

Novel rapid identification of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) by real-time RT-PCR using BD Max Open System in Taiwan
- Published
- Accepted
- Received
- Academic Editor
- Elliot Lefkowitz
- Subject Areas
- Microbiology, Molecular Biology, Virology
- Keywords
- SARS-CoV-2, BD Max platform, Real-time RT-PCR
- Copyright
- © 2020 Perng et al.
- Licence
- This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. For attribution, the original author(s), title, publication source (PeerJ) and either DOI or URL of the article must be cited.
- Cite this article
- 2020. Novel rapid identification of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) by real-time RT-PCR using BD Max Open System in Taiwan. PeerJ 8:e9318 https://doi.org/10.7717/peerj.9318
Abstract
Coronavirus disease 2019 has become a worldwide pandemic. By April 7, 2020, approximately 1,279,722 confirmed cases were reported worldwide including those in Asia, European Region, African Region and Region of the Americas. Rapid and accurate detection of Severe Acute Respiratory Syndrome Virus 2 (SARS-CoV-2) is critical for patient care and implementing public health measures to control the spread of infection. In this study, we developed and validated a rapid total nucleic acid extraction method based on real‐time RT-PCR for reliable, high‐throughput identification of SARS-CoV-2 using the BD MAX platform. For clinical validation, 300 throat swab and 100 sputum clinical samples were examined by both the BD MAX platform and in-house real-time RT-PCR methods, which showed 100% concordant results. This BD MAX protocol is fully automated and the turnaround time from sample to results is approximately 2.5 h for 24 samples compared to 4.8 h by in-house real-time RT-PCR. Our developed BD MAX RT-PCR assay can accurately identify SARS-CoV-2 infection and shorten the turnaround time to increase the effectiveness of control and prevention measures for this emerging infectious disease.
Introduction
On December 31, 2019, a cluster of pneumonia cases of unknown etiology was reported in Wuhan, Hubei Province, China (Chan et al., 2020a). Later, the Chinese Centers for Disease Control and Prevention (China CDC) reported a novel coronavirus as the causative agent of this outbreak, which was phylogenetically classified into a novel sister clade of SARS virus and named as the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The disease caused by this virus has been called as novel coronavirus disease 2019 (COVID-19).
COVID-19 is an emerging whole world crisis issue. On March 11, 2020, the COVID-19 outbreak was characterized as a pandemic by the World Health Organization. By April 7, 2020, 72,614 fatalities and 1,279,722 laboratory-confirmed cases were reported globally (Centers for Disease Control & Prevention (CDC), 2020; Ghinai et al., 2020; World Health Organization (WHO), 2020; Wu & McGoogan, 2020).
A robust, sensitive, specific and high-throughput molecular detection method is urgently needed for SARS-CoV-2 diagnosis. Various methods for detecting SARS-CoV-2 have been reported, including real-time reverse transcription polymerase chain reaction (RT-PCR) and serological testing (Ai et al., 2020; Li et al., 2020b; Yu et al., 2020). Currently, real-time RT-PCR is considered as the gold standard of diagnosis for SARS-CoV-2 because of its high sensitivity; this method can detect SARS-CoV-2 in various samples types, including oropharyngeal swab, sputum and blood (Wang et al., 2020a; Xie et al., 2020).
The BD MAX System (BD Diagnostic Systems, Franklin Lakes, NJ, USA) is an automated platform which nucleic acid extraction and real-time RT-PCR are performed on the same instrument. This BD MAX System offers not only FDA-cleared panel assays but also an open system mode for user-developed tests (Hofko et al., 2014; McHugh et al., 2018; Stokes et al., 2019; Widen, Healer & Silbert, 2014). This study was designed to develop a dual RT-PCR tests for detecting the E and RdRp genes of SARS-CoV-2 directly from clinical samples using the open system mode of the BD MAX instrument and compare the results to those obtained by the in-house real-time RT-PCR method used in our hospital.
Materials and Methods
Clinical specimens
This study was approved by Institutional Review Board, Tri-Service General Hospital (TSGHIRB No.: C202005041), registered on 20 March 2020. Informed consent was obtained from patients who signed permission to participate. Throat swab (COPAN COVID-19 Collection & Transport Kits with Universal Transport Medium or Virus Transport Swabs 147C) (n = 300) and sputum (n = 100) samples were collected from patients with highly suspected travel or contact history in northern Taiwan. Positive control was used with patient’s diluted positive RNA aliquoted into Eppendorf tube stored in −80 °C (a range of Ct (threshold cycle) value 34 ± 2 for each run acceptance). Throat swabs were placed in 0.5 mL phosphate-buffered saline and mixed vigorously with a vortex mixer for 30 s to release the cells. Sputum was liquefied by adding an equal volume of 2% N-acetyl-L-cysteine in phosphate-buffered saline followed by incubation for 10 min.
In-house SARS-CoV-2 laboratory-developed test (LDT)
Nucleic acid extraction
Total nucleic acid containing viral RNA was extracted from 0.3 mL of the throat swab supernatant or liquefied sputum, by using LabTurbo Viral nucleic acid extraction kits on a LabTurbo 48 automatic extractor (Taigen Bioscience Corp., Taipei, Taiwan). RNA was eluted with 60 µL of RNase-free water.
Real-time one-step RT-PCR
The primer and probe sequences of the two target genes (E gene as the first-line screening target, followed by confirmatory testing with the RdRp gene) has been previously described (Corman et al., 2020) (Table 1). The 10× TCID50 Equine arteritis virus (EAV) (DIA-EIC; Diagenode, Belgium) was added to extraction buffer for internal control of monitoring RT-PCR inhibitors (Ct value 32 ± 2 as acceptance level for each assay). All primers and probes were synthesized and provided by Tib-Molbiol (Berlin, Germany). All assays were performed under the same conditions with some modifications. A 20-μL reaction was prepared containing five μL of RNA, 10 μL of 2× SensiFAST Probe No-ROX One-Step mix (Bioline Reagents Ltd., London, UK), 400 nM of forward and reverse primers, 200 nM of probe, 0.2 μL of reverse transcriptase, and 0.4 μL of RiboSafe RNase inhibitor (Bioline Reagents Ltd., London, UK). Thermal cycling was performed as follows: reverse transcription for 10 min at 50 °C, followed by 95 °C for 2 min and then 50 cycles of 95 °C for 5 s and 58 °C for 30 s on a Rotor-Gene Q real-time PCR machine (Qiagen, Hilden, Germany).
| Target gene | Primer name | Sequence (5′→3′) | References |
|---|---|---|---|
| RdRp (ORF1ab) | RdRp_SARSr-F2 | GTGARATGGTCATGTGTGGCGG | Corman et al. (2020) |
| RdRp_SARSr-R2† | CAAATGTTAAAAACACTATTAGCATA | ||
| RdRp_SARSr-P2 | FAM-CAGGTGGAACCTCATCAGGAGATGC-BBQ | ||
| E | E_Sarbeco_F1 | ACAGGTACGTTAATAGTTAATAGCGT | |
| E_Sarbeco_R2 | ATATTGCAGCAGTACGCACACA | ||
| E_Sarbeco_P1 | FAM-ACACTAGCCATCCTTACTGCGCTTCG-BBQ | ||
| Equine arteritis virus | EAV-IPC-F | CATCTCTTGCTTTGCTCCTT | GenBank EU586274 |
| (EAV) | EAV-IPC-R | AGCCGCACCTTCACATTGAT | |
| IPC | EAV-IPC-P | HEX-CTGACAGCGCTTCTGGTTTCATCAGCT-BHQ |
Note:
BD MAX system procedure
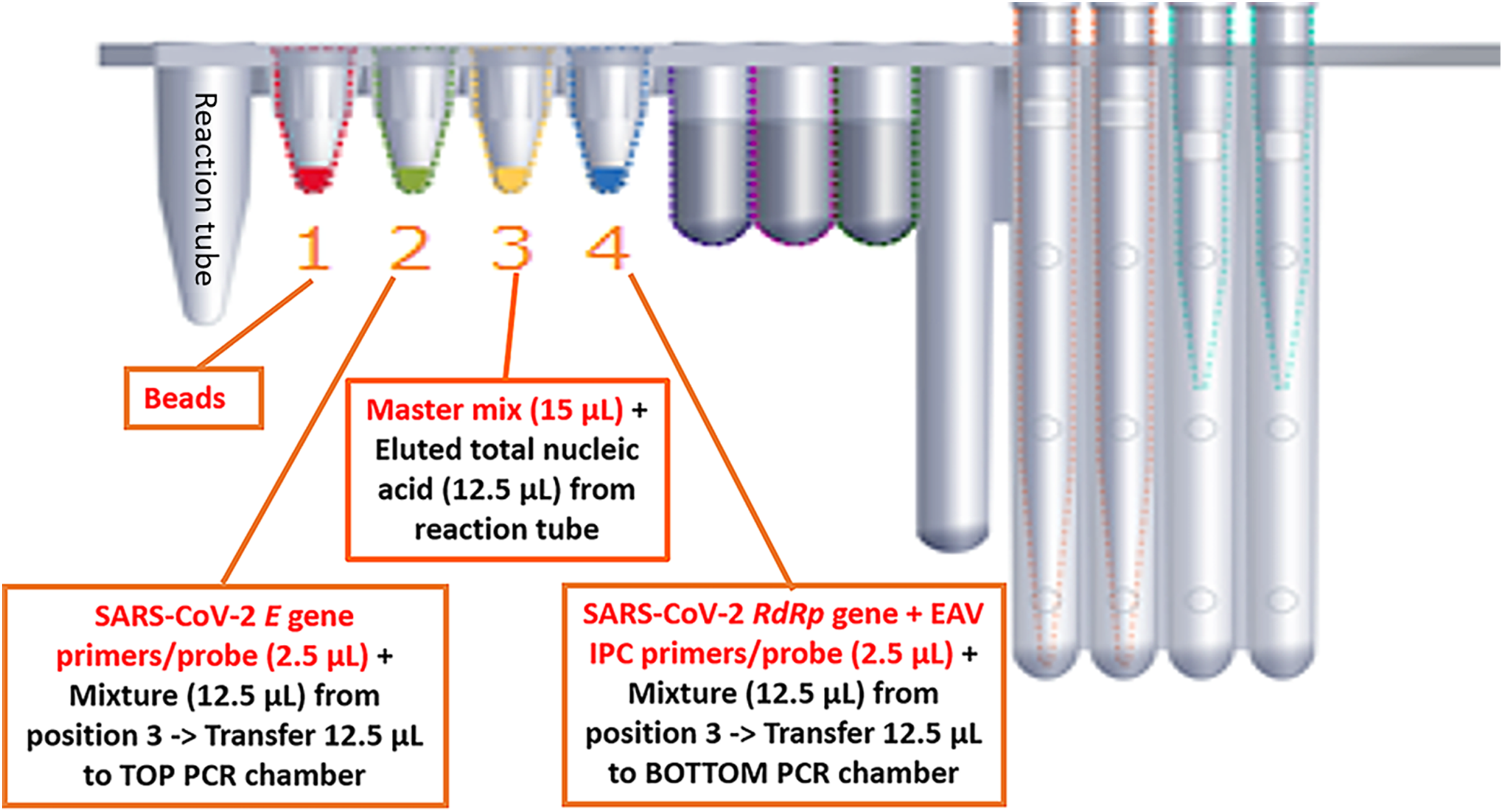
We optimized the BD MAX ExK TNA 3 total nucleic acid Extraction Kit on the BD MAX. The BD MAX uses sample buffer tubes containing 750 μL lysis buffer to which the maximal 500 μL primary sample can be added manually. We compared the in-housed SARS-CoV-2 real-time RT-PCR assay with BD MAX System open mode using the same primers, probe and RT-PCR reagents to detect the E and RdRp genes of SARS-CoV-2. The RT-PCR master mixture without primers & probe (15 μL of 2× SensiFAST Probe No-ROX One-Step mix, 0.3 μL of reverse transcriptase and 0.6 μL of RiboSafe RNase inhibitor) was added to the position 3 on BD cartridge (Fig. 1). The volume of 2.5 μL of primers and probe mixture of E gene and RdRp + IPC gene was added to the position 2 and position 4. Finally, 12.5 μL eluted nucleic acid was added to position 3 and mix with RT-PCR master mixture. A total of 12.5 μL of above mixture was added to position 2 and mix with 2.5 μL E gene primers (2.4 pmole/μL) & probe (1.2 pmole/μL). Residual 12.5 μL mixture was added to position 4 mixing with 2.5 μL RdRp + IPC gene primers (2.4 pmole/μL) & probe (1.2 pmole/μL). The mixture in position 2 and 4 were transferred to TOP/BOTTOM PCR chamber (Fig. 1). We carried out the entire sample-to-result procedure in the BD MAX PCR Cartridges. Assay precision was determined by testing individual samples divided into five parts and extracted/assayed separately. The LDT SARS-CoV-2 real-time RT-PCR assay was used as the “gold standard” to assess the diagnostic performance of the BD MAX assay. The BD MAX assay hands-on time was estimated as the sum of the times required to complete sample preparation, device loading and cleaning and result review and reporting.

Figure 1: Experimental design in detecing SARS-CoV-2 on the BD MAX platform.
{kind=link}
Results
Turnaround time for detecting SARS-COV-2 on the BD MAX System
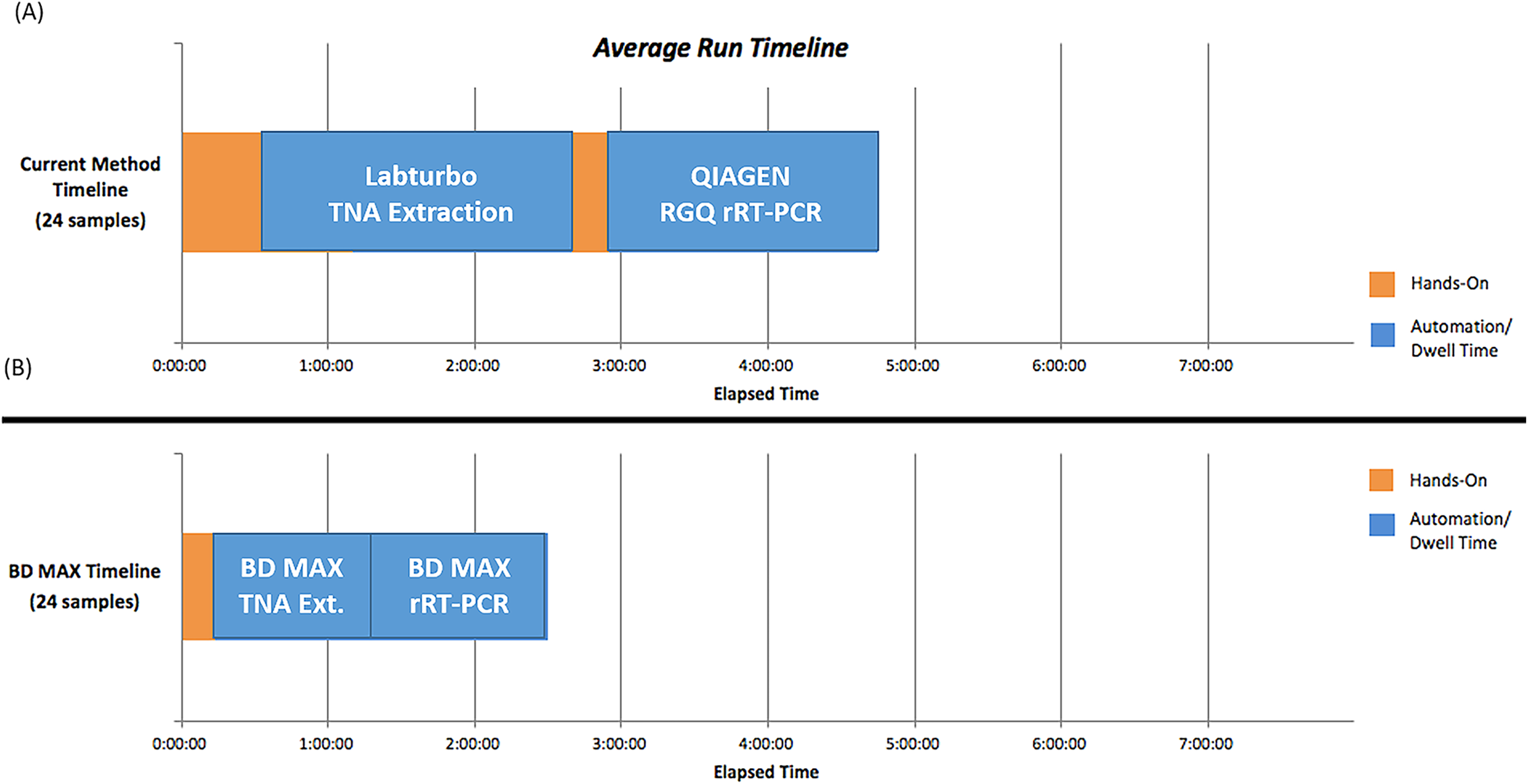
The procedures used for the BD MAX System included sample preparation, device loading, total nucleic acid extraction, RT-PCR, and results interpretation. The hands-on time and turnaround time between the LDT and BD MAX System were compared (Fig. 2). Use of the BD MAX System improved the turnaround time from 4.8 h to approximately 2.5 h with 24 samples processed simultaneously including prepare samples, clean and prepare rack, create worklist, and prepare MMK (master mix), while also decreasing hands-on time, reducing exposure risk. The BD MAX System can also provide results for 192–216 samples in 11 h (depending on how many batches), showing improved capacity compared to the LDT method.

Figure 2: Hands-on time and TAT (turnaround time) comparison between in-house LDT and BD MAX System (A) In house LDT assay (B) BD MAX assay.
{kind=link}
Clinical performance of BD MAX System
The analytical specificity of SARS-CoV-2 E and RdRp gene detection by real-time RT-PCR as well as the cross-reactivity with other respiratory pathogens were determined previously (Corman et al., 2020). Here, we focused on the clinical performance of detection using the BD MAX System.
Reproducibility of BD MAX assay
Five replicates of serial dilutions of SARS-CoV-2-positive samples and a negative template control were tested to evaluate the intra- and inter-assay reproducibility of the BD MAX assay (Table 2). The reproducibility of the Ct values was satisfactory, showing a coefficient of variation of less than 10%.
| SARS-CoV-2 | Inter-run | Intra-run | ||
|---|---|---|---|---|
| No. of positive replicates | Mean Ct ± SD(% coefficient of variation) | No. of positive replicates | Mean Ct ± SD(% coefficient of variation) | |
| E gene | ||||
| +++ | 5 | 15.24 ± 0.95 (6.22) | 5 | 16.80 ± 0.95 (5.65) |
| ++ | 5 | 25.06 ± 0.59 (2.35) | 5 | 25.34 ± 0.58 (2.29) |
| + | 5 | 34.68 ± 0.56 (1.62) | 5 | 35.34 ± 0.61 (1.72) |
| RdRp gene | ||||
| +++ | 5 | 17.04 ± 1.12 (6.58) | 5 | 17.26 ± 1.49 (8.65) |
| ++ | 5 | 26.03 ± 0.82 (3.11) | 5 | 26.92 ± 0.74 (2.75) |
| + | 5 | 36.74 ± 0.41 (1.12) | 5 | 37.20 ± 0.43 (1.16) |
Note:
+, weak positive; ++, positive; +++, strong positive.
Comparison of sensitivity of BD MAX assay and LDT RT-PCR
The empirical sensitivity of the BD MAX assay was determined by evaluating serial dilutions of positive samples and comparing the results to those of the LDT assay. As shown in Fig. 3, diluted specimens were reliably detected by both assays, from the original titer to the 10−3 titers. BD MAX assay detected four times in eight replicates in 10−4 titers which showed less sensitivity compared to LDT assay. Here we used AcroMetrix Coronavirus 2019 (COVID-19) RNA Control (Thermo Fisher Scientific, Waltham, MA, USA) that contain N, S, E and Orf1ab regions of SARS-CoV-2 genome for absolute quantification and studying the limit of detection (LOD). Replicate reactions were done at concentrations around the detection end point. The LOD from replicate tests was 8.5 copies per reaction for the E gene and RdRp gene in LDT assay, while 13.9 copies per reaction for the E gene and RdRp gene in BD MAX assay.
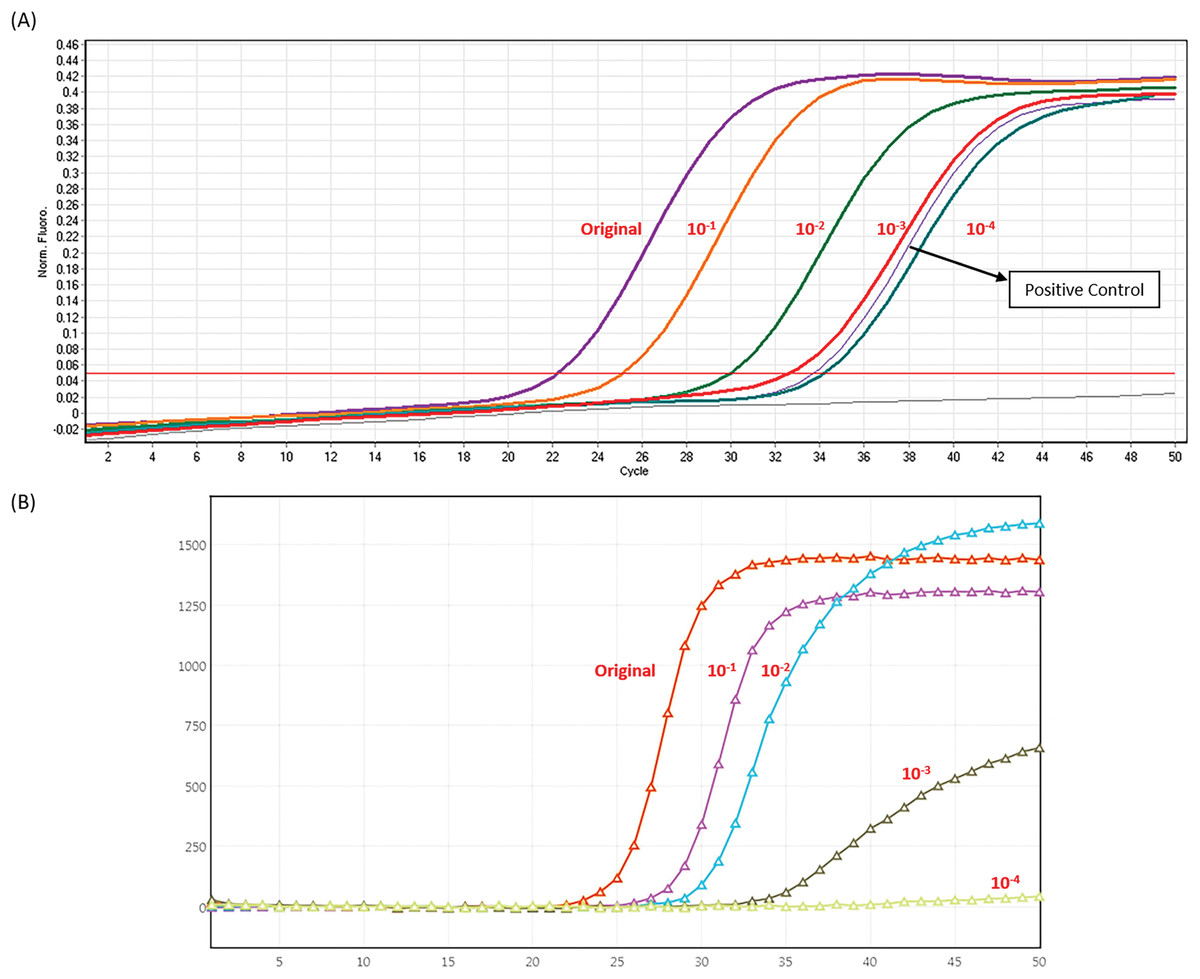
Figure 3: Analytic sensitivity of LDT and BD MAX System (A) In house LDT assay (B) BD MAX assay.
{kind=link}
Clinical validation of BD MAX assay
A total of 400 clinical samples were included in this study. Most samples were throat swabs (n = 300), followed by sputum (n = 100). Among the 400 samples, 28 samples were positive and 272 samples were negative for SARS-CoV-2 real-time RT-PCR with the LDT assay and BD MAX System. These 28 positive samples were further confirmed by Taiwan CDC central laboratory. Concordant results were obtained for both assays in SARS-CoV-2 detection, showing 100% agreement (Table 3). The Ct values of the positive specimens for SARS-CoV-2 (n = 28) were highly correlated in the comparison of the LDT assay and BD MAX System, with Spearman coefficients of 0.96 and 0.91, respectively (Fig. 4).
| BD MAX assay | |||
|---|---|---|---|
| SARS-CoV-2 | Positive | Negative | |
| LDT real-time RT-PCR | Positive | 28 | 0 |
| Negative | 0 | 372 | |
Note:
Positive, both E gene and RdRp gene were detected; Negative, neither E gene nor RdRp gene were detected.
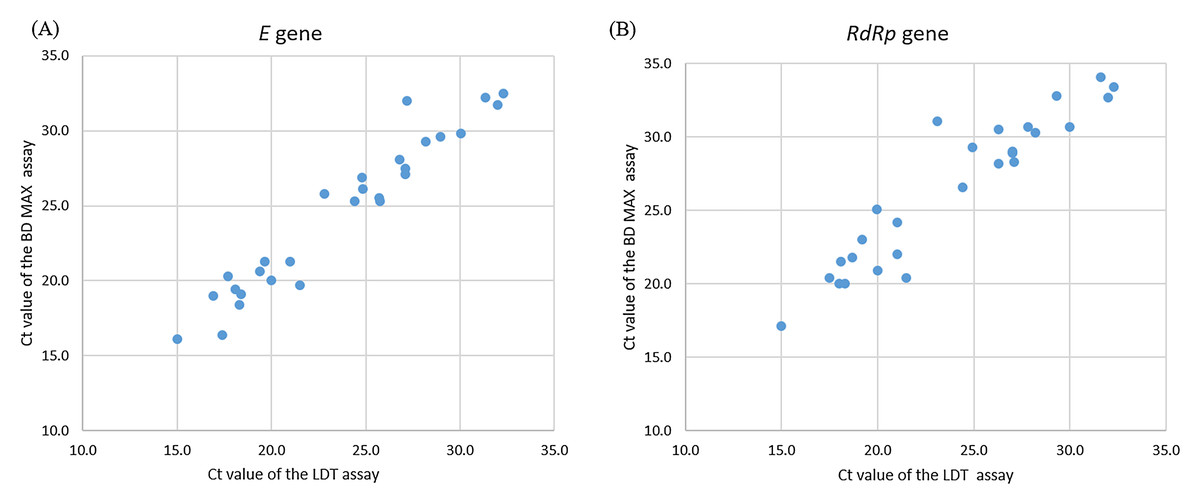
Figure 4: Correlation of Ct values of clinically positive specimens by LDT and BD Max SARS-CoV-2 assays.
(A) E gene for SARS-CoV-2, Spearman coefficient of 0.96. (B) RdRp gene for SARS-CoV-2, Spearman coefficient of 0.91.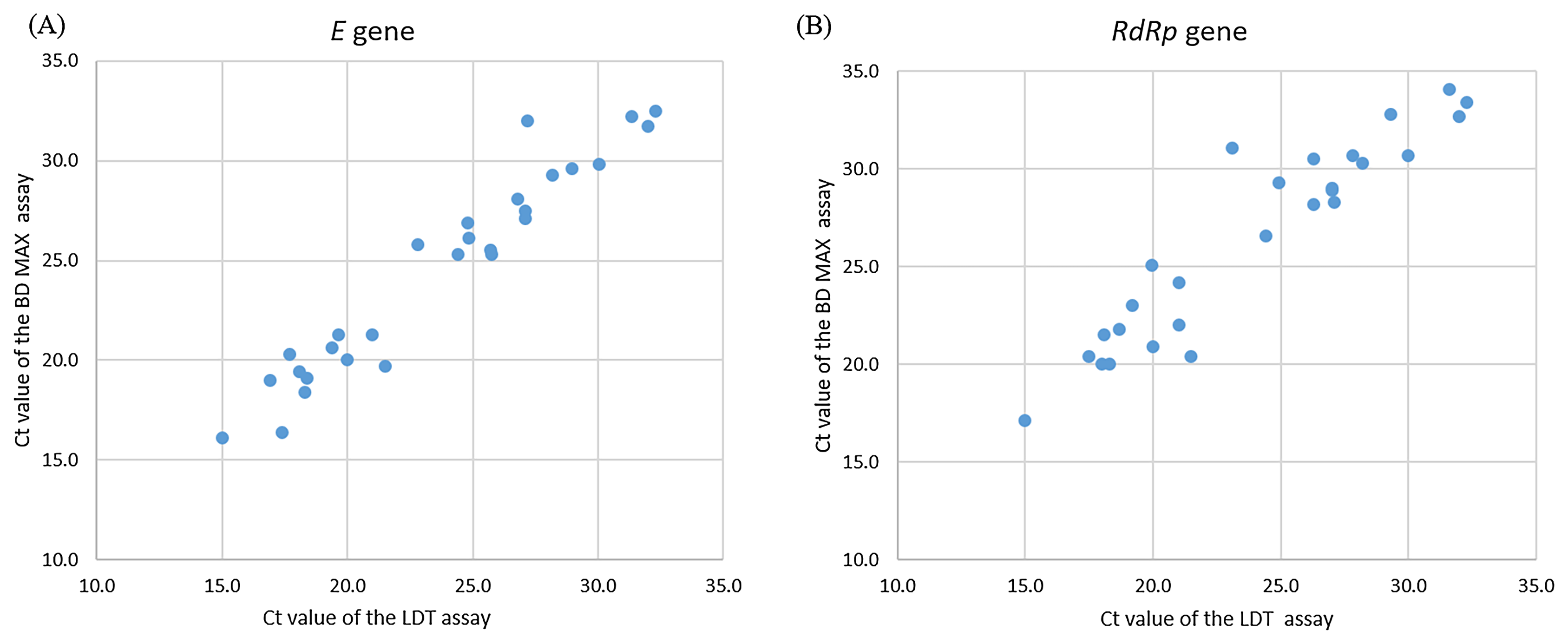{kind=link}
Discussion
This is the first study of the performance of the SARS-CoV-2 detection assay using the BD MAX System. Compared to the in-house results and those from the reference laboratory, the SARS-CoV-2 assay on the BD MAX showed good performance. In this study, we successfully validated a rapid and high-throughput method on the BD MAX platform for accurately and reproducibly identifying SARS-CoV-2 with a greatly reduced turnaround time and fewer hand-on preparation steps including preparing ready-to-use tubes (e.g., 100 Rx without reverse transcriptase stored in −80 °C).
Several studies have reported that real-time RT-PCR gives false-negative results in detecting SARS-CoV-2 (Li et al., 2020a; Liu et al., 2020; Winichakoon et al., 2020). Combining real-time RT-PCR testing with other clinical features is necessary to diagnose COVID-19 (Wang et al., 2020b).
Many detection methods have been used or reported for the diagnosis and/or surveillance of SARS-CoV-2 (Chan et al., 2020b; Corman et al., 2020; Wang et al., 2020b; Yang et al., 2020), among which real-time RT-PCR is the most sensitive. Although this method is routinely used, it requires specialized interpretation and has a long turnaround time. The performance of Molecular BD MAX System for different pathogens has been evaluated previously (Leach et al., 2019; Stokes et al., 2019). These studies demonstrate that the BD MAX System is a good diagnostic tool with a rapid turnaround time, enabling appropriate treatment decisions. During the writing of this manuscript, several molecular assays have been developed for detecting and identifying SARS-CoV-2, including the Cobas SARS-CoV-2 test (Roche, Basel, Switzerland) and TaqPath Covid-19 Combo Kit (Thermo Fisher Scientific, Waltham, MA, USA), which have been authorized for use by the US Food and Drug Administration. To overcome the SARS-CoV-2 pandemic, more sensitive and robust methods are required.
Our designed BD MAX method had several advantages. First, the use of an automated platform with the same primers, probe and master mix as used in our manual LDT assay. Second, there was comparable accuracy, sensitivity and specificity and easy integration into the laboratory workflow. Third, our findings confirm the suitability of the BD MAX system for directly detecting SARS-CoV-2 from clinical specimens. Fourth, the laboratory-developed SARS-CoV-2 BD MAX assay is a dual assay for detecting both E and RdRp gene, allowing for screening and confirming of SARS-CoV-2 infection simultaneously. Fifth, the use of only one platform test in routine settings for the clinical diagnosis of emerging infectious agents in various clinical specimens, including sputum and throat swab samples.
Conclusion
In summary, a SARS-CoV-2 real-time PCR molecular test was developed on the BD MAX System. This test showed excellent sensitivity and specificity and can be used to rapidly detect SARS-CoV-2 infection.
Our SARS-CoV-2 test is also rapid and high-throughput, providing accurate and reproducible results with a significantly reduced turnaround time and fewer hands-on preparation steps. This method is very easy with less skillful requirements and can be implemented in emergency medical laboratories for only short training course.