength, power, and functional performance |
| Ribeiro et al. [51] | 4 | Investigate the effect of RT performed in a pyramid (PR) vs. constant (CT) load system on muscular strength and hypertrophy in older women | 33 women from Brazil and USA (69.7 ± 5.9 years) | Randomized into two groups: RT + PR or RT + CT load | Both groups > 1RM Chest press and muscle mass without differences between groups; PR is not superior to CT for inducing improvements |
| Riberio et al. [52] | 5 | Investigate the effect of RT performed on a pyramid (PR) versus traditional (TD) system on muscular strength and muscle mass in older women | 25 women (67.6 ± 5.1 years) | Women performed both a PR and TD RT intervention in a balanced crossover design | Significant > observed in both groups for muscular strength in 1RM chest press, knee extension, preacher curl and for skeletal muscle mass with no diffs between groups |
| Souza et al. [53] | 4 | To compare the effect of conventional RT (CRT) to elastic band RT (ERT) on functional fitness | 21 Brazilian women (66 ± 6.0 years) | Randomly assigned to CRT or ERT | CRT > 6 min walk vs. ERT |
| Strandberg et al. [54] | 4 | Evaluate the effects of RT + healthy dietary approach in healthy and physically active older women | 55 Swedish women (65–70 years; no mean age given) | Three-arm randomized controlled trial: RT + healthy diet group (RT + HD), RT only (RT), or control (CTL) | 1RM leg extension and maximal isometric quadriceps strength > in RT + HD and RT but not in CTL; Lean leg mass > only in RT-HD |
| Strandberg et al. [55] | 4 | Examine changes in skeletal muscle of older women in response to combined RT and N-3 PUFA-rich healthy diet | 63 Swedish women (ages 65–70 years) | Three-arm randomized control trial: RT + N-3 PUFA (RT+HD), RT only (RT) or CTRL | Hypertrophy of fast twitch TIIA muscle fibers in RT-HD only |
| Sugihara et al. [56] | 5 | Investigate the effect of whey protein (WP) supplementation on muscular strength, hypertrophy and muscle quality in older women preconditioned to RT | 31 Brazilian women (67.4 ± 4.0 years) | Randomized double-blind placebo into WP (35 g) + RT or PLA + RT | Both groups > skeletal muscle mass and total strength; WP + RT had > increases compared with PLA + RT; muscular quality > in both groups without statistical differences |
| Tiggemann et al. [57] | 4 | Compare the effects of traditional resistance training and power training to determine impact of training intensity on improvements in strength, muscle power, and ability to perform functional tasks in older women | 30 women (60–75 years; no mean age given) | Random assignment to traditional resistance training (TRT) or power training group (PT) | Maximal dynamic strength muscle strength for leg press and knee extension, muscle power, and functional fitness > significantly and similarly in both groups after training |
| Tucci et al. [58] | 6 | Examine if quadriceps femoris muscle performance of older women can be improved by applying photobiomodulation therapy after a RT intervention | 45 sedentary women (>60 years) classified as active or insufficiently active | Randomized controlled trial with assignment into quadriceps femoris RT plus active group (RT + active) or placebo group (RT + placebo) or a control group (CTL) | No diffs among three groups in fatigue index for vastus medialis, rectus femoris and vastus lateralis; RT + active improved fatigue indexes while the other groups did not; both training groups improved 1RM; quadriceps femoris performance of older women was not improved when photobiomodulation was added to the RT intervention |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ransdell, L.B.; Wayment, H.A.; Lopez, N.; Lorts, C.; Schwartz, A.L.; Pugliesi, K.; Pohl, P.S.; Bycura, D.; Camplain, R. The Impact of Resistance Training on Body Composition, Muscle Strength, and Functional Fitness in Older Women (45–80 Years): A Systematic Review (2010–2020). Women 2021, 1, 143-168. https://0-doi-org.brum.beds.ac.uk/10.3390/women1030014
Ransdell LB, Wayment HA, Lopez N, Lorts C, Schwartz AL, Pugliesi K, Pohl PS, Bycura D, Camplain R. The Impact of Resistance Training on Body Composition, Muscle Strength, and Functional Fitness in Older Women (45–80 Years): A Systematic Review (2010–2020). Women. 2021; 1(3):143-168. https://0-doi-org.brum.beds.ac.uk/10.3390/women1030014
Chicago/Turabian StyleRansdell, Lynda B., Heidi A. Wayment, Nanette Lopez, Cori Lorts, Anna L. Schwartz, Karen Pugliesi, Patricia S. Pohl, Dierdra Bycura, and Ricky Camplain. 2021. "The Impact of Resistance Training on Body Composition, Muscle Strength, and Functional Fitness in Older Women (45–80 Years): A Systematic Review (2010–2020)" Women 1, no. 3: 143-168. https://0-doi-org.brum.beds.ac.uk/10.3390/women1030014