

- Department of Neurological Surgery, University of Florida, Gainesville, Florida, USA
- Department of Neurosurgery, North Shore Long Island Jewish, Manhasset, NY, USA
- Department of Pathology, Immunology, and Laboratory Medicine, University of Florida, Gainesville, Florida, USA
Correspondence Address:
Kristopher G. Hooten
Department of Neurological Surgery, University of Florida, Gainesville, Florida, USA
DOI:10.4103/2152-7806.180300
Copyright: © Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Hooten KG, Oliveria SF, Sadrameli SS, Gandhi S, Yachnis AT, Lewis SB. Bilateral internal auditory canal gangliogliomas mimicking neurofibromatosis Type II. Surg Neurol Int 13-Apr-2016;7:39
How to cite this URL: Hooten KG, Oliveria SF, Sadrameli SS, Gandhi S, Yachnis AT, Lewis SB. Bilateral internal auditory canal gangliogliomas mimicking neurofibromatosis Type II. Surg Neurol Int 13-Apr-2016;7:39. Available from: http://surgicalneurologyint.com/surgicalint_articles/bilateral-internal-auditory-canal-gangliogliomas-mimicking-neurofibromatosis-type-ii/
Abstract
Background:Gangliogliomas are rare low grade, typically well-differentiated, tumors that are composed of mature ganglion cells and neoplastic glial cells. These tumors can appear at virtually any location along the neuroaxis but classically occur in the temporal lobe of young patients. In a small number of cases, gangliogliomas have presented as masses in the brainstem or involving cranial nerves. With the exception of vestibular schwannomas, bilateral tumors in the region of the internal auditory canal (IAC) or cerebellopontine angle (CPA) are exceedingly rare.
Case Description:We report a case of a 58-year-old male who presented with hearing loss, tinnitus, and vertigo. Initial magnetic resonance imaging revealed bilateral nonenhancing IAC/CPA tumors. Based on this finding, a presumptive diagnosis of neurofibromatosis Type II was made, which was initially managed conservatively with close observation. He returned for follow-up with worsening vertigo and tinnitus, thus prompting the decision to proceed with surgical resection of the symptomatic mass. Intriguingly, pathological study demonstrated a WHO Grade I ganglioglioma.
Description:We report a case of a 58-year-old male who presented with hearing loss, tinnitus, and vertigo. Initial magnetic resonance imaging revealed bilateral nonenhancing IAC/CPA tumors. Based on this finding, a presumptive diagnosis of neurofibromatosis Type II was made, which was initially managed conservatively with close observation. He returned for follow-up with worsening vertigo and tinnitus, thus prompting the decision to proceed with surgical resection of the symptomatic mass. Intriguingly, pathological study demonstrated a WHO Grade I ganglioglioma.
Conclusion:This is the first reported case of bilateral IAC/CPA gangliogliomas. When evaluating bilateral IAC/CPA lesions with unusual imaging characteristics, ganglioglioma should be included in the differential diagnosis.
Keywords: Bilateral, cerebellar-pontine angle, gangliogliomas, internal auditory canal, tumors
INTRODUCTION
Gangliogliomas are relatively rare tumors accounting for only 1% of all intracranial neoplasms. These tumors are composed of a combination of both neuronal and glial cell types and are typically benign, low-grade, and well differentiated.[
Bilateral internal auditory canal (IAC)/cerebellopontine angle (CPA) tumors are virtually pathognomonic for vestibular schwannomas in the setting of neurofibromatosis Type II (NFII).[
CLINICAL PRESENTATION
A 58-year-old male presented with new onset vertigo and chronic asymmetric hearing loss, which was worse in the left than the right ear. The patient also complained of mild left-sided tinnitus. Over 3 months he developed progressively worsening balance causing him to fall, typically to his right side. Neurological exam was unremarkable except for bilateral sensorineural hearing loss. His initial audiogram confirmed the finding of bilateral sensorineural hearing loss, with profound loss of hearing in the higher frequencies that were most prominent on the left side. Magnetic resonance imaging (MRI) of the brain revealed bilateral nonenhancing IAC/CPA masses [Figure
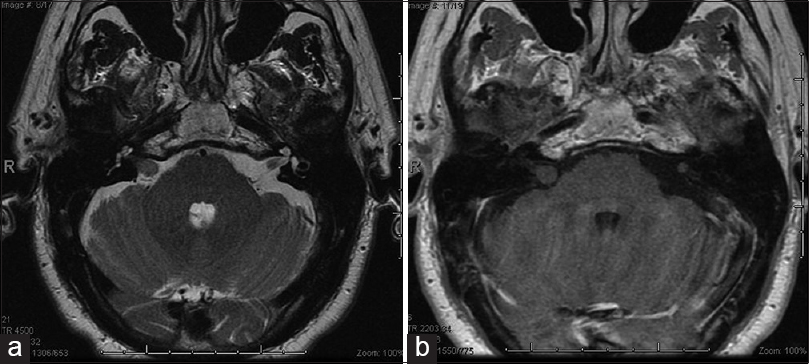
At his 1 year follow-up visit, the patient reported worsening left-sided hearing loss, tinnitus, and otalgia and had begun taking a benzodiazepine to alleviate his symptoms. Repeat MRI of the brain at this time demonstrated the modest growth of both IAC/CPA masses, which remained nonenhancing. The mass on the left measured 6 mm × 5 mm × 4 mm; the right-sided mass measured 10 mm × 8 mm × 7 mm with growth of the intracanalicular portion to 8 mm in length [Figure

INTERVENTION
The patient underwent a left retrosigmoid craniotomy for tumor resection. A small lesion involving the intracanalicular portion of the eighth nerve complex was encountered and completely resected.
The excised tumor was an oval, well circumscribed, gray-tan, nodule that measured 0.5 cm × 0.5 cm × 0.4 cm. One-half was submitted for intra-operative consultation, which yielded a diagnosis of “ganglioneuroma versus ganglioglioma.” Examination of formalin-fixed, paraffin-embedded tissue sections reveled circumscribed neuroglial tissue composed of mature ganglion cells existing in a background of low-grade astrocyte-like cells with coarse processes [Figure
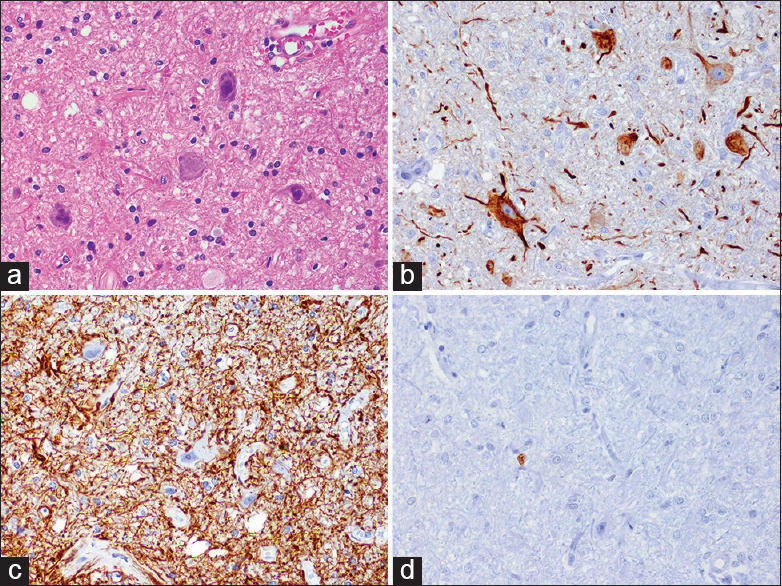
Figure 3
Surgical pathologic studies consistent with ganglioglioma. (a) H and E staining. Several ganglion cells, with cytoplasmic Nissl substance and smudgy nuclei, exist within a low grade appearing glial stroma. (b) Ganglion cells within the tumor show strong neurofilament protein immunoreactivity and haphazardly oriented cell processes. (c) Glial fibrillary acidic protein is strongly immunoreactive within a background astrocyte-like cell processes. (d) Only a rare cell was immunoreactive for Ki-67 (MIB-1)
Neurofilament protein was strongly immunoreactive in the ganglion cells and revealed un-oriented cells’ processes extending into the glial stroma [
Postoperatively, the patient's complaints of tinnitus improved. Postoperatively, his hearing remained stable and his House–Brackman grade was 1/6 bilaterally.
DISCUSSION
Gangliogliomas are rare, mixed glioneuronal tumors comprising only 1.3% of all brain tumors.[
Classically, these tumors arise in the temporal lobe with seizures being the most common presenting symptom. Gangliogliomas have nevertheless been reported in all regions of the neuroaxis including the spinal cord, brainstem, cerebellum, ventricular system, cranial nerves, pituitary and pineal glands, with varying clinical presentations dependent on location.[
Bilateral IAC/CPA masses are characteristic of NFII with bilateral schwannomas occurring on either the vestibular or less commonly facial nerves.[
The desired surgical treatment strategy for gangliogliomas is gross total resection when feasible. Adjuvant chemotherapy or radiation is not typically recommended for low-grade tumors (WHO I), but may be appropriate for select patients.[
In this case, gross total resection was achieved for the left sided tumor. Based on the low grade of the left-sided tumor and minimal symptoms associated with the right-sided tumor, the patient is being followed closely with regular hearing monitoring and serial imaging. For chronic and/or benign lesions, it is paramount to approach the patient conservatively, focusing on preservation of hearing, and facial nerve function.
CONCLUSION
Gangliogliomas are rare and typically benign tumors that may occur at any location along the neuroaxis. Clinical course and MRI can aid the diagnosis of gangliogliomas affecting cranial nerves before surgery. When evaluating bilateral IAC/CPA lesions with unusual imaging characteristics, ganglioglioma should be included in the differential diagnosis.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
References
1. Baldwin D, King TT, Chevretton E, Morrison AW. Bilateral cerebellopontine angle tumors in neurofibromatosis type 2. J Neurosurg. 1991. 74: 910-5
2. Becker AJ, Löbach M, Klein H, Normann S, Nöthen MM, von Deimling A. Mutational analysis of TSC1 and TSC2 genes in gangliogliomas. Neuropathol Appl Neurobiol. 2001. 27: 105-14
3. Blatt GL, Ahuja A, Miller LL, Ostrow PT, Soloniuk DS. Cerebellomedullary ganglioglioma: CT and MR findings. AJNR Am J Neuroradiol. 1995. 16: 790-2
4. Bonneville F, Sarrazin JL, Marsot-Dupuch K, Iffenecker C, Cordoliani YS, Doyon D. Unusual lesions of the cerebellopontine angle: A segmental approach. Radiographics. 2001. 21: 419-38
5. Bushe KA, Naumann M, Warmuth-Metz M, Meixensberger J, Müller J. Maffucci's syndrome with bilateral cartilaginous tumors of the cerebellopontine angle. Neurosurgery. 1990. 27: 625-8
6. Casar Borota O, Jacobsen EA, Scheie D. Bilateral atypical choroid plexus papillomas in cerebellopontine angles mimicking neurofibromatosis 2. Acta Neuropathol. 2006. 111: 500-2
7. Compton JJ, Laack NN, Eckel LJ, Schomas DA, Giannini C, Meyer FB. Long-term outcomes for low-grade intracranial ganglioglioma: 30-year experience from the Mayo Clinic. J Neurosurg. 2012. 117: 825-30
8. DeMarchi R, Abu-Abed S, Munoz D, Loch Macdonald R. Malignant ganglioglioma: Case report and review of literature. J Neurooncol. 2011. 101: 311-8
9. Ergün T, Lakadamyali H, Avci S. Bilateral cerebellopontine angle lipoma in an asymptomatic patient: A case report. Kulak Burun Bogaz Ihtis Derg. 2009. 19: 106-8
10. Friedman WA, Vries JK, Quisling RG. Ganglioglioma of the medulla oblongata. Surg Neurol. 1979. 12: 105-8
11. Gerganov VM, Hore N, Herold C, Wrede K, Stan AC, Samii A. Bilateral malignant melanoma metastases to the internal auditory canal/cerebellopontine angle: Surgical management and preservation of function. J Neurosurg. 2008. 108: 803-7
12. Gopalakrishnan CV, Shrivastava A, Nair S, Radhakrishnan N. Brainstem ganglioglioma in an infant: Case report and review of literature. J Pediatr Neurosci. 2013. 8: 41-5
13. Hargus G, Bink A, Nagel I, Paulus W, Harder A. Bilateral ganglioglioma of the trigeminal nerve in an 83-year-old man. Neuropathology. 2014. 34: 159-63
14. Hariharan S, Zhu J, Nadkarni MA, Donahue JE. Metastatic lung cancer in the cerebellopontine angles mimicking bilateral acoustic neuroma. J Clin Neurosci. 2005. 12: 184-6
15. Jalali R, Deopujari CE, Bhutani R, Suhas U, Rajasekharan P, Kane SV. Suprasellar ganglioglioma with unusual diffuse involvement of the entire optico-chiasmal hypothalamic pathway. J Cancer Res Ther. 2008. 4: 140-3
16. Johnson MD, Jennings MT, Lavin P, Creasy JL, Maciunas RJ. Ganglioglioma of the pineal gland: Clinical and radiographic response to stereotactic radiosurgical ablation. J Child Neurol. 1995. 10: 247-9
17. Kasliwal MK, Suri A, Rishi A, Suri V, Sharma BS, Sarkar C. Symptomatic bilateral cerebellar mass lesions: An unusual presentation of intracranial xanthogranuloma. J Clin Neurosci. 2008. 15: 1401-4
18. Kempermann G, Neumann HP, Scheremet R, Volk B, Mann W, Gilsbach J. Deafness due to bilateral endolymphatic sac tumours in a case of von Hippel-Lindau syndrome. J Neurol Neurosurg Psychiatry. 1996. 61: 318-20
19. Kim MS, Lee SI, Sim SH. Brain tumors with cysts treated with Gamma Knife radiosurgery: Is microsurgery indicated?. Stereotact Funct Neurosurg. 1999. 72: 38-44
20. Kwon JW, Kim IO, Cheon JE, Kim WS, Chi JG, Wang KC. Cerebellopontine angle ganglioglioma: MR findings. AJNR Am J Neuroradiol. 2001. 22: 1377-9
21. Liauw SL, Byer JE, Yachnis AT, Amdur RJ, Mendenhall WM. Radiotherapy after subtotally resected or recurrent ganglioglioma. Int J Radiat Oncol Biol Phys. 2007. 67: 244-7
22. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007. 114: 97-109
23. Luyken C, Blümcke I, Fimmers R, Urbach H, Wiestler OD, Schramm J. Supratentorial gangliogliomas: Histopathologic grading and tumor recurrence in 184 patients with a median follow-up of 8 years. Cancer. 2004. 101: 146-55
24. Miller G, Towfighi J, Page RB. Spinal cord ganglioglioma presenting as hydrocephalus. J Neurooncol. 1990. 9: 147-52
25. Milligan BD, Giannini C, Link MJ. Ganglioglioma in the cerebellopontine angle in a child. Case report and review of the literature. J Neurosurg. 2007. 107: 292-6
26. Pant I, Suri V, Chaturvedi S, Dua R, Kanodia AK. Ganglioglioma of optic chiasma: Case report and review of literature. Childs Nerv Syst. 2006. 22: 717-20
27. Rades D, Zwick L, Leppert J, Bonsanto MM, Tronnier V, Dunst J. The role of postoperative radiotherapy for the treatment of gangliogliomas. Cancer. 2010. 116: 432-42
28. Rush S, Foreman N, Liu A. Brainstem ganglioglioma successfully treated with vemurafenib. J Clin Oncol. 2013. 31: e159-60
29. Selch MT, Goy BW, Lee SP, El-Sadin S, Kincaid P, Park SH. Gangliogliomas: Experience with 34 patients and review of the literature. Am J Clin Oncol. 1998. 21: 557-64
30. Shuangshoti S, Kirsch E, Bannan P, Fabian VA. Ganglioglioma of the optic chiasm: Case report and review of the literature. AJNR Am J Neuroradiol. 2000. 21: 1486-9
31. Springborg JB, Poulsgaard L, Thomsen J. Nonvestibular schwannoma tumors in the cerebellopontine angle: A structured approach and management guidelines. Skull Base. 2008. 18: 217-27
32. Tanaka S, Pollock BE. Hearing preservation after stereotactic radiosurgery for bilateral cerebellopontine angle meningiomas. Minim Invasive Neurosurg. 2009. 52: 259-62
33. Vajramani GV, Dambatta S, Walker M, Grundy PL. Multiple gangliogliomas of the optic pathway. Br J Neurosurg. 2006. 20: 428-30

