

Abstract
Objective. To compare the clinical features and outcome between patients with juvenile psoriatic arthritis (JPsA) and non-JPsA juvenile idiopathic arthritis (JIA).
Methods. Fifty-three children with JPsA, 32 with < 5 joints in the first 6 months of disease (oligo–JPsA) and 21 (≥ 5 joints) polyarticular-onset (poly-JPsA) were compared to 53 patients with JIA who were matched by sex, age, date of diagnosis, and articular onset pattern.
Results. There was no difference in the percentage of patients between the oligoarticular groups who developed extended oligoarthritis or in the percentage of patients who were positive for antinuclear antibodies. The only differences were that 25% of patients with oligo-JPsA had dactylitis compared to 0% of patients with oligo-JIA (p < 0.01) and 50% had nail pitting as compared to 18.7% (p < 0.05). In polyarticular patients the percentages with dactylitis were similar (19% vs 38%; p = 0.25). The frequency of uveitis was identical in the oligoarticular patients but a higher rate was seen in poly-JPsA compared to poly-JIA (23.8% vs 0%; p = 0.02), while contractures were more frequent in poly-JIA compared to poly-JPsA during the course of the illness (47.6% vs 14.3%; p = 0.03) but not at last followup (14.3% vs 4.7%; p = 0.6). At last followup the mean Childhood Health Assessment Questionnaire scores were similar in both the polyarticular and oligoarticular groups.
Conclusion. There were only a few differences between patients with JPsA and JIA regarding disease onset, disease course, and outcome. We suggest that large, longterm prospective studies are required to accurately determine whether subdividing JIA according to psoriasis is worthwhile.
In 1962 Ansell and Bywaters first described juvenile psoriatic arthritis (JPsA) as a distinct clinical entity, defined as a chronic inflammatory arthritis, beginning before the age of 16 years, and associated with psoriasis1. The psoriasis may have preceded the onset of arthritis, occurred at the same time as arthritis, or followed the onset of arthritis within 15 years. This definition was used until new classification criteria, the “Vancouver Criteria,” were proposed in 19892. The Vancouver criteria were used until 1997, when they were superseded by the International League Against Rheumatism (ILAR) criteria, which were later refined in 20013,4. The justification for the designation of JPsA as a distinct subtype of juvenile idiopathic arthritis (JIA) is based on previous observations that patients with JPsA have a form of JIA that differs both in its clinical manifestations and in its outcome, and the observation that adults with psoriatic arthritis (PsA) differ from adults with rheumatoid arthritis2,5,6.
Patients with oligoarticular-onset JPsA have been reported to differ from patients with oligoarticular-JIA in the pattern of joint involvement, with small joints of the hands and feet more commonly involved in JPsA than other types of JIA7. In addition, it has been reported that patients with oligoarticular-onset JPsA will more commonly develop polyarthritis than patients with oligoarticular JIA6,8. However, others have questioned whether the pattern of joint involvement was useful in discriminating between patients with JPsA and nonpsoriatic subtypes of JIA and whether these were truly distinct clinical entities; one previous report demonstrated a similar rate of extension9,10. Patients with polyarticular-onset JPsA tend to be older and more prone to develop contractures and longterm disability as compared to patients with oligoarticular-onset JPsA2,5,11.
These data suggest that JPsA and nonpsoriatic JIA may have very similar features. To date there has been only one report that directly compared cohorts of patients with JPsA and other forms of JIA7. However, that study only compared patients with oligoarticular-onset JPsA to nonpsoriatic JIA. The aim of our study was to compare the clinical findings, pattern of disease, and outcome between children with nonpsoriatic subtypes of JIA and JPsA, and to determine how similar or different these subtypes of JIA are.
MATERIALS AND METHODS
The charts of 65 patients who met the Vancouver criteria (definite or probable)2 or ILAR criteria4 for JPsA and who were diagnosed and followed at the Rheumatology Clinic at the Hospital for Sick Children, Toronto, between 1985 and 2005 were randomly selected by their identification number from our database. The 65 charts represented a random sample of the total cohort of 122 patients with JPsA followed at the hospital. Seven of the 65 patients were eliminated from further study as they met the definition for more than one ILAR subset: 3 were rheumatoid factor (RF)-positive and 4 had enthesitis in addition to arthritis. The total number of eligible patients with JPsA was therefore 58 (34 with oligoarticular-onset and 24 with polyarticular-onset JPsA). We then searched the hospital rheumatology database to match the 34 patients with oligoarticular-onset and 24 patients with polyarticular-onset JPsA to patients with oligoarticular-onset or polyarticular-onset subtypes of JIA. The hierarchy for matching of each patient with JPsA to a patient with JIA was (1) sex; (2) age at diagnosis; and (3) date of diagnosis matched for month and year. The matching of onset type and sex was mandatory and the matching for month and year was as close as possible. JIA patients with RF-positive polyarticular JIA, enthesitis-related arthritis (ERA), or systemic arthritis or who fit the criteria for more than 1 category of JIA were excluded. We then eliminated 12 patients with JIA who were subsequently found to have a first-degree relative with psoriasis. One patient with definite psoriasis, who met the Vancouver criteria, was eliminated as he was HLA-B27-positive and was a boy > 6 years old (who fulfilled criteria for both PsA and ERA) and therefore was unclassifiable according to ILAR criteria. Following these inclusion and exclusion criteria and the hierarchical requirement, a further 5 patients with JPsA were eliminated as we were unable to find an appropriate control patient with JIA. The JPsA and nonpsoriatic JIA cohorts therefore each consisted of 52 patients: 31 with oligoarticular arthritis in the first 6 months from disease diagnosis and 21 with polyarticular arthritis.
Data collection
Patients’ charts were reviewed at presentation and at 1, 3, 6, 12, 36, and 60 months following the first presentation and every 5 years thereafter. The following clinical variables at presentation and at each defined followup visit were obtained: joint involvement, presence or absence of symmetric arthritis, nail pitting (defined as more than 1 nail pit at any clinical visit), dactylitis (swelling of 1 or more fingers that extend beyond the joint margin), presence of psoriatic rash (diagnosed by either rheumatology or dermatology), and uveitis (diagnosed by an ophthalmologist). All medications including joint injections were obtained for each visit. Serologic variables studied were (1) RF as detected by latex agglutination; a positive test result was defined as titer ≥ 1:2 on at least 2 occasions ≥ 3 months apart (data were available on 77% of patients with JPsA and 71% with nonpsoriatic JIA); (2) antinuclear antibody (ANA) as detected by immunofluorescent microscopy using the Hep-2 cell line. A positive result was defined as a titer ≥ 1:40 on at least 1 occasion (data were available on 85% of patients with JPsA and 90% with nonpsoriatic JIA); and (3) HLA-B27 antigen (data were available on 42% of patients with JPsA and 25% with nonpsoriatic JIA).
The following complications were recorded at each visit: presence of joint contracture, and presence of leg-length discrepancy. Childhood Health Assessment Questionnaire (CHAQ)12 assessment was available at last followup in 74% of the patients (77% with JPsA and 71% with nonpsoriatic JIA). For patients with uveitis the final vision acuity and complications were obtained as per our previous study13.
Definitions
Symmetric arthritis was defined as present if the number of affected joint pairs divided by the total number of joints involved was ≥ 50%. The following 11 joint pairs were used: shoulders, elbows, wrists, any metacarpophalangeal (MCP) joint involvement (number or location did not need to match), any proximal interphalangeal (PIP) joint involvement of the hand (number or location did not need to match), hips, knees, ankles, any metatarsophalangeal joint involvement (number or location did not need to match) of the foot, any PIP joint involvement of the foot (number or location did not need to match), and the temporomandibular joint. These definitions have been used in previous adult and pediatric studies14,15.
Inactive disease was defined as absence of clinically evident synovitis for a minimum of 3 months. Patients may have been receiving medication at the time of meeting the criteria for inactive disease.
Statistical methods
All descriptive data were expressed as the mean ± standard deviation (SD). Comparisons between matched pairs were performed using McNemar’s test for categorical variables and paired T-test for continuous variables. Kaplan-Meier survival analysis for time to first remission, either on or off therapy, was compared between the groups and the p value was calculated using log-rank chi-squared test.
Institutional review board approval was obtained for our study (no. 0019980177).
RESULTS
The cohort consisted of 52 patients with JPsA: 47 patients with definite and 5 patients with probable JPsA by the Vancouver criteria. All patients who met the Vancouver criteria for JPsA also fulfilled the ILAR criteria for JPsA. The clinical features determining the classification of patients as JPsA are presented in Table 1. Forty-four patients had a definite psoriatic rash and one patient had a psoriatic-like rash.
Clinical features determining the classification of patients as either juvenile psoriatic arthritis (JPsA) or nonpsoriatic juvenile idiopathic arthritis (JIA). Values are number of patients (%).
At the time of the first visit 30 patients fulfilled the Vancouver criteria, with 26 patients having definite and 4 patients probable JPsA. The same 30/52 patients fulfilled the ILAR criteria. The mean time from onset of arthritis to diagnosis of JPsA in the 23 patients who were not diagnosed in the first visit was 2.7 ± 3.7 years (range 2 months to 16.5 yrs) to meet the Vancouver criteria and 3.2 ± 3.8 years (range 2 months to 16.5 yrs) to meet the ILAR criteria.
Oligoarticular groups
There were 25 girls and 6 boys in the oligoarticular groups of JPsA and nonpsoriatic JIA patients. There was no statistically significant difference in the age at time of diagnosis of arthritis and length of followup between the 2 groups (Table 2). We did not find any statistically significant difference in the number of patients who progressed to a polyarticular course or in the time to extension between the groups (Table 2). There was no difference in the number of patients who were ANA or HLA-B27-positive (Table 2). However, dactylitis was significantly more common in the JPsA group as compared to the nonpsoriatic JIA group (25.0% vs 0%; p < 0.01). None of the patients with dactylitis had nail pitting. Nail pitting was more commonly seen in patient with JPsA compared to patients with nonpsoriatic JIA (50.0% vs 18.7%; p < 0.05).
Characteristics of patients with juvenile psoriatic arthritis (JPsA) and nonpsoriatic juvenile idiopathic arthritis (JIA).
Comparing the joint involvement, we did not find any statistically significant differences in the frequencies of individual joint involvement at presentation or during followup between the 2 groups (Table 3). However, there was a trend for more frequent PIP but not MCP involvement (31.2% vs 15.6%; p = 0.09 and 15.6% vs 9.3%, respectively; p = 0.47) in the JPsA group compared to the nonpsoriatic JIA group. When we considered involvement of any small joint of the hand or foot again we did not see any statistically significant difference in the percentage of patients with small joint involvement between the groups (Table 3). Although both cervical spine and distal interphalangeal (DIP) involvement were rarely seen, they were exclusively seen in patients with JPsA and not those with nonpsoriatic JIA. There was a trend toward a higher percentage of patients to have DIP involvement in the JPsA group compared to the nonpsoriatic JIA group (9.3% vs 0%; p = 0.08). There was no difference in the number of patients with JPsA and nonpsoriatic JIA who had symmetric joint involvement (15/32 vs 16/32, respectively; p = 0.6).
Frequency of individual joint involvement at presentation and at any time during course of disease.
Treatment
All of the children in our series were treated with nonsteroidal antiinflammatory drugs (NSAID). Methotrexate was the most commonly prescribed second-line drug and was used at a similar rate in patients with JPsA and nonpsoriatic JIA: 7/32 patients (21.8%) in the JPsA group compared to 6/32 (18.7%) patients in the nonpsoriatic JIA group (p = 0.76). We could not compare the differences in the use of any of the other second-line medications due to small numbers of patients treated with azathioprine, hydroxychloroquine, sulfasalazine, and leflunomide. There was no difference in the use of anti-tumor necrosis factor-α therapy or prednisone between the groups (3.1% vs 6.2%).
Outcome measures
We did not find any statistically different frequency in the presence of contractures at any time during the followup period (6.2% of the patients with JPsA compared to 18.7% in the nonpsoriatic JIA group; p = 0.10) or in the percentage of patients with a contracture at last visit (3.1% vs 6.2% of the patients, respectively; p = 1.0; Table 4). A leg-length discrepancy at last followup was present in 15.6% of the patients in both groups (Table 4).
Medication use during course of disease.
At last followup, the mean CHAQ scores were similar between patients with JPsA and nonpsoriatic JIA (0.137 ± 0.33 vs 0.1 ± 0.29, respectively; p = 0.7).
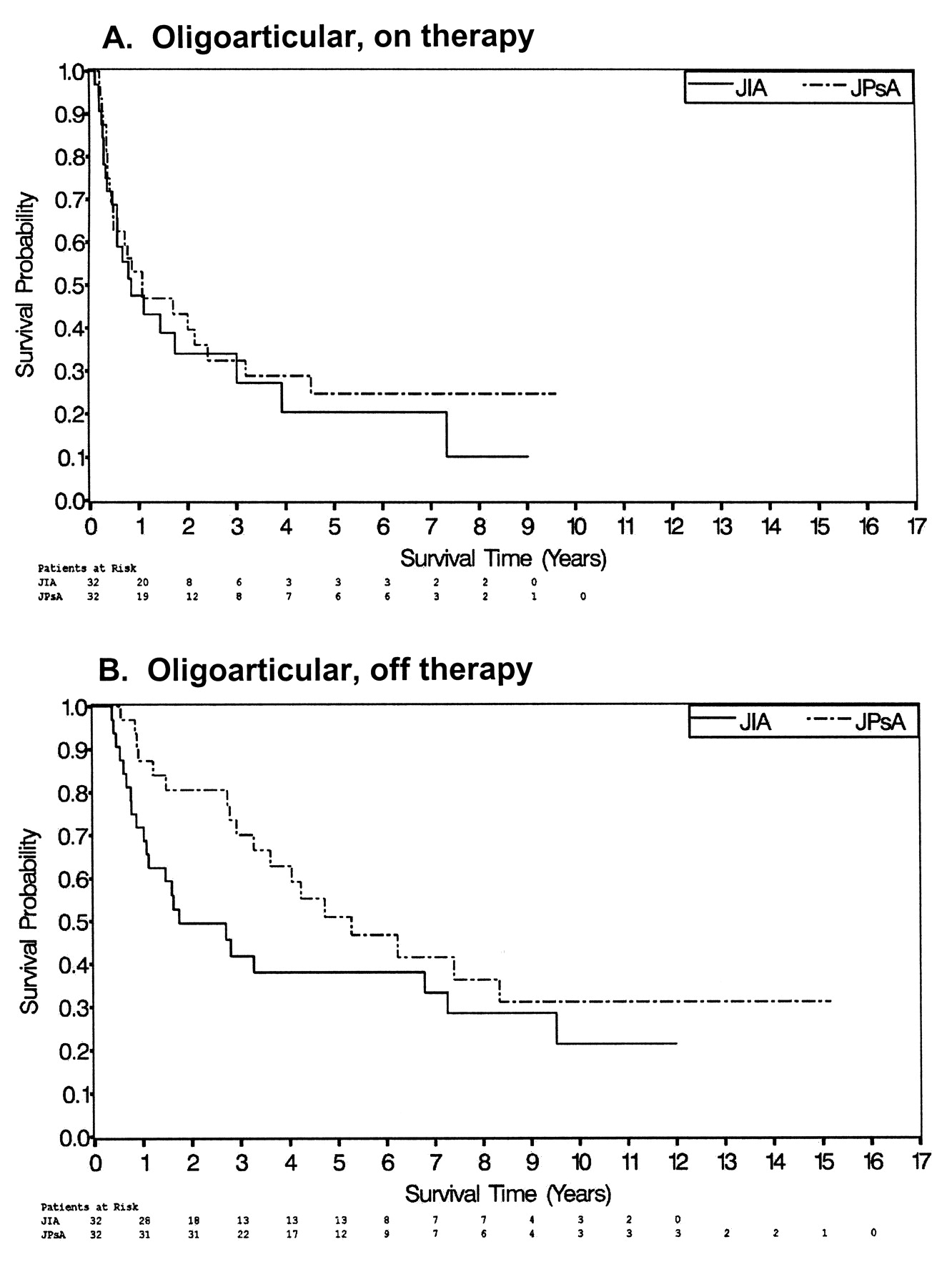
The number of patients with inactive disease, either on or off therapy, did not differ between patients with JPsA or nonpsoriatic JIA (75% vs 63%, respectively, for patients on therapy; p = 0.7; and 56% vs 62%, respectively, for patients off therapy; p = 0.5). Using Kaplan-Meier survival analysis, there was no difference in the mean time to first inactive disease on therapy between oligoarticular-onset groups (2.0 ± 0.32 yrs for JPsA patients and 2.4 ± 0.57 yrs for nonpsoriatic JIA patients; p = 0.55) and to remission off therapy (4.2 ± 0.7 for JPsA patients and 5.2 ± 0.5 yrs for nonpsoriatic JIA patients; p = 0.10).
Polyarticular-onset groups
There were 16 girls and 5 boys in each polyarticular-onset group. There was no statistically significant difference in the age at the time of diagnosis of arthritis or length of followup between the patients with JPsA and nonpsoriatic JIA (Table 2). There was no difference in the number of patients who were ANA or HLA-B27-positive between the groups. There was no significant difference in the percentage of patients with dactylitis at presentation or during followup between patients with polyarticular-onset JPsA and nonpsoriatic JIA (38.0% vs 19.0%; p = 0.25; and 19.0% vs 4.8%, respectively; p = 0.12; Table 2). Nail pitting was more commonly seen in patients with JPsA compared to patients with nonpsoriatic JIA (57.0% vs 4.8%; p < 0.001).
When comparing the pattern of joint involvement between the 2 groups, patients with JPsA were less likely than patients with nonpsoriatic JIA to have hip involvement only during the followup period (28.6% vs 66.7%; p = 0.04) but not at presentation (14.3% vs 38.0%; p = 0.12). There was no significant difference between the 2 groups for involvement of any of the other joints (Table 3). The majority of patients in both groups had symmetric joint involvement (90.5% for JPsA and 95.5% for nonpsoriatic JIA; p = 1.0).
Treatment
All of the children in our series were treated with NSAID at presentation and/or during followup. Methotrexate was the most common second-line drug and was used at similar rates in patients with JPsA and those with nonpsoriatic JIA (62.0% and 71.4%, respectively; p = 0.56). Similarly, there was no significant difference in the use of any other medication (data not shown).
Outcome measures (Table 5)
Comparison of outcome measures in patients with juvenile psoriatic arthritis (JPsA) and nonpsoriatic juvenile idiopathic arthritis (JIA).
Patients with JPsA were significantly less likely than patients with nonpsoriatic JIA to have a contracture during the disease course, but there was no significant difference between the groups at last followup (66.7% vs 28.6%; p = 0.04; and 4.7% vs 14.3%, respectively; p = 0.6). One patient in the nonpsoriatic JIA group required a hip arthroplasty but none in the JPsA group. A leg-length discrepancy at last followup was found in only 1 patient with JPsA and none with nonpsoriatic JIA. At last followup, the mean CHAQ scores were similar between the 2 groups, at 0.19 ± 0.30 for the patients with JPsA and 0.18 ± 0.29 for the patients with JIA (p = 0.32).
The number of patients with inactive disease, either on or off therapy, did not differ significantly between the groups, at 81% for the patients with JPsA and 85% for those with nonpsoriatic JIA (p = 1.0) for patients with inactive disease receiving therapy, and 19.0% versus 38.0%, respectively (p = 0.28), for patients with inactive disease off therapy (Figure 1). Similar to the findings with the oligoarticular-onset group, using Kaplan-Meier survival analysis, there was no difference in the mean time to first inactive disease, on therapy at 4.1 ± 1.0 years for patients with polyarticular JPsA and 3.6 ± 0.8 years for patients with nonpsoriatic JIA (p = 0.68) and off therapy at 5 ± 0.4 and 5 ± 0.4 years, respectively (p = 0.23; Figure 2).
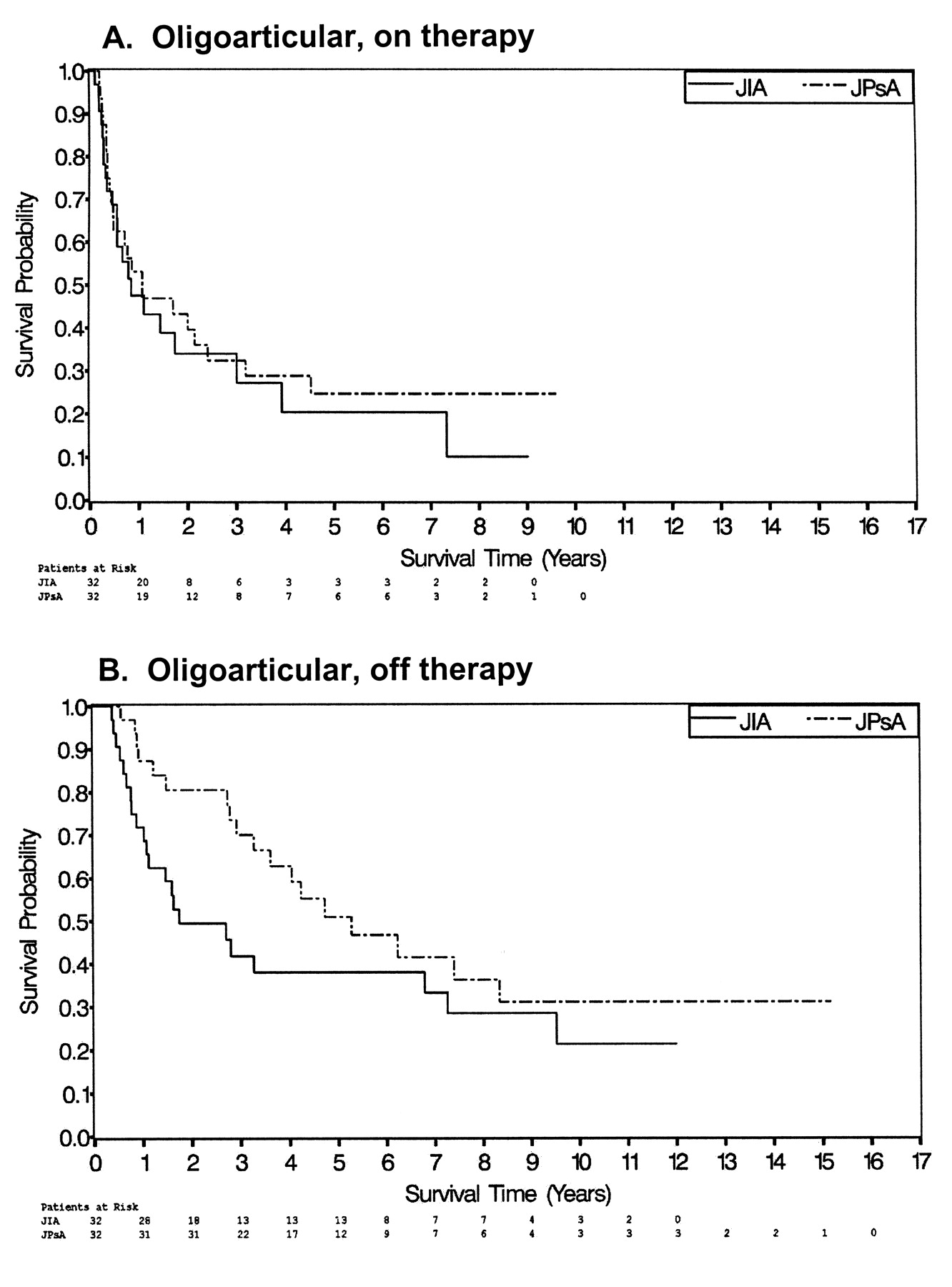
A. Kaplan-Meier survival analysis for the time to first inactive disease for patients with oligoarticular-onset JIA (solid line) and JPsA (broken line), for patients undergoing therapy. B. Survival analysis for the time to first inactive disease for patients with oligoarticular-onset JIA (solid line) and JPsA (broken line), for patients off therapy.
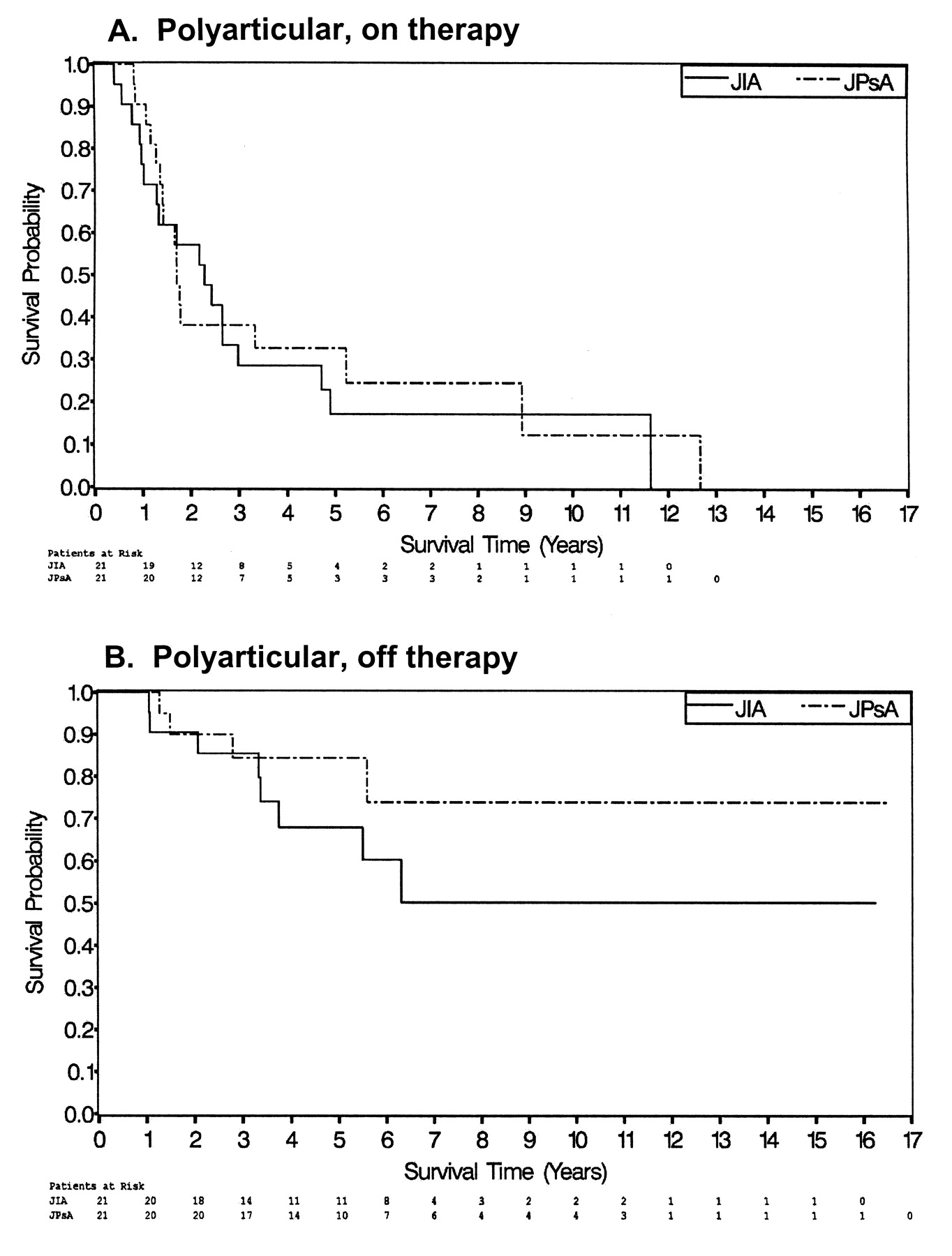
A. Kaplan-Meier survival analysis for the time to first inactive disease for patients with polyarticular-onset JIA (solid line) and JPsA (broken line), for patients undergoing therapy. B. Survival analysis for the time to first inactive disease for patients with polyarticular-onset JIA (solid line) and JPsA (broken line), for patients off therapy.
Combined Group Analysis
Inactive
When we examined the time with inactive disease between the groups for the 81% of the patients who were followed for a minimum of 3 years, we did not find any significant difference in the percentage of time patients were inactive between the groups (30.2% for JPsA and 35.8% for nonpsoriatic JIA; p = 0.5). Similarly, when we separately compared the oligoarticular groups (31.3% for JPsA vs 40.6% for nonpsoriatic JIA) and polyarticular groups (23.8% for JPsA vs 28.50% for nonpsoriatic JIA), there was no significant difference (p = 0.34 and p = 0.87, respectively).
Growth
We were able to collect data about height at the first and last visit to the clinic in 72% of the patients. There was no significant difference in the change in the height percentile between patients with JPsA and patients with nonpsoriatic JIA (data not shown). This finding was also true comparing the patients with oligoarticular-onset arthritis and the patients with polyarticular-onset arthritis separately.
Uveitis
We did not find any difference in the frequency of uveitis between the oligoarticular-onset groups, at 18.8% each. However, we found that a statistically significant higher percentage of patients with polyarticular JPsA developed uveitis, 23.8%, compared to none of the patients with polyarticular JIA (23.8% vs 0%; p = 0.02).
Of the 11 patients with uveitis in the JPsA group (14 affected eyes), 5 had chronic anterior uveitis, 3 had chronic recurrent anterior uveitis, 2 each had 2 short episodes of uveitis that resolved after a short course of corticosteroid eye drops, and 1 patient had acute anterior uveitis. Of the 6 patients with nonpsoriatic JIA and uveitis (8 affected eyes), 4 had chronic anterior uveitis, 1 had chronic recurrent uveitis, and 1 patient had a single short episode of uveitis that resolved after a short course of corticosteroid eye drops.
The visual outcome was similar in both groups. In the nonpsoriatic JIA group, visual impairment was found in 25% of the involved eyes and blindness in 1 eye, compared to visual impairment in 14% of the involved eyes and blindness in 1 eye in the JPsA group. Complications were reported in 5 patients with JPsA (45%; keratopathy, glaucoma, synechia, macular edema, or cataract) compared with 2 patients (33%) in the nonpsoriatic JIA group.
In both groups we found a similar association of the presence of ANA and uveitis between the groups.
DISCUSSION
Various definitions used to classify chronic arthritis in childhood have been proposed to define clinical syndromes, all of which have the common features of a persistent inflammatory arthritis beginning prior to age 16 years. The current ILAR subclassifications of JIA are based on clinical presentation and laboratory data and are used to define homogenous groups of patients to determine prognosis and response to therapies3,16,17. Most researchers in JIA agree with the major classifications of the ILAR criteria, which classify patients into oligoarticular-onset, polyarticular-onset, ERA, and systemic-onset subgroups. However, patients with PsA pose a unique classification dilemma, as they will have features of 1 of the 4 major subsets in addition to meeting the definition of PsA. It is not clear whether patients who meet the classification criteria for PsA have a different longterm prognosis or response to therapy than patients with similar onset type without psoriasis. Studies in adults have demonstrated that there may be differences in the pathogenesis between PsA and RA18,19. Although there are limited data on the pathogenesis of JIA, the data on the pathogenesis of JPsA are even more limited compared to nonpsoriatic JIA20,21. The question of whether JPsA and PsA are pathogenetically the same disease is beyond the scope of our study. The purpose of our study was to determine whether children with oligoarticular- and polyarticular-onset nonpsoriatic JIA and JPsA had a phenotypically similar disease, i.e., similar disease characteristics, outcome, complications, and response to therapy. This may be important when designing therapeutic trials and when speaking to patients regarding prognosis.
The most commonly found onset type of arthritis in childhood is oligoarticular-onset. We found that patients with JPsA and oligoarticular-onset arthritis had clinical features similar to patients with oligoarticular-onset JIA, with a similar pattern of joint involvement and frequency of symmetric arthritis. Although DIP joint involvement and cervical spine involvement were seen only in patients with JPsA, these joints were involved in less than 10% of patients with JPsA. Our finding of a similar frequency of small joint involvement in patients with oligoarticular-onset JIA and JPsA is in contrast to the only previous study directly comparing the distribution of joints between these 2 groups of patients7. Compared to that study, we found both a higher frequency of small joint involvement in JIA patients at presentation and a lower frequency in JPsA patients7. Previously reported frequencies of small joint involvement at presentation of oligoarticular-onset JIA and JPsA have given conflicting results, making comparisons difficult2,5,6,8,11,20. We found a similar frequency of extension to polyarticular course in JPsA and nonpsoriatic JIA, which was similar to the previously reported frequency of extension7,8,20,22–25. Further, we found that the time to extension was similar in both groups. No previous study has compared time to extension. In our study the only differences between the 2 groups of patients with oligoarticular-onset arthritis were that dactylitis and nail pitting were more common in JPsA than nonpsoriatic JIA both at presentation and during followup. Of course dactylitis and nail pitting may be the features that classify a patient as having JPsA, and therefore it may be difficult to accurately determine the frequency of these characteristics in patients with nonpsoriatic JIA. Indeed, in more than one-third of the patients with JPsA and dactylitis, the dactylitis was required to meet the definition of JPsA. Finally, we did not find any differences between the groups in the types of therapies used or in the frequency in which they were used. Other independent studies are needed to confirm our findings. The use of nail pitting as a criterion is also problematic, as the ILAR criteria do not define the number of nail pits required to meet this minor criterion.
The second most frequent onset type of arthritis is RF-negative polyarticular-onset. Comparing the type and frequency of joint involvement between the 2 groups, the only difference that we found was that patients with JPsA were less likely to have hip involvement than patients with nonpsoriatic JIA. Similar to previous studies, knees, ankles, and wrists were the most commonly involved joint in both groups, and the groups did not differ regarding frequency of involvement of any other joints including small joints of hands or feet, the presence of symmetric arthritis, or the presence of dactylitis5,9,11,20. Our findings are unique, as none of the previous studies in JPsA separately examined patients with polyarticular-onset and oligoarticular-onset JPsA. There was no difference between the polyarticular-onset groups in the percentage of patients with dactylitis at presentation or during followup. We did not find any difference in the frequency of the use of methotrexate or any other therapies between the groups.
One potentially important aspect to differentiate JPsA and nonpsoriatic JIA would be longterm joint outcome and growth. We found that patients with polyarticular JIA had a higher frequency of contractures during the course of the illness than patients with JPsA. However, at last followup there was no difference in the frequency of persistent contractures or in the joints with contractures. Similarly, we did not find any difference in the frequency of contractures between the groups for patients with oligoarticular-onset arthritis. Only 1 patient in either cohort, a patient with nonpsoriatic JIA, had a joint replacement and only 1 patient had a leg-length discrepancy at last followup. In addition there was no difference in the mean CHAQ scores between the patients with nonpsoriatic JIA and JPsA, regardless of onset type. We did not find any difference in the percentage of time patients had inactive disease between the groups when all patients were considered or when onset types were considered separately. We did not find any significant differences regarding time to first inactive disease. Finally, there was no difference in the overall rate of growth between patients with nonpsoriatic JIA or JPsA. Although these results suggest that longterm outcome, mean followup of > 6 years, did not differ between patients with psoriasis and JIA and without psoriasis, longer followup times and larger cohorts are needed to confirm the results.
The last important outcome to measure is uveitis. There was no difference in the outcome of uveitis in patients with oligoarticular-onset nonpsoriatic JIA and JPsA. Surprisingly, none of the patients with polyarticular JIA developed uveitis, while 23% of patients with polyarticular JPsA developed uveitis. The absence of uveitis in our RF-negative polyarticular-onset cohort has not previously been reported, and was significantly lower than the frequency previously reported from our center13. In this larger cohort we found a 14% frequency of uveitis in patients with polyarticular RF-negative JIA, which was similar to the frequency of uveitis found in our JPsA cohort. This suggests that the finding of a difference in the frequency of uveitis in our current study was a result of the smaller sample size13. In our study and in previous studies, the type and course of uveitis seen in JPsA closely resembles the uveitis of nonpsoriatic JIA in its onset type and longterm outcome, and not the uveitis reported to be associated with adult psoriatic arthritis26,27. We found that patients with nonpsoriatic JIA and JPsA who developed uveitis had the same association with a positive ANA.
The main limitations of our study were its retrospective design and the relatively small numbers of patients. We matched patients for date of diagnosis, in order to control for the new modalities in JIA therapy that have emerged from the beginning of the study in 1985 to 2005. This matching resulted in the inability to determine if demographic data such as age at onset and male:female ratio are factors that may differ between patients with nonpsoriatic JIA and JPsA. However, our major focus was on the clinical question of whether the presence or absence of psoriasis alters the clinical course or response to therapy. The only way to determine the importance of psoriasis in clinical outcome was by matching patients according to the above criteria, and the benefit of the matching supersedes the limitations imposed by this matching process. A limitation of all articles describing JPsA is whether the ILAR or the Vancouver criteria should be used28. We decided to use both the ILAR and the Vancouver criteria in our cohort, as both of them were previously used and it is not clear which is the most appropriate. Unlike the report from Stoll, et al11, which eliminated 58% of patients diagnosed with the Vancouver criteria using the ILAR criteria, we eliminated only 1 patient when applying the ILAR criteria. The major difference between our findings and that of Stoll, et al was the high frequency of “psoriatic-like rash” reported by Stoll, et al (44%). The practice at our institution was to classify the rash as fulfilling the rash criterion only in patients with true psoriasis, as we were not sure of the definition of psoriatic-like rash. Finally, we do not have data on outcome of these patients into adulthood, but more than 80% of patients were followed for a minimum of 3 years.
In our study, we have shown that nonpsoriatic JIA and JPsA have very similar clinical phenotype and longterm outcome. The clinical manifestations and outcome of oligoarticular-onset JPsA more closely resembled oligoarticular-onset JIA than polyarticular-onset JPsA. The only exception was that dactylitis occurred only in patients with oligoarticular JPsA and not in patients with oligoarticular JIA. In addition, the longterm joint and functional outcomes were similar between the groups, as was the type and course of uveitis. Similarly, polyarticular-onset JPsA more closely resembled polyarticular-onset nonpsoriatic JIA than oligoarticular-onset JPsA regarding disease characteristics, outcome, and therapy, except for a lower frequency of hip and knee involvement. There was no difference in the frequency of dactylitis between the cohorts of patients with polyarticular-onset arthritis. We suggest that large, longterm prospective studies are required to accurately determine whether patients with JPsA should be grouped with patients with nonpsoriatic JIA in therapeutic trials and whether the presence of psoriasis or 2 minor criteria warrants a separate category within the ILAR classification, or rather, that patients who are currently classified as having JPsA are better classified within the oligoarticular and polyarticular categories. Our study was not designed to determine whether JPsA and nonpsoriatic JIA are pathogenetically identical.
Footnotes
- Accepted for publication February 25, 2009.








{kind=link}
{kind=link}